
Abstract
Across much of the developed world in recent decades, it has been policy to close the long-stay institutions that previously provided residential and health care for people with intellectual disabilities. Residential and health care have generally been devolved to community-based services. Models of psychiatric service provision have developed differently in different countries. Most developed countries, such as Australia, no longer routinely provide specialist health services for persons with intellectual disabilities, who instead rely on mainstream health services available for the whole population. Other countries that still have specialist services, such as the UK, appear to be moving in the direction of mainstream service provision [1].
People with intellectual disabilities comprise 1–2% of the population. People with intellectual disabilities have high rates of mental ill health with comorbid physical health problems, sensory, motor, and communication impairments, thereby creating complex clinical challenges. The prevalence of mental ill health among people with intellectual disabilities is as high as 40% in adults (95% confidence interval = 37.8–43.9%) [2], and 31–41% in children and adolescents, depending on age [3]. The diverse range of mental health problems in people with intellectual disability, often referred to as dual disabilities, includes neurobehavioural syndromes (such as autism) and behaviour disorders as well as the psychotic and mood disorders that are the central focus of public mental health service provision in Australia.
In 1994 Lennox and Chaplin surveyed the views of psychiatrists in the state of Victoria, Australia, regarding the psychiatric care of adults with intellectual disabilities [4]. Respondents generally considered that adults with intellectual disabilities and mental health disorders received a poor standard of care in both inpatient and community mental health settings, and thought that a higher standard of care would be provided by specialist services if they existed. A number of senior psychiatrists perceived a decline in the quality of psychiatric services for adults with dual disabilities over their professional lifetime, attributing this to the philosophy of ‘normalization’ and de-medicalization of the field. Furthermore, most respondents agreed that subspecialists in intellectual disability psychiatry should be responsible for the management of adults with dual disabilities.
The majority of respondents agreed that they had not received sufficient training in the assessment and management of behavioural and psychiatric disorders in adults with intellectual disabilities. This lack of training was borne out in practice, with respondents agreeing that their treatment of adults with intellectual disabilities was symptomatic rather than based on a diagnostic assessment. Support for training positions in dual disabilities was almost universal.
The responding psychiatrists also noted difficulties with the interface between psychiatric and disability services. They emphasized that residential care staff needed training in (i) the identification and management of psychiatric disorders, and (ii) the use of psychotropic medications. Furthermore, they believed that the morale and motivation of residential care staff was low, leading to high staff turnover, and supported improved resourcing and support for care staff.
Since that survey the needs of adults with dual disabilities have been acknowledged in key policy documents in Australia. The Second National Mental Health Plan identified people with intellectual disabilities and mental illness as one of the target groups with high-level needs and called for improved treatment and care, and improved access to and response by services, but this was to be achieved using current resources [5]. Little progress was made. The Steering Committee for the Evaluation of the Second National Mental Health Plan concluded that the development and implementation of effective service models for people with intellectual disabilities and mental disorder had not been realized and needed to be afforded higher priority [6]. The National Mental Health Plan 2003–2008 calls for better coordination of existing services for people with complex needs but makes no mention of the need for specialist expertise or clinical services [7].
Nonetheless, there have been a number of service developments and training initiatives in the State of Victoria. Academic units in developmental disability health were established in the early 1990s to provide medical education and clinical consultancy services. Academic teaching of trainee psychiatrists in intellectual disability commenced prior to the 1994 survey. A centralized statewide service was established in 2000 to provide education and consultation support services to mainstream, public, area mental health services providing services to people with dual disabilities [8]. During the last decade there have been a limited number of clinical training opportunities for trainee psychiatrists. This is in keeping with developments and progress in some States of Australia, and more generally in other developed countries.
