
Abstract
Keywords
Stroke is an important cause of morbidity and mortality in Western societies [1]. Psychological and behavioural changes are common following stroke and may contribute to further complicate the management of patients [2]. Recently published results from the Framingham study showed that strokes double the risk of incident dementia over a 10-year period [3]. Stroke has also been associated with increased risk of depression and anxiety disorders, with depression reportedly affecting as many as one in three people who survive a stroke for 1 year [4]. Both post-stroke dementia and depression have been associated with poor functional outcome and increased mortality [5, 6], although the number of reports in this area remains small and the results of available studies may have been confounded by selection bias and the inclusion of prevalent cases of mental health disorders. We know, for example, that depression increases the risk of mortality by stroke [6]. As a result, the outcome of stroke patients with pre-existing mental disorders may be less favourable than for people with no previous mental health history. Therefore, it is conceivable that the reported increased mortality associated with post-stroke mental health disorders is due to the presence of pre-existing clinically significant psychiatric symptoms rather than the onset of a new mental disorder after stroke. Clarifying this issue may have important implications for the design of effective secondary and tertiary prevention strategies.
We conceived the present study with the aim of determining: (i) the incidence of first-ever mental health disorder in the population of stroke patients admitted to hospital in Western Australia in 1990; (ii) the 10-year psychiatric morbidity of post-stroke patients; and, (iii) the 10-year mortality associated with incident post-stroke mental health disorders.
Methods
Identification of cohorts
This study used the recently established Western Australian Health Services Research Linked Database (WA Linked Database) [7]. Briefly, the WA Linked Database groups together records of all hospital admissions (private and public) since 1980 with the Mental Health Information System (MHIS), the WA death register and the WA hospital morbidity data. The MHIS is a record of all contacts with inpatient mental health services (private and public) in WA since 1966, and all contacts with state psychiatric outpatient clinics (which also provide community-based mental health services) since 1972, along with records of people resident in psychiatric hostels. The chains link together all acute hospital admissions, death records, hospital movements and psychiatric outpatient contacts for each patient.
For the purposes of this study, de-identified subjects receiving a diagnosis of stroke from the 1 January 1990 to 31 December 1990 according to the following selected ICD-9 diagnostic codes: 430.xx to 438.xx, but excluding category 435.9 (transient ischemic attack). We also excluded people with a prior history of myocardial infarction or fractured neck of femur (to exclude common causes of significant morbidity in this age group).
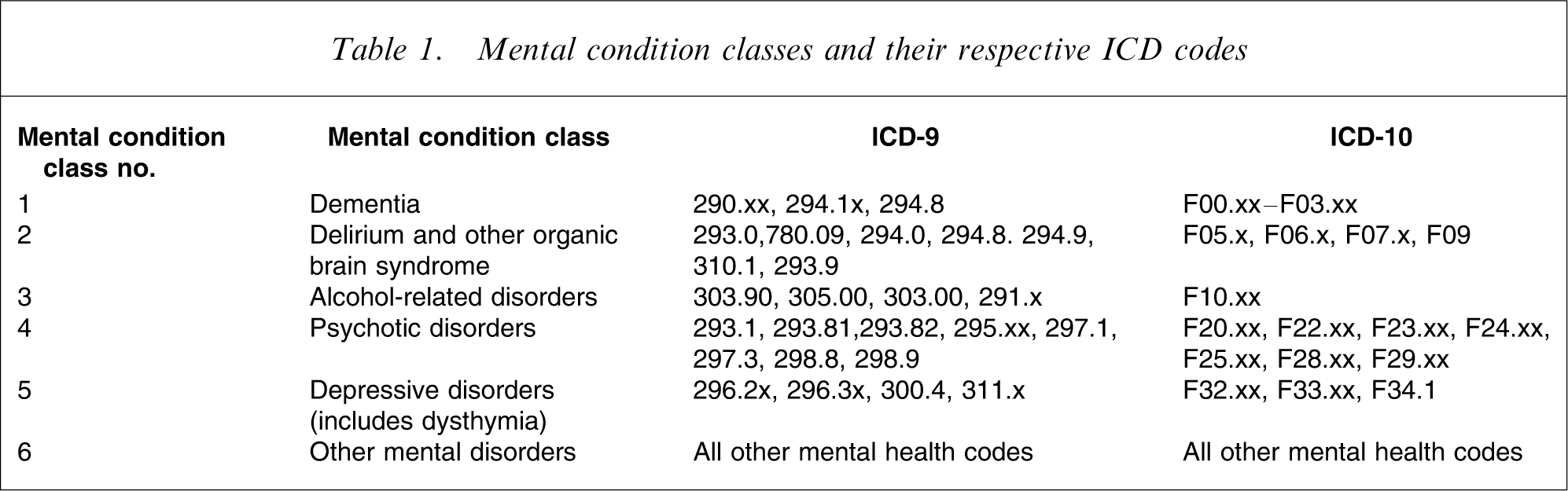
The administrative records of all eligible subjects were systematically assessed, and the index mental health disorder was defined as the first mental health diagnosis recorded during the 24 months following the stroke. Subjects who had a recorded mental health diagnosis between 1 July 1966 and 31 December 1989, or a prior diagnosis of stroke, were excluded from the analyses (i.e. only incident cases were included). Subjects who met the study's criteria for incident mental health disorder were classified as ‘cases’. The date of onset of the mental health disorder was defined as the index date. From the index date, all subjects were followed up for 10 years or until death, whichever came first. Mental health conditions were classified into six syndromic groups, as outlined in Table 1.
