
Abstract
Objective:
Antipsychotics are widely used for treating psychosis, but it is unclear whether they can also prevent psychosis. This study attempted a longitudinal evaluation of antipsychotics under real-world conditions in China to evaluate their effect on the rate of conversion to psychosis in individuals with a clinical high risk (CHR) of psychosis.
Method:
A total of 517 CHR individuals were recruited between 2011 and 2016 and followed up for 3 years. Among these, 450 (87.0%) individuals completed follow-up, 108 (24.0%) showed conversion to psychosis and 309 (68.7%) received antipsychotics. The main outcome was conversion to psychosis. The sample was further stratified according to the severity of positive symptoms.
Results:
Patients who did not receive antipsychotics showed a lower conversion rate than those who did (17.7% vs 26.9%; odds ratio [OR] = 0.660, 95% confidence interval [CI] = [0.442, 0.985], p = 0.035). In mild CHR cases, antipsychotic treatment was more likely to be associated with conversion to psychosis, compared with the no-antipsychotics group, with no such difference observed in severe CHR cases. Among those who received antipsychotics, monotherapy or low-dose treatment was associated with lower conversion rates. Our results did not favor any specific type of antipsychotics and suggested that a very small subgroup of CHR individuals with severe positive and general symptoms but mild negative symptoms may benefit from antipsychotic treatment.
Conclusions:
Administration of antipsychotics to CHR patients is potentially harmful with no preventive benefits. We do not recommend antipsychotic treatment for CHR individuals, which is practiced widely in China, and strongly advise caution if these drugs are used.
Introduction
Despite increasing awareness of the importance of early intervention for psychosis in China, various misunderstandings prevent patients from receiving optimum care. Antipsychotics, as the traditional, classical and more accessible form of treatment for patients with psychosis, have been assumed to be also effective in preventing psychosis. Although clinical trials have shown that initiation of antipsychotic treatment effectively reduces symptom burden versus placebos (Leucht et al., 2009), the appropriate time for initiation of antipsychotic treatment has still not been conclusively identified. In early intervention research on psychosis, a reliable criterion termed the ‘clinical high risk (CHR)’ status has been adopted to categorize clinical help-seeking persons who are at heightened risk for emerging psychosis but do not meet the criteria of first-episode psychosis at present. Notably, less than 40% of CHR individuals will show conversion to psychosis in following 3 years (Fusar-Poli et al., 2012, 2013); thus, those with false-positive CHR individuals may be exposed to the adverse effects of antipsychotics but may not necessarily benefit from antipsychotic administration. Therefore, the appropriateness of administering antipsychotics to CHR individuals is an important issue.
Limited previous randomized controlled trials (RCTs) of antipsychotic treatment for CHR individuals indicated possible short-term efficacy on psychotic symptoms with unclear long-term effects. The first RCT by McGorry et al. (2002) showed that low-dose risperidone treatment plus cognitive behavioral therapy (CBT) may reduce, or at least delay, the possibility of progression to psychosis. However, a subsequent study Yung et al. (2011) showed negative results that antipsychotic did not provide any advantage over CBT. The first double-blind, placebo-controlled clinical trial by McGlashan et al. (2006) found a nearly significant difference when comparing conversion rates between 31 CHR individuals treated with olanzapine (5–15 mg/day) and 29 with placebo, but the olanzapine group gained significantly more weight. Considering the lack of evidence supporting antipsychotic prescription for CHR individuals, many guidelines (Galletly et al., 2016; Schmidt et al., 2015) include warnings for clinicians to exercise caution while making the decision to treat CHR individuals with antipsychotics.
Although RCTs and guidelines have recommended against use of antipsychotics for CHR individuals, clinicians often do not follow the guidelines. The complexity of daily clinical practice has often been used as an excuse for clinicians to offer easy therapy instead of optimal therapy. Therefore, there is an important and urgent need for adequate evidence from real-world pragmatically designed studies that better reflect real-life clinical practice. More recently, the quality of evidence from real-world observational studies has improved and has received more attention and concern. Despite the emphasis on pharmacological effects in prevention of psychosis, to our knowledge, no real-world study with a large CHR sample (n > 300) treated with antipsychotics alone and with long-term follow-up data (>2 years) has been conducted to date.
The current study, we reported our clinical observations in an exploratory perspective to see whether antipsychotics can delay or prevent the onset of psychosis. Four previously published reports (Zhang et al., 2017, 2018a, 2018b, 2018c) focused on risk assessment and prediction with detailed study design, recruitment procedures, baseline characteristics and follow-up measurements. A key element of our sample is that all participants were psychotropically naïve when they entered the study and were assessed clinically. They had received no treatment of any kind for a psychiatric disorder. It’s also worth mentioning that psychosocial treatment was not available for the current sample due to the limited clinical resources for psychosis. Notably, there was also no history of drug (such as methamphetamine) abuse or dependence in this sample, because drug abuse is one of the exclusion criteria for CHR recruitment. The current report focuses on the effects of antipsychotics from real-life data over a 2- to 3-year follow-up period to provide a fuller picture of intervention effectiveness and realistic antipsychotic treatment outcomes, and may yield useful insights into alternative management approaches in more challenging CHR cases.
