
Abstract
Objective:
To examine the consequences of alcohol consumption and symptoms of alcohol use disorder during adolescence and later adulthood psychopathology and social outcomes.
Methods:
A longitudinal, prospective birth cohort study, the Christchurch Health and Development Study, was examined across a 35-year period. We estimated the associations between two measures of adolescent alcohol use (volume of alcohol consumed and symptoms of alcohol use disorder) and two later internalising disorders, externalising psychopathology measured by substance use disorders and psychosocial outcomes in adulthood, adjusting for individual and family factors from childhood.
Results:
The pattern of results indicates alcohol symptoms predict internalising disorder in adulthood. Volume of alcohol used in adolescence predicted adult substance use disorders, lower educational attainment and higher risk of welfare benefit receipt in adulthood in fully adjusted models.
Conclusion:
Early consumption of larger volumes of alcohol led to continuation of this pattern in adult life with resulting poorer educational achievement, increased welfare benefit receipt and substance use disorders. Early symptoms of alcohol use disorder, however, led to increased adult levels of mental health disorders. This relationship persisted within a 20-year study period and after adjustment for statistically significant covariate factors. The study shows that early patterns of alcohol use have a direct and specific impact upon adult outcomes.
Introduction
Early life alcohol use has been of interest to researchers, policymakers and society for decades. There seems to be a clear link between early alcohol use and later adult problems, but understanding this relationship is a genuine ‘wicked problem’ (Head, 2008; Rittel and Webber, 1973) that is recognised as essential to address (Kelly et al., 2017). The complexity of understanding the relationship between early alcohol use and later adult alcohol problems has led to both a broad and diverse research base. The difficulty in translating the harms as they are currently understood into interventions that mitigate against these harms is clear (Rehm et al., 2009; Whiteford et al., 2013). On the basis of these findings, public health strategies have been developed although reviews have suggested a key research question that remains outstanding is understanding how reducing underage drinking leads to ‘ … carryover benefits in adult life’ (Harding et al., 2016).
Many early large-scale studies find correlations between early alcohol use and later alcohol use disorder (AUD), however defined. Three large US studies, the Investigation of the National Epidemiologic Survey on Alcohol and Related Conditions (NESARC) (Dawson et al., 2008; Hingson et al., 2006), the National Longitudinal Alcohol Epidemiologic Survey (NLAES) (Grant and Dawson, 1997) and National Survey of Labour Market Experience in Youth (NLSY) (Grant et al., 2001) all found correlations between early alcohol use, usually described as a first drink (not sip or taste) and later alcohol problems. These studies indicate a clear link but have a number of limiting factors. Being US-based questions their generalisability to societies other than the United States, as there are significant variations in the social and cultural elements of alcohol use. Each of these studies had limited time points for data collection, limiting their capacity to adequately take into account multiple covariates that may be time sensitive. Complicating this is the assessment of age of first drink that has a high risk of recall bias (Maimaris and McCambridge, 2014) with most participants being years beyond this time at age of first interview. In addition, each of these studies examined only the impact of early alcohol use on later alcohol problems, limiting the understanding of impact on other mental health or psychosocial problems, reducing the utility of their findings.
Furthermore, these studies do not provide any indication of what reductions in early alcohol use may be of benefit or what benefits these reductions may have. For example, it is not clear from these early studies if raising the age for drinking (and presumably the age of first drinking) would have an impact or if individual efforts to reduce symptoms or minimise overall volumes of alcohol consumed in individuals is more likely to lead to sustained change. It is also not clear what positive changes to expect, or conversely what negative adult outcomes are targets for intervention. This stream of research enables us to say with some confidence that early alcohol use leads to later alcohol problems, but little beyond that.
The most common metrics to measure alcohol use in the literature are volume consumed or symptoms of AUD (or meeting criteria for AUD). These two indices are linked, at least at the extreme poles of both (Rehm et al., 2013) but may indicate substantially differing alcohol syndromes, with equally different trajectories (Boden et al., 2019) as is the case with other metrics of early life use of alcohol (Newton-Howes et al., 2019). Understanding both symptoms and volumes in adolescent use may enable differing prognostic outcomes to be identified. Furthermore, in order to control for overlapping variance in these measures, both variables need to be modelled simultaneously. This has yet to be done in any large scale, or general population cohort.