In 2004 we conducted a repeat survey of the perceptions of psychiatrists in the Australian State of Victoria, with regards to the adequacy of their training, mental health service provision for meeting the mental health needs of people with intellectual disabilities and the working relationship with disability services. In a previously published report on generic versus specialist models of psychiatry training and service provision for people with intellectual disabilities, the results of the 2004 survey of perceptions of psychiatrists in Victoria have been compared with perceptions of learning disability psychiatrists in the UK, where specialist mental health services for people with intellectual disabilities are provided [9]. The aim of the present study was therefore to examine the impact of policy, service and training developments in the State of Victoria over the previous decade on the perceptions of psychiatrists, by comparing the contemporary perceptions of psychiatrists with the perceptions of psychiatrists elicited in the 1994 study. We hypothesized that there would be perceived improvements in all these areas in 2004 compared with 1994.
Methods
Questionnaire
The original questionnaire has been used by Lennox and Chaplin [4] and in other published studies [10], [11]. The questionnaire has face and construct validity, but formal tests of repeatability have not been performed. It was used in the present study to enable a direct comparison of 2004 and 1994 results, but was slightly modified for a comparison study between Victorian psychiatrists and specialist learning disability psychiatrists in the UK [9]. Some questions were re-worded to take into account differences between Australia and the UK while maintaining the meaning of the question. The 1994 survey defined people with intellectual disabilities who have a psychiatric disorder as people with dual disabilities, while the 2004 survey refers to people with intellectual disabilities and mental health need. The 2004 questionnaire also contains additional questions about training, professional confidence, the adequacy of acute admission ward for both adults with mild and severe intellectual disabilities, and autism spectrum disorders. For the 1994 questionnaire, please go to the following website: http://www.som.uq.edu.au/research/qcidd/files/1994_Psychiatrist_Questionnaire.pdf.
The 50-item questionnaire is divided into five sections, covering demographic characteristics of participants, details about the needs of their patients, their opinions on assessment and management, the role of psychiatry in intellectual disabilities, and services for adults with dual disabilities. The main section of the survey asks about the role of psychiatry in intellectual disabilities. It consists of 31 statements on a 1–6 point Likert scale ranging from ‘disagree very much’ to ‘agree very much’. The statements cover areas of service provision, training, and perceptions of competency in working with people with dual disabilities, use of psychotropic medications and other areas.
The sections about the role of psychiatry in intellectual disabilities, and services for adults with dual disabilities use open questions. Participants were asked their opinion as to whether they believed that there should be a specialty of intellectual disability psychiatry and what the role of such a service would be if it were to become a reality. Suggestions were sought on improving training of psychiatrists and improving services for this population.
Participants
Questionnaires were included in the mailout of the newsletter of the Victorian Branch of the Royal Australian and New Zealand College of Psychiatrists (RANZCP). The newsletter is sent to Fellows of the RANZCP (psychiatrists) and accredited trainees. The Victorian Branch of the RANZCP reported that approximately 624 Fellows were registered at the time of the survey. Respondents were asked to indicate if they were psychiatrists or trainee psychiatrists. Questionnaires returned from trainee psychiatrists were not included in the present study. Questionnaires were included in the next mailout of the newsletter of the Victorian Branch of the RANZCP, inviting those who had not previously responded to participate.
Ethics
Ethics approval was sought and granted by the Monash University Standing Committee on Ethics in Research in Humans.
Statistical analysis
Data were managed and analysed using Stata software version 10.0 (StataCorp, College Station, TX, USA). Descriptive statistics were computed and groups were compared using independent sample t-tests. To account for multiple comparisons p < 0.001 was considered statistically significant. We used NVivo software version 2 (QRS International, Doncaster, Vic., Australia) to analyse the qualitative data.
Results
A total of 170 psychiatrists (27%) responded to the 2004 survey and of these, 69% were male. They had graduated from medical school on average 26 years earlier (range 9–50 years) and 85% had at sometime worked with adults with intellectual disabilities.
Of the 170 psychiatrists who responded, in the previous 6 months 116 did not have any consultations with adults with intellectual disabilities, 32 conducted public but not private consultations, four conducted private but not public consultations, and 18 conducted both public and private consultations. The mean±SD number of visits for adults with dual disabilities in public settings only was 3.3±0.9, and for private settings only it was 3.3±0.5. The mean±SD number of visits for adults with dual disabilities in both public and private settings was 6.1±2.6 for public and 5.9±1.9 for private practitioners. These results indicate that there was very little difference between the caseload for public and private practice for dual disability.
