
Abstract
Objective:
We aimed to examine whether suicidal thoughts and behaviour were independently associated with a wide range of health and social risk behaviours.
Methods:
We conducted cross-sectional analyses of data collected from 13,763 adult males who participated in The Australian Longitudinal Study on Male Health. We fit generalised linear models to estimate the relative risk of engaging in a range of health and social risk behaviours across several domains by suicidal thoughts and behaviour status.
Results:
Men with recent suicidal ideation (relative risk range, 1.10–5.25) and lifetime suicide attempts (relative risk range, 1.10–7.65) had a higher risk of engaging in a broad range of health and social risk behaviours. The associations between suicidal thoughts and behaviour and health and social risk behaviours were typically independent of socio-demographics and in many cases were also independent of depressive symptoms.
Conclusion:
Suicidal thoughts and behaviour overlaps with increased risk of engagement in a wide range of health and social risk behaviours, indicating the need for an alignment of broader public health interventions within clinical and community-based suicide prevention activities. The experience of suicidality may be an important catalyst for a broader psychosocial conversation and assessment of health and social risk behaviours, some of which may be modifiable. These behaviours may not carry an imminent risk of premature death, such as from suicide, but they carry profound health and social consequences if left unaddressed.
Background
Non-fatal suicidal thoughts and behaviours (STB) are common. The lifetime prevalence of STB in general population samples typically ranges between 9.0% and 14.0% for suicidal ideation and 2.7% and 4.6% for suicide attempts (Nock et al., 2008), and their occurrence signals extra vigilance is needed to prevent future suicide. A moderate proportion (7.0–12.0%) of people who experience suicidal ideation are estimated to progress to a suicide attempt within 12 months (Pirkis et al., 2000; ten Have et al., 2009), and a recent cohort study estimated that 5.4% of people who attempt suicide will die by suicide (follow-up 3–25 years) (Bostwick et al., 2016). Yet, while the majority of people experiencing STB will not go on to die by suicide, these behaviours have significant public health implications in their own right.
Persons with STB often have contact with the health system. Yet, clinicians focus on the persons’ suicide risk and any associated mental disorders, often not paying sufficient attention to many other potentially modifiable factors, including other health and social risk behaviours (HSRBs) that may co-occur with STB and that may have profound health and social impacts. There is good evidence that people with severe depression and other serious mental illness have an increased risk of premature death, with a 10- to 20-year reduction in life expectancy (World Health Organization, 2018). Although the risk of suicide has been a major focus, most of the risk of excess mortality is due to chronic physical illness, both non-communicable and communicable (Lawrence et al., 2013). An area that has received much less attention is the increased risk of morbidity and premature mortality for people who experience suicidal behaviours. The studies that have been conducted suggest that people who self-harm are at increased risk of dying from not only suicide but also a wide range of other causes (Bergen et al., 2012; Hawton et al., 2006; Neeleman, 2001). For example, Bergen et al. (2012) undertook a cohort study of people of all ages presenting to emergency departments in the United Kingdom after self-harm and observed that deaths from a wide range of causes other than suicide were 2–7.5 times more frequent than expected. Notably, diseases of the circulatory and digestive systems accounted for a third of all deaths.
One of the predominant explanations given for this excess risk of non-suicide morbidity and mortality among people experiencing suicidal behaviours is underlying psychiatric morbidity. Psychiatric morbidity may result in inequalities in access to physical health care, side effects from pharmaceutical treatments, poor levels of self-care for chronic diseases like diabetes and greater exposure to social disadvantages associated with worse health outcomes (Lawrence and Kisely, 2010; Thornicroft, 2011).
Another explanation is that persons with STB also bear important risk factors with other causes of morbidity and premature death, including engagement in HSRBs that contribute to physical illness and premature mortality (Hawton et al., 2006). These behaviours may exist on an aetiological continuum of self-destruction from sub-intentional to intentional. Studies have observed positive associations between STB and a range of health risk behaviours, for example, smoking (Miller et al., 2000), harmful alcohol (Bergen et al., 2012) and other drug use (Afifi et al., 2007), a high number of sexual partners and non-condom use (Armstrong et al., 2013, 2015; Sicard et al., 2017), sharing needles/injecting equipment with others (Armstrong et al., 2013) and sedentary behaviour (Vancampfort et al., 2019). Associations have also been observed between STB and a range of behaviours that may carry social risks, for example, shoplifting (Afifi et al., 2007), problematic gambling (Maccallum and Blaszczynski, 2003), intimate partner violence (Rhodes et al., 2009) and dating violence and other assaults (Nahapetyan et al., 2014; Orpinas et al., 2017). Some of these social risk behaviours may contribute to poor health through accidental injury or may even lead to death. Others may have important negative consequences for interpersonal and community relationships, and increased risk of criminal justice system involvement, likely compounding existing psychological distress.
