
Abstract
Purpose:
This study aimed to explore risk factors for suicide in Aboriginal and non-Aboriginal people following hospital admission for suicidal ideation and self-harm in the Northern Territory, Australia to help clarify opportunities for improved care and intervention for these population groups.
Methods:
Individuals with at least one hospital admission involving suicidal ideation and/or self-harm between 1 July 2001 and 31 December 2013 were retrospectively recruited and followed up using linked mortality records to 31 December 2014. Survival analyses stratified by Indigenous status identified socio-demographic and clinical characteristics from index hospital admissions associated with suicide.
Results:
Just over half of the 4391 cohort members identified as Aboriginal (n = 2304; 52.4%). By 2014, 281 deaths were observed comprising 68 suicides, representing a 2.6% and 2.0% probability of suicide for Aboriginal and non-Aboriginal people, respectively. After adjusting for other characteristics, a higher risk of suicide was associated with male sex (Aboriginal adjusted hazard ratio: 4.14; 95% confidence interval: [1.76, 9.75]; non-Aboriginal adjusted hazard ratio: 5.96; 95% confidence interval: [1.98, 17.88]) and repeat hospital admissions involving self-harm (Aboriginal adjusted hazard ratio: 1.37; 95% confidence interval: [1.21, 1.55]; non-Aboriginal adjusted hazard ratio: 1.29; 95% confidence interval: [1.10, 1.51]). Severe mental disorders were associated with a four times higher risk of suicide (adjusted hazard ratio: 4.23; 95% confidence interval: [1.93, 9.27]) in Aboriginal people only.
Conclusion:
The findings highlight non-clinical risk factors for suicide that suggest the need for comprehensive psychosocial assessment tailored to Aboriginal and non-Aboriginal people hospitalised with suicidal ideation or self-harm. Implementing appropriate management and aftercare within a broader public health framework is needed to support recovery and reduce long-term suicide risk in the community, especially for Aboriginal people and males.
Introduction
Hospital-treated self-harm is one of the strongest predictors of subsequent suicide (Carroll et al., 2014) and has consistently been associated with up to 50 times greater risk of suicide compared to the general population (Geulayov et al., 2019; Hawton et al., 2015). The Northern Territory (NT) population experiences the highest rates of both suicide (Australian Bureau of Statistics [ABS], 2021) and self-harm (Australian Institute of Health and Welfare [AIHW], 2021) of any jurisdiction in Australia. Aboriginal and Torres Strait Islander people (hereafter, respectfully referred to as Aboriginal people) are the original inhabitants of Australia and make up approximately 30% of the NT’s residents (ABS, 2018) but account for 50% of suicides each year (ABS, 2021). The higher burden of suicide and self-harm carried by the Aboriginal population of the NT is consistent with the rest of Australia where rates of self-harm hospital admissions (AIHW, 2021) and suicide deaths (ABS, 2021) are more than twice those of the general Australian population.
Several case series studies point to important differences in the characteristics of suicide by Aboriginal and non-Aboriginal people. In particular, they have shown that psychosocial risk factors, such as substance misuse, interpersonal conflict, and relationship breakdown, were more common precipitants in Aboriginal suicides, and mental illness was more prevalent in suicides by non-Aboriginal people (Kuipers et al., 2012; Parker and Ben-Tovim, 2002). One of these studies also identified an increased likelihood of a history of self-harm among Aboriginal compared to non-Aboriginal suicides (Parker and Ben-Tovim, 2002). Additionally, Aboriginal people have also identified suicidal ideation as one of a range of worrying expressions of distress experiencing increasing trends in recent years (Leckning et al., 2016) that may be associated with an increased risk of suicide (McHugh et al., 2017). The absence of evidence supporting a difference in the relative risk of suicide following suicidal ideation or self-harm (Large et al., 2021) further reinforces the need for the inclusion of suicidal ideation in longitudinal studies of suicide for both Aboriginal and non-Aboriginal populations to better understand opportunities for prevention.
Hospital responses to suicidal ideation and self-harm are considered an important part of the health care system’s role in a public health approach to preventing suicide (World Health Organization, 2012). However, no longitudinal population-level studies of hospital-treated self-harm from a 2014 systematic review and meta-analysis reported results for an Indigenous population (Carroll et al., 2014) and only one recent study of hospital-treated self-harm by adolescents and young adults reported the relative risk of suicide by Indigenous identity (Olfson et al., 2018). In this study, we will address this critical gap in the evidence by exploring the long-term risk for suicide distinct to Aboriginal and non-Aboriginal people recorded in administrative hospital records following admission for suicidal ideation and self-harm that can inform more appropriate and targeted approaches to prevention for these population groups.