Methods
Sample
The ShangHai At Risk for Psychosis (SHARP) study was conducted with CHR individuals enrolled in an early identification program for psychosis, and implemented at one site, the Shanghai Mental Health Center (SMHC) in China. The Research Ethics Committees at the SMHC approved these studies. All participants gave written informed consent at the recruitment stage of the study. Subjects younger than 18 years of age had their consent forms signed by their parents, and the youths gave assent. Four studies and three funded projects contributed to establish this SHARP cohort. The SHARP sample was taken from the Shanghai Psychotherapy and Psychological Counseling Center (SPCC) at SMHC, which is China’s largest outpatient medication-management and psychotherapy-providing mental health clinic. These help-seeking participants from different parts of the country were included in the study. In supplemental data 1 eFigure 1, we have included a flowchart showing enrolment in the SHARP program and the 2- or 3-year follow-up data of CHR individuals. A total of 517 CHR individuals were identified using a face-to-face interview based on the Structured Interview for Prodromal Syndromes (SIPS) (Miller et al., 2002, 2003). At baseline, these participants were between 13 and 45 years of age (mean = 20.5 years; standard deviation [SD] = 6.2 years), of which 47.2% were male and had completed at least 6 years of primary education. Among these, 450 (87.0%) completed a 2- or 3-year follow-up assessment, while 67 (13.0%) were lost to follow-up at the 2-year follow-up visit. The participants who completed follow-up and those lost to attrition showed significant differences (see supplemental data-2 eTable 1). Details of the study procedures, study setting, implementation of the measurement and assessment are reported elsewhere (Zhang et al., 2012, 2014, 2015, 2017).
CHR criteria, clinical variables and stratification
The SIPS (Miller et al., 2003) was used to determine whether subjects met the criteria for CHR status, which consists of 19 items that assess four symptom domains: positive symptoms (scales P1–P5: P1, unusual thought content; P2, suspiciousness; P3, grandiosity; P4, perceptual abnormalities; and P5, disorganized communication), negative symptoms (scales N1–N6: N1, social anhedonia; N2, avolition; N3, expression of emotion; N4, experience of emotions and self; N5, ideational richness; and N6, occupational functioning), disorganized symptoms (scales D1–D4: D1, odd behavior of appearance; D2, bizarre thinking; D3, trouble with focus and attention; and D4, impairment in personal hygiene) and general symptoms (scales G1–G4: G1, sleep disturbance; G2, dysphoric mood; G3, motor disturbances; and G4, impaired tolerance to normal stress). There are three subtypes in the CHR criteria, including attenuated positive symptom syndrome (APSS), genetic risk and deterioration syndrome (GRDS) and brief intermittent psychotic syndrome (BIPS). The global assessment of function (GAF) was used to measure global psychological, social and occupational functioning of the patients, which was used to assess the functional deterioration (score relative to 12 months prior) in the SIPS interview.
In our previous studies (Zhang et al., 2014, 2017), the Chinese version (Zheng et al., 2012) of SIPS, which was developed by the SHARP team, also demonstrated good interrater reliability (intraclass correlation coefficient r = 0.96, p < 0.01 on the SIPS total score) and validity (26.4%, converted to psychosis in the succeeding 2 years) in China. The first author was certified on the SIPS at Yale University-sponsored SIPS trainings, along with Drs. Woodberry and Seidman, who have extensive experience with the SIPS in the North American Prodrome Longitudinal Study (NAPLS) and other CHR research projects.
In consist with our previous reports (Li et al., 2018; Zhang et al., 2017) and other studies (Cannon et al., 2008; Fusar-Poli et al., 2012), CHR individuals with more severe positive symptoms were more likely to convert to psychosis. Therefore, we further subdivided CHR individuals on the basis of severity of their baseline symptoms into the high-level and low-level groups. The high-level group included CHR individuals with the total positive symptoms’ scores of 10 or higher (Carrion et al., 2017) according to the SIPS.
Conversion definition and follow-up procedures
Conversion to psychosis was the major outcome in this study, which was determined using the criteria for Presence of Psychotic Symptoms (POPS) (McGlashan et al., 2010) from SIPS. Specifically, conversion was defined by the presence of a 6-level positive symptom (the rating ‘6’ refers to severe and psychotic) that is either dangerous, disorganized, or occurring at least an hour a day on average over 4 days a week for at least longer than 16 hours. Among the 108 converters, 95 were diagnosed with schizophrenia, 11 with bipolar disorder with psychotic symptoms, and 1 with obsessive-compulsive disorder with psychotic symptoms. One subject with psychotic symptoms committed suicide. Among the converters, 89 subjects were hospitalized either at SMHC or in local psychiatric units.
The CHR individuals were followed up every 6 months through face-to-face and phone conversations by research psychiatrists. Both the CHR individuals and their caregivers had been told that they could contact the interviewer and study clinicians anytime for questions and progress reports on the patients’ medical condition. The clinical outcome determination was based mainly on face-to-face interviews (of 450 CHR individuals, 359 had at least a face-to-face interview during the follow-up) and partly from telephone interviews of CHR individuals or their caregivers, and on the medicine information confirmed using clinician reports and medical records.
Medication data
Use of antipsychotics was examined in every follow-up interview by asking about the subjects’ medication history since the previous visit (or telephone interview). Depending on whether antipsychotic was taken for at least 2 weeks during the follow-up period, the sample was divided into a no-antipsychotic group (n = 141) and an antipsychotic group (n = 309). Next, using an olanzapine-equivalent dose of antipsychotic (Leucht et al., 2016) lower than 10 mg/day as the cutoff value, the antipsychotic group was further divided into a low-dosage group (n = 203) and a high-dosage group (n = 106). Finally, depending on whether antipsychotic was discontinued at least two times, the antipsychotic group was further divided into regular use of antipsychotic group (n = 169) and irregular use of antipsychotic group (n = 140). A small group of participants took psychoactive medication other than antipsychotics (131 individuals took antidepressants, with a fluoxetine-equivalent (Hayasaka et al., 2015) dose of 45.7 [SD = 38.4] mg, and the mean duration for which it was taken was 39.8 [SD = 35.9] weeks).