Mental condition classes and their respective ICD codes
Stroke patients who did not have any mental condition in the first 2 years after stroke (potential controls, n = 834) were individually matched to cases for gender and age (within 5 years). The duration between the first-ever stroke date and the occurrence date of the first-ever mental condition during the first 2 years after stroke for each case was used as the duration between the first stroke date and the index date for its control. This resulted in 287 pairs. Controls were followed up for 10 years from the index date or until death, whichever came first. Information on age, gender, country of birth, marital status, residential postcode and Aboriginality was available for all health contacts.
The study was reviewed and approved by the Confidentiality of Information Committee of the Department of Health of Western Australia.
Data preparation
The duration in months between the index date and the date of death was determined for each patient. If a subject was still alive at the end of the follow-up period, a total follow-up period of 120 months (10 years) was assigned. Postcode for the index episode of each patient was mapped to the Socio-economic Index for Area (SEIFA) code based on Australian Bureau of Statistics publications [8], with lower scores indicating worse socio-economic status. Marital status on index date was classified into five categories: never married, widowed, married/de facto, divorced, and separated. Country of birth was grouped into five categories: Australia, Europe, Asia, Africa, and Other.
Data analysis
Raw mortality rate and mortality per 1000 person-years (taking into account total duration of follow-up) were computed. Rate ratios were calculated and used in order to test whether or not there were statistically significant differences in mortality rates between patients who developed mental health conditions and patients who did not develop any mental conditions in the first 2 years after stroke. Information on the cause of death was available for all participants who died during the follow-up period.
Cox regression analysis was used to determine the relative contribution of risk factors, including mental health disorders, on survival. The hazard ratio was used to measure the magnitude of the effect of a risk factor on death compared with its reference category. For continuous variables, such as SEIFA score, the smallest magnitude (e.g. lowest SEIFA score) is the reference category. For mental health grouping, patients with no mental health entry were used as the reference category.
SPSS for Windows, version 12, was used to conduct data preparation and statistical analysis.
Results
General description of the sample
A total of 1129 patients received a primary diagnosis of stroke for the first-ever time in 1990. The mean age of stroke patients was 71.0 years (SD = 14.9; range = 0–101), 84.5% were older than 60 years and 50.7% were women. Twenty-one people died on the same day they were admitted to hospital. The cumulative incidence of the various mental disorders during the subsequent 12 years after the first-ever recorded stroke diagnosis was calculated for the 1008 survivors at risk: dementia, 12.1% (2.01 per 1000 person-years); delirium or other organic brain syndrome, 7.6% (1.26 per 1000 person-years); alcohol-related disorders, 16.2% (2.70 per 1000 person-years); psychotic disorders, 6.7% (1.11 per 1000 person-years); depression or dysthymia, 5.5% (0.91 per 1000 person-years); other mental health disorders, 4.2% (0.70 per 1000 person-years); and any mental health disorder, 36.6% (6.08 per 1000 person-years).