Method
Study design and population
We conducted a retrospective cohort study of all NT residents with at least one hospital admission involving a diagnosis of intentional self-harm (International Statistical Classification of Diseases and Related Health Problems, 10th Revision, Australian Modification [ICD-10-AM] codes: X60-X84) and/or suicidal thoughts (ICD-10-AM codes: R45.81) between 1 July 2001 and 31 December 2013. Consistent with the prevailing nomenclature in the literature, the term self-harm will continue to be used to refer to admissions involving diagnosis codes of intentional self-harm since these codes only capture the non-accidental nature of the act but do not differentiate between suicidal and non-suicidal intent. Individuals were excluded if they met any of the following criteria at the time of their first hospital admission involving suicidal ideation and/or self-harm (index admission): no Indigenous status recorded (n = 2); age less than 10 years (n = 10) because the diagnoses of self-harm or suicidal ideation may reflect administrative coding errors or extreme cases of early-onset suicidality; or death occurred during admission (n = 22, with 15 [68%] determined to be due to suicide) since these cases would not contribute any follow-up time to the longitudinal analysis described below.
Data sources and collection
Three key data sources were used for this study: the NT Inpatient Activity collection containing records of admissions to all NT public hospitals, and mortality records from the NT Death Certificates Registry held by the Department of Health and the National Death Index (NDI) held by the Australian Institute of Health and Welfare.
For all individuals included in the study, de-identified records of public hospital admissions (including admissions to emergency departments) were extracted from the NT Inpatient Activity collection from 1 July 2000 to 31 December 2014 to ensure each individual in the study had at least 1 year of hospital records prior and subsequent to the date of their index admission. Each record includes patient socio-demographic information, the date of admission and discharge, hospital and ward of admission, and up to 50 diagnosis codes from the ICD-10-AM for conditions assessed and treated during admission. It should be noted that public hospital admissions alone are representative of hospital admissions in the NT involving suicidal ideation and self-harm since these presentations are unlikely or would not be treated at the only private hospital in the NT, which does not have an acute care or mental health service.
Mortality records for the study cohort were obtained by combining the result of two separate linkages. A copy of the NT Death Certificate Registry, which contains records of all deaths registered in the NT, is held by the NT Department of Health who matched all decedents to their corresponding Hospital Registration Number (HRN). The HRN uniquely identifies all individuals who have used a government-run health service and has been regularly validated since 1991 (Foley et al., 2012). Individuals in the study cohort were linked deterministically to the NT Death Registry using their HRN from the hospital admission records. All causes of death were coded by a trained research assistant who followed the standard ICD-10 coding procedures. The study cohort was also probabilistically linked to the NDI, which holds coded mortality records from all Australian jurisdictions. To ensure the research team were not exposed to identifiers used in the linkage process, the NT Department of Health facilitated linkages and clerical review of the matches from the NDI and Death Certificates Registry to produce de-identified mortality records for the study cohort.
Individuals were followed up from their index admission through hospital and mortality records until death or 31 December 2014, whichever came first.
Measure of suicide
Suicide is the main outcome of interest and was identified in mortality records with ICD-10-AM codes X60 to X84 in the underlying cause of death field. The inclusion of one (1) death due to self-harm with undetermined intent (ICD-10-AM codes Y10-Y34) was identified and its inclusion in the analysis made no difference to the results and, therefore, has not been included. Individuals were censored if they died from any cause other than suicide.
Risk factors explored
Socio-demographic characteristics
Differences in outcome by sex, age, Indigenous status (Aboriginal vs non-Aboriginal) and residence were calculated using information obtained from the record of index admission. Residence was coded into seven administrative districts established by the NT Department of Health for planning and organising health service delivery (see Table 1). They were aggregated into two regions: the Top End, which groups residents from the northern, mostly tropical communities including the capital city of Darwin, and; Central Australia, which represents the more arid, southern communities and towns including the important service hub of the Alice Springs township. Residence was also aggregated into remoteness categories of urban (comprising Darwin Urban and Alice Springs Urban administrative districts) or remote (comprising Darwin Rural, Alice Springs Rural, Barkly, Katherine, and East Arnhem administrative districts) residence. Finally, an interaction of these two aggregated geographical categories was also created: Top End Urban, Top End Remote, Central Australia Urban and Central Australia Remote.