The work that the psychiatrists undertook was most commonly with problem behaviours, schizophrenia and depression. Table 1 outlines the diagnostic groupings that psychiatrists commonly addressed with adults with dual disabilities, and compares the differences between 1994 and 2004. The 2004 survey captured the breadth of disorders being treated, which include dementia, sleeping disorders and alcohol dependence.
Most common health needs of adults with intellectual disabilities, according to psychiatrists
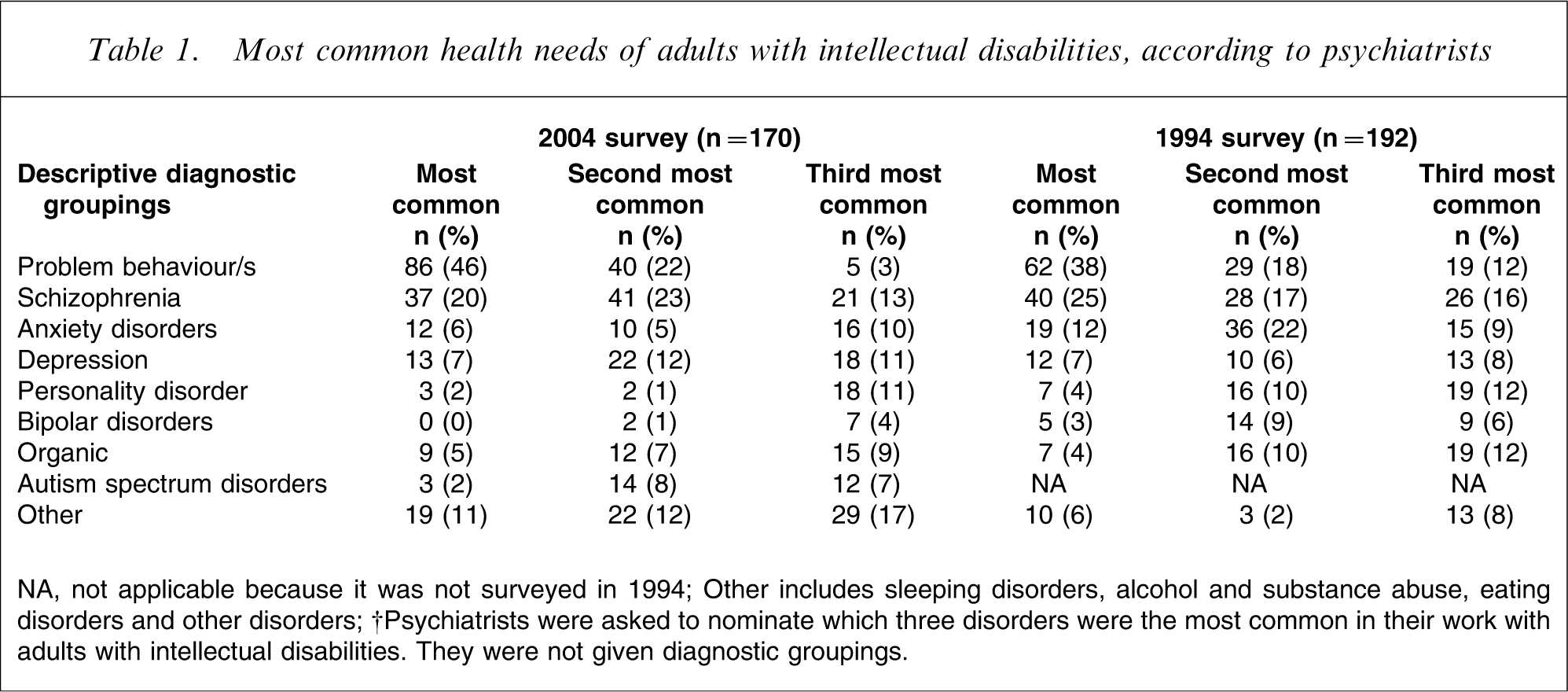
NA, not applicable because it was not surveyed in 1994.