During the subsequent 24 months, 287 patients had a recorded mental health disorder. They were paired for gender and age with another 287 stroke patients without a mental health entry during the same period of time. Table 2 displays their basic demographic information.
Demographic and clinical characteristics of subjects with and without post-stroke mental disorders
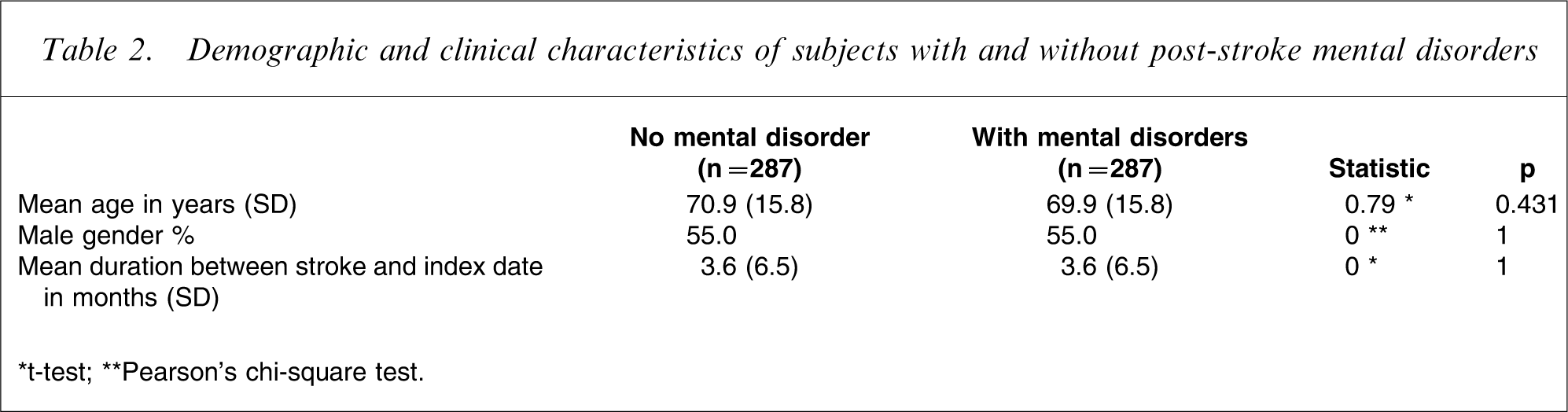
∗t-test; ∗∗Pearson's chi-square test.
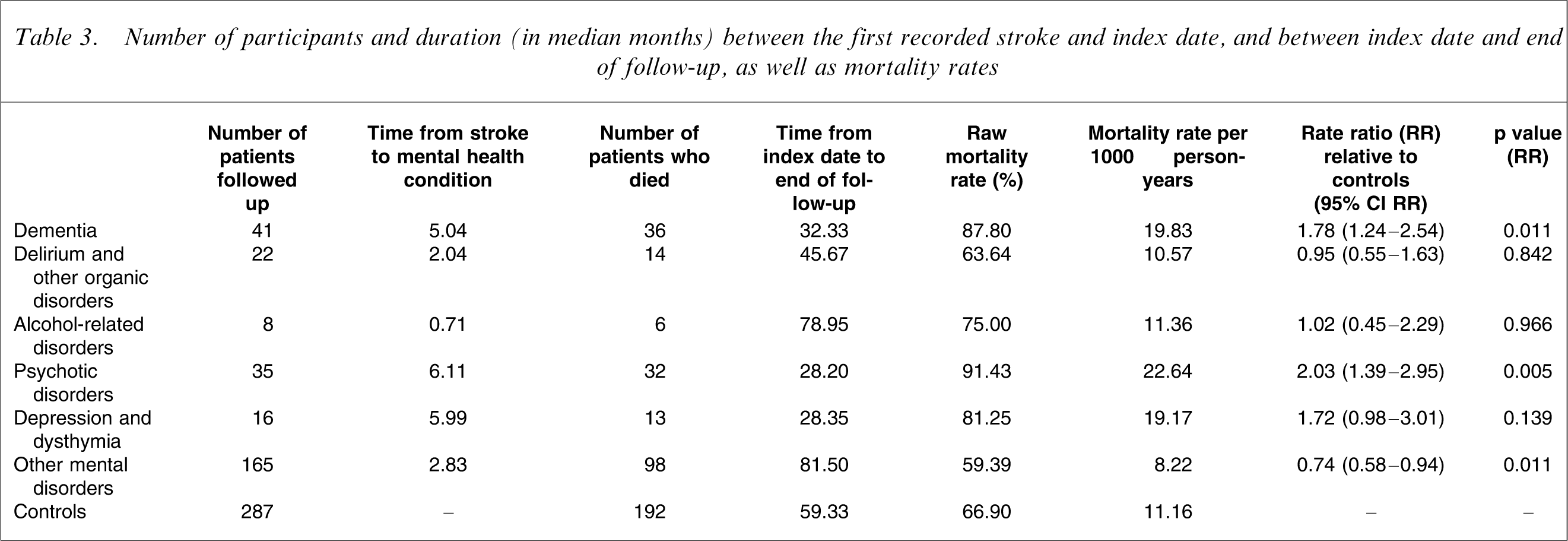
Of the 287 subjects with a mental health diagnosis, 14.3% had dementia, 7.7% delirium or other organic mental disorders, 2.8% alcohol-related disorders, 12.2% psychotic disorders, 5.6% depression or dysthymia, and 57.5% other mental disorders. Table 3 describes relevant information about participants, time between stroke and the index mental health condition as well as mortality rates. The median period of time between stroke and the onset of a mental health disorder was consistently under 6 months for all mental health disorders, with psychotic disorders having a median