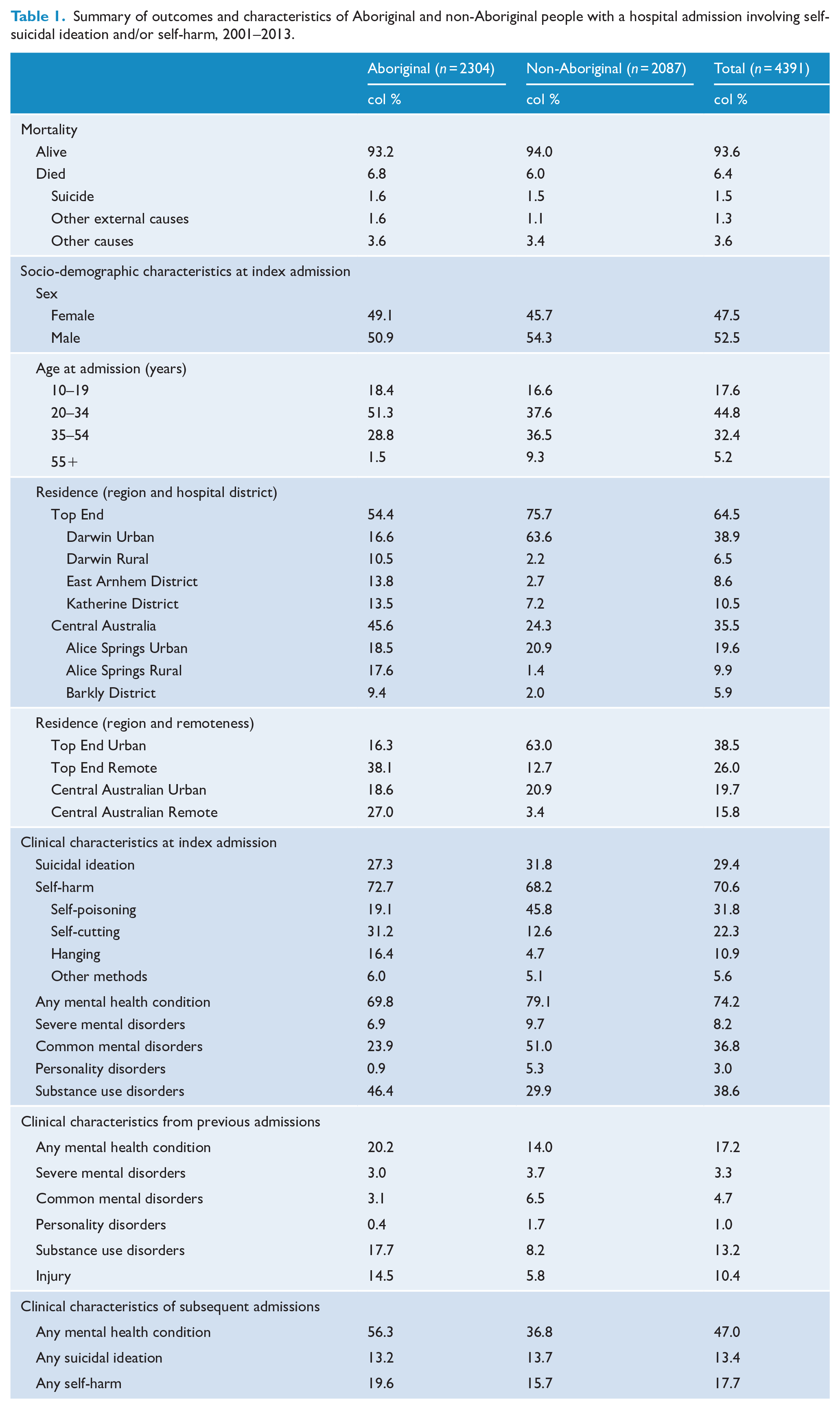
Summary of outcomes and characteristics of Aboriginal and non-Aboriginal people with a hospital admission involving self-suicidal ideation and/or self-harm, 2001–2013.
Categories of suicidal ideation and self-harm
Index admissions distinguished between two common pathways to suicide: suicidal ideation and self-harm. Self-harm is further distinguished by common methods that may reflect differences in suicide risk (Spittal et al., 2012): self-poisoning (ICD-10-AM: X60-X69), self-cutting (ICD-10-AM: X78), hanging (ICD-10-AM: X70) and other types of self-harm (ICD-10-AM: X71-X77 and X79-X84). Where diagnosis codes of suicidal ideation and self-harm were co-present, admissions were coded into the relevant category of self-harm to ensure mutually exclusive categories. Where more than one type of method of self-harm was found, the admission was coded into the most lethal category of self-harm defined by case fatality ratio (Spittal et al., 2012). Counts of subsequent admissions involving any type of suicidal ideation and self-harm were also calculated over the follow-up period to be used as time-varying covariates in the modelling.
Mental health conditions
Historical and current mental health conditions known to have some association with higher risk of suicide (Carroll et al., 2014) were derived from the diagnosis codes of prior and index hospital admission records, respectively. These codes were organised into the following mutually exclusive clinically relevant groups that have been validated in other studies using administrative data sources (Dean et al., 2018): (1) severe mental disorders, comprising psychotic symptoms and illnesses; (2) common mental disorders, such as depression and anxiety; (3) personality disorders; (4) substance use disorders; (5) other adult-onset disorders; and (6) other childhood-onset disorders. Other adult- and child-onset disorder categories were excluded from the final analysis due to the small numbers and their relatively weak association with suicide risk in the existing evidence (Carroll et al., 2014; Too et al., 2019). A count of subsequent admissions involving any mental health condition was also calculated over the follow-up period for each individual to be used as a time-varying covariate in the modelling.
