
Abstract
Objective:
To compare the prevalence of psychiatric conditions in a population-based cohort of people with intellectual disability and matched comparators in New South Wales, Australia.
Method:
The study cohort included 97,644 people with intellectual disability and 451,502 comparators aged ⩾ 5 between 1 July 2001 to 30 June 2018. We used linked records of hospital admissions, emergency department presentations, ambulatory mental health service contacts, and Medicare rebates to identify any, serious, and specific psychiatric conditions.
Results:
People with intellectual disability showed greatly elevated period prevalence of any psychiatric condition (76.0% vs 38.3%), serious mental illness (16.2% vs 5.1%), and all specific psychiatric conditions compared to comparators. Among people with intellectual disability and congenital/developmental conditions, people with Down syndrome showed reduced risk of most psychiatric conditions while people with attention-deficit hyperactivity disorder and people with learning disorders showed increased risk. Age-specific analysis showed earlier onset of dementia and heightened prevalence of self-injury/suicidality in adulthood among people with intellectual disability. Annualised prevalence trends showed increases in 2006–2007 for most psychiatric conditions and decreases in 2014–2015 to 2017–2018.
Conclusions:
The higher prevalence of psychiatric conditions in people with intellectual disability indicates the importance of systemic responses to address the mental health needs of this population. Our findings highlight the importance of considering the psychiatric profiles of specific congenital/developmental conditions among people with intellectual disability, and the need to provide targeted services to high-risk groups such as those with co-occurring attention-deficit hyperactivity disorder.
Background
People with intellectual disability represent approximately 1% of the population (Maulik et al., 2011). People with intellectual disability experience significantly worse health outcomes than people without intellectual disability (Emerson and Hatton, 2014), including high vulnerability to psychiatric conditions, with a recent first ever meta-analysis suggesting a prevalence of 33.6% (95% CI: 25.2–43.1%) (Mazza et al., 2020). The high risk of psychiatric conditions in this population is related to a range of medical, social and psychological factors. Some genetic causes of intellectual disability and higher rates of certain physical health conditions confer predisposition to psychiatric conditions (Abbeduto et al., 2019; Perera et al., 2020). However, people with intellectual disability also commonly experience trauma (McNally et al., 2021), stigma (Scior et al., 2020), loneliness and social isolation (Alexandra et al., 2018), lower socioeconomic status and impoverished living situations (Emerson and Parish, 2010), all of which contribute to poorer mental health.
Existing Australian and international research into the prevalence of psychiatric conditions in people with intellectual disability has produced widely varying estimates ranging from 7% to 97% (Buckles et al., 2013; Cooper et al., 2007; Einfeld et al., 2011; Morgan et al., 2008). Variation is likely due to differences in definition and identification of intellectual disability, definition and identification of psychiatric conditions, and sampling and data collection methods (Buckles et al., 2013; Mazza et al., 2020). The meta-analysis by Mazza et al. (2020) consisted mainly of small-scale projects focused on recipients of a specific health or disability service, and the few population-based studies were mostly limited to small geographic regions or showed under-ascertainment of intellectual disability. In addition, most existing studies do not include a comparison group, making relative risk comparisons problematic. Even fewer studies have examined prevalence of psychiatric conditions in people with intellectual disability and specific genetic syndromes or neurodevelopmental conditions, though the data available suggests these subgroups have unique needs that would benefit from tailored services (Rivelli et al., 2022; Underwood et al., 2012).
In addition to experiencing greater rates of psychiatric conditions, people with intellectual disability face a range of difficulties accessing mental health services (Whittle et al., 2018). Australian public mental health services (i.e. funded by the Australian government) can have long wait times or stringent eligibility criteria, while private services (i.e. funded by private health insurance and patient fees) usually charge out-of-pocket fees that make them less affordable to people with intellectual disability, who are less likely to have high incomes (Australian Institute of Health and Welfare, 2024). Once accessing services, difficulties in self-reporting their symptoms, along with complex clinical presentations and diagnostic overshadowing can complicate effective service delivery (Jamieson and Mason, 2019; Whittle et al., 2018). Overall, the risk factors, complexities, and cost of mental health services for this population warrants specific focus on psychiatric conditions in people with intellectual disability.
Reform in mental health services for people with intellectual disability requires a comprehensive picture of the population prevalence and presentation rates. These have not been accurately determined because people with intellectual disability are often excluded from health research (Bishop et al., 2024) and are not identifiable in routine health data sets. People with cognitive disability are an identified priority group of the National Mental Health and Suicide Prevention Agreement (Government of Australia, 2020), and are identified as experiencing disproportionate barriers to healthcare in the Royal Commission into Violence, Abuse, Neglect and Exploitation of People with Disability (2023). The Fifth National Mental Health and Suicide Prevention Plan also recognised people with intellectual disability as a vulnerable group experiencing multiple mental health disadvantages (National Mental Health Commission, 2017). Addressing the gap between policy aspiration and knowledge is crucial in view of Article 31 of the United Nations Convention for the Rights of Persons with Disabilities, which states an obligation to ‘collect appropriate information, including statistical and research data, to enable them to formulate and implement policies to give effect to the present Convention’ (United Nations, 2006).
We have access to a comprehensive linked data set encompassing multiple health and disability service data sources. This resource facilitates extensive identification of people with intellectual disability in New South Wales, Australia, along with a matched comparator cohort without recorded diagnosis of intellectual disability (Reppermund et al., 2024). This data set enables an investigation into representative prevalence estimates of psychiatric conditions across a range of service settings. The inclusion of a comparator group also gives a clearer view of additional mental health disadvantages faced by people with intellectual disability. Our study aimed to (1) compare the period prevalence of any psychiatric condition, serious mental illness, and specific psychiatric conditions from July 2001 to June 2018, stratified by sex and specific congenital or developmental conditions; (2) compare age-specific prevalence of psychiatric conditions; and (3) examine annual time trends in age-standardised annualised prevalence across both cohorts.
Methods
Study population
The linked data set was comprised of 20 individual administrative data sets from health, disability, and other services, with nine data sets used for cohort identification. The cohort of people with intellectual disability includeds all people who received disability services in NSW where intellectual disability is a primary or a secondary disability, or have a recorded diagnosis of intellectual disability in health service data sets, as described by Reppermund et al. (2024). The comparator cohort consists of people without recorded intellectual disability from the Medicare Consumer Directory matched on 5-year age, sex and area of residence in a ratio of 5:1. Our study sample included all individuals aged ⩾ 5 years during the study period from both cohorts.
The sample was stratified by sex and selected congenital/developmental diagnoses, as these variables have been known to influence prevalence of psychiatric conditions. See Supplementary Material S1 for definitions and methods of ascertainment.