Although several studies have examined HSRBs as risk factors for suicidality, the literature on these associations is limited. Many studies have been undertaken on selective samples and often among adolescents exclusively, limiting the generalisability of findings. Furthermore, typically only a handful of HSRBs are examined without being able to sufficiently account for confounding by socio-demographics and other depressive symptoms. Many studies have examined the independent effects of HSRBs on the risk of suicidal ideation and attempts, yet reverse causality cannot be categorically excluded, and few studies have attempted to estimate the independent association of suicidality with the risk of engaging in HSRBs.
This paper addresses these limitations. Using data from a survey of adult males in the general population in Australia, we aimed to: (1) estimate the prevalence of a range of HSRBs among males experiencing recent suicidal ideation or a lifetime history of suicidal attempts compared to controls without STB; and (2) examine whether associations between HSRBs and STB are independent of socio-demographics and other depressive symptoms.
Methods
Data source
The study population consisted of 13,763 adult males who participated in The Australian Longitudinal Study on Male Health, a large-scale cohort study of Australian males aged 10–55 years at baseline. Our paper presents cross-sectional analyses of data collected in 2013–2014 from the baseline wave. Full details of the study design and methods are available elsewhere (Currier et al., 2016). In brief, multistage stratified cluster sampling was used to recruit Australian boys and men from households in major cities, inner regional and outer regional areas. A total of 15,988 Australian males were recruited into the study. The questionnaires given to those aged under 18 differed substantially from those aged ⩾18 years with respect to questions pertaining to HSRBs. Therefore, we excluded males aged <18 years old (n = 2102) from our analyses and those who did not provide valid age data (n = 123).
Questionnaires were self-administered and captured information about suicidal thoughts and attempts, physical and mental health, health-related behaviours, social and environmental determinants of health, health literacy and health service use. The study received ethical clearance from the University of Melbourne Human Sciences Human Ethics Sub-Committee (HREC 1237897 and 1237376).
Measures
HSRBs
A range of HSRBs were assessed across the domains of: (1) substance use; (2) weight, diet and physical activity; (3) sexual behaviour; and (4) intimate partner violence.
We measured substance use based on self-reports of any of the following behaviours: current tobacco smoking; harmful alcohol use as assessed using the Alcohol Use Disorders Identification Test (AUDIT) (Bohn et al., 1995); use of cannabis, ecstasy or cocaine, and heroin or opiates for non-medical purposes at least once in the past 12 months, respectively; and a lifetime history of injecting drug use for non-medical reasons.
We measured weight, diet and physical activity. Being obese or overweight was assessed using self-report measures of height and weight which were used to calculate body mass index (i.e. overweight = 25.0–29.9 kg/m2; obese = >30 kg/m2). Inadequate intake of fruit and vegetables was assessed against a World Health Organization dietary indicator (i.e. less than five serves of fruit and/or vegetables per day) (World Health Organization, 2013). Insufficient or sedentary physical activity was assessed using an indicator based on a combination of time spent exercising and the number of exercise sessions per week (i.e. sedentary = 0 minutes or sessions of exercise per week; insufficient physical activity = between 1 and 149 minutes of exercise per week or between 1 and 4 sessions of exercise per week; sufficient physical activity = 150 or more minutes of exercise and 5 or more sessions per week) (Australian Institute of Health and Welfare, 2003).
We assessed sexual behaviour in the following ways: having sex with people other than regular sexual partner; agreement with the statement ‘if I could, I would frequently change sexual partners’; the number of sexual partners in lifetime (both sexes combined); and number of sexual partners in past 12 months (both sexes combined). Data were unavailable on condom use. To assess engagement in intimate partner violence, participants were asked if they had ever forced a partner to have sex, if they had ever made a partner feel frightened or anxious, and if they had ever physically hurt a partner (all yes vs no responses).
Measurement of depression and suicidal ideation and attempts
Depressive symptoms were measured using the Patient Health Questionnaire-9 (PHQ-9) for adults, a nine-item screening tool based on criteria for depressive disorders in the Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV). The PHQ-9 has well-established criterion, construct and external validity (Kroenke et al., 2001). The PHQ-9 asks participants whether they have been bothered with nine symptoms in the past 2 weeks, with response options on a 4-point Likert-type scale: not at all (0), several days (1), more than half the days (2) and nearly every day (3). Items 1–8 were scored as a continuous measure of depressive symptoms, while Item 9 was used separately as a binary measure of suicidal ideation. Item 9 asks participants how often they had been bothered by ‘thoughts you would be better off dead or of hurting yourself in some way’. This measure was dichotomised to compare participants who responded ‘several days’, ‘more than half the days’ and ‘nearly every day’ with those who responded ‘not at all’. Endorsement of suicidal ideation on this item has been associated with a 75–185% increase in the risk of suicide in a study of veterans in the United States (Louzon et al., 2016). The lifetime prevalence of suicide attempt(s) was assessed by asking participants if they had ever tried to kill themselves.