Statistical analyses
All analyses were stratified by Indigenous status to identify characteristics distinct to Aboriginal and non-Aboriginal people that are associated with a higher risk of suicide. The Kaplan–Meier (KM) method was used to estimate the probability of survival (and 95% confidence intervals) and suicide (1 – KM) over the follow-up period. Univariate hazard ratios (HRs) were estimated using Cox proportional hazards regression to determine the association between suicide and socio-demographic and clinical characteristics of the study cohort. To determine whether multivariable models required adjustment for secular trends over the lengthy study period (13 years), the association between year of index admission and survival time was tested and found not to be statistically significant. A backward elimination approach, starting with all characteristics showing some evidence of association with suicide in univariate analyses (i.e. p < 0.2), was used to build multivariable models to estimate adjusted hazard ratios (aHR). Distinct categories of residence were used for each of the multivariable models for Aboriginal (interaction of region and remoteness) and non-Aboriginal (region only) people that reflect important differences in geographic distribution of each population and which contained enough numbers to support analysis. Time-varying covariates measuring the count of subsequent hospital admissions involving (a) any mental health condition, (b) suicidal ideation only and (c) self-harm were added separately as a final step to observe their effect on other covariates that may indicate shared causal pathways (i.e. >10% change in estimated coefficients or change in statistical significance of time-invariant covariates). No such effects were observed among the time-varying covariates explored and, therefore, no exclusions or adjustments were made on this basis. The proportionality assumption of each covariate was tested formally (Grambsch and Therneau, 1994) and visually (Hess, 1995) using Schoenfeld residuals and no violations were found. Socio-demographic characteristics and categories of suicidal ideation and self-harm were retained in all models to ensure adjustment by these important population and clinical characteristics. The variation in outcomes explained by each multivariable Cox regression model was calculated using Royston’s pseudo adjusted R2 (Royston, 2006). All analyses were undertaken using Stata 15.0.
Ethical approval
Ethical approval for this study was provided by the Human and Research Ethics Committees of Central Australia (Ref: 13-150) and the NT Department of Health and Menzies School of Health Research (Ref: 15-392), and by the Australian Institute of Health and Welfare (Ref: 2013-3-31) for linkage to national mortality records.
Results
A total of 4391 individuals were included in the study with an index admission involving self-harm (n = 2956), suicidal thoughts (n = 1292) or both (n = 143) between 1 July 2001 and 31 December 2013. Just over half identified as Aboriginal and/or Torres Strait Islander and just under half were female. Some notable differences in the distribution of socio-demographic and clinical characteristics of Aboriginal and non-Aboriginal members of the cohort were observed at index admission (see Table 1). In particular, a higher proportion of Aboriginal people were observed at index admission to be younger, come from remote areas, include self-harm by hanging or cutting, and include diagnoses of substance use disorders compared to non-Aboriginal people. A higher proportion of non-Aboriginal compared to Aboriginal people at index admission were found with diagnoses of common mental disorders, such as depression and anxiety.
In total, 281 deaths were observed by 31 December 2014, with suicide representing almost a quarter of all deaths (n = 68/281; 24.2%). Hanging was the most common method of self-harm in the cases of suicide (n = 53/68; 77.9%). A summary of follow-up time and absolute risk of suicide over time by Indigenous status is presented in Table 2 and illustrated in Figure 1.
Summary of follow-up time and suicide overall and by Aboriginal and non-Aboriginal people following index hospital admission involving suicidal ideation and/or self-harm, 2001–2013.
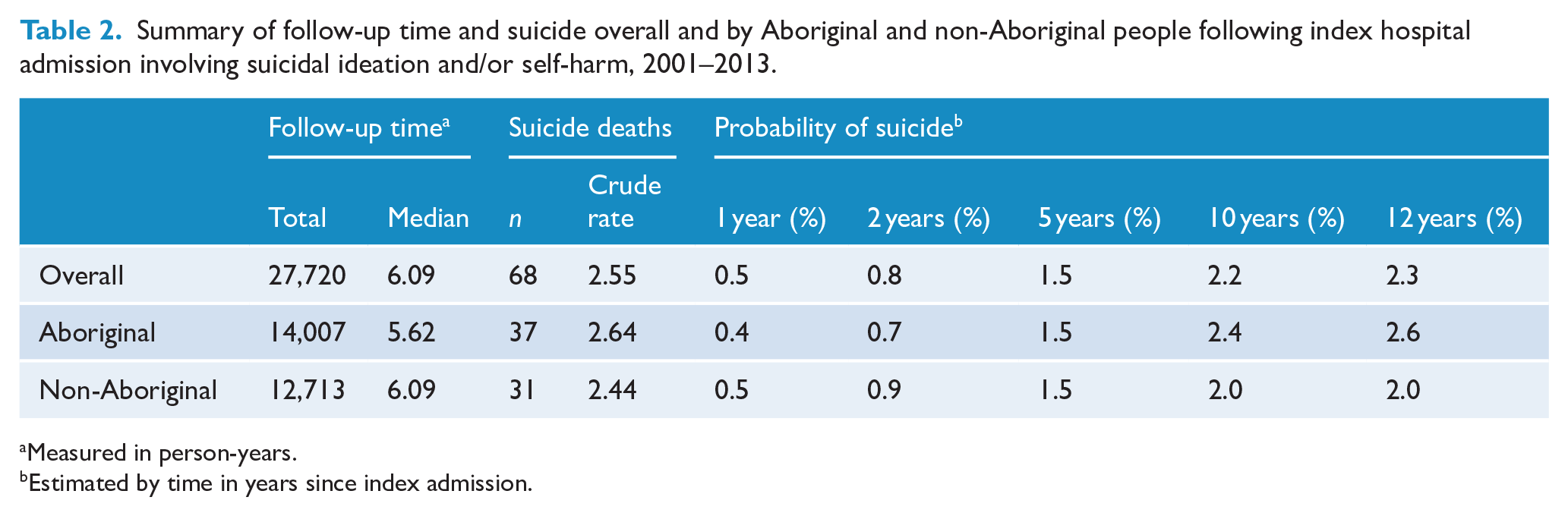
Measured in person-years.