Data sets and record linkage
De-identified linkage was performed by the NSW Centre for Health Record Linkage (CHeReL) and Australian Institute of Health and Welfare (AIHW), as described by Reppermund et al. (2024). We then accessed data through the Secure Unified Research Environment (SURE). See Table 1 for descriptions of data sets we used to ascertain psychiatric and congenital/developmental diagnoses.
Data sets for outcome ascertainment.
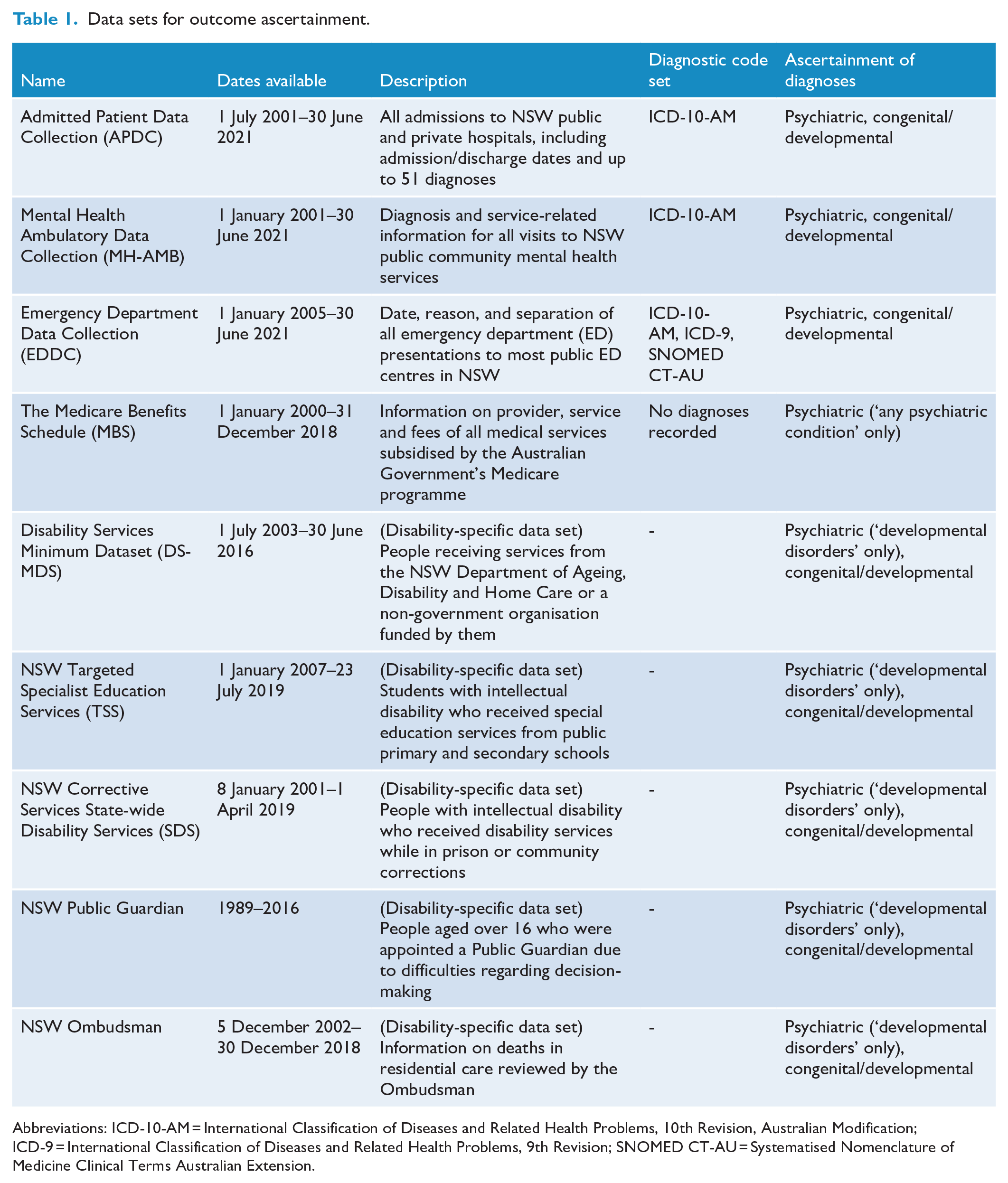
Abbreviations: ICD-10-AM = International Classification of Diseases and Related Health Problems, 10th Revision, Australian Modification; ICD-9 = International Classification of Diseases and Related Health Problems, 9th Revision; SNOMED CT-AU = Systematised Nomenclature of Medicine Clinical Terms Australian Extension.
We used date of death information from the NSW Registry of Births, Deaths and Marriages (RBDM) and AIHW National Dath Index (NDI) data sets to determine end of follow-up.
We set the study period as 1 July 2001 to 30 June 2018 to account for differences in reference period between data sets and to align with Australian financial years for comparison with government data. Follow-up for each individual began on 1 July 2001 or their fifth birthday, whichever was later, and ended on 30 June 2018 or date of death, whichever was earlier.
Variables of interest
Supplementary Material S1 contains detailed information on ascertainment of variables of interest. Any psychiatric condition was defined as at least one of the following:
Record of an eligible ICD-10 psychiatric diagnosis or ICD-9 equivalent in the Admitted Patient Data Collection (APDC) or Emergency Department Data Collection (EDDC), or
APDC record of admission to a non-emergency department psychiatric unit with any diagnosis, or
Service receipt in the Mental Health Ambulatory Data Collection (MHAMB) with any diagnosis, or
Receipt of a Medicare Benefits Schedule (MBS) service suggesting a diagnosable psychiatric condition, or
Record of a developmental disorder other than intellectual disability from disability-specific data sets (see Table 1).
Systematised Nomenclature of Medicine Clinical Terms Australian Extension (SNOMED CT-AU) codes were converted to International Classification of Diseases and Related Health Problems, 10th Revision (ICD-10-AM) using SnoMAP Starter (Lawley et al., 2017) and Snapper (Australian e-Health Research Centre, n.d.).
There are multiple approaches to defining serious mental illness (SMI) in the literature (Gonzales et al., 2022). Our approach uses a combination of diagnostic categories and service use intensity to capture the subpopulation most likely to have high service needs:
APDC hospital admission where the principal diagnosis recorded was an eligible psychiatric diagnosis (defined as above), or
MHAMB episode with a psychosis-related diagnosis (F20, F23, F25, F30, F31, F32.3, F33.3), or
APDC admission to a non-emergency department psychiatric unit with any diagnosis.