Data analysis
Means and SDs were applied to describe continuous variables; counts and percentages were applied to describe categorical variables. Independent t tests were conducted to measure AP vs no-AP group differences in continuous variables, and either Chi-square statistics or a Mann–Whitney U test were used to examine categorical variables. Kaplan–Meier method and log-rank tests was used to plot survival curves and for comparisons between groups. Chi-square statistics were used to calculate odds ratios (OR) with p-values and 95% confidence intervals (CIs). Cox regression analysis was conducted to explore independent predictive factors and calculate hazard ratios (HR) with p-values and 95% CIs. On the basis of the predictive properties described above, we propose and summarize three TEN rules that can be used to identify a potential CHR subgroup that is more likely to be benefit from antipsychotic usage.
Results
Baseline demographics and clinical characteristics
Table 1 shows the comparative baseline demographic and clinical characteristics for CHR individuals with and without antipsychotic treatment.
Demographics and clinical variables comparing CHR individuals with and without antipsychotic treatment for at least for 2 weeks during the follow-up.
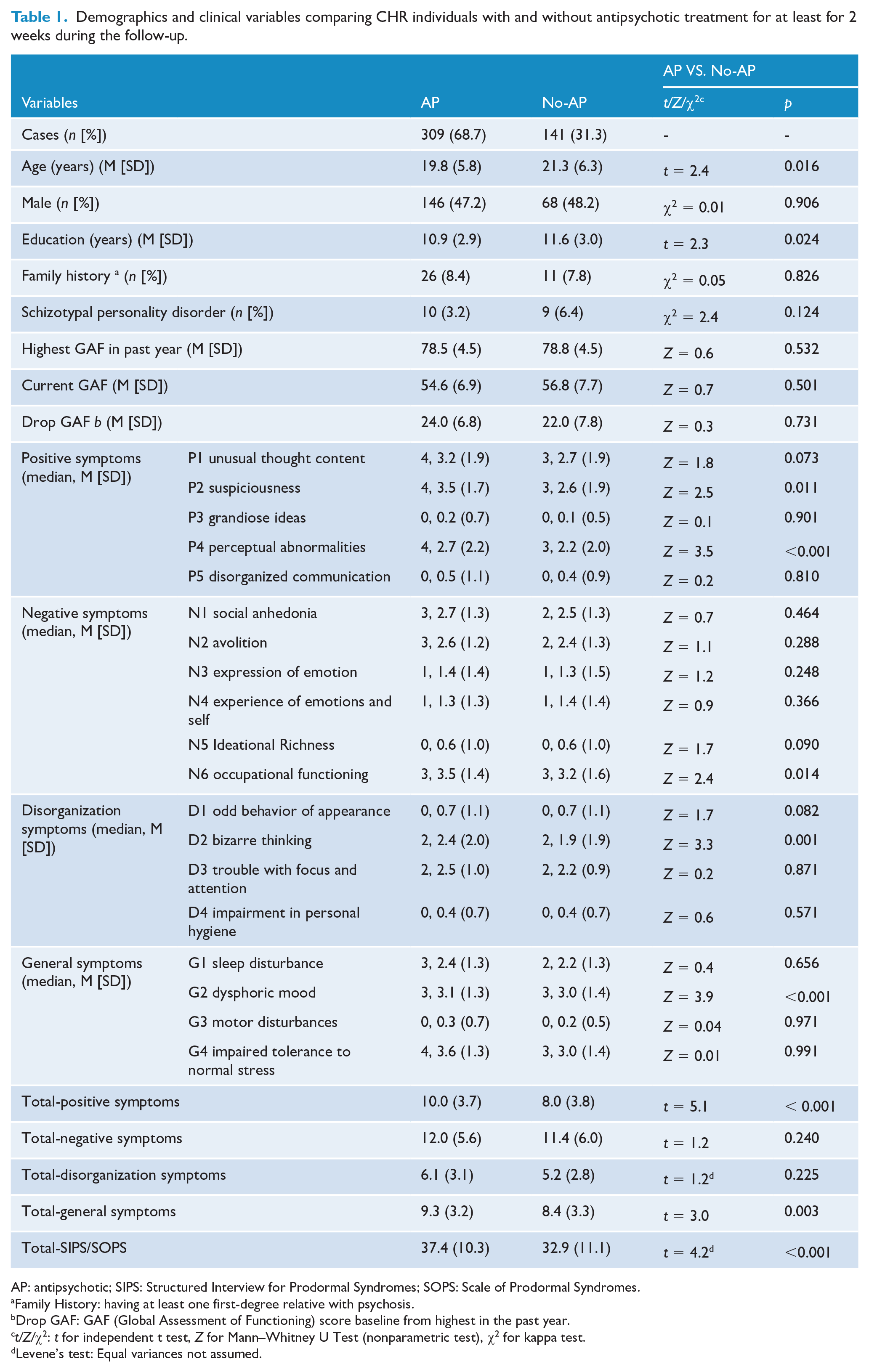
AP: antipsychotic; SIPS: Structured Interview for Prodormal Syndromes; SOPS: Scale of Prodormal Syndromes.
Family History: having at least one first-degree relative with psychosis.
Drop GAF: GAF (Global Assessment of Functioning) score baseline from highest in the past year.
t/Z/χ2: t for independent t test, Z for Mann–Whitney U Test (nonparametric test), χ2 for kappa test.
Levene’s test: Equal variances not assumed.
Antipsychotic exposure
Among the 309 CHR individuals who had taken antipsychotics in the follow-up period, 203 (65.7%) received a low dose, 266 (86.1%) received antipsychotic monotherapy and 144 (46.6%) had stopped receiving antipsychotics (see supplemental data 3 eTable-2). On the basis of daily doses in monotherapy, the five most commonly used antipsychotics were aripiprazole (27.8%), olanzapine (18.8%), risperidone (14.6%), amisulpride (11.7%) and quetiapine (7.4%).