Socio-demographics
To adjust for potential confounders, we measured age group (18–29; 30–39; 40–49; 50–55), marital status (never married; currently married; separated/divorced/widowed), combined annual household income, all sources and before tax (<$80,000 vs ⩾$80,000) and highest educational qualification (high school or less vs any post-high school education).
Statistical analyses
All analyses were conducted in Stata version 15.0 and accounted for the complex multistage sampling design and unequal probability of selection (Spittal et al., 2016). We estimated (weighted) prevalence of HSRBs stratified by recent suicidal ideation and lifetime suicide attempt. We fit generalised linear models (using the binomial family) to estimate the relative risk (RR) of engaging in a range of HSRBs by suicidal behaviour status (i.e. one set of models for suicidal ideation and another for suicide attempt). However, where the outcome variable was of count form, negative binomial models were used to estimate the incident rate ratio by suicidal behaviour status. We did this in three steps. Models in Step 1 were unadjusted while models in Steps 2 and 3 were adjusted for socio-demographics (age, marital status, income and highest level of education) and additionally adjusted for recent depressive symptoms, respectively.
Results
Sample characteristics
The characteristics of the 13,763 adult males in the study population are presented in Table 1. Approximately half (48.2%) of the sample were aged between 40 and 55 years (range, 18–55 years), almost two-thirds were currently married (65.3%), 61.9% earned at least AUD$80,000/year (2013$) and the majority had completed qualifications above high-school level (75.2%). More than 1 in 10 participants (12.5%) had at least moderate depressive symptoms, 1 in 10 (9.7%) reported suicidal ideation in the preceding 2 weeks and 5.6% had attempted suicide in their lifetime.
Participant characteristics (n = 13,763).
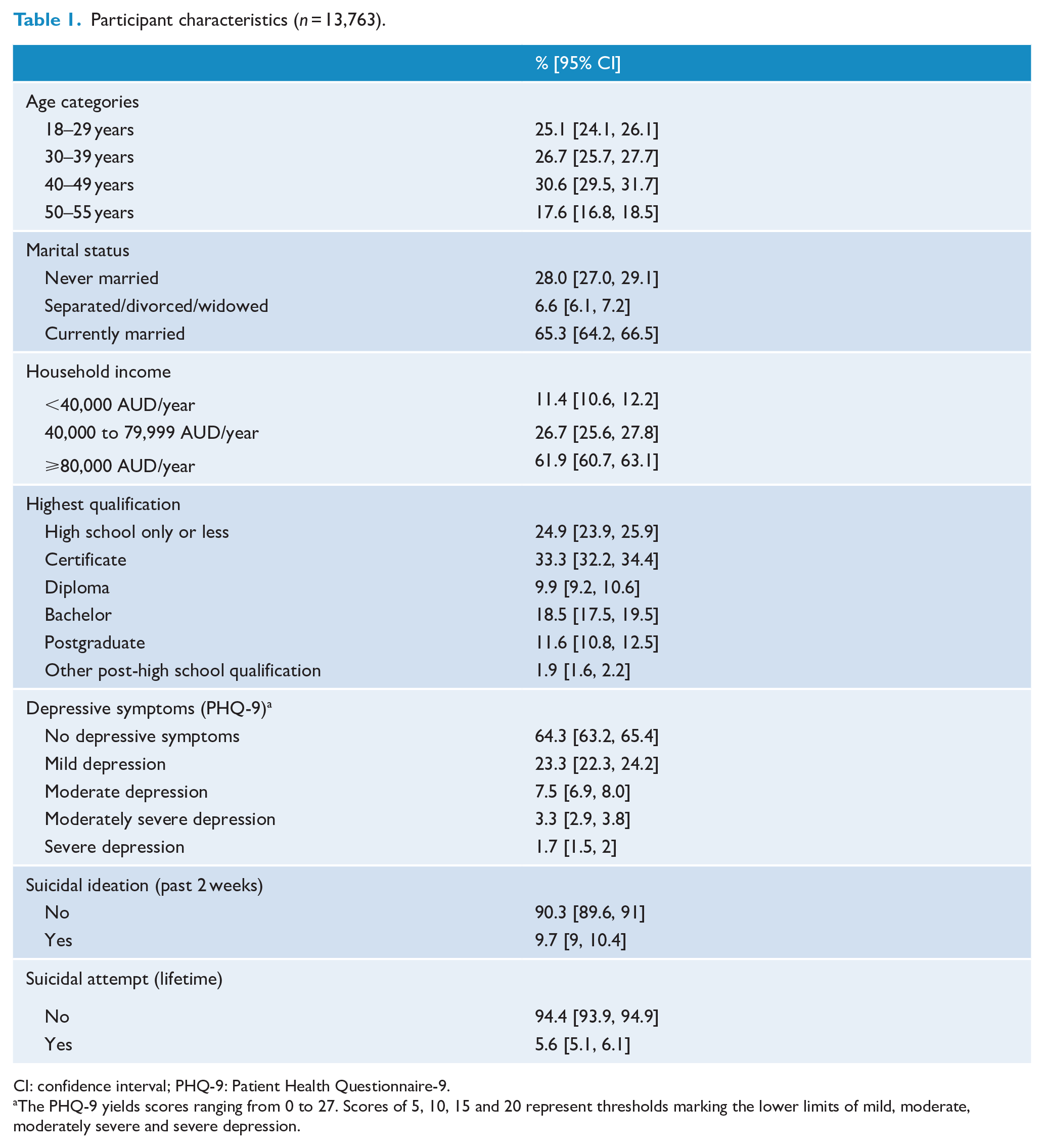
CI: confidence interval; PHQ-9: Patient Health Questionnaire-9.