onset of 6.1 months. Noticeably, subjects with psychotic disorders and depression/dysthymia had the shortest duration between index date and death, whereas patients with other mental health problems or alcohol-related disorders had the greatest duration between index date and death. The diagnosis of psychosis and dementia were associated with increased death-rate ratio relative to controls, with the rate ratio for depression/dysthymia being borderline non-significant (Table 3).
Number of participants and duration (in median months) between the first recorded stroke and index date, and between index date and end of follow-up, as well as mortality rates
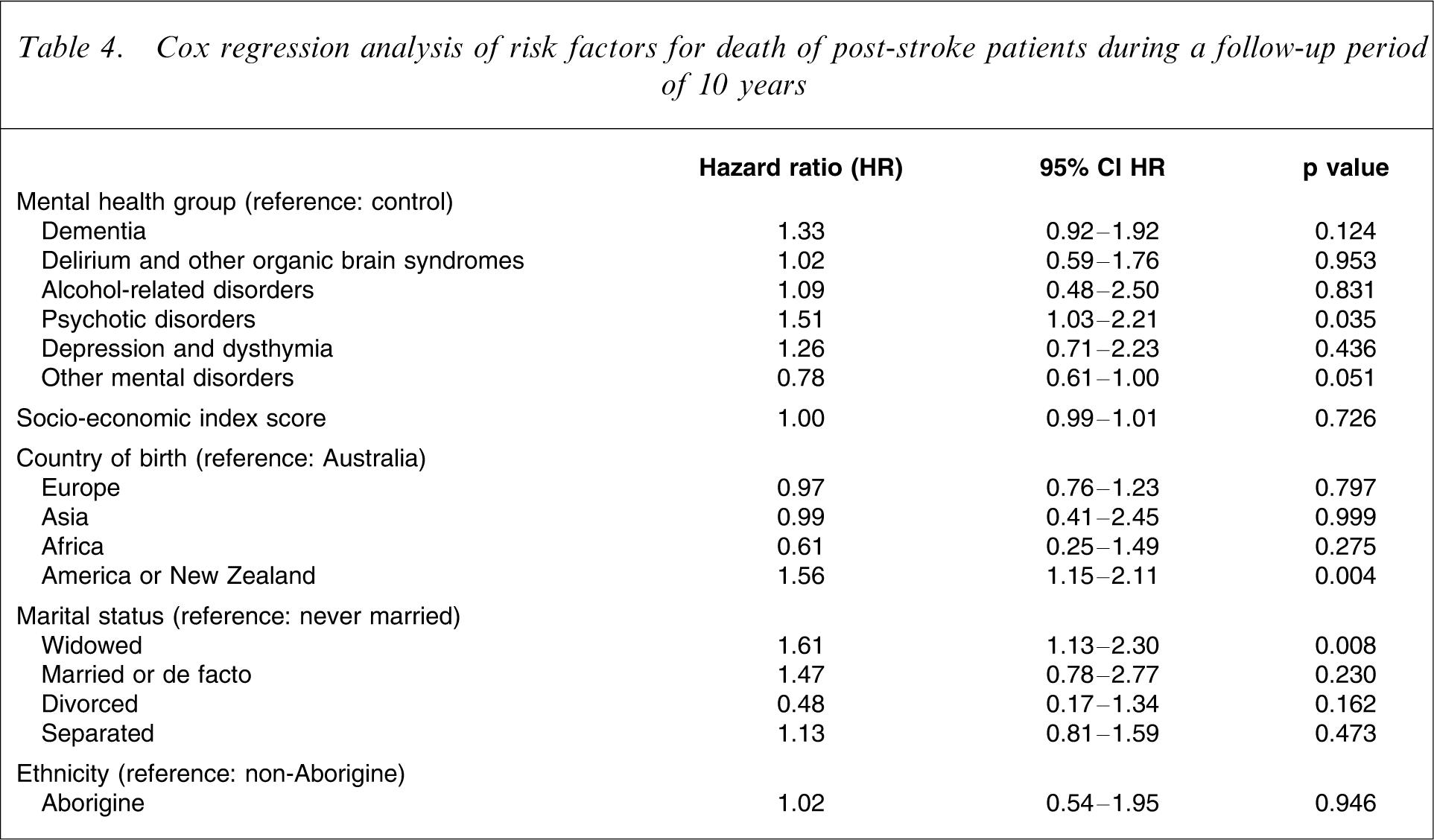
In addition to mental health diagnoses, other relevant variables associated with mortality in this sample were included in a Cox regression analysis (Table 4). The results showed that post-stroke patients who developed a psychotic disorder were 51% more likely to die during the 10-year follow-up period than controls. Likewise, people born in ‘other countries’ were 