Specific psychiatric conditions included mood/affective disorders, anxiety disorders, substance use disorders, psychotic disorders, intentional self-injury/suicidality, dementia, non-dementia organic psychiatric disorders, personality disorders, and developmental disorders.
Statistical analysis
We used Stata 18 for all statistical analyses. Demographic characteristics included age, sex, remoteness, and Area-Based Index of Relative Socioeconomic Disadvantage (IRSD). We were unable to include information on ethnocultural background due to inconsistent collection across data sets, and omitted reporting of Aboriginal and Torres Strait Islander status due to ethical constraints. We calculated period prevalence as the number of people in a given group who experienced the variable of interest at any time during the study period, divided by the total number of people in that group (Vaughan et al., 2021). We calculated period prevalence stratified by sex in people with intellectual disability and comparator cohorts, and by congenital/developmental conditions in people with intellectual disability only. To calculate age-specific prevalence in people with intellectual disability and the comparator cohort, we split individuals’ age at the end of each financial year into 5-year age bands. The denominator was the total number of individuals in the specified age band summed across all financial years. The numerator was the total number of individuals in each financial year who experienced the variable of interest while in the specified age band, summed across all financial years.
We calculated annualised prevalence for both cohorts using the number of people who experienced the variable of interest in a given financial year as the numerator, and the total number of people in that financial year as the denominator (Vaughan et al., 2021). We assigned psychiatric episodes to a financial year according to the date of service or episode start date. Episodes with start and end dates spanning more than one financial year were included in annualised prevalence of both years. Developmental conditions ascertained from disability-specific data sets