Although adolescent AUD diagnosis is unstable, with half of adolescents with an AUD diagnosis no longer meeting criteria for the disorder by their mid-twenties (Wells et al., 2006), these symptoms may provide differing insights as compared to age of first drink. For example, early life symptoms of mental disorder may herald a predisposition to mental disorder, or mental disorder subtypes, such as externalising disorders. As of yet this remains understudied (Eaton et al., 2011; Newton-Howes et al., 2015). Similarly, understanding psychosocial outcomes from early alcohol use is of greater relevance to individuals and policy makers. An understanding of the way in which early consumption patterns or AUD symptoms relate to outcomes such as adult welfare benefit receipt is of significantly greater value to policymakers than simply knowing that early alcohol use relates to later alcohol problems.
Compared to the previously noted study designs, cohort studies that aim to describe the course of early alcohol use are less common. For example, Tuithof et al. ( 2014) used a cohort to examine relapse in a general population as opposed to an ‘enriched’ addiction population. They noted that relapse rates of AUD were significantly lower in their general population sample compared to treatment samples (Trim et al., 2013). This study, although overcoming some of the limitations described above, was still impacted by recall bias and a single early point of focus. Seeley et al. (2019) examined a cohort from 16 to 30 years using a population sample; however, findings were limited to alcohol relapse from a basis of early AUD symptoms, without a measure of quantity of alcohol consumed. Furthermore, data were collected at three time points only, limiting the covariates available. This, and the inclusion of general and treatment populations at baseline (Boschloo et al., 2012), limits cohort data with respect to outcomes other than relapse. Examining general population cohorts to understand the association between simultaneous measures of early alcohol consumption levels and problems, and later psychopathology and social outcomes, has not previously been studied in cohorts with prospective questioning of alcohol use, and repeated measures data to account for continuity and change over time.
In addition, despite the relative methodological weaknesses, it seems highly likely that early alcohol use links to later AUD, an externalising problem (Newton-Howes et al., 2015), but the links to internalising problems, such as depression and anxiety, are far less clear. The work undertaken to examine this link to date is largely cross sectional (Buydens-Branchey et al., 1989). Internalising problems such as depression and anxiety are related to significant adult morbidity, with depression on track to be the disorder with this single greatest impact of quality adjusted life years (QALYs) lost (World Health Organization, 2017). If a link exists between adolescent alcohol use and later depression and anxiety disorders, the archetype internalising disorders, this too becomes an important outcome in adulthood to understand. What is needed to address all of these issues is a study measuring both amounts of alcohol consumed and problems with alcohol simultaneously, accounting for a range of potential confounding factors, and with repeated data collection points for outcomes across several domains of adult functioning.
Against this background, we have used data from a longitudinal birth cohort studied to age 35 (The Christchurch Health and Development Study [CHDS]) in order to further understand this ‘wicked problem’. In this analysis, we examined the associations between two adolescent alcohol variables: symptoms of AUD and volumes of alcohol consumed; and three adult domains of interest: internalising psychopathology (major depression and anxiety disorders), externalising psychopathology (substance use disorder) and psychosocial functioning (educational attainment and welfare benefit receipt).
Methods
In order to examine these interrelated questions, we estimated the associations between two measures of adolescent alcohol use (amount of alcohol consumed; symptoms of AUD) and a series of internalising, externalising and psychosocial outcomes in adulthood, adjusting for a set of individual, behavioural and family factors know to be associated with alcohol use.
Participants
The data were gathered from the CHDS. In this study, a birth cohort of 1265 children (635 males, 630 females) born in the Christchurch (New Zealand) urban region in mid-1977 has been studied at birth, 4 months, 1 year and annually to age 16 years, and again at 18, 21, 25, 30 and 35 years (Fergusson et al., 1989; Fergusson and Horwood, 2001). The original cohort comprised 97% of all individuals born in Christchurch during the study entry period (97% response rate). All study information was collected on the basis of signed consent from study participants and is fully confidential. All aspects of the study have been approved by the Canterbury (NZ) Ethics Committee. Sample sizes ranged from 1025 (age 18) to 962 (age 35), representing 79–82% of the surviving sample at each observation. The primary driver of sample loss over the course of the study has been emigration from New Zealand, with loss of contact. CHDS research has been approved by the Southern Health and Disability Ethics Committee (New Zealand).
Outcome measures: lifetime psychopathology and psychosocial measures
Data collected in adulthood (from 18 years of age) were used to create the following outcome measures:
Internalising disorder (18–35 years). Based on the Composite International Diagnostic Interview (CIDI; Smeets and Dingemans, 1993) at ages 21, 25, 30 and 35 years, cohort members were classified as to whether they met Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV) criteria for major depression and anxiety disorder over the intervals 18–21, 21–25, 25–30 and 30–35 years. Participants who met criteria for either disorder during any assessment period were classified as having that disorder.