56% more likely to die at follow-up than their Australian-born counterparts, whereas widowed people were 61% more likely than never-married people to be deceased during the follow-up period. Socio-economic status and ethnicity did not make a significant contribution to the mortality hazard. Table 5 summarizes the most frequent causes of death of subjects with and without mental health disorders. The most frequent cause of death among patients with incident post-stroke psychotic disorders was cardiovascular disease (22/32), with 14 people dying as a consequence of cerebrovascular disease.
Cox regression analysis of risk factors for death of post-stroke patients during a follow-up period of 10 years
Causes of death of patients with and without (controls) the diagnosis of a mental health disorder within 2 years of stroke
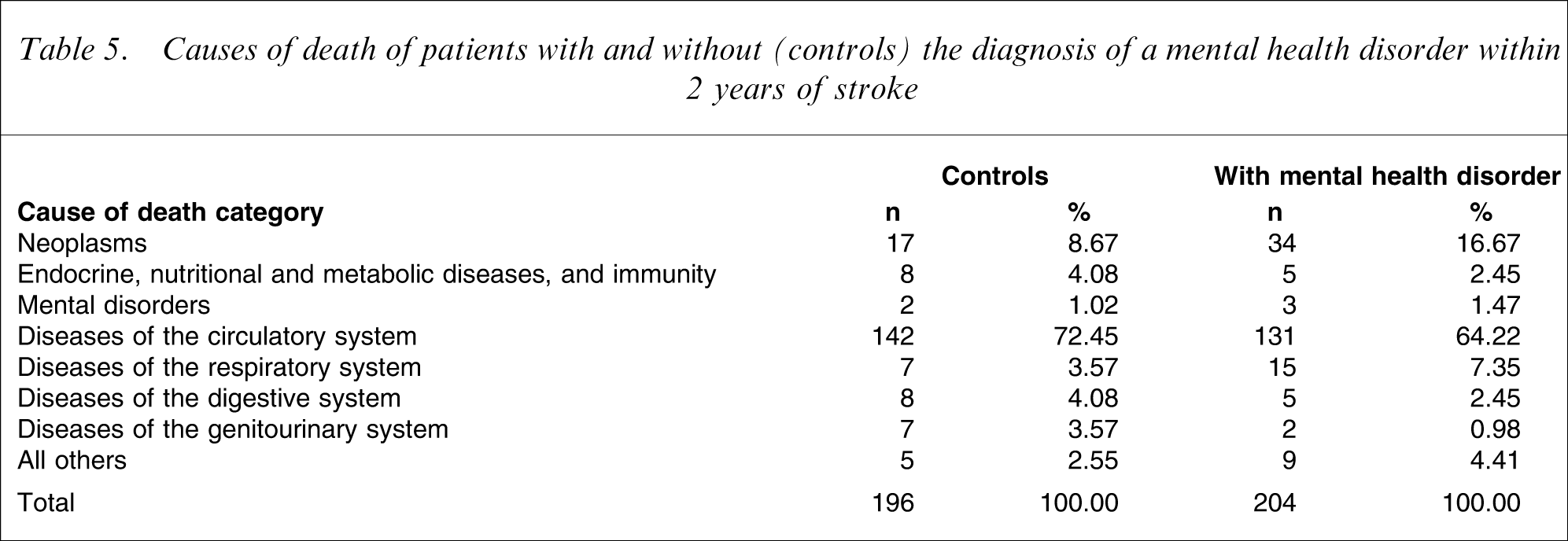
Figure 1 shows the cumulative survival rate for each mental condition group and for controls. Subjects with psychotic disorders had the lowest survival rate, with only 3/35 surviving 5 years or more.
