
Abstract
Objectives:
The COVID-19 pandemic poses significant risks to the vulnerable patient population supported by community mental health (CMH) teams in South Australia. This paper describes a plan developed to understand and mitigate these risks.
Methods:
Public health and psychiatric literature was reviewed and clinicians in CMH teams and infectious disease were consulted. Key risks posed by COVID-19 to CMH patients were identified and mitigation plans were prepared.
Results:
A public health response plan for CMH teams was developed to support vulnerable individuals and respond to the COVID-19 pandemic. This plan will be reviewed regularly to respond to changes in public health recommendations, research findings and feedback from patients and clinicians.
Conclusions:
The strategic response plan developed to address risks to vulnerable patients from COVID-19 can assist other CMH services in managing the COVID-19 pandemic.
Coronavirus disease 2019 (COVID-19) is an infectious disease caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). First identified in December 2019, COVID-19 was declared a pandemic by the World Health Organisation (WHO) in March 2020. 1 Individuals with cardiovascular disease, uncontrolled hypertension, diabetes and respiratory disease have been found to be more vulnerable, with increased risk of respiratory complications and death. 2
Since the first reported case in Australia on 25 January 2020, significant efforts have been made on state, national and international levels to limit the spread and impact of the illness. These include travel bans and social distancing, with a reduction in cases but widespread effects on community functioning. Significant psychological consequences of the pandemic and resultant social upheaval require attention, particularly for the most vulnerable.
Community mental health (CMH) teams in the Northern Adelaide Local Health Network (NALHN) serve a highly vulnerable patient population. In 2016, the City of Playford was ranked as one of the most disadvantaged urban local government areas in Australia. 3 Determinants of poor mental and physical health include poor educational attainment, high unemployment, financial insecurity, mortgage and rental stress, over- and under-nutrition, unsafe neighbourhoods, and high rates of domestic violence and drug and alcohol abuse. 4 Socio-economically patterned disease cascades 5 are evident, with the outcomes of transgenerational trauma and social marginalisation seen in levels of psychiatric morbidity and 10-year life expectancy gap compared to those living in Adelaide’s least disadvantaged suburbs. 6
The majority of people supported by the CMH service have diagnoses of chronic schizophrenia and other serious mental illnesses (SMI) including major affective disorders and borderline personality disorder, often complicated by comorbid substance abuse and physical comorbidity. Primary mental health disorders increase the risk of infections including pneumonia. 7 This has been linked to the use of medications increasing cardiometabolic risk, 8 high prevalence of smoking 9 and substance abuse, 10 and higher rates of medical comorbidities such as obesity, diabetes, cancer and cardiovascular disease. 11 Clozapine, in particular, is associated with pneumonia secondary to sialorrhea and risk of aspiration. 12 These factors increase the risk of more serious illness and mortality from COVID-19.
In addition to direct medical risk, there is concern about the ability of people with SMI to engage in public health measures. Cognitive impairment, a core feature of schizophrenia, can affect the ability to understand and think critically about information, which may lead to difficulty adhering to health advice. Disorganised behaviour may increase risk of disease transmission. Positive symptoms of schizophrenia may be exacerbated, with social distancing, increased isolation and conspiracy theories leading to increased distress and anxiety through intensified delusional beliefs.
Negative symptoms of schizophrenia may lead to neglect of physical health and protective measures, and lack of insight poses another challenge through mistrust of services. However, Maguire et al. 13 found people with schizophrenia reported willingness to adopt protective measures during the 2009 H1N1 pandemic, although at lower rates compared to the general population. A study of risk perception in people with schizophrenia found that some degree of anxiety may increase likelihood of considering protective measures, but too high a level of concurrent anxiety resulted in individuals feeling less likely to utilise meaures. 14 Engagement and education is therefore critical.
It has been suggested that pre-existing mental health conditions would increase the risk of psychological distress during the pandemic. 15 Changes in routine and psychosocial stressors could increase the risk of relapse in bipolar disorder and psychotic disorders, exacerbate anxiety disorders such as illness anxiety and obsessive compulsive disorder, and precipitate situational crises in those with underlying personality vulnerabilities.
This is particularly concerning in the face of social change and significant decline in the economy. In 2016, youth unemployment in the City of Playford was 23.5%, with some of its suburbs recording rates as high as 50%–60%, 16 further compounded by the 2017 closure of car-maker Holden’s local manufacturing site. In the wake of COVID-19, mass scale job loss, particularly of younger casual workers, is likely to worsen conditions further with implications for mental health and suicide risk. 17 People with SMI are likely to be rendered more vulnerable, further increasing their risk of homelessness, 18 an additional challenge for follow-up, risk of transmission and mortality.