were not counted in annualised prevalence as no date information was available. We then employed direct standardisation using the Australian standard population in 2001, as recommended by the Australian Bureau of Statistics (ABS, 2013), to compare annualised prevalence time trends in people with intellectual disability and the comparator cohort while controlling for differences in life expectancy.
Results
From the original cohort of 100,089 people with intellectual disability and 455,677 comparators, we excluded 2445 people with intellectual disability and 4174 comparators who died before the start of follow-up or reached age 5 after the end of follow-up, resulting in 97,644 eligible people with intellectual disability and 451,502 comparators. Total follow-up duration was 1,177,095.07 years in people with intellectual disability (M = 12.05, SD = 5.23), and 5,603,839.25 years in comparators (M = 12.41, SD = 5.25). As expected from the matching process, there are minimal demographic differences between the two cohorts (see Table 2).
Sample demographics.
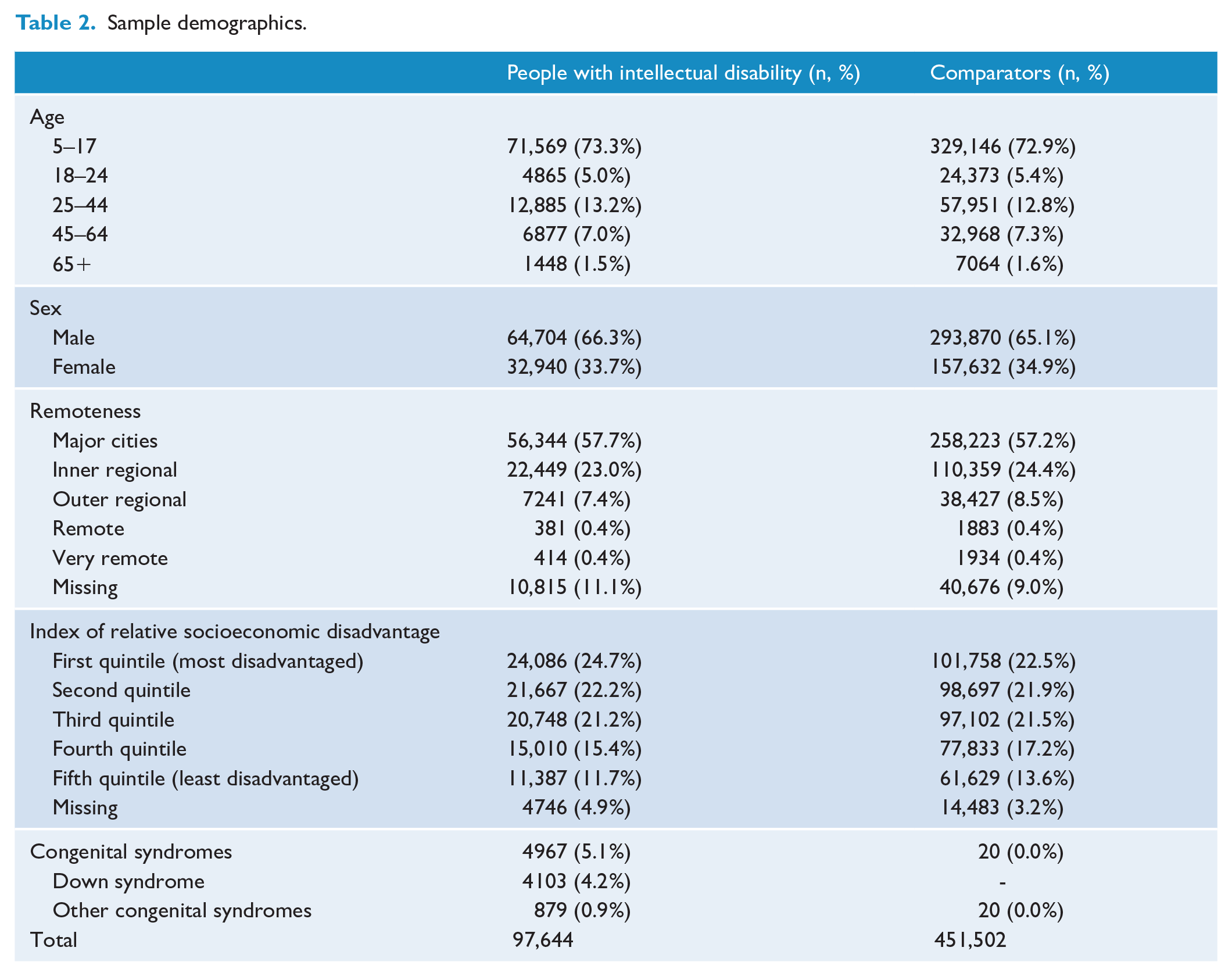
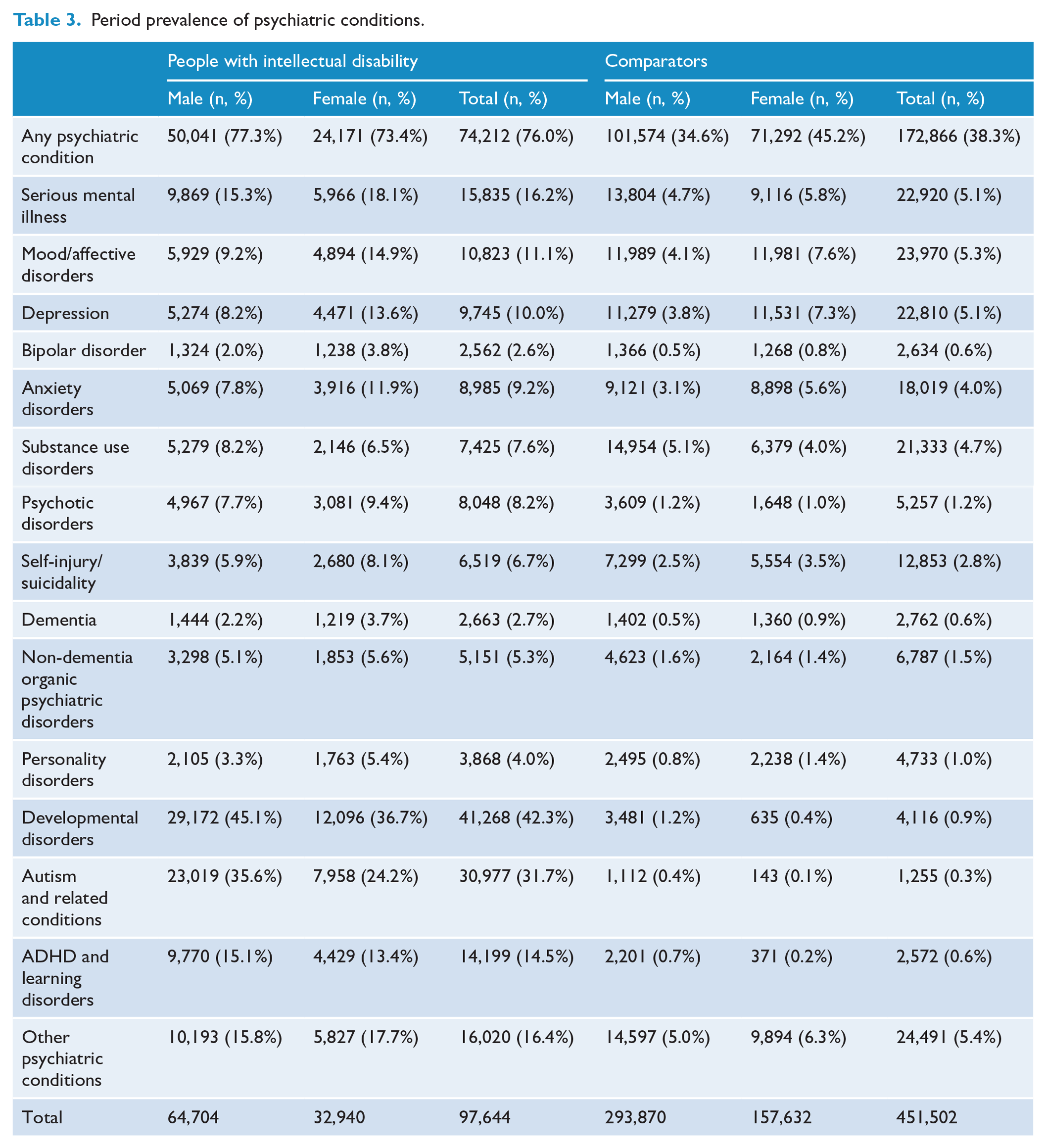
Table 3 shows an approximately twofold prevalence of any psychiatric condition (76.0%) and approximately threefold prevalence of SMI (16.2%) among people with intellectual disability during the study period compared with matched comparators (38.3% and 5.1% respectively). The prevalence of most specific psychiatric conditions in people with intellectual disability were two to three times as high as in the comparators. In addition, the prevalence of psychotic disorders (8.2% vs 1.2%), dementia (2.7% vs 0.6%), and developmental disorders (42.3% vs 0.9%) were greatly elevated. Males had higher prevalence of any psychiatric condition than females in people with intellectual disability (77.3% vs 73.4%), but this sex difference was reversed in comparators (34.6% vs 45.2%). Sex differences in SMI and specific psychiatric conditions were mostly mirrored in people with intellectual disability and comparators, though the higher prevalence of developmental disorders in males was less pronounced in people with intellectual disability (45.1% vs 36.7%) than in comparators (1.2% vs 0.4%).