Cumulative survival rate by mental condition categories over a 10-year follow-up period.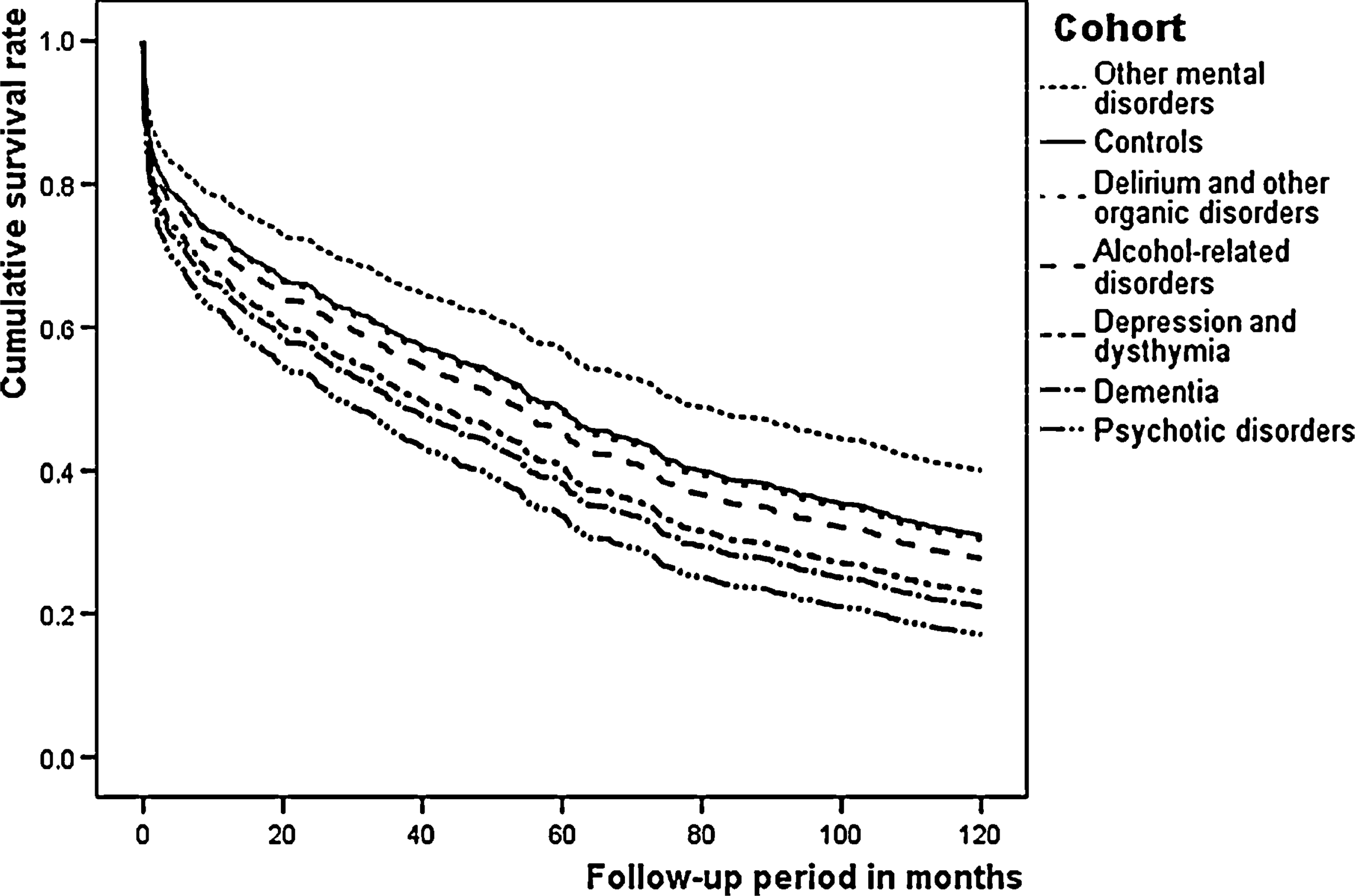
Discussion
The results of this population-based study provide, as far as we are aware, are the most complete epidemiological evidence to date of the association between stroke, incident mental health disorders and mortality. Our findings show that the incidence of clinically significant post-stroke mental health disorders is high, but probably lower than previously suggested (6.1 per 1000 person-years or 36.6% of the sample) [9].