Estimated by time in years since index admission.
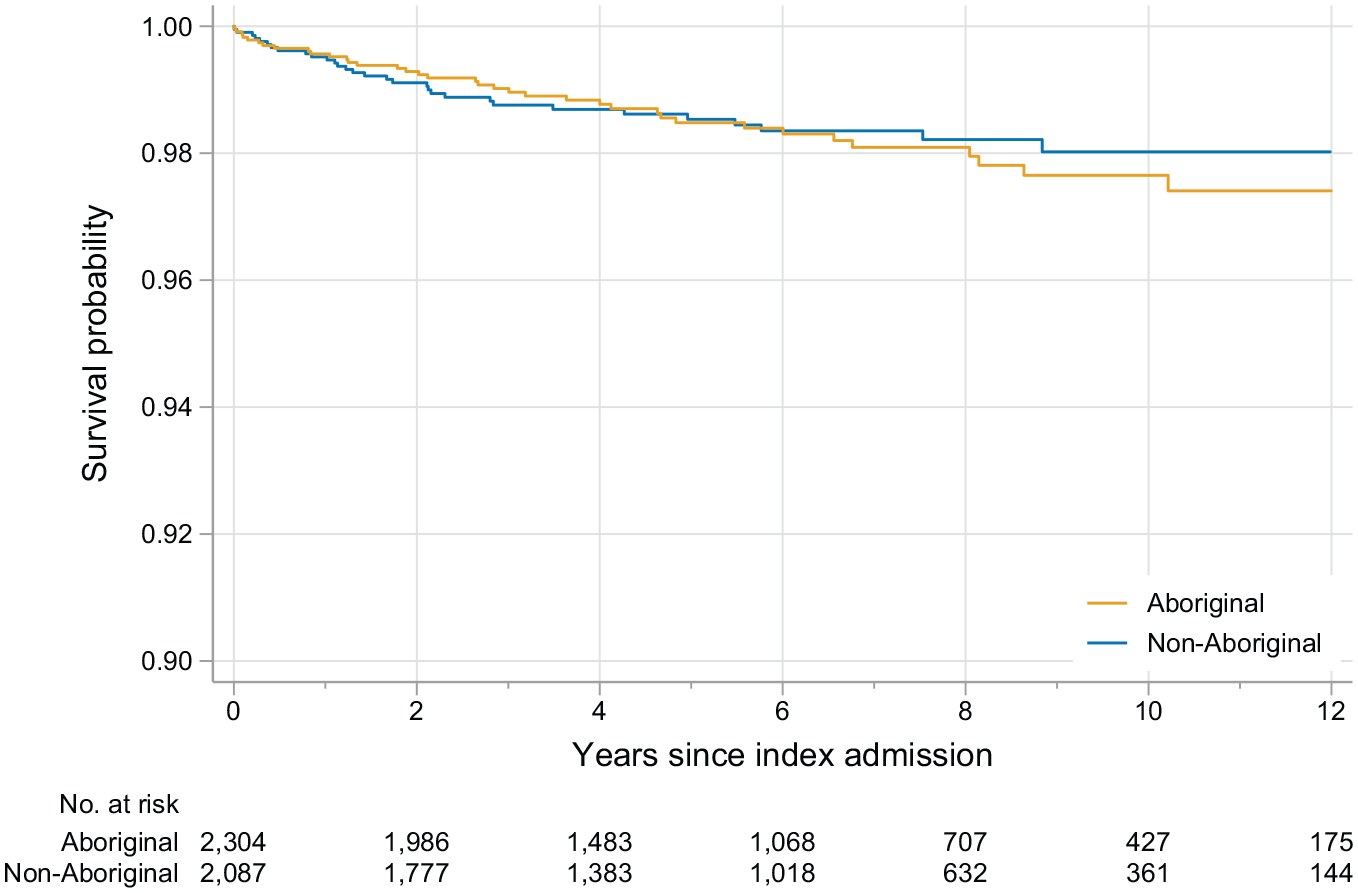
Probability of survival following index hospital admission involving suicidal ideation and/or self-harm by Aboriginal and non-Aboriginal people, 2001-2013
Approximately half of all suicides observed in this study occurred within 2 years of index admission for both the Aboriginal (n = 16/37 suicides) and non-Aboriginal (n = 18/31 suicides) people. Although the absolute risk of suicide at the end of the study was greater among Aboriginal compared to non-Aboriginal people, the univariate estimates of relative risk across Indigenous status suggest this was not statistically significant (HR: 1.08; 95% confidence interval [CI]: [0.67, 1.75]).