Convertors versus non-converters
Kaplan–Meier survival curves were constructed for 450 CHR individuals (108 converters and 342 non-converters) separated by dose (no-antipsychotic, n = 141, vs low-dose, n = 203 vs high-dose, n = 106), mode of treatment (no-antipsychotic, vs monotherapy [one-antipsychotic], n = 266 vs combination [at least two types of antipsychotic], n = 43) and current status (no-antipsychotic, vs stopped, n = 144 vs continued, n = 165). Figure 1(a) shows that the conversion rate was significantly higher in those who received high-dose and continued at the end follow-up point. Considering the difference in baseline positive symptoms between the antipsychotic and no-antipsychotic groups as the biggest confounder, the survival analysis was stratified according to positive symptoms’ level (cutoff score, 10). For low-level baseline positive symptoms, significant differences in those comparisons were maintained. For high-level baseline positive symptoms, significant differences were not maintained (Figure 1[b]).
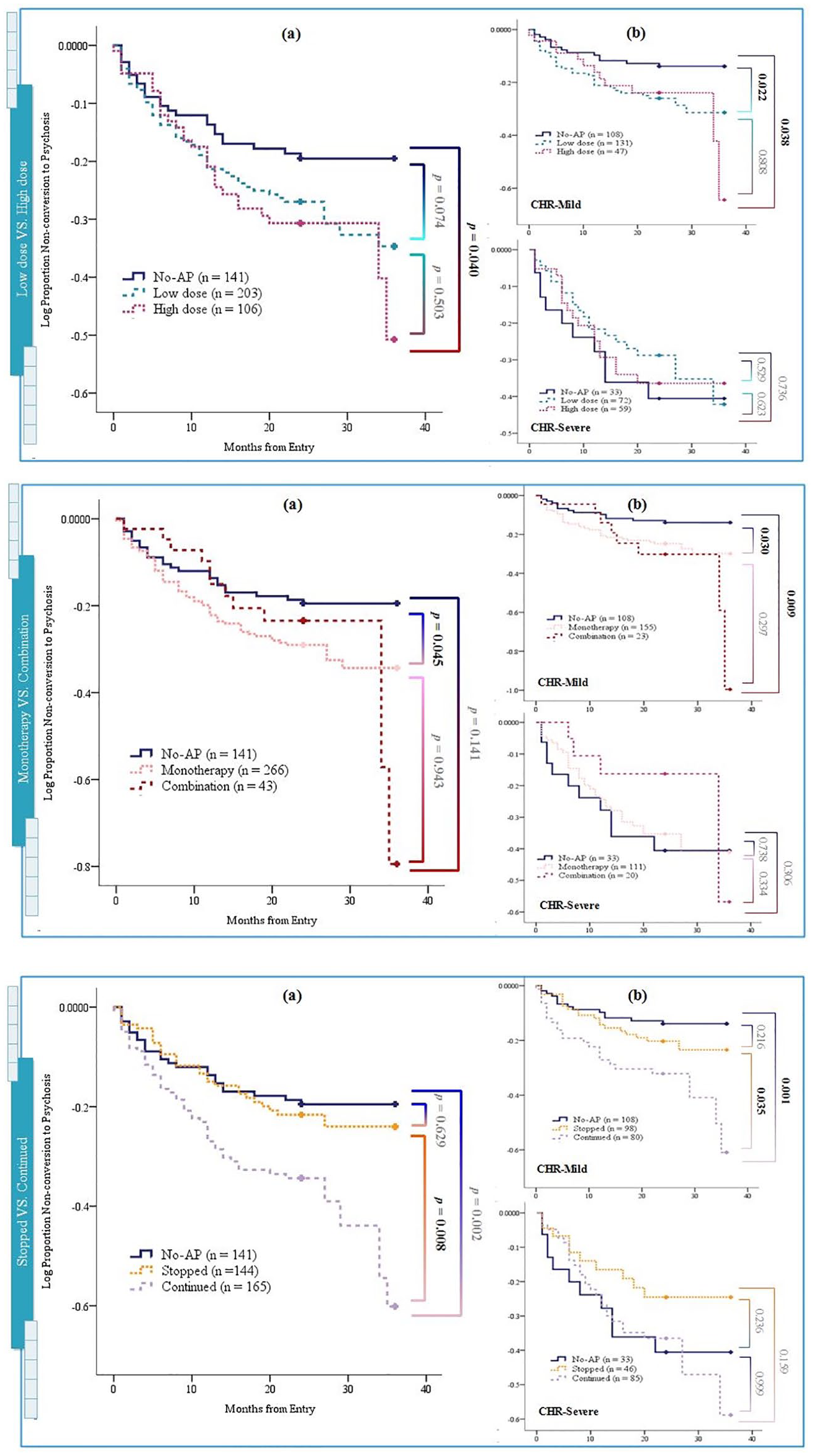
(a) Kaplan–Meier curves for overall survival and (b) CHR individuals with mild/severe positive symptoms, by comparison (log-rank test) between low and high doses, short-term and long-term, monotherapy and combination therapy, stopped and continued antipsychotic (AP) use at the end point of follow-up.
Antipsychotic types and conversion
In comparison with the no-antipsychotic CHR individuals, CHR individuals treated with olanzapine or aripiprazole showed a significant increase in the risk of conversion to psychosis. Higher doses of risperidone or olanzapine and longer period of usage of olanzapine, aripiprazole, or amisulpride were associated with a significantly higher risk of conversion to psychosis (Figure 2).