Period prevalence of psychiatric conditions.
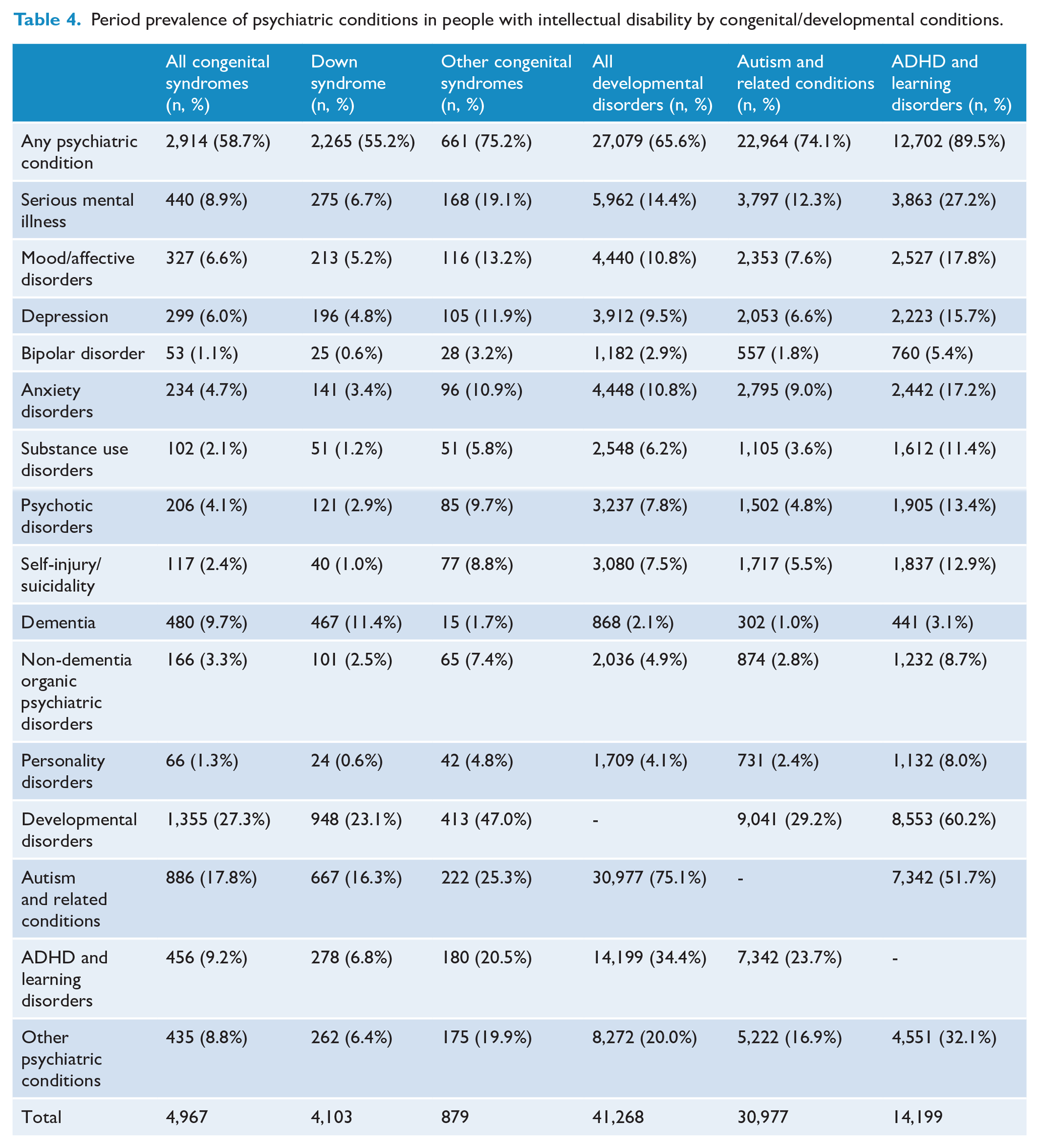
Among people with intellectual disability and specific congenital/neurodevelopmental conditions (Table 4), people with Down syndrome had substantially reduced period prevalence of most psychiatric conditions compared to all people with intellectual disability (see Table 3) and people with other congenital syndromes, except greatly increased prevalence of dementia (11.4% vs 2.7% vs 1.7%). Notably, prevalence of depression, anxiety, and substance use were lower in people with Down syndrome than the comparator cohort in Table 3. Among people with intellectual disability, the subgroup of people with attention-deficit hyperactivity disorder (ADHD) and learning disorders showed substantially increased period prevalence of most psychiatric conditions, most notably SMI (27.2% vs 16.2%), self-injury/suicidality (12.9% vs 6.7%), anxiety disorders (17.2% vs 9.2%), mood/affective disorders (17.8% vs 11.1%), other developmental disorders (60.2% vs 42.3%), and other psychiatric conditions (32.1% vs 16.4%). In contrast, the subgroup of people with autism and related conditions showed slightly reduced period prevalence of most psychiatric conditions compared to all people with intellectual disability, particularly substance use disorders (3.6% vs 7.6%).
Period prevalence of psychiatric conditions in people with intellectual disability by congenital/developmental conditions.
Age trends in psychiatric conditions were mostly similar in people with intellectual disability and comparators, though the earlier onset of dementias was clearly evident (Figure 1, see Supplementary Material S2 for data). There was a peak in any psychiatric condition, SMI, and mood/affective disorders at ages 75+ in the comparator cohort only. Self-injury/suicidality showed peak prevalence at age 30–34 in people with intellectual disability versus age 15–19 in comparators.
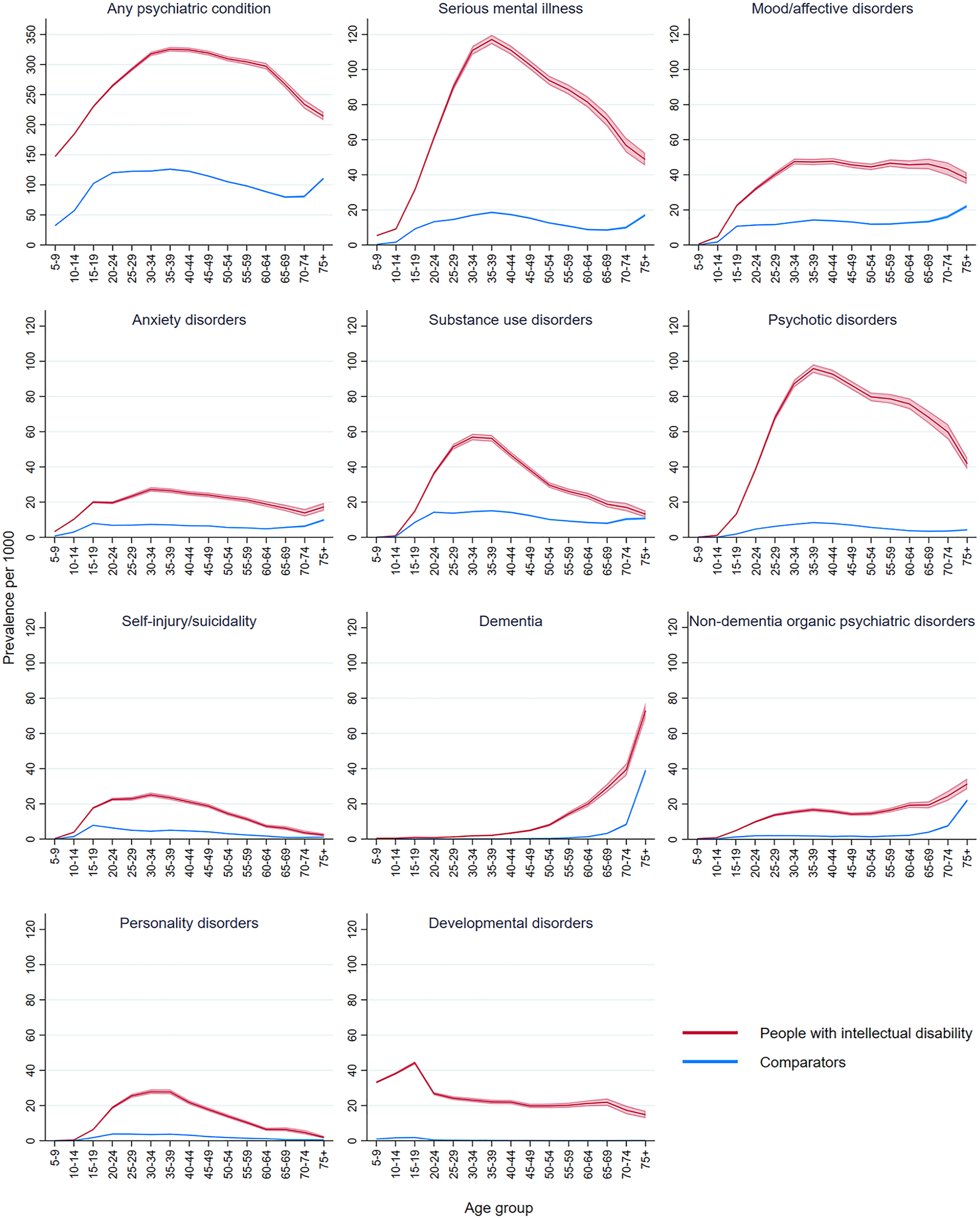
Age group period prevalence of psychiatric conditions by intellectual disability status.