Other includes sleeping disorders, alcohol and substance abuse, eating disorders and other disorders.
†Psychiatrists were asked to nominate which three disorders were the most common in their work with adults with intellectual disabilities. They were not given diagnostic groupings.
Participants’ opinions on the role of psychiatry in intellectual disabilities are listed in Table 2, where they are compared to results from the 1994 survey. Psychiatrists in 2004 disagreed less strongly that acute admission wards are adequate to meet the needs of adults with mild intellectual disabilities in contrast to 1994. In 2004, however, psychiatrists disagreed more strongly that the acute wards were suitable for adults with severe intellectual disabilities. In 2004 psychiatrists were more emphatic that patients with intellectual disabilities in general were vulnerable to exploitation on the acute wards. Psychiatrists indicated that they felt better trained in assessing and managing psychiatric disorders and behaviour problems in adults with intellectual disabilities, than they did in 1994, but that they felt inadequately trained to assess adults with autism.
Comparison of 2004 (n = 170) and 1994 survey of psychiatrists (n = 192)
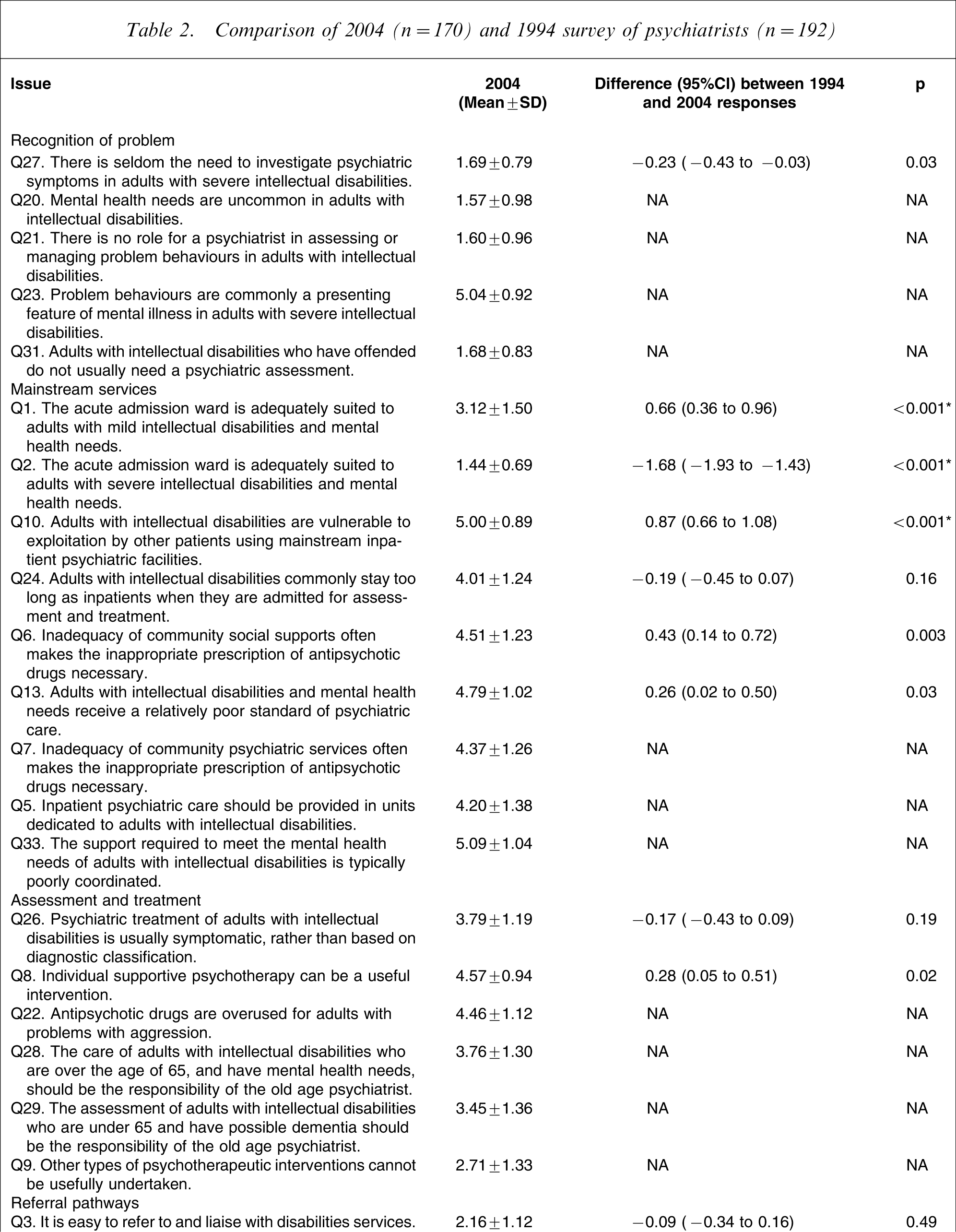
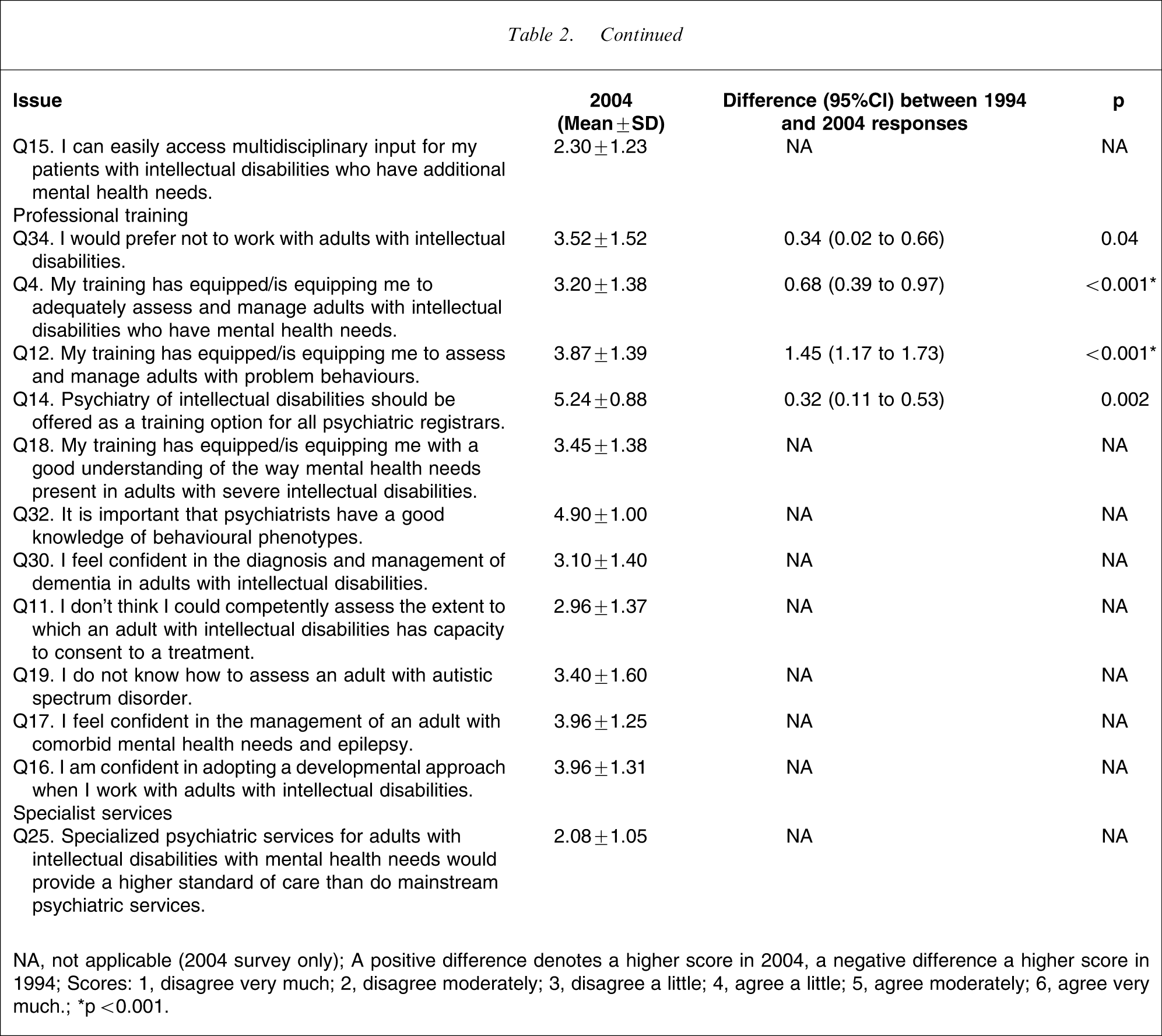
NA, not applicable (2004 survey only).
