
Abstract
Background:
Australian and US guidelines recommend routine brain imaging, either computed tomography or magnetic resonance imaging, to exclude structural lesions in presentations for first-episode psychosis. The aim of this review was to examine the evidence for the appropriateness and clinical utility of this recommendation by assessing the frequency of abnormal radiological findings in computed tomography and magnetic resonance imaging scans among patients with first-episode psychosis.
Methods:
PubMed and Embase database were searched from inception to April 2018 using appropriate MeSH or Emtree terms. Studies were included in the review if they reported data on computed tomography or magnetic resonance imaging scan findings of individuals with first-episode psychosis. No restriction on the geographical location of the study or the age of participants was applied. We calculated the percentage of abnormal radiological findings in each study, separately by the two diagnostic methods.
Results:
There were 16 suitable studies published between 1988 and 2017, reporting data on an overall 2312 patients with first-episode psychosis. Most were observational studies with a retrospective design and the majority examined patients with computed tomography. While structural abnormalities were a relatively common finding, these rarely required clinical intervention (range across studies: 0–60.7%; median: 3.5%) and were very rarely the cause of the psychotic symptoms (range: 0–3.3%; median: 0%). Only 2 of the 16 studies concluded that brain imaging should be routinely ordered in first-episode psychosis.
Conclusion:
There is insufficient evidence to suggest that brain imaging should be routinely ordered for patients presenting with first-episode psychosis without associated neurological or cognitive impairment. The appropriate screening procedure for structural brain lesions is conventional history-taking, mental status and neurological examination. If intracranial pathology is suspected clinically, a magnetic resonance imaging or computed tomography scan should be performed depending on the clinical signs, the acuity and the suspected pathology. National guidelines should reflect evidence-based data.
Introduction
Since Weinberger (1984) first proposed the use of computed tomography (CT) in first-episode psychosis in 1984, neuroimaging has been part of the medical work-up of these cases to exclude contributory neurological conditions. Recommendations for brain imaging have been incorporated into practice guidelines although considerable disparity remains among national guidelines about whether scanning should be routinely undertaken (Table 1).