Externalising disorder (18–35 years). Using information from the CIDI, cohort members were classified as meeting DSM-IV criteria for AUD, nicotine dependence, cannabis dependence and other drug dependence over the intervals 18–21, 21–25, 25–30 and 30–35 years. Again, participants who met the criteria for any disorder during any assessment period were classified as having that disorder.
Psychosocial outcome: Educational attainment. At ages 21, 25, 30 and 35 years, cohort members were asked a series of questions concerning their educational activities, enrolment in educational programmes and any qualifications they had obtained. This information was used to create a comprehensive measure of educational qualifications obtained to age 35 years, classified according to a 7-point scale ranging from no qualifications to University degree attainment.
Psychosocial outcome: Welfare benefit receipt. At ages 25, 30 and 35, cohort members were asked detailed questions concerning their receipt of social welfare benefits since the previous assessment. Cohort members who reported receiving one or more benefit during an assessment period were classified as receiving welfare benefits during that period (21–25; 25–30; 30–35 years). For the purposes of the present measure, cohort members who reported receipt of at least one benefit in any assessment period were classified as having been in receipt of welfare benefits.
Primary alcohol-related predictors (amount of alcohol consumed; alcohol problems), ages 14, 15 and 16 years
As part of the assessment at ages 14, 15 and 16 years, cohort members were asked a series of questions concerning their alcohol consumption, and any problems they may have had relating to alcohol consumption. The questions concerning problems with alcohol were based on the Diagnostic Interview Schedule for Children (DISC) (Costello et al., 1982) at ages 15 and 16 years, in order to obtain information pertaining to Diagnostic and Statistical Manual of Mental Disorders (3rd ed., revised; DSM-III-R) (ages 15 and 16) (American Psychiatric Association, 1987) symptoms of alcohol abuse/alcohol dependence (AUD). These data provide a count measure of the number of symptoms of AUD during each 12-month period following the previous assessment. Therefore, the present analyses used two alcohol use measures:
Amount of alcohol consumed. For the 12 months prior to each assessment at ages 14, 15 and 16, the amount of alcohol consumed by cohort members in a ‘typical’ drinking session was the basis for the first primary alcohol–related predictor. These data were summed across all three assessments and then used to classify participants on a three-level measure representing the lowest 80%, 81–95% and finally the top 5% on the measure.
Number of problems with alcohol reported. Again, for the 12 months prior to each assessment at ages 15 and 16 years, the number of problems stemming from alcohol consumption was the basis of the second primary alcohol–related predictor. These data were summed across the two assessments and then used to classify participants on a three-level measure representing the lowest 80%, 81–95% and finally the top 5% on the measure.
Covariate factors
Twenty-one covariate factors were included in the analyses, on the basis that they were (a) used in a prior analysis of the age of first alcohol use in the CHDS cohort (Fergusson et al., 1994b) or (b) have been found to be related to substance use outcomes in other studies of the CHDS cohort (Fergusson et al., 1993, 1994a, 1995, 2007, 2008; Lynskey et al., 1998). These fell into three broad domains including socioeconomic/demographic, personality/behavioural and family/parental. There are described in detail in the online supplement and are listed in Table 2.
Statistical analyses
The first set of analyses (shown in Table 3) modelled the unadjusted associations between the two primary alcohol–related predictors and the adult outcomes using logistic regression (for dichotomous outcomes) and negative binomial regression (for the measure of level of education). Both predictors were entered into the model simultaneously. These models were of the form

where Y is either the log odds (for dichotomous measures) or the log rate (for the educational achievement measure) for person i; B0 is the intercept term; ∑BijXij represented the value for the predictor for person i; and ei is a random error term.
In the second step of the analyses, the models shown above were extended to include the set of covariate factors drawn from those factors found to be statistically significantly correlated (p < 0.05) with the two primary alcohol–related predictors noted above. These models were of the form

where ∑BijXij represented the set of covariate factors for person i. Covariate factors were entered into the model using methods of forward and backward variable substitution in order to obtain stable and parsimonious models. All models were fitted using SAS 9.4 (SAS Institute Inc, 1999).