A nested case-control study originating from the Framingham cohort showed that the incidence of dementia was 19% [3] compared to 12% in the present study. The cross-sectional design of previous studies, their likely inclusion of prevalent cases, as well as the exclusion of cases of aphasia or of subjects who were unable/unwilling to consent may have contributed to inflate previously published estimates of the incidence of post-stroke dementia.
Similarly, the incidence of post-stroke depression in this study was lower than previously reported. We found that only 5.5% of patients received the diagnosis of a depressive episode or dysthymia during the 12 years following a stroke. A previous investigation of 294 patients from the Perth Community Stroke Study detected the presence of clinically significant depression in 23% of patients 4 months after the stroke [10]. Other studies have produced prevalence estimates ranging from 16% to 47% but, again, selection bias and the inclusion of prevalent cases might have inflated the number of people with post-stroke depression in some surveys [11].
Surprisingly, we observed a relatively high incidence of mental disorders not commonly reported in association with stroke. Sixteen per cent of stroke patients had a recorded diagnosis of alcohol-related disorder during the course of follow-up, although the factors leading to such an elevated figure are not immediately apparent. It is possible that many people who consume alcohol at harmful or hazardous levels only come to medical attention when a major health event, such as a stroke, takes place. As a result, our estimates may have been inflated by the presence of people with previously undiagnosed alcohol-related conditions.
A relatively large proportion of patients (6.7%) had a recorded psychotic disorder after the stroke (no other mental health diagnoses, such as delirium or dementia, were recorded in association with the diagnosis of psychosis). Rabins et al.[12], in a small case-series of 10 post-stroke patients, observed that their five patients with psychosis had more brain pathology and more frequent seizures than those without, suggesting that post-stroke psychotic symptoms may indicate the presence of significantly disrupted cerebral function. Likewise, the investigation of post-stroke delirium to date has been haphazard. Available estimates suggest that a quarter of patients develop delirium after stroke [13], although our findings indicate a much lower incidence (7.6% over 12 years). As the diagnosis of delirium is frequently overlooked in day-to-day clinical practice, it is possible that the results of the current study underestimate its true incidence. It is also conceivable that the diagnosis of delirium is not systematically recorded, as it may be considered a secondary clinical expression of a primary medical condition (such as acute stroke). In addition, as delirium is associated with increased mortality [14], severe cases that are more prone to delirium may be censored and consequently decrease the size of the population at risk (survivorship bias).
Patients who developed a psychotic disorder during the initial 2 years after a stroke were more likely to die than people in the comparison control group during the subsequent 10 years. Most previously published studies have associated depression and dementia with increased mortality [5, 6] but, as far as we are aware, this is the first study indicating that incident post-stroke psychosis is associated with increased mortality. Psychosis has been associated with rapid cognitive decline among people with dementia, as well as increased mortality [15]. There is also growing evidence that the use of antipsychotic medication for the treatment of people with underlying brain pathology increases mortality (mostly due to strokes) [16], which may partly explain the worryingly poor outcome of patients with post-stroke psychosis. Post-hoc analysis did not identify a distinct cause of death pattern among subjects with and without post-stroke psychosis, so that it remains to be determined why people with incident post-stroke psychosis have such a poor clinical outcome.