Any, serious, and specific psychiatric conditions all showed consistently higher annualised prevalence in people with intellectual disability than comparators. There was a general upwards trend in annualised prevalence of any psychiatric condition in both cohorts (Figure 2, see Supplementary Material S3 for data). This trend mirrored MBS case ascertainment, rather than ascertainment from other sources (see Supplementary Material S4). Several conditions showed peaks around 2005 and 2007, gradual declines from 2013 and drops in 2017, along with a sudden increase in mood/affective disorders prevalence in 2015–2016.
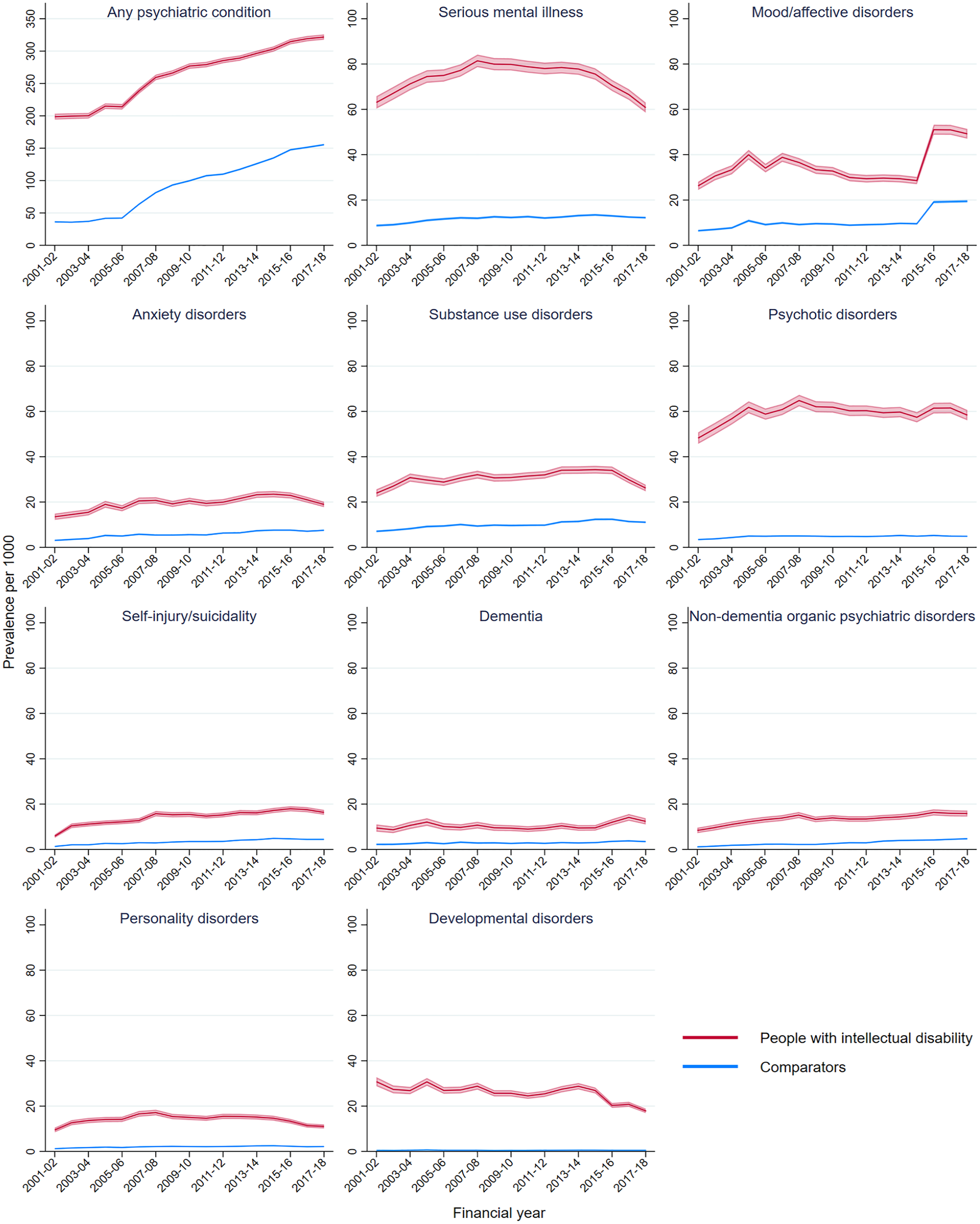
Annualised age-standardised prevalence of psychiatric conditions by intellectual disability status.
Discussion
The data source for this study had a high proportion of population capture of people with intellectual disability living in NSW and is one of the largest cohorts of people with intellectual disability internationally (Reppermund et al., 2024). Our results showed an approximately twofold prevalence of any psychiatric condition and threefold prevalence of SMI in people with intellectual disability compared to matched comparators, consistent with existing literature (Buckles et al., 2013; Mazza et al., 2020). All specific psychiatric conditions showed elevated prevalence in people with intellectual disability, with greatly elevated prevalence of psychotic disorders and dementias. Annual prevalence trends showed drop-offs in the prevalence of several conditions after 2015. Among people with intellectual disability, individuals with Down syndrome have slightly reduced rates of most psychiatric conditions compared to all people with intellectual disability, except for significantly increased rates and earlier onset of dementia. However, individuals with Down syndrome still have higher rates of most psychiatric conditions than the comparator cohort. Among people with intellectual disability, individuals with ADHD or learning disorders showed increased rates of psychiatric conditions compared to the whole cohort.