Finally, the direct and indirect impacts on mental health of COVID-19 are unclear, both in the short term and long term. Elevated levels of depression, anxiety and post-traumatic symptoms have been found a year after exposure to SARS 19 and quarantine has been linked to post-traumatic stress symptoms, confusion and anger. 20 For others, such as those with social anxiety, an alleviation of usual pressures may bring short-term relief. There is much still to be learnt about the neuropsychiatric sequalae of COVID-19 infection, with consideration given to the impact infection and treatment may have on precipitating or exacerbating psychosis.21,22 For those already affected by SMI, the impacts of further uncertainty and loss may be especially profound.
The aim of this paper was to highlight some of these considerations and the strategies put in place in CMH teams in NALHN to manage patient care during the pandemic, in the context of significant ongoing community disadvantage.
Methods
The NALHN Mental Health Service has a catchment population of 350,000, with three CMH teams supporting the region.
As COVID-19 cases began to rise in Adelaide, health service management, consultant psychiatrists and CMH team leaders worked together to develop a plan to manage the risks of this vulnerable population. Potential concerns and responses were collated, relevant public health and psychiatric literature were reviewed, and an infectious disease specialist (MB) was consulted. A summary of recommendations was devised.
Results
A public health response document was developed, identifying five key areas to support vulnerable individuals during the COVID-19 pandemic (Figure 1).
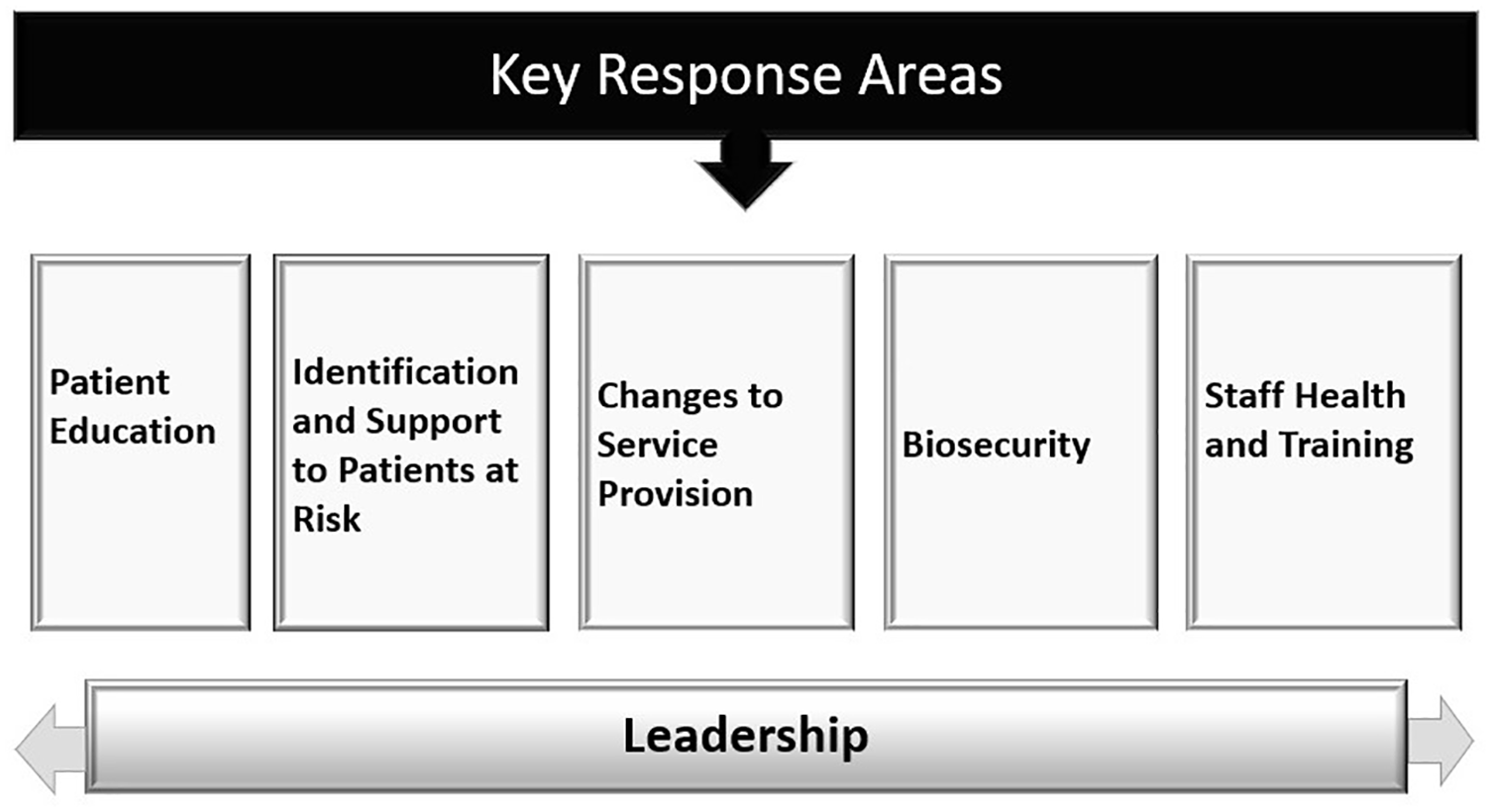
Key response areas.