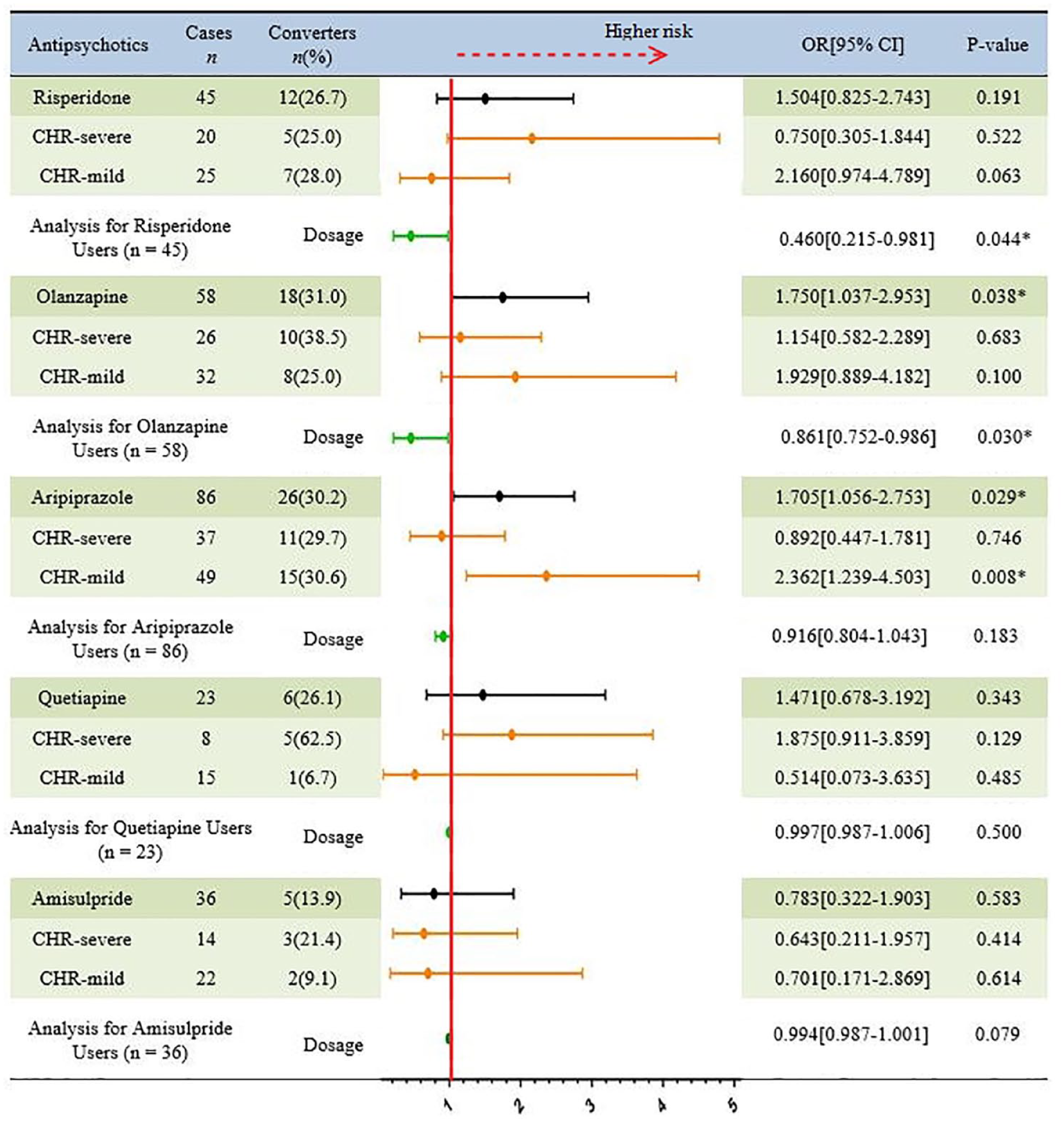
Comparison of the proportion of CHR individuals converted and not converted to psychosis after treatment with different types of antipsychotics.
Multivariate Cox regression
We conducted multivariate Cox regression analysis to appraise all accessible demographic and clinical variables and antipsychotic usage information for CHR individuals treated with antipsychotics (n = 309). Figure 3 indicates that the total positive, negative and general symptoms scores, GRDS and a family history of psychosis were independent predictive factors of conversion. Furthermore, the dosage of antipsychotics was also related to conversion.