Our data on age-standardised annualised prevalence showed minor peaks in the prevalence of several conditions around 2005 and 2007, and noticeable decreases towards the end of the study period. There was also a sharp increase in mood/affective disorders prevalence in 2015–2016. These trends are most likely due to the nature of linked administrative data and structural changes in Australian health and disability services, rather than fluctuations in true underlying prevalence. The peaks around 2005 and 2007 align with commencement of the EDDC data set in 2005 and introduction of the Better Access initiative in 2006–2007. The Better Access initiative introduced a large number of Medicare rebates for mental health services (Jorm, 2018), contributing to increased identification and treatment of psychiatric conditions and improved ascertainment in the MBS and other health data sets. Regarding reduced prevalence of specific psychiatric conditions in more recent years, our secondary analysis showed this was likely due to decreases in case ascertainment from the MHAMB data set and increased ascertainment from MBS where specific diagnoses could not be determined (Supplementary Material S4). As the APDC records each episode at discharge, individuals who had not yet been discharged at the end of the study period may also have contributed to lowered prevalence in 2017–2018. Greater reductions among people with intellectual disability may be attributable to the rollout of the National Disability Insurance Scheme (NDIS) in NSW beginning in 2013, which provided individual funding for people with disability to access a range of services from private providers (National Disability Insurance Agency, 2023), thus reducing reliance on hospitals and public ambulatory mental health services. Although definitive interpretations are not possible, the reduction in hospital admissions and public ambulatory mental health service use is in line with the positive outcomes reported in the NDIS evaluation report (Mavromaras et al., 2018). More comprehensive identification of people with intellectual disability in future collection of administrative data is needed to evaluate the effectiveness and impacts of policy initiatives on this population group. The increase in mood/affective disorder prevalence in 2015–2016 is likely attributable to the introduction of supplementary codes for chronic conditions including depression in the ICD-10-AM 9th Edition (Independent Health and Aged Care Pricing Authority, 2015), thus increasing the number of records with depression coded in the APDC data set (Australian Institute of Health and Welfare, 2023).
Importantly, our data also identified substantial differences in psychiatric condition prevalence in subpopulations of people with intellectual disability and specific congenital syndromes and/or developmental disorders. Notably, our study identified 4103 individuals with Down syndrome, or 0.05% of the NSW population in 2018. This is comparable with global prevalence estimates of 3.3–6.7 per 10,000 individuals (Antonarakis et al., 2020). Reduced rates of most psychiatric conditions in the subgroup of people with Down syndrome compared to the whole cohort of people with intellectual disability is consistent with past epidemiological studies of adults with Down syndrome (Mantry et al., 2008; Tassé et al., 2016). Our finding of greatly increased rates of dementia in people with Down syndrome is also consistent with research suggesting specific genetic risks (Ballard et al., 2016), yet we note substantially higher rates of dementia were also apparent for the whole intellectual disability cohort.
In contrast, the subgroup of people with intellectual disability and co-occurring ADHD or learning disorders (15.1% of the cohort of people with intellectual disability) showed the highest risk of co-occurring psychiatric conditions, with SMI occurring in more than a quarter of this group. As specific learning disorder diagnoses are typically given only to people with average intellectual functioning or above (Australian Disability Clearinghouse on Education and Training, n.d.), it can be assumed that most individuals with intellectual disability in the subgroup of people with ADHD or learning disorders are diagnosed with ADHD. Inattentive and hyperactive symptoms in people with intellectual disability have historically been attributed to intellectual disability itself rather than ADHD (Antshel et al., 2006; Neece et al., 2013), which contributed to a lack of research into the mental health needs of this subgroup. Existing research into the mental health of people with ADHD have consistently shown increased prevalence of mood, anxiety, substance abuse, and personality disorders (Choi et al., 2022). As one of the first studies examining the overlap of ADHD, intellectual disability, and mental health, our findings suggest the co-occurrence of ADHD and intellectual disability may further increase individuals’ vulnerability to psychiatric conditions. More accurate and comprehensive identification of ADHD and co-occurring psychiatric conditions in people with intellectual disability is needed to fully understand the mental health needs of this subgroup.
The subgroup of people with intellectual disability on the autism spectrum showed similar prevalence of any psychiatric condition to the whole cohort of people with intellectual disability. It is difficult to compare this with past research as few studies examined the relationship between autism and mental health in people with intellectual disability, with inconsistent findings (Cervantes and Matson, 2015; Dunn et al., 2020; McCarthy et al., 2010; Melville et al., 2008). In addition, we found notable differences in the prevalence of specific psychiatric conditions. Our finding of reduced mood/affective and psychotic disorder prevalence in the autism subgroup contradicts past research, which found that this group had higher risk of these disorders than people with intellectual disability only (Bakken et al., 2010; Cervantes and Matson, 2015; Peña-Salazar et al., 2022). This may be due to diagnostic overshadowing and challenges in differential diagnosis of autism and other psychiatric conditions with the added complexity of intellectual disability (Lai et al., 2019), which may be exacerbated when behaviours of concern are present (McCarthy et al., 2010). Our findings regarding reduced prevalence of dementia in the autism subgroup are consistent with a study of American adults aged 30–64 (Vivanti et al., 2021). Our finding of reduced substance use disorder prevalence in this subgroup is consistent with two systematic reviews, which suggested that core difficulties in social interaction may prevent people on the autism spectrum from accessing recreational drugs (Arnevik and Helverschou, 2016; Lugo-Marín et al., 2019). Overall, our findings are of particular importance to clinicians in understanding nuances in supporting the mental health of people with intellectual disability and specific congenital or neurodevelopmental conditions.
Our findings identify people with intellectual disability as an ultra-high-risk group for mental illness and stratify this risk using additional characteristics. As such the results can be used to shape system-wide reform to address the need and level of complexity of this population group. Coupled with the recent Australian Royal Commission into Violence, Abuse, Neglect and Exploitation of People with Disability (DRC; 2020) which found that ‘people with cognitive disability have been and continue to be subject to systemic neglect in the Australian health system’ (p. 140), our findings should shape responses of clinicians, services and policy makers to ensure that the mental health needs of people with intellectual disability are prioritised and proactively addressed by public and private mental health services. This entails investment in both dedicated clinician capacity within mainstream as well as highly specialised services for those with more complex needs. We have previously identified that people with intellectual disability in NSW, despite being 1%–2% of the population, make up 6% of public mental health service users and 12% of the mental health budget spend (Srasuebkul et al., 2021), though these findings did not include MBS related costs. Urgent action is needed to ensure mental health needs are addressed in the implementation of the National Roadmap for Improving the Health of People with Intellectual Disability. Key opportunities in keeping with DRC recommendations relate to development of improved service models and funding, as well as equipping the mental health workforce with specific skills to meet the needs of people with intellectual disability. In addition, actions aimed at improving mainstream mental health supports and services must prioritise the needs of people with intellectual disability given their high rates of mental illness. Actions are also required to address the upstream social determinants of mental health, such as reduced economic opportunities (Alegría et al., 2018). Future research into the impact of DRC recommendations and other initiatives would help highlight specific strengths and barriers to implementation, and prepare the ground for future initiatives.