The PHQ-9 yields scores ranging from 0 to 27. Scores of 5, 10, 15 and 20 represent thresholds marking the lower limits of mild, moderate, moderately severe and severe depression.
Prevalence of HSRBs, by suicidal behaviour status
The prevalence of all HSRBs among people experiencing recent suicidal ideation and those with a history of suicide attempts is displayed in Table 2.
Prevalence of health and social risk behaviours, by suicidal behaviour status (n = 13,763).
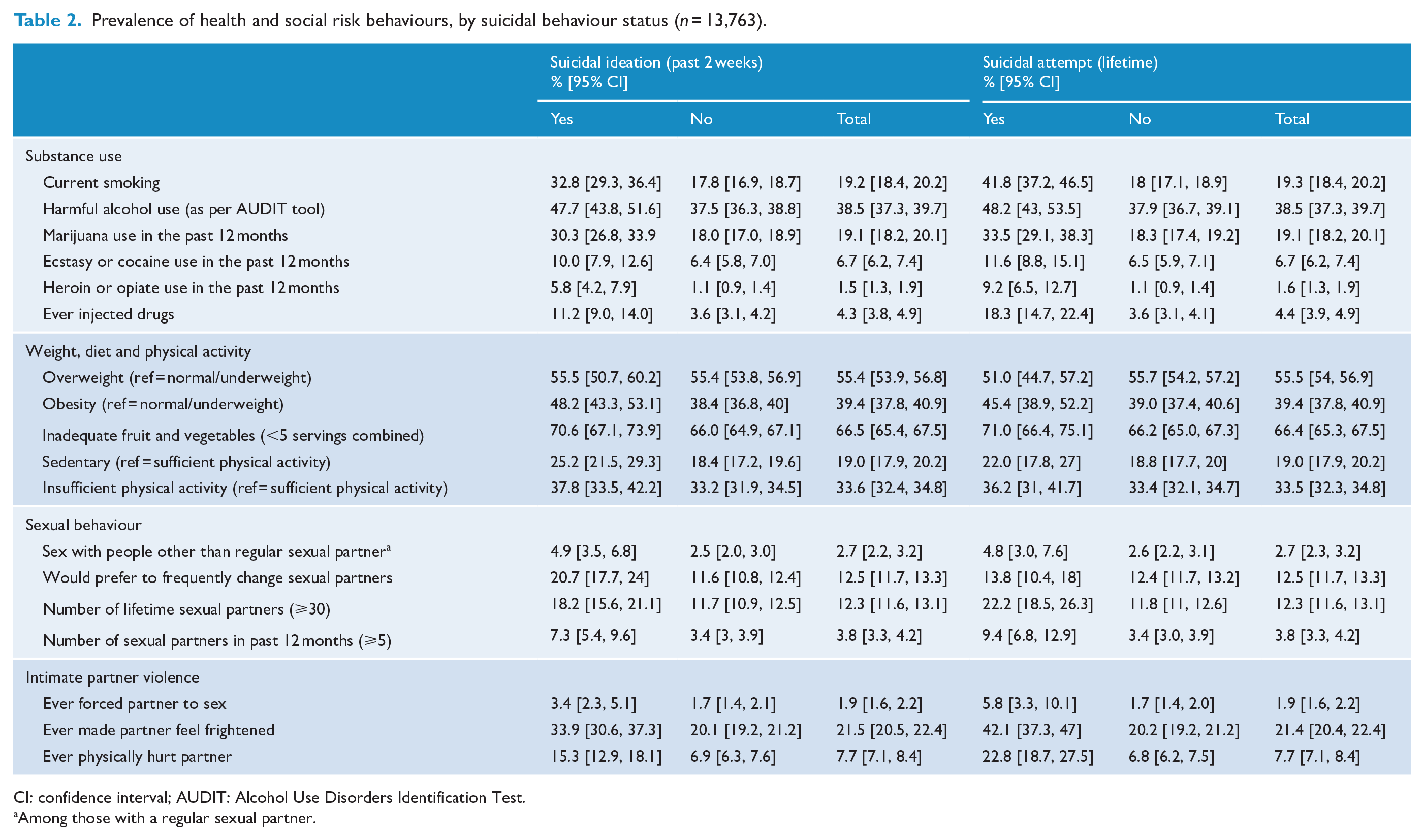
CI: confidence interval; AUDIT: Alcohol Use Disorders Identification Test.