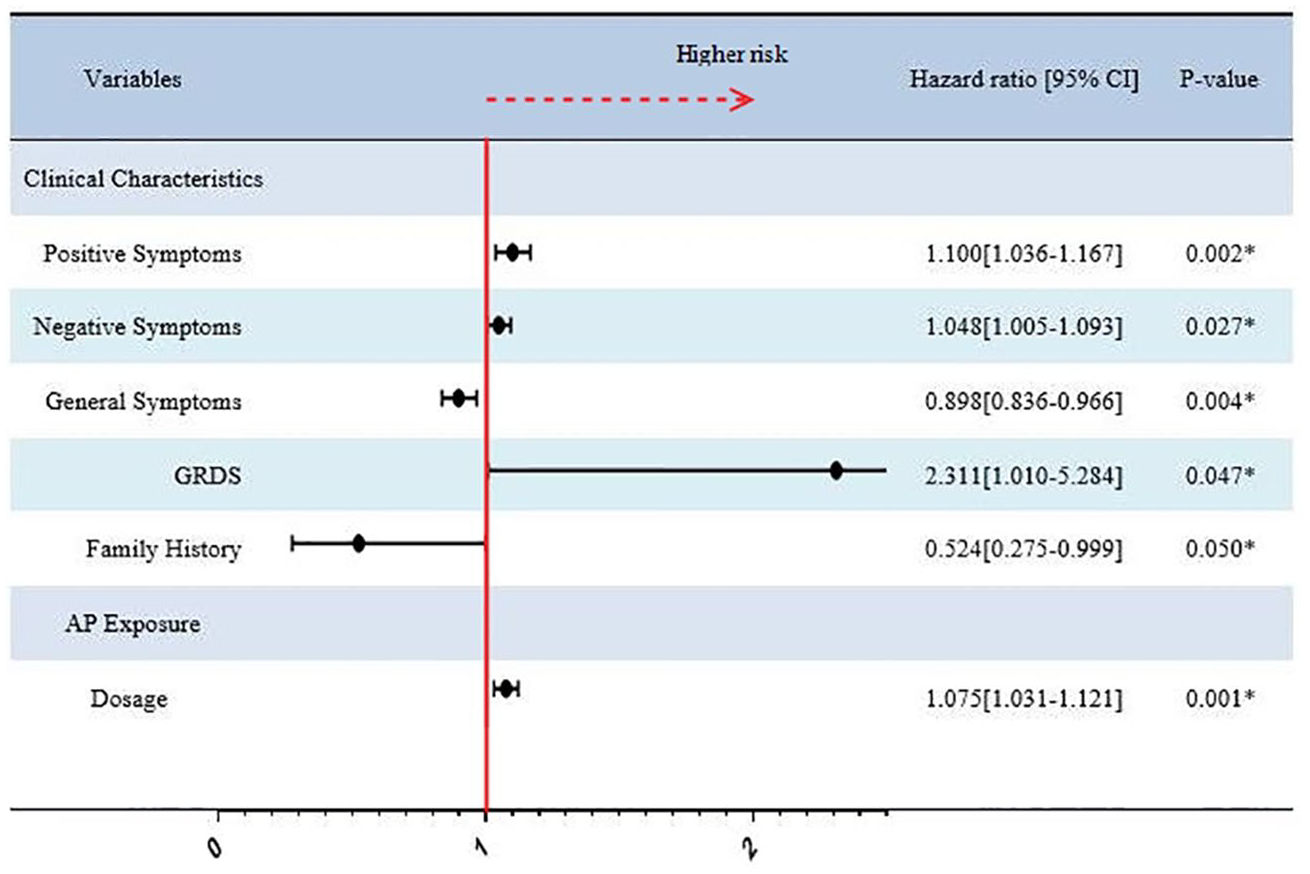
Cox proportional hazards regression analysis for prediction of conversion after treatment with antipsychotics.
The three TEN rules
We further developed a probabilistic decision pathway based on the three TEN rules (Figure 4). Specifically, for CHR individuals with a higher score of 10 (the first TEN) for positive symptoms, a lower score of 10 (the second TEN) for negative symptoms, and a higher score of 10 (the third TEN) for general symptoms at the baseline, the benefit of a reduction in the conversion risk with antipsychotic administration emerged gradually (conversion rates decreased by 30% to about 10%).
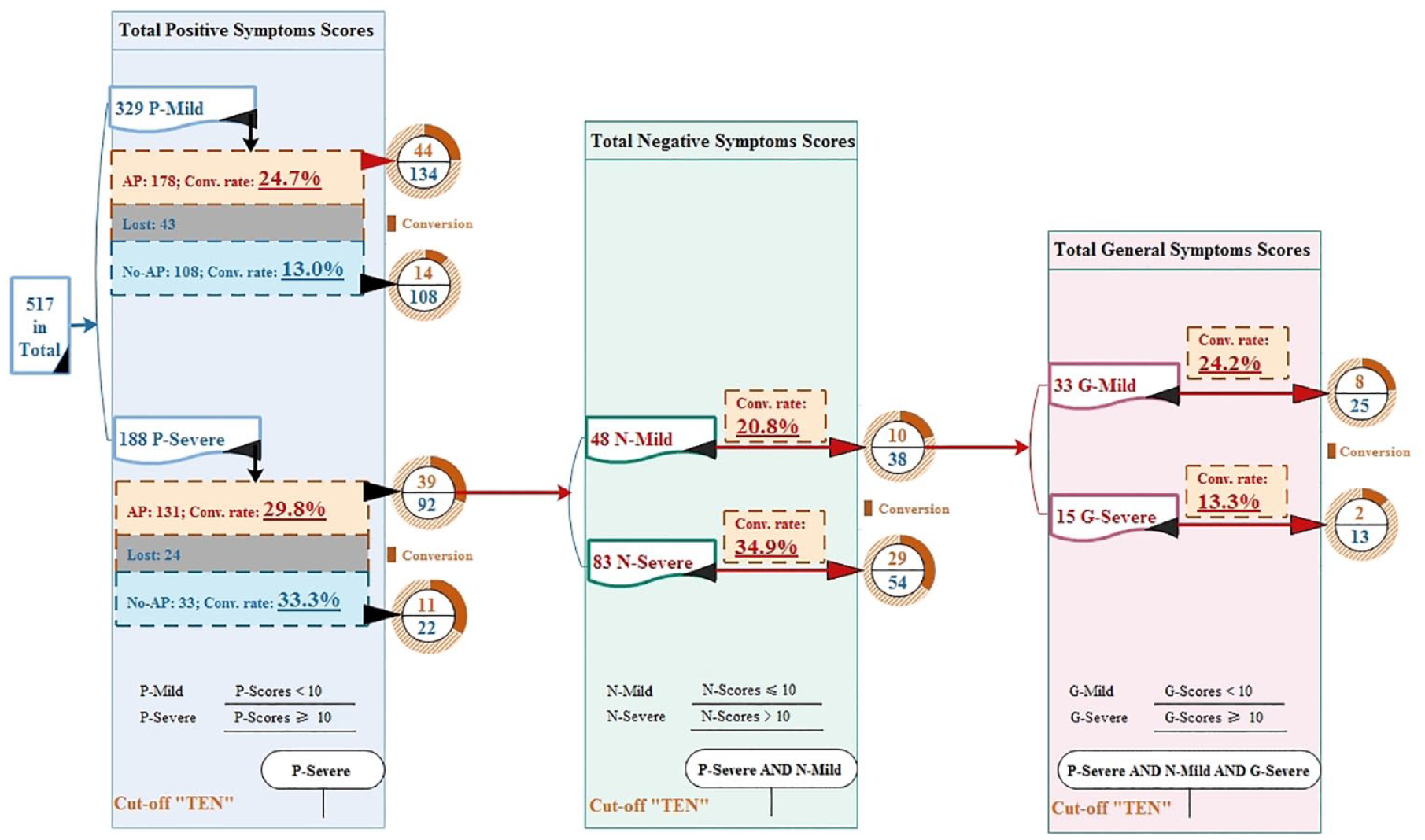
The three TEN rules for antipsychotic treatment decision for CHR individuals.