Limitations
Several limitations and strengths relate to the use of linked administrative data. Linkage of multiple data sets from a variety of sources allowed for identification of one of the largest population-based cohorts of people with intellectual disability internationally, who would otherwise be difficult to reach using survey methods. It is possible that people with mild intellectual disability not eligible for or not accessing education supports or disability services were not identified. The use of health service data to identify intellectual disability may have led to over-estimation of psychiatric conditions in this cohort, as those with health system contact are more likely to have recorded psychiatric diagnoses. Another shortcoming of using service receipt administrative data is that mental health service use is not fully synonymous with mental ill-health. The 2020–2022 National Study of Mental Health and Wellbeing (NSMHWB), a nationally representative survey study, showed that only 45% of the 4.3 million people experiencing a mental disorder within the past 12 months saw a health professional for their mental health in that time (ABS, 2023). Using a definition of SMI based on service receipt could also underestimate prevalence for people with intellectual disability given difficulties accessing services. As a result, our estimates are affected by the omission of undiagnosed/untreated psychiatric conditions.
Reporting of specific psychiatric and congenital/neurodevelopmental diagnoses is limited by level of detail available in data sets. Specifically, the MBS data set only recorded mental health service use without diagnostic information. Under-ascertainment of self-injury/suicidality also occurred as diagnostic codes in APDC/EDDC may include only the site and type of injury and not the cause of injury. We were unable to report on people with ADHD separate to learning disorders as both were assigned to the same category in the DS-MDS data set. Similarly, support for people with developmental conditions may be provided via pathways not covered by our data sets (such as NDIS and its predecessors), which is likely to have contributed to the very low estimates of developmental disorders in the comparator cohort. It would be valuable for future research to incorporate more comprehensive data from disability services, such as the newly established National Disability Data Asset (Department of Social Services, 2024), to improve estimates of neurodevelopmental conditions and other disabilities. This would also allow examination of how changes to disability services such as the NDIS have impacted mental health service use.
Conclusion
Drawing from one of the largest international cohorts of people with intellectual disability with extensive population ascertainment, we have confirmed the substantially increased prevalence of psychiatric conditions in people with intellectual disability compared to a matched comparator cohort. Particularly, people with intellectual disability and ADHD experience substantially elevated risk of co-occurring psychiatric conditions. People with Down syndrome had lower prevalence of co-occurring psychiatric conditions than other people with intellectual disability, except for increased rates of dementia. Findings also highlight the need for systemic responses to this high need and neglected population group. Future research directions include exploring risk factors of psychiatric conditions in people with intellectual disability, as well as service usage and whole of government health care expenditure towards this population group.
Supplemental Material
sj-docx-1-anp-10.1177_00048674251324824 – Supplemental material for Prevalence of psychiatric conditions in people with intellectual disability: A record linkage study in New South Wales, Australia
Supplemental material, sj-docx-1-anp-10.1177_00048674251324824 for Prevalence of psychiatric conditions in people with intellectual disability: A record linkage study in New South Wales, Australia by Samuel RC Arnold, Yunhe Huang, Preeyaporn Srasuebkul, Rachael C Cvejic, Stefan C Michalski and Julian N Trollor in Australian & New Zealand Journal of Psychiatry
Supplemental Material
sj-docx-2-anp-10.1177_00048674251324824 – Supplemental material for Prevalence of psychiatric conditions in people with intellectual disability: A record linkage study in New South Wales, Australia
Supplemental material, sj-docx-2-anp-10.1177_00048674251324824 for Prevalence of psychiatric conditions in people with intellectual disability: A record linkage study in New South Wales, Australia by Samuel RC Arnold, Yunhe Huang, Preeyaporn Srasuebkul, Rachael C Cvejic, Stefan C Michalski and Julian N Trollor in Australian & New Zealand Journal of Psychiatry
Supplemental Material
sj-docx-3-anp-10.1177_00048674251324824 – Supplemental material for Prevalence of psychiatric conditions in people with intellectual disability: A record linkage study in New South Wales, Australia
Supplemental material, sj-docx-3-anp-10.1177_00048674251324824 for Prevalence of psychiatric conditions in people with intellectual disability: A record linkage study in New South Wales, Australia by Samuel RC Arnold, Yunhe Huang, Preeyaporn Srasuebkul, Rachael C Cvejic, Stefan C Michalski and Julian N Trollor in Australian & New Zealand Journal of Psychiatry
Supplemental Material
sj-docx-4-anp-10.1177_00048674251324824 – Supplemental material for Prevalence of psychiatric conditions in people with intellectual disability: A record linkage study in New South Wales, Australia
Supplemental material, sj-docx-4-anp-10.1177_00048674251324824 for Prevalence of psychiatric conditions in people with intellectual disability: A record linkage study in New South Wales, Australia by Samuel RC Arnold, Yunhe Huang, Preeyaporn Srasuebkul, Rachael C Cvejic, Stefan C Michalski and Julian N Trollor in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
We acknowledge the contribution of all data custodians, the NSW Ministry of Health, the NSW Centre for Health Record Linkage, and the Australian Institute of Health and Welfare for providing the data and performing the linkage. We also acknowledge the Independent Health and Aged Care Pricing Authority for providing the ICD-10 AM information. We acknowledge the contribution of Katrina Sneath into the co-produced Easy-read summary for the study, and Michaela Kobor for workplace support.
Author Contributions
S.A. and Y.H. contributed equally to this work. S.A., Y.H., P.S., R.C., and J.T. contributed to the conceptualisation and design of this study. Y.H. and P.S. completed data analysis. S.A. and Y.H. drafted this manuscript with input from all authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The National Health and Medical Research Council Australia grants funded this work: Understanding Health Service System Needs for People with Intellectual Disability (GNT 1123033) and Addressing Health Inequality Experienced by People with Intellectual Disability (GNT2009771). Down Syndrome Australia and Aspen Foundation also provided financial support for this study. R.C. was supported by a Dementia Australia Research Foundation Post-doctoral Fellowship funded by the Dementia Australia Research Foundation and Bartle Pathway to Care.
Ethical Approval statement
The study was approved by the NSW Population and Health Services Research Ethics Committee (HREC/17/CIPHS/49; Cancer Institute NSW reference number: 2017/HRE1106), the Australian Institute of Health and Welfare (EO2017/5/404), ACT Health (ETH.11.17.262), Calvary Public Hospital Bruce (53-2017), Corrective Services NSW (approval date 19/07/2018) and the NSW Department of Education (SERAP2017600).
Data Availability Statement
The data that support the findings of this study were supplied by the NSW Centre for Health Record Linkage, but restrictions apply to the availability of these data, which were used under licence for the current study, and so are not publicly available.
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.