A positive difference denotes a higher score in 2004, a negative difference a higher score in 1994.
Scores: 1, disagree very much; 2, disagree moderately; 3, disagree a little; 4, agree a little; 5, agree moderately; 6, agree very much.
∗p < 0.001.
The two open-ended questions in the 2004 survey of psychiatrists sought ideas for the improvement of psychiatric training and mental health services to better meet the mental health needs of adults with intellectual disabilities. Suggestions were given by 117 of the respondents. There was overwhelming support for some form of training (n = 106), in particular, experiential specialist clinical training (n = 97) and specialist services of some kind (n = 74). Teaching in intellectual disability at undergraduate and postgraduate levels (n = 43), RANZCP mandatory training requirement (n = 11), and training of other mental health professionals were also recommended (n = 18). Suggestions for the improvement of clinical services included increased resourcing (n = 17), replication of the UK model of specialist services (n = 4), specialist services integrated within mainstream services (n = 12) and accessible, mobile and timely consultation–liaison-type services (n = 11). There was clearly expressed dissatisfaction with the current model of consultation only service (n = 14). This was summed up succinctly by one respondent: ‘To stop assessing and start treating’. Poor professional attitudes, lack of coordination and hostility between mental health and disability services were commonly condemned (n = 35).
Discussion
During the decade from 1994 to 2004, a number of initiatives in the training of psychiatrists and mental health service provision for people with dual disabilities were implemented, so we expected to see an improvement in perceptions of training and service provision. There was a small but significant increase in professional confidence among psychiatrists in Victoria, and a greater sense of being better trained in the assessment and management of psychiatric and behaviour disorder in adults with intellectual disabilities. Nonetheless, respondents do not feel confident about assessing people with autism and consider training in general to be inadequate. Respondents overwhelmingly called for the availability of specialist training positions.
In addition there continues to be as much, if not more, concern about the quality of mainstream mental health service provision for adults with intellectual disabilities, especially severe intellectual disabilities, as there was a decade ago. Psychiatrists disagreed less that acute admission wards are suitable for adults with mild intellectual disabilities, possibly indicating a degree of acceptance of the role of public mental health in providing care to adults with dual disabilities. This is counterbalanced, however, by concerns about the potential for exploitation of people with intellectual disabilities in general on the acute wards. Furthermore, the acute wards are considered to be unsuitable for adults with severe intellectual disabilities. This is of concern because there is no alternative inpatient setting for adults with severe intellectual disabilities and acute, serious mental health problems. The lack of coordination and cooperation between mental health and disability services remains a major concern and source of frustration. This could explain why many psychiatrists prefer not to work with people with intellectual disabilities. Responding psychiatrists overwhelmingly identified the need for specialist assessment and management mental health services for adults with dual disabilities.
There is a failure by policy makers to recognize the need for specialist clinical services to assess and manage complex clinical care of people with intellectual disabilities and mental health need. Indeed, subspecialist mental health services have been resisted by policy makers while medical and surgical services become ever more specialized. The psychiatrists recognize the role of psychiatrists in assessing and managing problem behaviours in people with intellectual disabilities. The statewide dual disability service was established to address this need by providing a one-off assessment and management plan. This model, however, has limitations because it does not allow for direct specialist management and it does not address problems related to autism and behavioural disorder that do not fall within the remit of public mental health services.