Results
Bivariate associations between adolescent alcohol-related predictors and lifetime mental health, substance use, education and welfare outcomes (spanning ages 18–35 years)
Table 1 shows the cohort divided into three groups across two measures. The first is a measure of the amount of alcohol consumed during the 12 months prior to ages 14, 15 and 16 years, classified as the lowest 80%, 81–95% and finally the top 5% on the measure. The second is a measure of symptoms of alcohol dependence at ages 15 and 16 years, again classified as the lowest 80%, 81–95% and finally the top 5% on the measure. Table 1 shows the percentage of each group meeting criteria for each of several mental health and substance use disorders over the period 18 to 35 years, as well as the mean score on the measure of educational attainment, and the percentage of each group who had been in receipt of a welfare benefit at some point during the period 21 to 35 years. Linear tests of association were derived from one-way analysis of variance (ANOVA). Table 1 shows that:
Associations between alcohol-related predictors in adolescence (ages 14–16) and lifetime mental health, substance use, education and welfare dependence outcomes (from ages 18 to 35 years).
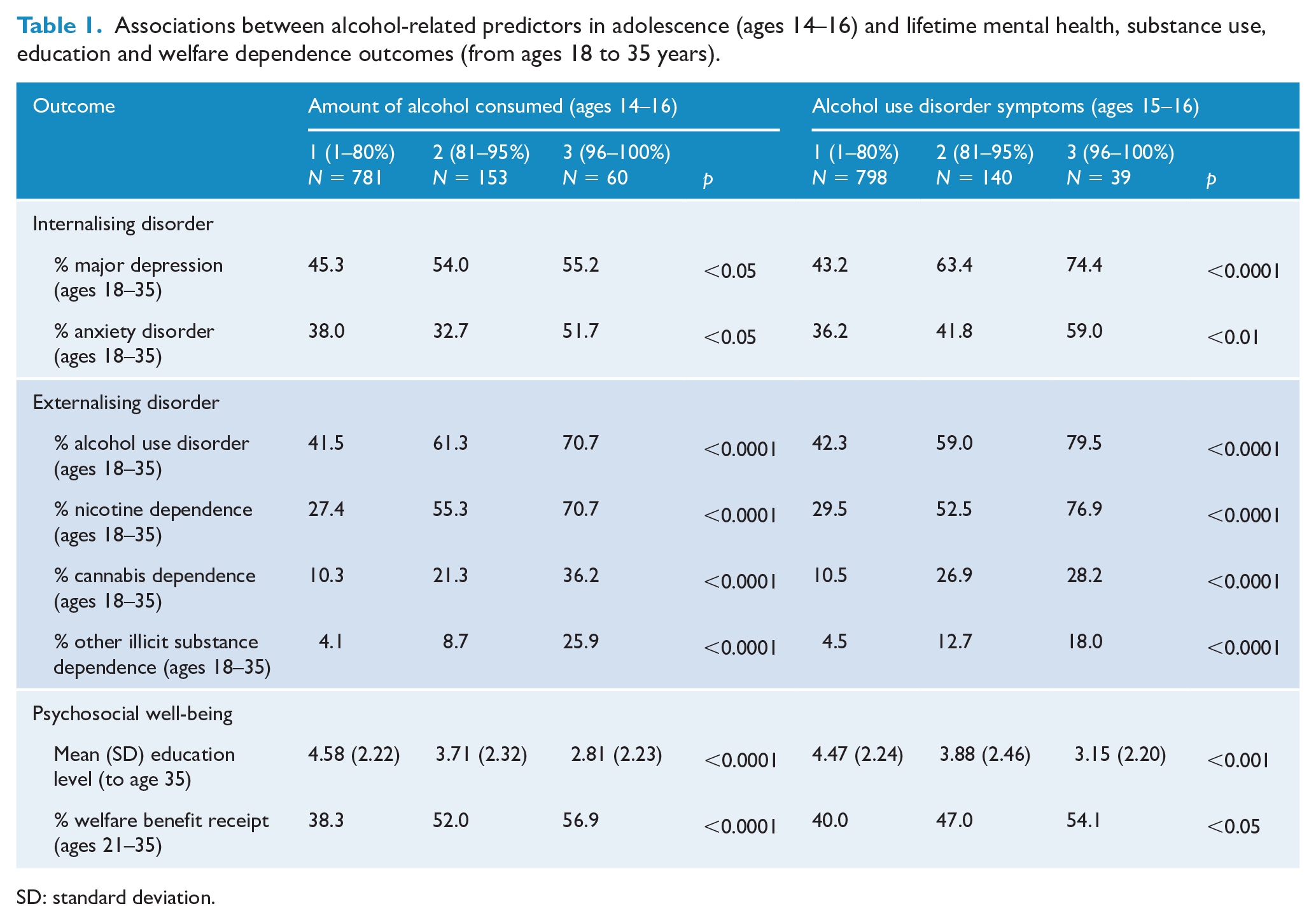
SD: standard deviation.