Discussion
Study elements
To our knowledge, this is the largest CHR cohort analysis of patients treated with antipsychotics to suggest that antipsychotics may not be effective in preventing psychosis among at-risk youth. The SHARP cohort implemented methods similar to those used in NAPLS-2 for the identification of CHR individuals in Mainland China since 2010 and followed up these patients carefully over the subsequent 2–3 years. When the baseline severity of symptoms was considered, no significant difference was detected in the severe CHR group in terms of conversion rate, but even worse, those in the mild CHR group who been treated with antipsychotic were at an increased risk for psychosis. If antipsychotic is prescribed, low-dose, short-term monotherapy is recommended. Our results are not in favour of any specific type of antipsychotic and suggest the three TEN rules for selection of a very small subgroup of CHR individuals (severe positive and general symptoms, but mild negative symptoms) who may benefit from antipsychotic treatment.
The current study adds to the literature in several ways. First, this study fills in the gaps of real-world data to support the guidelines’ recommendations on antipsychotic prescription for the CHR population in time. Second, most prior studies assessed antipsychotic effectiveness in the short-to-medium term with a small, non-representative subset of CHR individuals and overlooked the important real-world interplay and interactions between the sample and the medication taken; this study was pragmatically designed to allow careful assessments and long-term follow-up to address these shortcomings. Third, the large sample size allowed us to stratify antipsychotic administration into different categories instead of the fixed dose and type classifications used in clinical trials. Finally, we summarized some preliminary operational rules for antipsychotic prescription in the CHR population, which are of clear value in improving the clinical practice in early intervention of psychosis.
Prevention of psychosis
The study revealed that antipsychotic should not be regarded as the first-choice intervention for prevention. It seems that the main reason for the limited effects of antipsychotic in the real-world data in this study was that antipsychotic may be effective in stabilizing psychotic symptoms, but may not achieve the target of prevention in the long term. As the finding from the first RCT by McGorry et al. (2002) showed, once CHR individuals were followed up over a longer term, the efficacy of specific preventive interventions will disappear. Another possibility is that the effect of antipsychotics may only be specific for the symptomatic level but not for functional outcomes, which may reflect the real course of progression in psychosis. It is noteworthy that those patients not treated with antipsychotic may have functionally benefited from less stigmatized stress, adverse effect and living in a more ‘normal’ and relaxed environment.
If antipsychotic treatment alone cannot truly prevent psychosis, assessments of other interventions are urgently needed. This study at least strongly reminds clinicians that antipsychotic prescriptions are not completely helpful, and other professional treatment modalities should be considered. In this context, it is crucial to question the clinical practice: why do we continue prescribing antipsychotics for CHR individuals? Did we simply conclude that antipsychotics play the same role in the treatment of psychotic patients as in CHR individuals? These real-world results also indicate that prescription of antipsychotics should be based on CHR individual vulnerability. If antipsychotics can be used for the purpose of symptomatic stabilization (Schmidt et al., 2015) or reducing prodromal symptom severity, (McGlashan et al., 2006) which CHR subtypes may show prevention of psychosis from symptomatic treatment and how can these be identified? These real-world findings provide some valuable lessons and indicate the need for more research to explore answers to the questions raised above.
Clinical implications
This study has important clinical and preventive implications for the management of CHR individuals. First, although non-drug treatments such as CBT (Morrison et al., 2004) are recommended as the first-choice treatment options for CHR individuals by many RCTs and guidelines, antipsychotics are still commonly used in psychiatric practice in China. Our results, in combination with the findings of previous RCTs, suggest that antipsychotics are less effective in reducing conversion to psychosis in CHR individuals and that clinicians should not take it for granted that since antipsychotics can treat psychosis, they can prevent psychosis as well. On the contrary, antipsychotic treatment is associated with much stigma and adverse events, and clinicians should exercise caution while prescribing antipsychotics for youth at risk of psychosis.
Generally, CHR individuals are highly variable in terms of their outcomes, which caused broad debates regarding the use of antipsychotics. Although it not yet sufficient evidences to show who can benefit or be harmed by antipsychotic treatment, current study clearly showed that those CHR individuals with mild level of symptoms should not be exposed to antipsychotics. On the basis of our results, we propose a stricter antipsychotic prescription strategy in preventing psychosis, such as the three TEN rules, in which antipsychotics would be administered to CHR individuals with severe positive and general symptoms, but mild negative symptoms.