Among those with a regular sexual partner.
Associations between HSRBs and suicidal ideation
In Step 1, participants with recent suicidal ideation had a higher risk of engaging in risk behaviours across all domains (RR range, 1.10–5.25), and these associations remained significant after adjusting for socio-demographic variables in Step 2 (Table 3). In Step 3, after adjustment for recent depressive symptoms, there was evidence that those with recent suicidal ideation still had a higher risk of engaging in ecstasy and/or cocaine use (RR = 1.27, borderline p-value 0.051), heroin or opiate use (RR = 1.89), injecting drug use (RR = 1.70), a higher number of lifetime (Incident rate ratio (IRR) = 1.18) and recent sexual partners (IRR = 1.74), a preference for sex with people other than their regular sexual partner (RR = 1.49), a preference for frequently changing sexual partners (RR = 1.34), and all intimate partner violence behaviours (RR range, 1.26–1.42) except a history of having forced a partner to have sex (p = 0.130; perhaps under-powered by the relatively small sub-sample of men who reported such a history, n = 233). After adjusting for both socio-demographic factors and recent depressive symptoms, there was no evidence that recent suicidal ideation was associated with smoking (p = 0.069), harmful alcohol use (p = 0.127), marijuana use (p = 0.177), nor any of the variables in the weight, diet and physical activity category (all p < 0.05).
The relative risk of engaging in health and social risk behaviours among people with recent (past 2 weeks) suicidal ideation (n = 13,763).
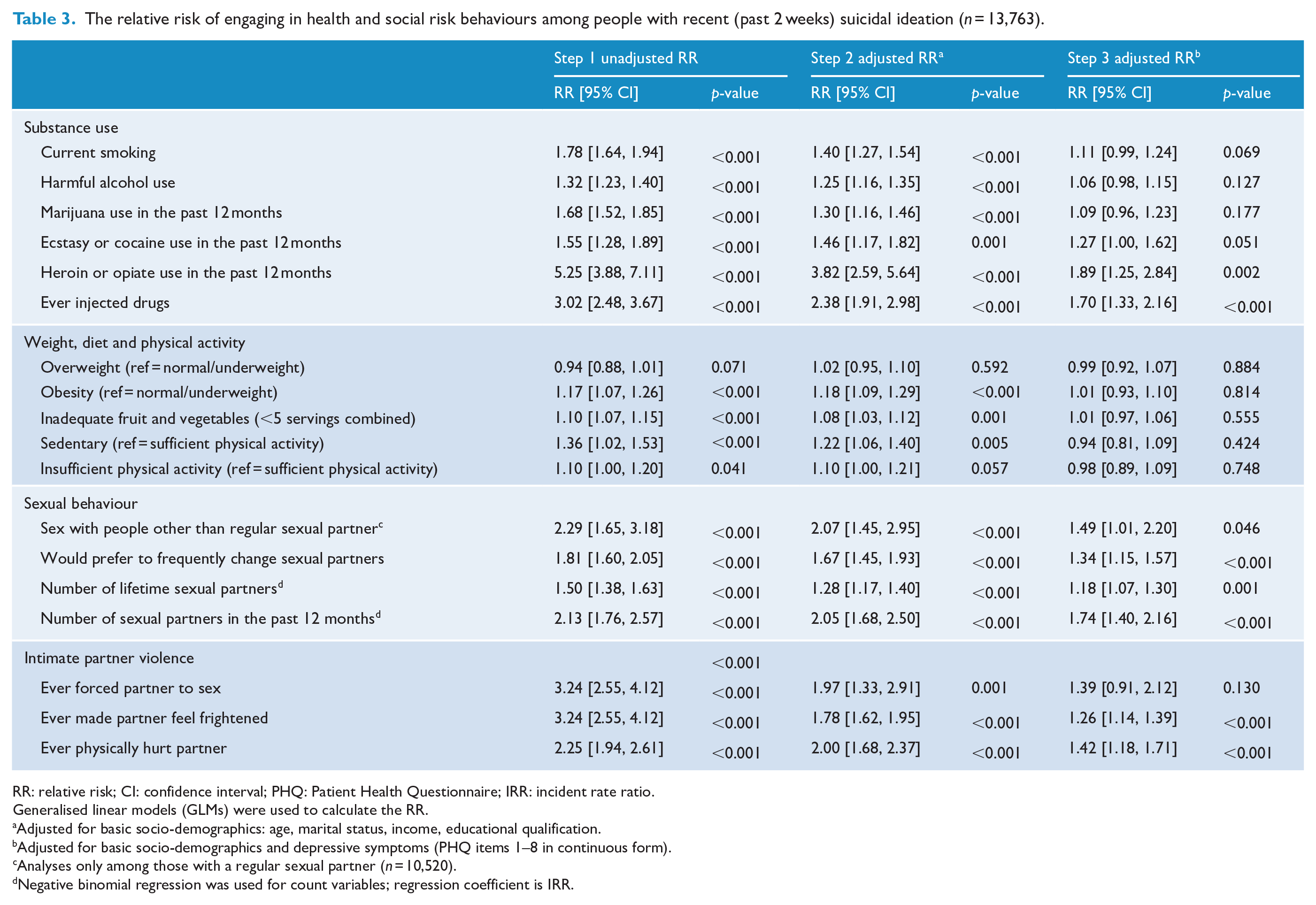
RR: relative risk; CI: confidence interval; PHQ: Patient Health Questionnaire; IRR: incident rate ratio.