Widowhood was also associated with increased risk of mortality in this and other cohorts [17]. Smoking and alcohol consumption is more frequent among unmarried than married individuals [18], and unmarried people have a lower concentration of HDL cholesterol [19], which may contribute to further increase cardiovascular morbidity. The results of this study also showed that stroke patients born in the ‘other countries’ group were 56% more likely to die than their Australian-born counterparts. It is not immediately apparent why that should be the case, but lifestyle factors may have contributed to such a finding. For example, people originating from Latin America have higher lifetime exposure to tobacco than individuals from other continents [20], and this could contribute to increase mortality. It is also possible that Western Australian recent migrants have medical and mental health morbidities that were not recorded in any of the administrative databases. In this case, subjects from other countries would be more likely to die due to the presence of prevalent medical (such as a prior myocardial infarction or stroke) and mental health conditions. Although we are unable to entirely dismiss this possibility, this would seem an unlikely explanation for our results, as the incidence rate of mental disorders in this study was low (such a bias associated with migration would have led to increased incidence rates of mental disorders), and data from the Australian Bureau of Statistics shows that Western Australia experiences minimal population movement in the older age group (mean age of patients in this study = 71 years) [21]. In addition, migrants in Australia have lower death and hospitalization rates, as well as lower rates of disability and lifestyle-related risk factors [22].
The design of this study has strengths that merit comment. Firstly, it included all new cases of stroke recorded in Western Australia in 1990, not a selected convenience sample. In addition, as only incident stroke cases were included in this cohort, the potential confounding associated with increased morbidity associated with previous strokes is minimal. Secondly, only people with no previously recorded mental health history were included in the study cohort, which maximises the likelihood that the mental health disorders that followed the stroke were truly incident. Thirdly, the matched case-control approach used in the analysis of the data enabled us to all but eliminate the risk of confounding associated with age and gender when estimating the contribution of factors associated with post-stroke mortality. Finally, the extensive follow-up period of 10 years enabled us to investigate not only the acute but also the long-term consequences of post-stroke mental health disorders. There are, however, limitations of the present study that should be acknowledged. The estimated incidence rates for post-stroke mental disorders were based on people who received a mental health diagnosis after presenting for treatment at a hospital or public mental health service. Therefore, we cannot entirely be sure how well the reported rates reflect the true incidence of post-stroke mental disorders in the community. We also concede that the use of patients in contact with acute health services might have led to selection bias due to suboptimal detection of conditions commonly managed in general practice, such as depression, and the over-representation of disruptive psychological and behavioural symptoms, such as in psychosis. In addition, the psychiatric assessment of patients was neither structured nor systematic, and this might have led to an underestimate of the true incidence of post-stroke mental health disorders. The consequence of such a bias would have been to reduce the power of the study (type II error), which may partly explain why we were unable to confirm the findings of previous reports indicating that post-stroke depression and dementia are associated with increased mortality. Furthermore, the validity of the psychiatric diagnoses recorded and the quality of linked data may be questioned, although previous studies demonstrated their face validity in relation to hardcore end points such as suicide, attempted suicide and death by other causes [23]. Jablensky et al.[24] have recently demonstrated the concurrent validity of this database for the diagnoses of schizophrenia and affective psychoses using a semi-structured interview covering the 90 items of the Operational Criteria for Psychosis diagnostic algorithm. Others have also shown that this database produces reliable and valid information for substance-related disorders [25]. Finally, we did not have access to information pertaining to type, location and severity of the stroke and, as a result, were unable to investigate the association between the characteristics of the stroke and the onset of mental health disorders and mortality.
In summary, the results of this study show that approximately one in three patients develop a mental health disorder after a stroke. The onset of more than 50% of all recorded psychiatric disorders takes place within the initial 6 months after the stroke, with psychotic disorders being associated with increased mortality. Future research should aim to determine how mental health disorders, such as psychosis, lead to increased mortality, so that appropriate preventative strategies can be devised and introduced in clinical practice.
Footnotes
Acknowledgements
The authors gratefully acknowledge the helpful critical comments made by Sergio Starkstein on an earlier draft of this manuscript. This project was partly funded by a project grant from the Australian Rotary Health Research Fund.