Increasing levels of both alcohol consumption and symptoms of AUD were associated with significantly (p < 0.05) higher rates of internalising disorder.
Alcohol consumption and symptoms AUD were associated with significantly (p < 0.0001) higher risks of externalising disorder from age 18 to age 35.
Both alcohol consumption and level of alcohol symptoms were associated with significantly poorer psychosocial outcomes, lower levels of educational attainment to age 35 (p < 0.001) and significantly greater risk of receiving welfare benefits (p < 0.05).
Bivariate associations between covariate factors and alcohol-related predictors (ages 14–16)
As noted in section ‘Methods’, it could be argued that the associations between the alcohol-related predictors and life course outcomes shown in Table 1 could be due to the influence of a series of individual, family and behaviour factors to which cohort members were exposed during childhood and early adolescence. In order to examine this issue, a series of potential covariate factors were extracted from the CHDS database, and the bivariate associations between these and alcohol-related predictors were estimated using Pearson product–moment correlations. The results of these analyses are shown in Table 2, which displays the correlation coefficient for each association, and tests of significance. Table 2 shows that, almost without exception, there were statistically significant correlations between alcohol-related predictors in adolescence and a range of sociodemographic, family functioning and individual factors in childhood and early adolescence. This pattern of correlations clearly shows that those reporting higher levels of alcohol consumption and a greater number of symptoms of AUD in adolescence were exposed to higher levels of adversity and risk in childhood and early adolescence. An exception to this pattern was for family living standards and socioeconomic status (SES), both of which showed positive correlations with higher levels of alcohol consumption and alcohol symptoms. This pattern may reflect a socioeconomic gradient in which young people from more affluent families were able to obtain and consume alcohol more easily.
Correlation coefficients for associations between covariates and alcohol-related predictors in adolescence.
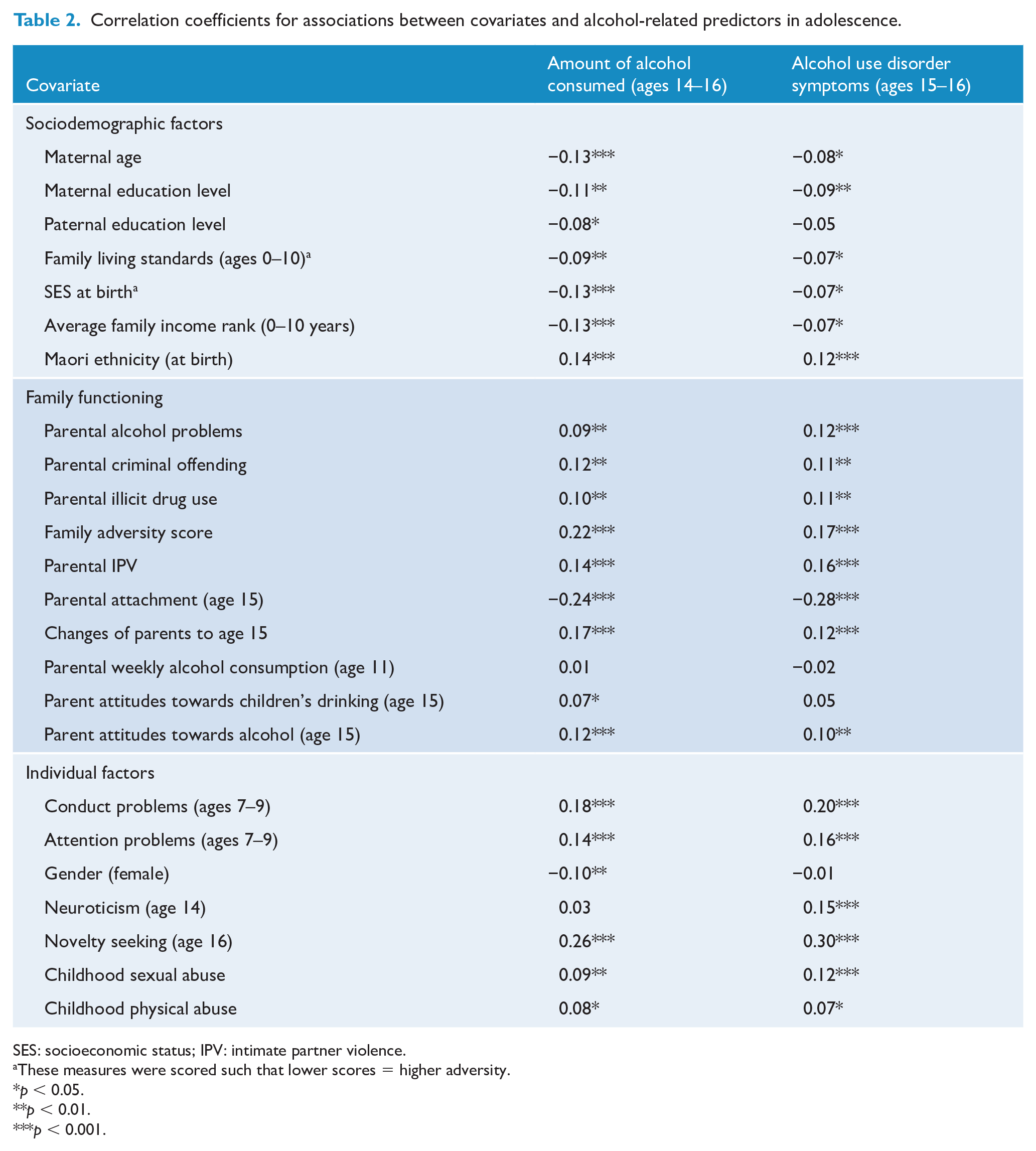
SES: socioeconomic status; IPV: intimate partner violence.