Generalised linear models (GLMs) were used to calculate the RR.
Adjusted for basic socio-demographics: age, marital status, income, educational qualification.
Adjusted for basic socio-demographics and depressive symptoms (PHQ items 1–8 in continuous form).
Analyses only among those with a regular sexual partner (n = 10,520).
Negative binomial regression was used for count variables; regression coefficient is IRR.
Associations between HSRBs and suicidal attempt
In Step 1, participants with a lifetime history of suicide attempt had a higher risk of engaging in almost all risk behaviours across all domains (RR range, 1.10–7.65), aside from an intention to frequently change sexual partners (p = 0.119) (Table 3). In Step 2, most associations remained after adjusting for core socio-demographic variables, except for inadequate fruit and vegetable intake and sedentary/insufficient physical activity, which did not remain significant (all p < 0.05) (Table 4). In Step 3, after also adjusting for depressive symptoms, those with a history of suicide attempt still had a higher risk of engaging in all substance use behaviours (RR, 1.11–3.18), a higher number of lifetime (IRR = 1.87) and recent sexual partners (IRR = 1.77), and all intimate partner violence variables (RR range, 1.68–2.27). However, after adjusting for socio-demographic factors and depressive symptoms, suicide attempt was no longer associated with a preference for sex with people other than their regular sexual partner, a preference for frequently changing sexual partners, nor any of the variables in the weight, diet and physical activity category (all p < 0.05).
The relative risk of engaging in health and social risk behaviours among people with a history of suicide attempt (n = 13,763).
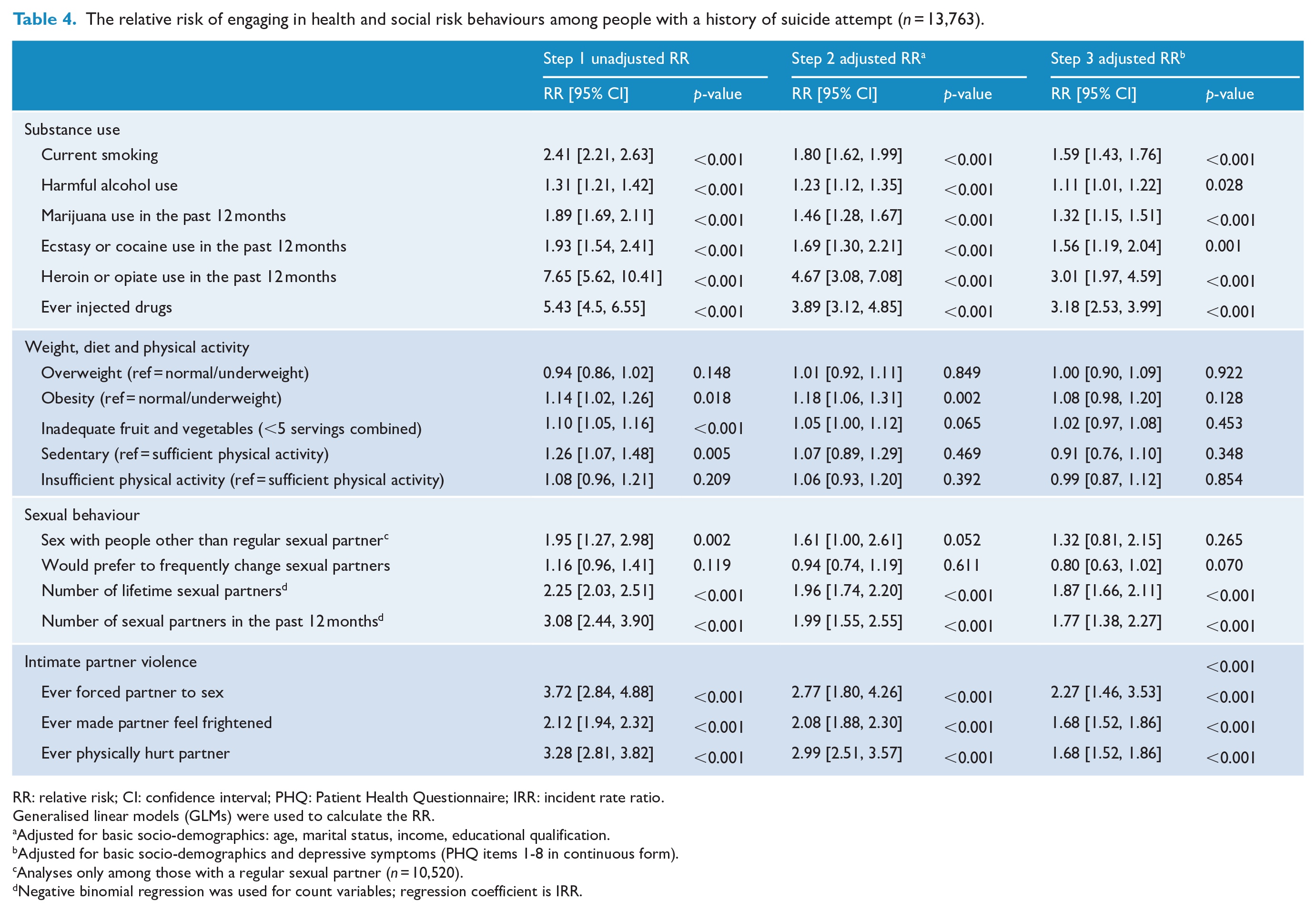
RR: relative risk; CI: confidence interval; PHQ: Patient Health Questionnaire; IRR: incident rate ratio.
Generalised linear models (GLMs) were used to calculate the RR.
Adjusted for basic socio-demographics: age, marital status, income, educational qualification.
Adjusted for basic socio-demographics and depressive symptoms (PHQ items 1-8 in continuous form).
Analyses only among those with a regular sexual partner (n = 10,520).
Negative binomial regression was used for count variables; regression coefficient is IRR.
Discussion
In cross-sectional analyses, we observed a significantly and substantially higher prevalence of HSRBs among men experiencing recent suicidal ideation or a history of attempting suicide. The associations between STB and HSRBs were typically independent of socio-demographics and in many cases were also independent of depressive symptoms.