The characteristics found to be associated with a higher hazard rate of suicide were similar for the Aboriginal and non-Aboriginal members of the cohort (see Table 2). Following the index admission, the risk for suicide in males compared to females is four times higher for Aboriginal people and almost six times higher for non-Aboriginal people. The risk of suicide is also increased by 37% for the Aboriginal and 29% for the non-Aboriginal members of the cohort for each hospital admission involving self-harm following the index admission. No clinical characteristics were found to be associated with time to suicide for non-Aboriginal people, but the risk of suicide was four times higher among Aboriginal people with diagnoses of severe mental disorders at index admission. No strong evidence of differences in the risk of suicide for either Aboriginal or non-Aboriginal people was found between index admissions involving suicidal ideation alone and those involving self-harm (see Supplementary Tables 1 and 2).
Each model was found to explain just over 40% of the variation in suicide as measured using Royston’s R2 shown in Table 3. Sex was observed to be the strongest predictor using univariate estimates of Royston’s R2, accounting for 31% and 42% of variation in suicide for Aboriginal and non-Aboriginal cohort members, respectively.
Socio-demographic and clinical characteristics associated with a higher risk of suicide by Aboriginal and non-Aboriginal people following index hospital admission involving suicidal ideation and/or self-harm, 2001–2013.
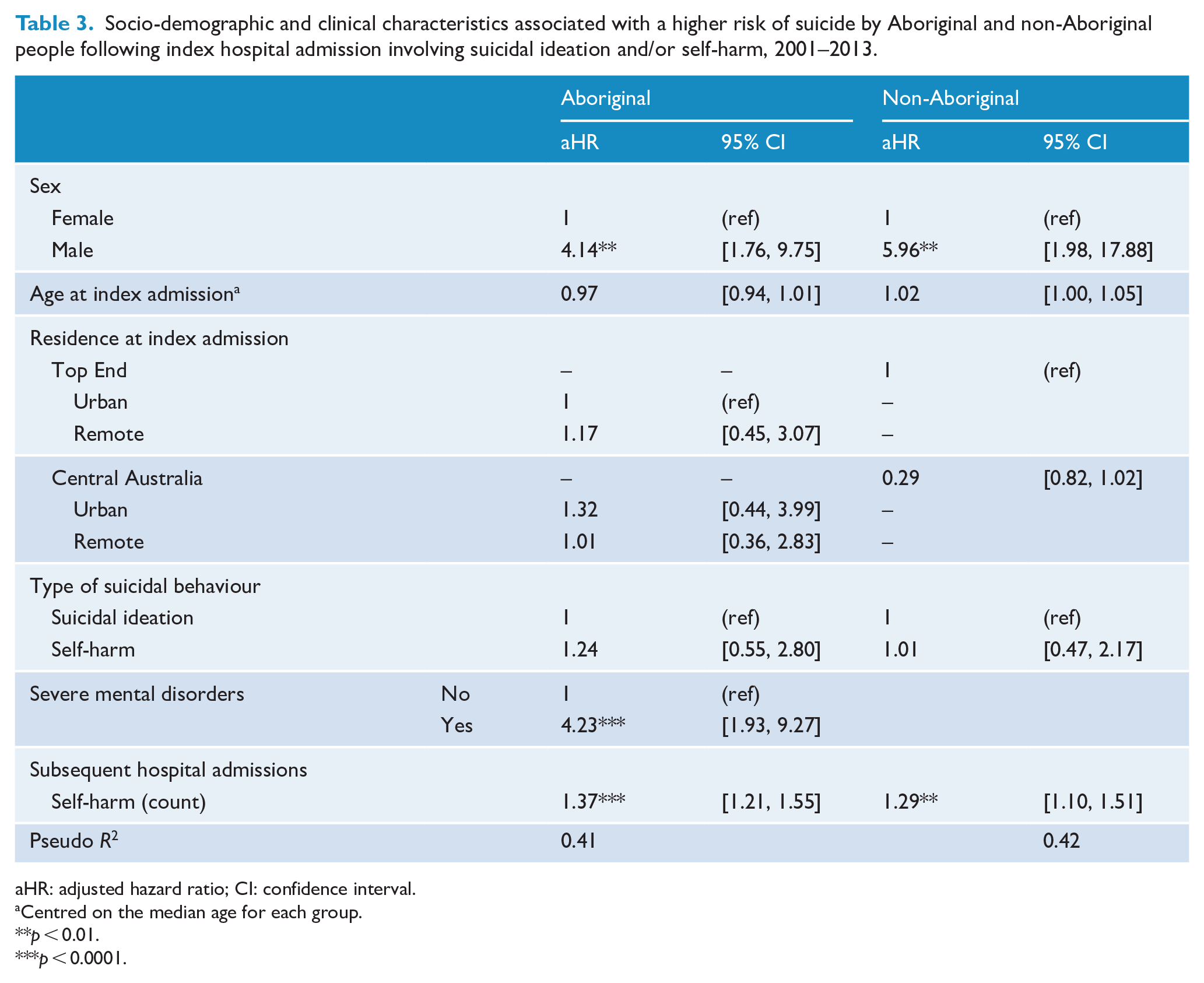
aHR: adjusted hazard ratio; CI: confidence interval.