These measures were scored such that lower scores = higher adversity.
p < 0.05.
p < 0.01.
p < 0.001.
Multivariate associations between alcohol-related predictors in adolescence (ages 14–16 years) and lifetime internalising disorder, externalising disorder and psychosocial well-being (spanning ages 18–35 years), after adjustment for covariate factors
In the next step of the analyses, the pair of alcohol-related predictors were entered into a series of logistic regression models, in which lifetime mental health and substance use disorders and welfare benefit receipt were modelled as a function of both adolescent alcohol consumption and symptoms of AUD. Furthermore, a negative binomial model was fitted that modelled educational attainment as a function of both adolescent alcohol consumption and symptoms of AUD.
In the final step of the analyses, these models were extended to include the set of covariate factors displayed in Table 2. The results of both of these modelling steps are shown in Table 3, which shows the parameter estimates and standard errors for the associations between alcohol-related predictors and each outcome, both in the unadjusted (both alcohol-related predictors only) and adjusted models (both alcohol-related predictors and the set of statistically significant covariate factors). This modelling strategy allowed us to directly compare the relative magnitude and significance of the effect of both predictors (alcohol consumption; alcohol disorder symptoms) in unadjusted and adjusted models. Table 3 shows that:
For internalising disorder (major depression and anxiety disorder), both the unadjusted and adjusted models show that the amount of alcohol consumed during the period 14–16 years was no longer a statistically significant predictor of lifetime mental health disorder. On the other hand, three of the four models (the adjusted model predicting anxiety disorder) found a statistically significant (p < 0.05) association between AUD symptoms and internalising disorders in adulthood.
For externalising disorder outcomes (alcohol, nicotine, cannabis and other illicit drugs), the opposite pattern was found, in which the amount of alcohol consumed in adolescence showed robust and statistically significant (p < 0.05) associations with each outcome in both unadjusted and adjusted models. However, while symptoms of alcohol dependence were robust and statistically significant (p < 0.05) predictors for alcohol dependence and nicotine dependence, they were not significantly associated with cannabis dependence in the adjusted model, or with other illicit drug dependence in either model.
As with substance use disorder outcomes, the amount of alcohol consumed in adolescence was significantly (p < 0.05) associated with educational attainment and welfare benefit receipt in both unadjusted and adjusted models. However, symptoms of AUD in adolescence were not significantly associated with educational achievement or welfare benefit receipt in either model.
Parameter estimates for the associations between alcohol-related predictors in adolescence (ages 14–16) and lifetime mental health, substance use, education and welfare dependence outcomes (from ages 21 to 35 years), before and after adjustment for covariate factors.