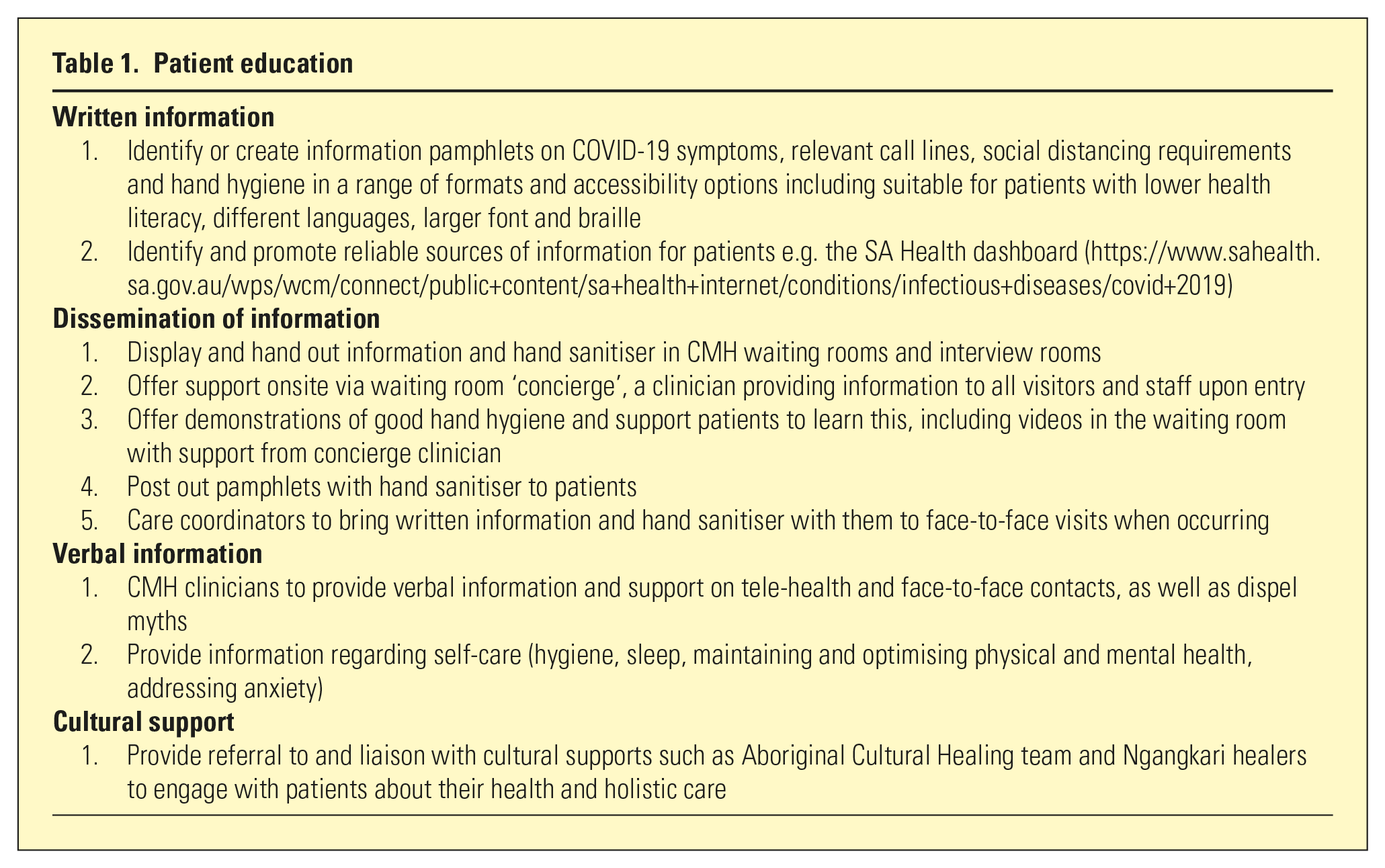
To provide accessible and consistent health messaging, educational strategies for patients were implemented (Table 1) and a pamphlet was adapted from Anglicare, drawn from SA Health and WHO recommendations (Figure 2).