Centred on the median age for each group.
p < 0.01.
p < 0.0001.
Discussion
This longitudinal cohort study is the first of its kind for the NT and, to the best of our knowledge, is the only population-level investigation in Australia to explore the distinct risk factors for suicide in Aboriginal and non-Aboriginal people hospitalised with suicidal ideation and self-harm. By the end of the study, the absolute risk of subsequent suicide for the Aboriginal members of the study cohort was non-significantly higher than their non-Aboriginal counterparts. The overall probability of subsequent suicide in the study – 0.05% after 1 year and 1.5% after 5 years with 1 in 44 people (2.3%) having died by suicide by the end of the study – is similar to estimates from other studies of hospital-treated self-harm (Carroll et al., 2014) and justifies the targeting of this population for hospital and follow-up interventions.
Characteristics of hospital admissions involving suicidal ideation and self-harm found to be associated with a higher risk of suicide offer insights into potential targets of preventive intervention. Sex was identified as the most influential predictor in the modelling with males found to carry the highest risk of suicide after adjusting for other influences, with similar associations identified for Aboriginal and non-Aboriginal males who died by suicide at around four to five times the rate of their female counterparts. This is higher than has been reported in most studies elsewhere (Carroll et al., 2014; Miranda-Mendizabal et al., 2019) and may reflect the relatively higher rate ratio of male to female hospital admissions in the NT (Leckning et al., 2016). Moreover, the association with sex persisted after adjustment for well-known clinically relevant factors for male suicide (e.g. lethality of self-harm method and mental health conditions) suggesting that hospitalisation may represent an important opportunity to engage at-risk males who are often disengaged from preventive support and healthcare (Stene-Larsen and Reneflot, 2019). The result also highlights the likely gendered influence of psychosocial and other population-level risk factors (Pitman et al., 2012) that were not able to be modelled in this study. Identifying and addressing these issues is particularly important for Aboriginal boys and men who typically do not have access to culturally appropriate services (Canuto et al., 2018) that can help them address additional challenges that may further exacerbate their vulnerabilities to suicidal ideation and self-harm, such as stigma (Smith et al., 2020), discrimination (Haregu et al., 2021) and cultural disconnection (Gibson et al., 2021). A priority for future research should, therefore, be on identifying male-specific modifiable psychosocial risk and protective factors in Aboriginal and non-Aboriginal populations that can inform improvements to hospital management and aftercare that better satisfy the unmet needs of boys and men that are known to hinder help-seeking behaviours and support recovery in the community (Taylor, 2003).
We found no evidence of a difference in the risk of suicide between patients with suicidal ideation only and those with self-harm at index admission. Although this would appear contrary to the evidence that self-harm represents one of the strongest risk factors for suicide (Carroll et al., 2014), it is consistent with findings from a recent systematic review and meta-analysis of suicidal ideation and self-harm (Large et al., 2021). However, this study did find subsequent hospitalisation involving self-harm was associated with a moderate increase in the risk of suicide over time. This suggests that self-harm may be more of a dynamic rather than static risk factor for suicide in the NT. This would be consistent with psychological theories proposing a progression from thinking about suicide to acting repeatedly on those thoughts in ways that elevate the risk of a fatal attempt (Bryan and Rudd, 2016). Because hospital presentations account for only a proportion of suicidal ideation and self-harm in the community (Geulayov et al., 2018), it is, therefore, quite likely that patients in this study may have experienced suicidal ideation and self-harm not captured in the hospital data. Thus, while our findings support recommendations that clinical decision-making should give equal consideration to the suicide risk of suicidal ideation and self-harm (Large et al., 2021), they also emphasise the importance of comprehensive psychosocial assessment in the hospital setting to identify needs, strengths and risks, such as a history of suicidal ideation and self-harm, to inform appropriate management and aftercare that best supports recovery (National Collaborating Centre for Mental Health [NCCMH], 2011a, 2011b). Further research to identify the risk factors for repeat hospital admissions in the NT involving self-harm could, therefore, help to inform improvements to hospital assessment, management, and aftercare and contribute to reducing the risk of suicide in this clinical population.
The presence of diagnoses of severe mental disorders at index admission was the only other clinically relevant factor associated with a higher risk of suicide and this was only observed in the Aboriginal cohort. The results from this study are similar to those from other studies concerning the association between psychosis and suicide risk (Yates et al., 2019). However, some caution is needed with interpreting diagnoses of severe mental disorder in Aboriginal people given the underlying symptoms of these diagnoses are less likely to be related to psychotic illnesses and their more enduring influence on suicide risk that are well established in the evidence (Mishara and Chagnon, 2016). On the contrary, psychotic symptoms and illness in Aboriginal people are more likely to be associated with acute and episodic responses to situational crises and interpersonal conflict (Parker and Milroy, 2003). Furthermore, substance misuse, especially involving alcohol, is known to be a particularly prevalent comorbid condition and predisposing influence of psychotic illness in Aboriginal people (Charlson et al., 2021) that points to contexts of social disadvantage and dysfunction that may also exacerbate the risk of suicidal behaviour (Hunter, 2013). This is partly supported by the high prevalence of comorbid substance misuse and substance-induced psychosis within the category of severe mental illness diagnoses observed in the Aboriginal cohort in this study (see Supplementary Table 1). Additionally, symptoms of apparent psychotic illness (especially auditory hallucinations) observed by clinicians in relation to suicidal ideation and self-harm may be culturally acceptable in the context of responses to some kinds of distress, especially in grief and mourning (Parker, 2010). These considerations reinforce the importance of comprehensive psychosocial assessment, especially with the involvement of Aboriginal mental health workers (Hinton et al., 2014) and family (Parker and Milroy, 2003) who can more appropriately contextualise behaviours and symptoms signalling potential mental illness and suicide risk. Access to culturally appropriate screening for mental disorders in culturally safe hospital settings (Kerrigan et al., 2020) will also help to ensure a proper understanding of the symptomatology of psychotic disorders and their context to inform recommendations for effective treatment of psychotic illness in the community for Aboriginal people who need it.