This provides further evidence to explain the increased risk of morbidity and premature mortality from adverse health behaviours for people exhibiting suicidal behaviour (Bergen et al., 2012; Hawton et al., 2006; Neeleman, 2001). These behaviours carry social and legal risks, including risks to others, though some may potentially be modifiable. This phenomenon has important implications for the assessment and management of suicidality in both clinical and community settings. Naturally, when a patient, client, friend or family member expresses suicidal ideation, our immediate and justifiable response is to narrow our focus to preventing suicide, including a thorough clinical assessment and treatment of distressed or poor mental state. This is essential and we are ever seeking to improve the effectiveness of our clinical and community-based responses to suicidality.
Yet, the majority of people who experience suicidal thoughts and attempts do not die by suicide (Bostwick et al., 2016; Pirkis et al., 2000; ten Have et al., 2009), and the experience of suicidality may be an important catalyst for a broader psychosocial conversation about the associated health and social impacts beyond the risk of suicide. Our findings suggest that HSRBs may be a key opportunity for prevention and also need to be assessed and addressed. While these behaviours may not imminently result in premature deaths, such as suicides, they often carry profound lifelong health and social consequences if left unaddressed. In some circumstances, these behaviours may result in drug-related fatalities or harm to others.
Thus, our findings provide evidence for a twofold approach. First, it is imperative to undertake holistic and comprehensive physical health, behavioural and social assessments of people reporting suicidality; effective care requires an integration of common risk public health interventions with clinical and community-based suicide prevention (Caine, 2013). While narrow clinical risk assessment scales have been observed to have limited predictive value for identifying suicides (Quinlivan et al., 2017), there may however be considerable value in holistic psychosocial assessments for people reporting suicidality to assess overlapping HSRBs that may cause harm to themselves and others. This would also align well with moves to highlight the importance of physical health as an outcome for people experiencing mental illness/distress (World Health Organization, 2018). Second, persons exhibiting significant HSRBs should be assessed for serious mental health concerns and suicidality (Rice et al., 2013). Moreover, understanding that STB can be evanescent, or may not yet have occurred, proactive preventive interventions are warranted for persons with HSRBs – given their association with all-cause premature mortality, even as preventing suicide is a central concern.