Limitations
The present study is subject to some limitations. First, the data may not be representative of the entire Chinese population since recruitment and follow-up were conducted only at a single site. The SMHC is the largest psychiatric service center in China (serving over 800,000 outpatients per year) and provides professional treatment for patients throughout the country, and about half of the current samples were not Shanghai natives. However, although a single-site design may increase sample homogeneity and continuity, it also could limit the generalizability of the findings. Second, similar to other real-world studies, real-world data may be subject to inaccuracies of drug information and missing data. Although we performed tripartite checks-involving the CHR individual, family members and medical records-to confirm the medical treatment details, the accuracy of our approach was insufficient in comparison with other strict methods such as pill counts plus self-report. Furthermore, no data are available regarding side-effects and stigmatized issues to antipsychotic usage in CHR population. In the future, the ongoing Phase-2 SHARP program (Trial Registration: NCT04010864) will record side-effects of antipsychotics in detail. The stigma of taking antipsychotic drugs maybe common in youth (Boyd et al., 2015) at risk and increases both physical and psychological burden to them during this critical premorbid period of psychosis. Third, although our primary outcome of conversion to psychosis had been widely used previously, functional outcomes were not assessed in this analysis. Finally, we did not account for the effect of other medications such as antidepressants, which may also be effective in psychosis prevention (Fusar-Poli et al., 2007).
Conclusion
In a longitudinal, large-scale, naturalistic CHR cohort, our report comprehensively demonstrated negative effectiveness of antipsychotics for youth at risk of psychosis. Prescription of antipsychotic would be more appropriate after thorough careful and individualized assessments, such as for those who meet the three TEN rules. When antipsychotics are prescribed, they may be better suited for a limited time period at a low dose and in monotherapy by targeting symptomatic stabilization, rather than prevention of psychosis. These results provide new insights into real-world antipsychotic prescription for prodromal phase psychosis, which is crucial for improving services and avoiding unnecessary harm in early intervention.
Supplemental Material
Supplemental_data-1 – Supplemental material for Real-world effectiveness of antipsychotic treatment in psychosis prevention in a 3-year cohort of 517 individuals at clinical high risk from the SHARP (ShangHai At Risk for Psychosis)
Supplemental material, Supplemental_data-1 for Real-world effectiveness of antipsychotic treatment in psychosis prevention in a 3-year cohort of 517 individuals at clinical high risk from the SHARP (ShangHai At Risk for Psychosis) by TianHong Zhang, LiHua Xu, XiaoChen Tang, YanYan Wei, Qiang Hu, YeGang Hu, HuiRu Cui, YingYing Tang, Li Hui, ChunBo Li, LiPing Cao, Zheng Lu and JiJun Wang in Australian & New Zealand Journal of Psychiatry
Supplemental Material
Supplemental_data-2 – Supplemental material for Real-world effectiveness of antipsychotic treatment in psychosis prevention in a 3-year cohort of 517 individuals at clinical high risk from the SHARP (ShangHai At Risk for Psychosis)
Supplemental material, Supplemental_data-2 for Real-world effectiveness of antipsychotic treatment in psychosis prevention in a 3-year cohort of 517 individuals at clinical high risk from the SHARP (ShangHai At Risk for Psychosis) by TianHong Zhang, LiHua Xu, XiaoChen Tang, YanYan Wei, Qiang Hu, YeGang Hu, HuiRu Cui, YingYing Tang, Li Hui, ChunBo Li, LiPing Cao, Zheng Lu and JiJun Wang in Australian & New Zealand Journal of Psychiatry
Supplemental Material
Supplemental_data-3 – Supplemental material for Real-world effectiveness of antipsychotic treatment in psychosis prevention in a 3-year cohort of 517 individuals at clinical high risk from the SHARP (ShangHai At Risk for Psychosis)
Supplemental material, Supplemental_data-3 for Real-world effectiveness of antipsychotic treatment in psychosis prevention in a 3-year cohort of 517 individuals at clinical high risk from the SHARP (ShangHai At Risk for Psychosis) by TianHong Zhang, LiHua Xu, XiaoChen Tang, YanYan Wei, Qiang Hu, YeGang Hu, HuiRu Cui, YingYing Tang, Li Hui, ChunBo Li, LiPing Cao, Zheng Lu and JiJun Wang in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
For the purpose of commemorate, Dr. Larry J. Seidman passed away on 7 September 2017. Dr. Robert W. McCarley passed away on 27 May 2017. Both were founders and core members of the SHARP (ShangHai At Risk for Psychosis) project.
Author Contributions
Dr. TH.Z. and JJ.W. conceptualized the study, wrote the first draft of the manuscript and conducted the statistical analyses. LH.X., HR.C. and YY.W. interviewed participants and collected and organized the primary data. YY.T., Q.H., L.H., YG.H. and XC.T. managed the literature searches, statistical analyses and edited the manuscript. CB.L., Z.L., LP.C. and JJ.W. designed the study and provided supervision in the implementation of the study. All authors have approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was supported by Ministry of Science and Technology of China, National Key R&D Program of China (2016YFC1306800), National Natural Science Foundation of China (81671329, 81671332, 81671332, 81971251), Shanghai Key Laboratory of Psychotic Disorders (13dz2260500) Science and Technology Commission of Shanghai Municipality (19ZR1477800, 19ZR1445200, 19441907800, 17411953100, 2018SHZDZX01, 19410710800, 19411969100), Shanghai Jiaotong University Foundation (ZH2018ZDB03, ZH2018QNB19, YG2016QN42), The Clinical Research Center at Shanghai Mental Health Center (CRC2018ZD01, CRC2018ZD04 and CRC2018YB01) and Multi-center Clinical Research Program of Shanghai Jiaotong University School of Medicine (DLY201817).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.