Patient education
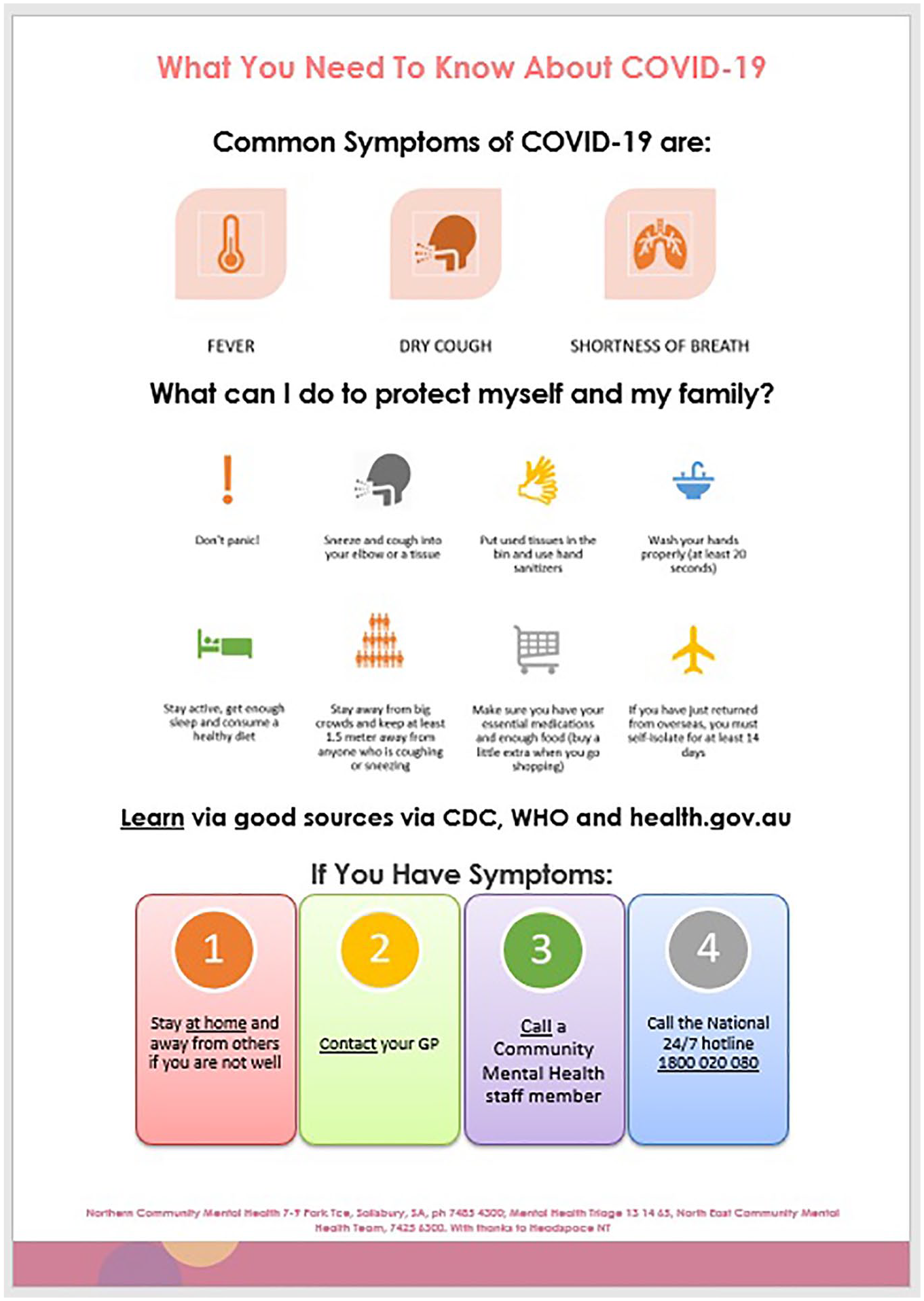
COVID-19 patient information pamphlet.
Identification of and support to vulnerable patients was key (Table 2). Vulnerable patients were identified based on:
(i) Medical vulnerability due to chronic medical comorbidities. An alert on the medical record was adopted to flag and monitor those deemed to be at medical risk from COVID-19;
(ii) Socio-economic and psychiatric vulnerability (homelessness, significant functional impairment, unstable psychiatric illness).