Guidance about neuroimaging in first-episode psychosis.
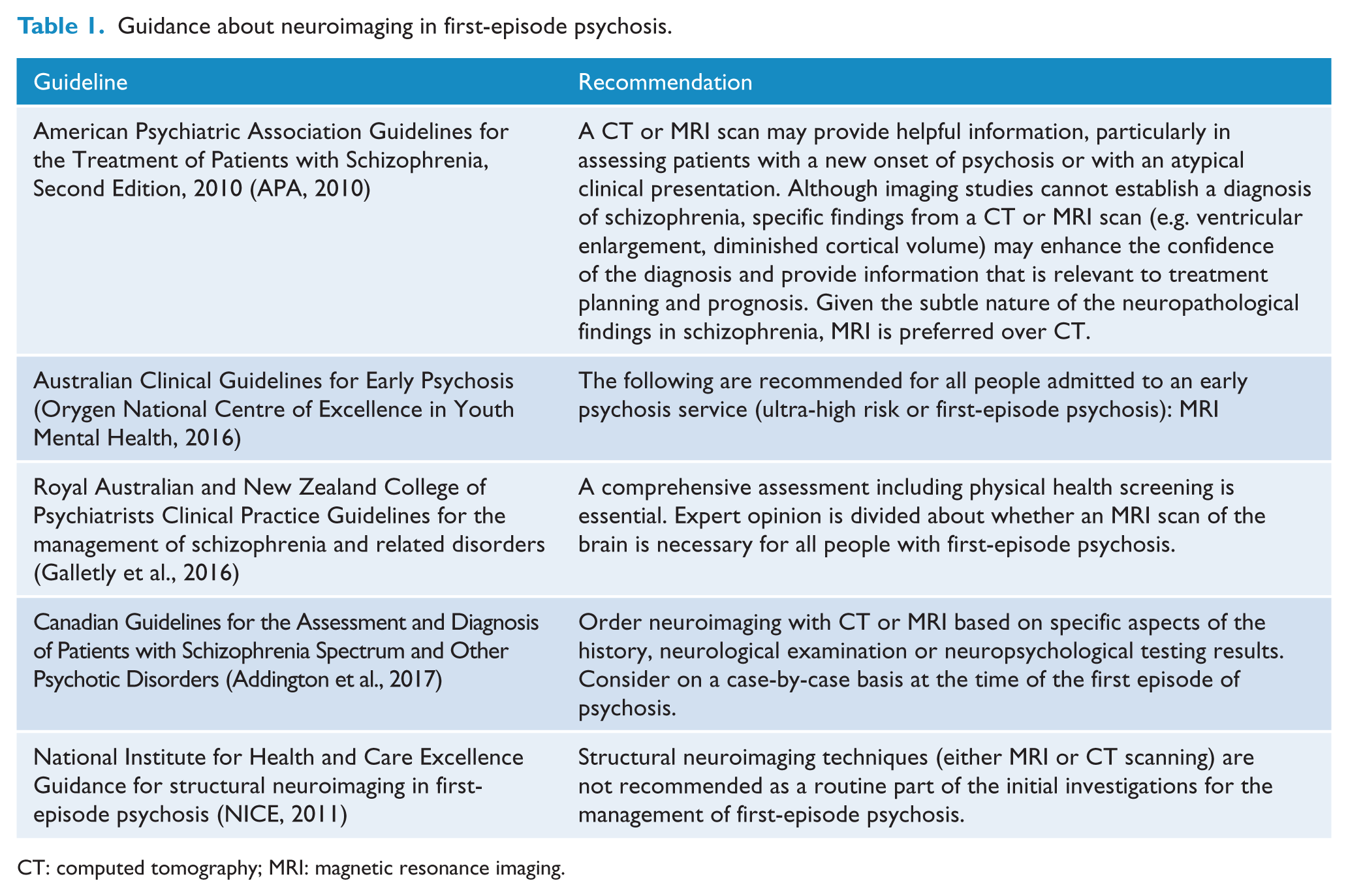
CT: computed tomography; MRI: magnetic resonance imaging.
The aim of this study is to systematically review the evidence for the clinical utility of CT or magnetic resonance imaging (MRI) in first-episode psychosis. In particular, we assessed the frequency of abnormal radiological findings in CT and MRI scans among patients who were admitted to hospital with first-episode psychosis. This review updates previous reviews by Albon et al. (2008), Goulet et al. (2009) and The National Institute for Health and Care Excellence (NICE, 2011) with new data. All of these reviews have concluded that routine neuroimaging is not indicated in first-episode psychosis.
Method
The methods are based on the Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA; Moher et al., 2009). We searched PubMed and Embase up to April 2018 using the following text, MeSH or Emtree terms as appropriate: (early OR first OR first-episode OR ‘first episode’) AND (psychosis OR psychotic OR schizophreniform) AND (neuroimaging OR ‘brain imaging’ OR CT OR MRI OR ‘computed tomography’ OR ‘magnetic resonance imaging’). The initial search was performed by M.F. The selected abstracts (109 papers) were reviewed by M.F., D.S. and M.B. to determine whether they met inclusion criteria. We (M.F., D.S. and M.B.) searched for further publications by scrutinising the reference lists of initial studies identified and other relevant review papers. M.F. contacted selected authors and experts to obtain further data where necessary. Radiological findings were classified by two authors (D.V. and S.S.). Conflicts between the three reviewers were resolved by discussion.
Our inclusion criteria were as follows: retrospective or prospective studies with primary data collection that included data on the radiological findings in individuals with first-episode psychosis. We applied no restriction on the geographical location of the study or the age of participants. We excluded studies that did not specifically state participants had first-episode psychosis and excluded morphological brain studies that provided volumetric or other data but did not provide radiological diagnosis. Only English-language studies were included.