In our analyses, suicidality was linked to externalising and aggressive behaviours (i.e. illicit drug use, number of sexual partners and preferences for multiple sexual partners, and intimate partner violence), independently of socio-demographics and other depressive symptoms. Meanwhile, we generated evidence that depressive symptoms attenuated the association between more internalising behaviours such as more socially acceptable forms of substance use (i.e. smoking tobacco and alcohol use), obesity, inadequate fruit and vegetable intake and sedentary behaviour. Such findings are consistent with research in clinical and community samples that has observed a link between suicidality and externalising behaviours (e.g. excessive substance use, aggression and poor impulse control, risk-taking) and that this relationship is independent of internalising depressive symptoms (Rice et al., 2015, 2019; Verona et al., 2004). Therefore, our findings lend more support to the hypothesis that suicidality is associated with externalising behaviours, whereby people’s inability to tolerate or communicate distress results in the avoidance of distress through anger and aggressive behaviour, impulsiveness, risk-taking, substance use or other maladaptive behaviours (Rice et al., 2013, 2019).
Prior research has indicated that while suicidality is associated with externalising behaviours in both males and females, externalising behaviours are more likely to be present in suicidal males (Brownhill et al., 2005; Oliffe et al., 2012; Verona et al., 2004), and screening for maladaptive externalising symptoms may be important for assessing suicide risk in males, rather than relying solely on measures consistent with gender neutral psychiatric diagnostic criteria (Rice et al., 2019). Consequently, Rice et al. (2013) developed the Male Depression Risk Scale (MDRS-22), measuring emotional suppression, drug use, alcohol use, anger and aggression, somatic symptoms and risk-taking. They have observed that scores on the scale are correlated with higher suicide risk in general populations of males, even after adjusting for internalising depressive symptoms and basic socio-demographics (Rice et al., 2019). Our findings support the use of such scales in the assessment of suicide risk, as there is a compelling argument for the inclusion of externalising symptoms in the clinical assessment of men experiencing suicidality. However, our findings indicate that addressing these HSRBs is important not just because they predict suicide risk but because suicidality may also predict engagement in behaviours that carry profound health and social consequences. Many males who have adverse health behaviours will not die by suicide, but many will die prematurely from HSRB-related medical disorders.
Moreover, it is worth taking note of the role of masculinity norms as an important context to our findings and their implications. Genuchi (2019) contends that men’s expressions of externalising symptoms are influenced by their alignment to dominant masculine norms, and Pirkis et al. (2017) have documented associations between some masculine norms (specifically, self-reliance) and an increased risk of suicidal thinking. Future research is required to more deeply examine the value of implementing gender-sensitive psychosocial assessments that (1) better engage men and (2) integrate our emerging knowledge around the role of masculine norms in both suicidal thinking and men’s behavioural responses to psychological distress (Oliffe et al., 2019; Seidler et al., 2019).
We believe our study is one of the first to systematically examine the effects of suicidality on the risk of engaging in a broad suite of HSRBs in a general population of adult males, independent of socio-demographics and other depressive symptoms. Nonetheless, our study has some limitations. First, as with all cross-sectional study designs, the causal nature of relationships cannot be determined. There is a temporal limitation, in that we are unsure what occurred first; the suicidality or the engagement in HSRBs, or indeed whether they co-occurred. Reverse causality cannot be ruled out, yet for the purposes of clinical practice with people who are suicidal, we contend that the association indicates the need for broader health and social assessment and intervention irrespective of the causal direction. Furthermore, our analyses provide a foundation upon which to undertake future longitudinal analyses as additional waves of data are collected in this cohort.
Second, our paper is based on secondary analyses of data that was not collected for the purposes of our analyses. As such, there are a range of other HSRBs that would have been useful to collect such as condom use (an important aspect of sexual risk-taking behaviour), in addition to other relevant measures of personality traits (e.g. impulsivity, which may play a role in both suicidality and risky behaviours) and other psychiatric symptoms (e.g. anxiety symptoms). Third, our analyses were restricted to males and further research is needed to establish if suicidality is similarly associated with HSRBs among females. Fourth, data are based on self-report and may be impacted by social acceptability bias, particularly in relation to sensitive questions such as a history of forcing a partner to have sex. However, anonymity, privacy and confidentiality were assured, and we expect this will have assisted in eliciting accurate responses.
Conclusion
The experience of suicidality may be an important catalyst for a broader psychosocial conversation about the associated HSRBs and impacts beyond the risk of suicide. Our findings suggest that identification of suicidality may represent an opportunity for holistic assessment and psychosocial intervention with regard to a suite of potentially co-occurring HSRBs. While these behaviours may not imminently result in premature deaths, such as suicides, they often carry profound lifelong health and social consequences if left unaddressed.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The research on which this paper is based was conducted as part of the Australian Longitudinal Study on Male Health (Ten to Men) by G.A.. We are grateful to the Australian Government Department of Health for funding and to the boys and men who provided the survey data. Ten to Men is managed by the Australian Institute of Family Studies. Ten to Men research data is the intellectual property of the Commonwealth. Additionally, G.A. is funded by an Early Career Fellowship from the National Health and Medical Research Council (GNT1138096).