Identification and support of patients at risk of COVID-19 complications
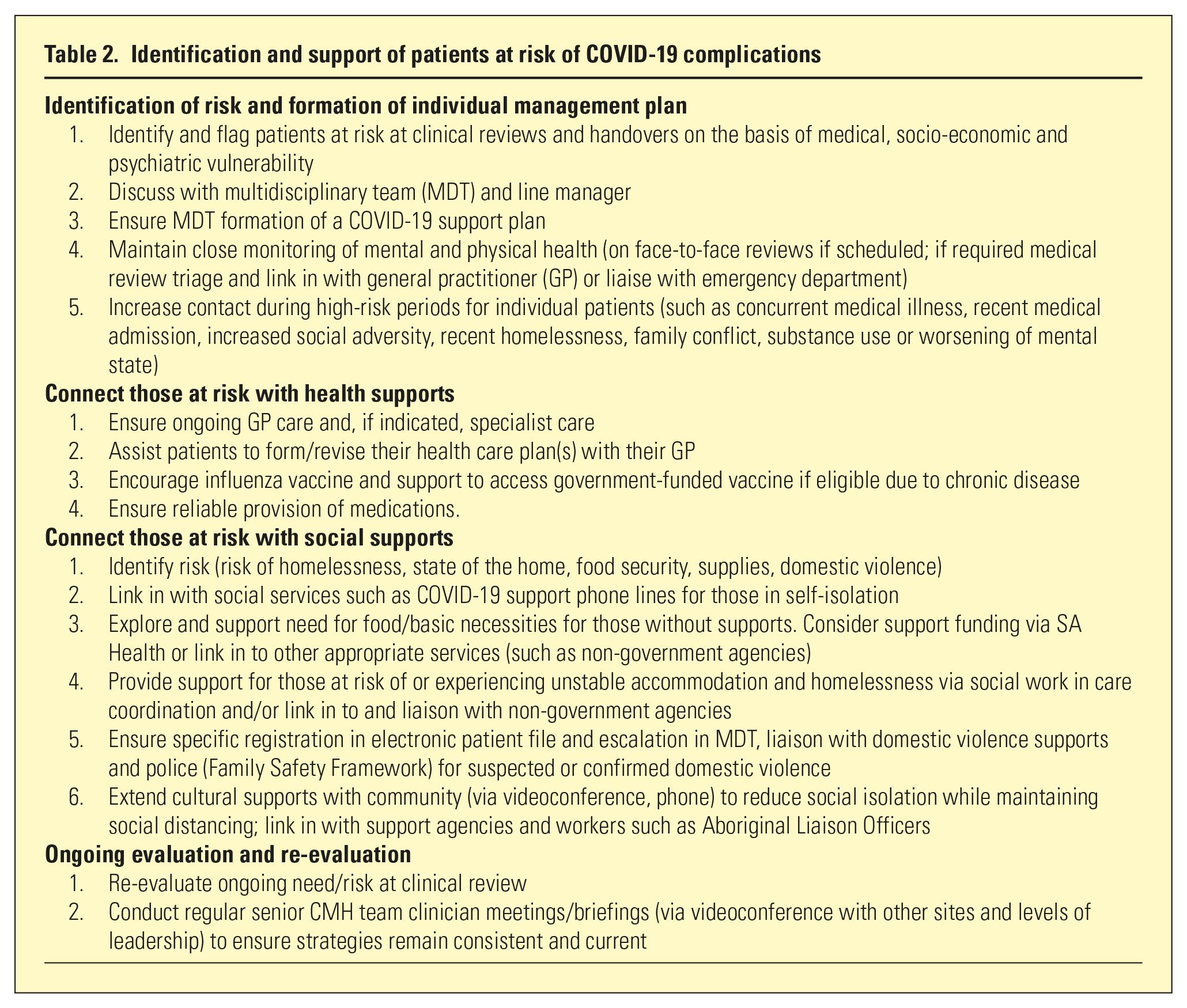
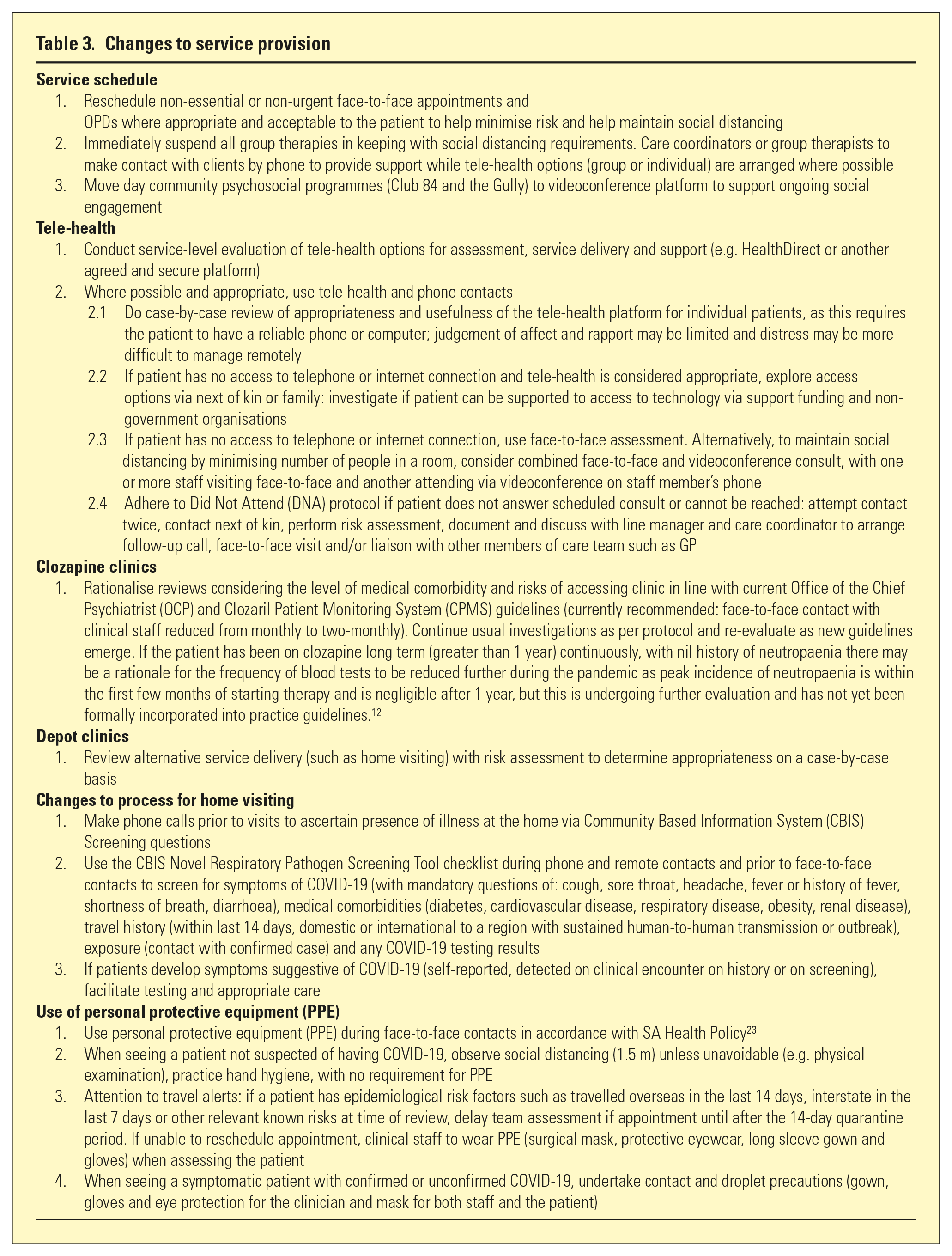
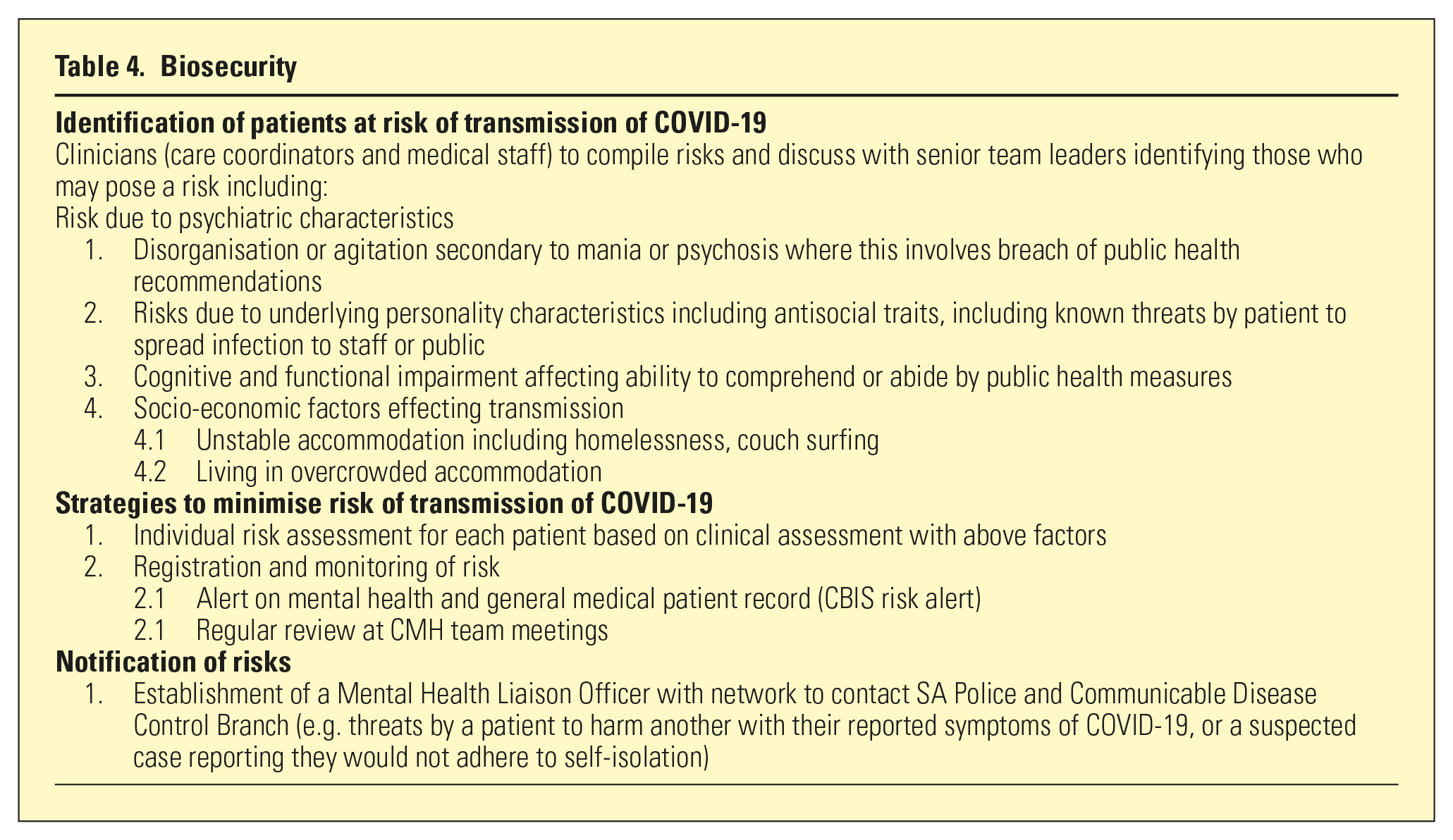
Strategies including development of individual plans and connection to health and social supports were implemented. Changes to service provision were required to meet the challenges of the pandemic, including use of tele-health and specific COVID-related considerations for outpatient programmes and home visits (Table 3). Patients with an increased risk of transmitting COVID-19 were also identified and strategies were formed to manage these risks (Table 4).
Changes to service provision
Biosecurity
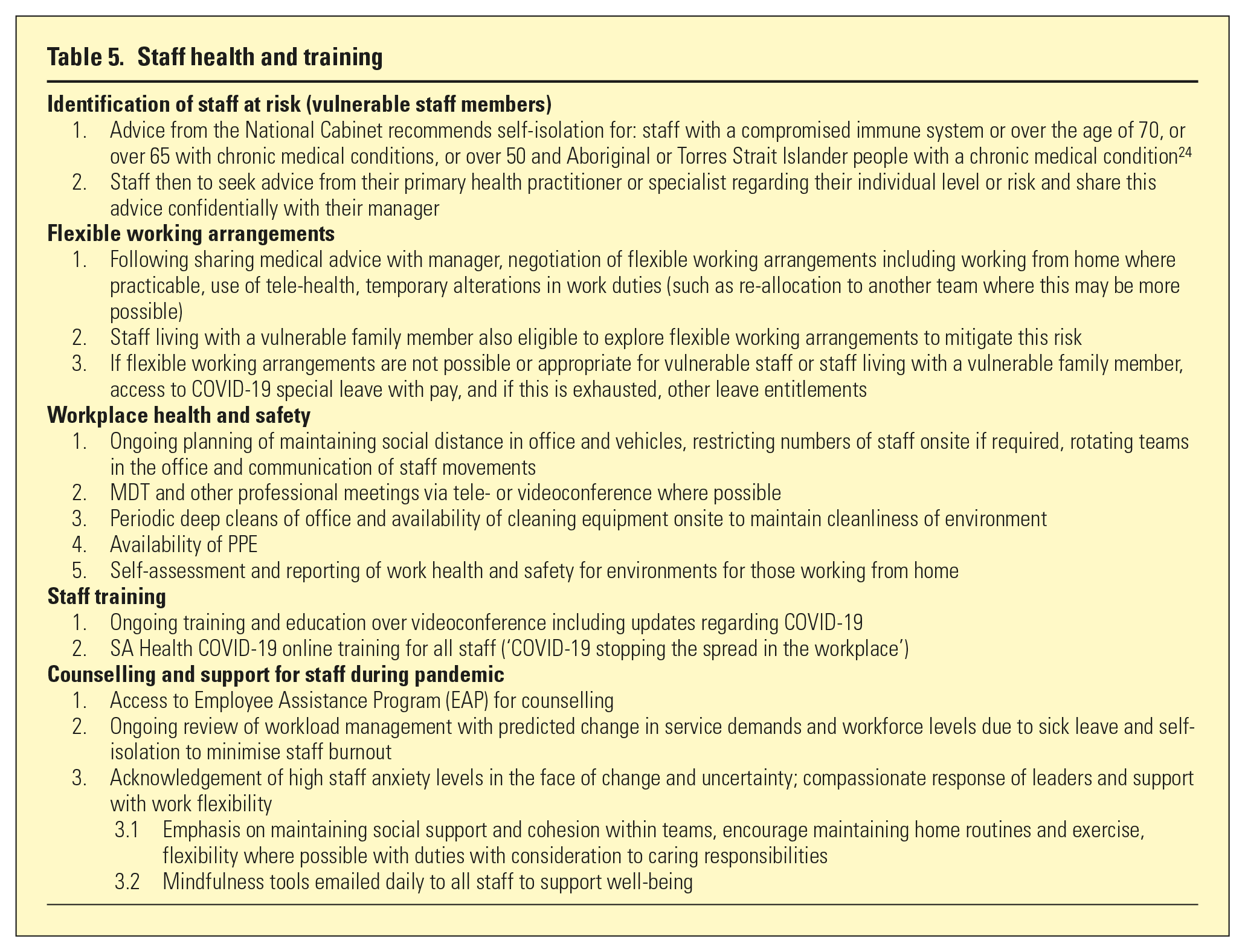
Overarching this, proactive and responsive leadership was needed to manage usual service demands and COVID-19-specific concerns. This included monitoring and evaluation of incidents via the online Safety Learning System and liaison between service departments