There has been no real shift in the perception of the overall quality of care provided by area mental health service and there was a clearly expressed dissatisfaction with consultation-only services. Respondents agree that inadequate services lead to inappropriate prescription of antipsychotic medications. Furthermore, specialist clinical training cannot occur in a vacuum. Specialist training requires placement and specialist supervision in specialist clinical services.
The survey asked respondents to recall and quantify their work with adults with dual disabilities. Individual caseloads and the common conditions encountered appear not to have changed significantly between 1994 and 2004. The 2004 survey, however, demonstrates the wide range of mental health problems seen in clinical practice.
In our previous study the perceptions of psychiatrists and trainees in Victoria were compared with specialist learning disability psychiatrists and trainees in the UK [9]. The UK participants had positive views about the specialist dual disabilities service model, which is unique to the UK. This model is reported as being responsive to the range of mental health needs of the population with intellectual disabilities, providing flexible accessible clinical services and a wide range of treatment modalities and supports. The UK specialists and trainees were knowledgeable, well-trained and confident. The UK respondents expressed doubts about the ability of mainstream mental health services to adequately meet the needs of people with dual disabilities. In contrast, services in Victoria were limited in modes of service delivery, the range of mental health needs addressed and the treatments offered. Psychiatrists and trainees in Victoria considered themselves unskilled, undertrained, inexperienced and lacking in confidence in working with people with intellectual disabilities [9].
The strength of the present study design lies in its ability to demonstrate trends over a 10 year period, but interpretation of survey results requires caution. The response rate of 27% to the 2004 survey was disappointing and difficult to explain. Factors such as increased requests to participate in research, the increased length of the questionnaire, to disinterest in intellectual disabilities, could account for the poor response [10]. The survey is potentially biased towards psychiatrists who have an interest in intellectual disability or who wished to express their frustration at the limitations of the current system. If so, the findings are not necessarily representative of all RANZCP fellows in Victoria. These findings, however, echo the findings of a similar survey of psychiatrists in the Australian State of Queensland [10], and indicate widespread dissatisfaction with current training opportunities and lack of specialist services and service coordination. Although the study was limited by being conducted in only one State, the similar nature and type of service provision and training across Australia and most developed countries (with the exception of the UK) suggest that its findings may be generalizable to other areas. We investigated the perceptions of one professional group, and future research to investigate the perceptions of service-users of their experiences and outcomes is therefore warranted.
Conclusion
Service and training developments over a decade have not translated into clear changes in the perceptions of psychiatrists that there have been improvements in the provision of mental health care of adults with intellectual disabilities by mainstream public mental health services. Indeed, psychiatrists continue to report the care provided by mainstream services as substandard and have not found consultation-only services to be of much value. Psychiatrists in Victoria overwhelmingly call for specialist mental health services for adults with intellectual disabilities.
The contrast between the views of psychiatrists within the generic service model in Australia and those within the UK specialist service model suggests that mainstream services, as currently configured, fail to meet the mental health needs of adults with intellectual disabilities or to provide training that prepares psychiatrists in assessing and managing mental health problems in adults with intellectual disabilities. Policy direction in the UK is moving away from the provision of specialist mental health care of adults with intellectual disabilities towards generic mental health service provision with specialist support. The present findings, however, serve as a cautionary lesson as to the potential negative consequences of dismantling specialist services and associated specialist clinical training in favour of mainstream service provision for people with dual disabilities. The present findings also support the reform of the model of generic mental health service provision to people with intellectual disabilities within Australia and other developed countries. The challenge is to provide integrated specialist mental health care of people with intellectual disabilities and specialist training of mental health professionals within the framework of mainstream services so that the historical segregation of care of adults with dual disabilities is not repeated and so that services are not duplicated at great costs to the taxpayer.
Footnotes
Acknowledgements
The work in this article was supported by a grant from the Victorian Government Department of Human Services and the cooperation of the RANZCP. The authors appreciate the time spent by the responding psychiatrists in completing the questionnaire.