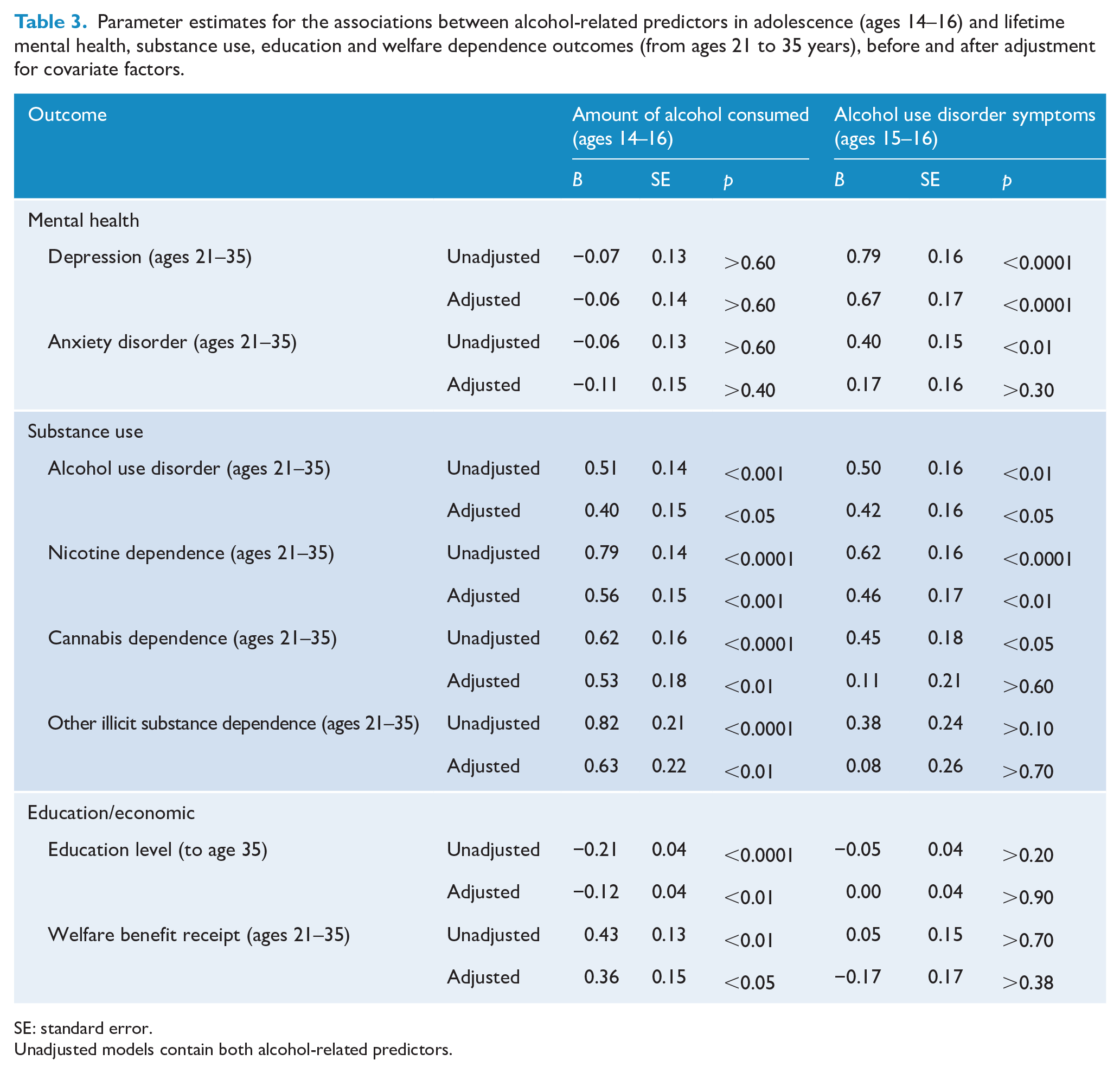
SE: standard error.
Unadjusted models contain both alcohol-related predictors.
Across the eight models, statistically significant (p < 0.05) covariate factors included maternal age; maternal and paternal education level; SES at birth; family living standards; parental illicit drug use; family adversity; parental intimate partner violence; gender; childhood conduct and attention problems; novelty seeking; neuroticism; childhood sexual abuse; and childhood physical abuse.
This pattern of results suggests that while early indications (symptoms) of AUD were more predictive of greater risk of internalising disorder in adulthood than the amount of alcohol consumed, this pattern reversed for increased risk of substance use disorders, lower educational attainment and higher risk of welfare benefit receipt.
Discussion
To the authors’ knowledge, this is the first cohort study with contemporaneously collected data on alcohol use that has examined two metrics of adolescent alcohol use simultaneously, volume of consumption and AUD symptoms, and estimated the associations between these and future psychopathology and psychosocial well-being. By undertaking simultaneous modelling for outcomes, two different patterns of adult problems emerge. For those who consumed more alcohol by volume in adolescence, the risk of later externalising disorder, namely substance use disorder, and psychosocial impairment significantly increased. On the other hand, those who displayed more symptoms of alcohol dependence had an increased future risk of internalising disorder, namely depression and anxiety disorders. Controlling for a range of confounding factors measured in childhood and adolescence did not materially alter this pattern of associations.