and government agencies. Staff health, crucial at a time when staff are anxious about their own health and the health of their families, was supported through practical measures and staff training (Table 5). Responding to staff concerns in a transparent and empathetic fashion was also important to reduce burnout and distress. Further consideration of long-term advocacy and planning for social supports and mental health resources was needed to help meet the anticipated demand in the medium and long term.
Staff health and training
Discussion
Development and implementation of a CMH pandemic response required careful thought and expediency. The rapidly changing situation presented challenges in developing a service plan, necessitating a response providing both structure and adaptability. This needed to be responsive to new concerns, tailored to the local service and individual patients. Risks of exposure and transmission of COVID-19 to vulnerable patients needed to be carefully balanced against risks created by changes in service provision.
As Australia emerges from the pandemic, planning, particularly in regard to potential long-term changes in mental health service delivery, will be critical. Some consequences of the pandemic may be positive. Increased awareness of hygiene could mitigate transmission risks of other infectious diseases, and efficiencies resulting from use of tele-health may improve access for those in remote or inaccessible settings. However, the impact of COVID-19 itself, economic deterioration and consequent effects on lives, livelihoods and families are likely to be significant. Ongoing planning, both in direct mental health service delivery and how best to meet the increasing social need, is crucial.
Conclusions
The COVID-19 pandemic continues to pose a significant risk to the vulnerable patient population supported by CMH teams in the northern suburbs of South Australia. A public health response document was developed in response to this pandemic. It is hoped this can assist other CMH services in responding to COVID-19, and future pandemics.
Footnotes
Acknowledgements
The authors thank and acknowledge the NALHN Mental Health Practice, Procedures and Guidelines group for support and feedback, including Dr Shaun Sweeney, Northern Mental Health Senior Project Officer; Dianne Callahan, Director of Nursing, Mental Health; Nicole Keller, Divisional Director, Allied Health & Community Mental Health; and Dr Sanmuganatham Sujeeve, NALHN Mental Health Clinical Director. We also thank Jade Gooding, Executive Manager at Mental Health Anglicare, Northern Territory, and Dr Owen Haeney, James Nash House, for their support and Lisa Hahn for her support and initial formatting. The appropriate NHMRC processes were followed and approvals received.
Disclosure
The authors report no conflict of interest. The authors alone are responsible for the content and writing of the paper.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.