Strengths and limitations
While this study makes an important contribution to the epidemiology of suicidal behaviours among Aboriginal people using data that reliably records Indigenous status (AIHW, 2013), caution is needed when generalising findings for Aboriginal people given the cultural and social diversity of communities both within the NT and across Australia. However, the implications have been developed with careful consideration of these limitations and reflection on the unique NT context. As is common with longitudinal studies of suicide, the small number of outcomes observed over the lengthy follow-up period in this study means that only the strongest associations will be reliably identified in the analyses. The results have been carefully developed and diagnosed using appropriate methodological approaches to minimise the prospect of biased estimates (Andersen et al., 1996). Care has been taken with interpreting mental health conditions reported in this study that are based on codes that do not distinguish between diagnoses arrived at through formal and comprehensive assessment and those determined through clinician observation and judgement of symptoms. More importantly, while the perspectives of Aboriginal people and the available evidence have been consulted in developing the findings from this study, the reliance on hospital data alone may not capture the range of factors important to caring for and supporting Aboriginal people experiencing suicidal ideation and self-harm. Further qualitative research is needed to address these gaps.
Conclusion
In summary, the absence of strong evidence pointing to clinically modifiable risk factors for suicide suggests that hospitals have a crucial role to play within a public health systems–based approach to prevention in the NT that emphasises greater community-level engagement. A better understanding of male-specific risk and protective factors for suicide, especially for Aboriginal boys and men, is needed to inform more appropriate care in the hospital that improves help-seeking behaviours in the community. Culturally appropriate screening of mental illness among Aboriginal people is needed to distinguish between psychiatric and psychosocial influences of suicidal ideation and self-harm that may require further attention. Identifying risk factors for repeat hospital admission involving self-harm for Aboriginal and non-Aboriginal people is also needed to further clarify targets for prevention. Therefore, an integrated approach to suicide prevention would require comprehensive psychosocial assessment in hospitals to inform properly targeted management and aftercare that can more effectively support recovery and prevent further self-harm in the community. Furthermore, a contextualised understanding of the results for Aboriginal people in this study suggests that efforts to reduce the gap in suicide mortality between Aboriginal and non-Aboriginal people is going to require greater focus on social risk factors and cultural strengths supported by greater investment in Aboriginal-led community-based suicide prevention, such as aftercare, and early intervention to reduce the disproportionate burden of suicidal ideation and self-harm in the first place.
Supplemental Material
sj-docx-1-anp-10.1177_00048674221099822 – Supplemental material for Suicides in Aboriginal and non-Aboriginal people following hospital admission for suicidal ideation and self-harm: A retrospective cohort data linkage study from the Northern Territory
Supplemental material, sj-docx-1-anp-10.1177_00048674221099822 for Suicides in Aboriginal and non-Aboriginal people following hospital admission for suicidal ideation and self-harm: A retrospective cohort data linkage study from the Northern Territory by Bernard Leckning, Rohan Borschmann, Steven Guthridge, Sven R Silburn, Tanja Hirvonen and Gary W Robinson in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
We would like to acknowledge people who have had direct experience of suicide, including those who have attempted suicide and those bereaved by suicide. We would like to thank the advisory group to this study comprising Aboriginal and non-Aboriginal experts with clinical and lived experience for their generous insight and feedback. We thank the NT Department of Health for their support in obtaining and understanding the data for this study. The views expressed in this publication are those of the authors and not necessarily those of the funding body and partners to this study.
Author Contributions
B.L., S.R.S. and G.W.R. were involved in study conception. B.L., R.B., S.R.S., S.G. and G.W.R. were involved in developing the study design and analysis plan. B.L. was responsible for data collection, preparation, and analysis with supervision from S.G. and feedback from R.B., T.H., S.R.S. and G.W.R. B.L. was primary author of the manuscript with revisions provided by R.B., S.G., T.H., S.R.S. and G.W.R.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: B.L. is supported by a research scholarship from the National Suicide Prevention Research Fund administered by Suicide Prevention Australia. R.B. is funded by a National Health and Medical Research Council (NHMRC) Emerging Leadership-2 Investigator Grant (GNT2008073).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.