It is of interest that those adolescents showing emergent AUD in the form of symptoms of AUD go on to be at greater risk for internalising disorder, rather than externalising disorder. This is somewhat counterintuitive, as most prior research suggests a link between early alcohol use and externalising problems (Kotov et al., 2017; Krueger et al., 2005; Tackett et al., 2009). It is likely because prior research measures consumption volumes, or first use of alcohol, not symptoms. It is likely that early first use and volume of alcohol used per session are more closely aligned than age of first drink and alcohol dependence symptoms. If this is the case, then this research linking increasing volume with later alcohol dependence and externalising disorder would be concordant with these earlier findings. The reasons for the link between early alcohol symptoms and later internalising disorder are not entirely clear, but possibly suggest the emergence of psychopathology in early life is an indicator of a greater tendency to overall psychopathology, or a higher ‘p’ factor (Caspi et al., 2013) as opposed to a link between alcohol symptoms and depression per se. Further research is needed to more clearly elucidate these linkages.
This study builds on the large body of literature that considers the potential outcomes from early alcohol use, providing methodological rigour and new findings. The analysis of a large, prospective, general population cohort overcomes issues pertaining to recall bias, error of measurement and confounding from multiple potential sources can be accounted for. The longitudinal design allows for the possibility that these associations may be causal in nature. The fact that findings pertain to a period within a 20 years suggests they are robust and likely have a significant effect over the life course (Phillips and Goodman, 2004).
Like all designs this study is limited by the methods and data used. Although a wide array of potential covariates were accounted for, it is not possible to ensure there are no other potential factors of significance. Data collection points in adolescents are also close, and this may impact on early interrelation of various factors of interest (such as alcohol use and childhood conduct). Further welfare receipt was only measured from age 21, preventing examination of this at an earlier time point. This, however, provides greater temporal distance between this outcome and the exposure, reducing the risk of confounding. Of note we did not account for genetic variants or neurobiological variation which may play an important role in the aetiology of addiction (Volkow et al., 2016). The population examined also limits the study. The birth cohort is largely a European (87%) and urban group, and it is unclear if these findings generalise into other population groups. Also the diagnosis of alcohol problems has evolved over time, with Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5) and DSM-IV having some dissimilarities in the manner in which AUD is conceptualised and assessed. There is also the use of a single alcohol use measure, with the potential for refinement in early alcohol use metrics. Although a more fine-grained approach to alcohol use in adolescents is possible, it becomes increasingly likely that any signal will be lost to noise over time. This is an issue with any study that examines early life events and later outcomes over a considerable period of time. We noted the use of volume, but not frequency, as the metric for alcohol consumed. This may have led to more heterogeneous groupings and therefore suggests the patterns found are robust, as greater precision in the groups would increase the signal from the data.
The two observed patterns of later problems, each dependent on an adolescent measure of alcohol-related behaviour, inform further research of the importance of measuring both symptoms and consumption volumes as these appear to be associated with specific patterns of outcome. Furthermore, it suggests the possibility of the emergence of a more general psychopathology attribute early in life, an inference supported by other data (Patalay et al., 2015). If this is the case, this work supports the idea higher psychopathology in early life predisposes to psychopathology in later life, in a way described as being similar to the ‘g’ factor for general intelligence (Gottfredson, 1998). A further implication of this study is the need for caution in generalising potential causal inferences from cross-sectional or repeated cross-sectional studies. Although these databases provide a rich understanding of the landscape of adolescent alcohol use and later adult problems, generally from their large sample size, they lack the depth of data to draw out the more subtle interactions and cannot account for multiple potential confounding effects. This research offers understanding both in the potential development of psychopathology over time and how early-onset alcohol use can inform us the potential risks to later mental health and psychosocial problems.
Supplemental Material
EASAVALMHAPO_supplement_260320 – Supplemental material for Alcohol use in adolescents and adult psychopathology and social outcomes: Findings from a 35-year cohort study
Supplemental material, EASAVALMHAPO_supplement_260320 for Alcohol use in adolescents and adult psychopathology and social outcomes: Findings from a 35-year cohort study by Joseph Boden, Sarah Blair and Giles Newton-Howes in Australian & New Zealand Journal of Psychiatry
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was funded by a grant from the Health Promotion Agency, New Zealand, and by the Health Research Council of New Zealand (Programme Grant 16/600).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.