In the data extraction phase, information on study design, number, age and sex of participants, as well as the field-strength of MRI scan (if available), was collected from all included studies. We utilised the same methodology as used by Goulet et al. (2009) and classified brain scans as follows:
Normal;
Abnormal, with radiological findings having no clinical impact: benign or nonspecific findings with no implication on diagnosis, management or treatment;
Abnormal, with radiological findings having an implication on management or treatment, but an unlikely causal link to psychotic symptoms;
Abnormal, with radiological findings having an implication on management or treatment, and a possible causal link to psychotic symptoms.
The number of patients who belonged to any of the above categories, together with their radiological diagnosis in case of abnormal findings, was extracted from each study. From this information, we calculated the percentage of patients with these outcomes from all scanned individuals. Data are presented separately in each study by CT and MRI scans. The data extraction procedure was led by the first author (M.F.), but D.S. and M.B. also checked the accuracy of reported values.
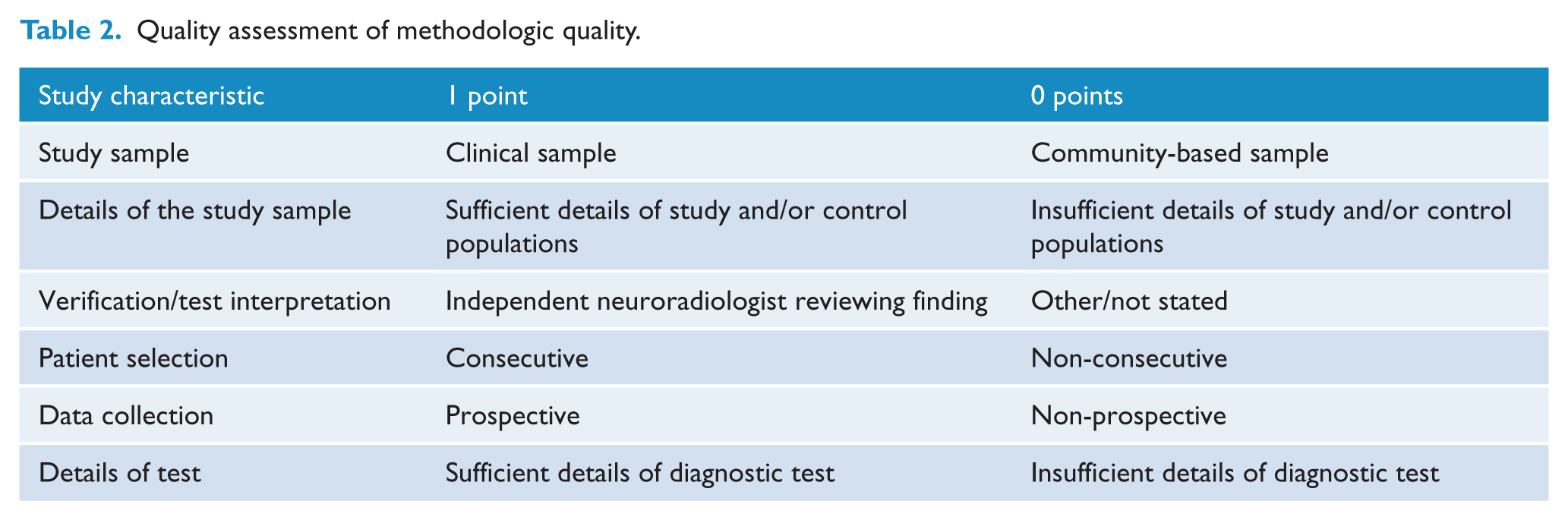
We (M.F., D.S. and M.B.) independently assessed methodological quality using a modified version of quality assessment tool used by Rao et al. (2005) which rates studies examining the clinical utility of a test based on details of study sample and patient selection, data collection, and verification and details of the test (Table 2).
Quality assessment of methodologic quality.
Results
There were 2314 citations of interest in the initial electronic searches, of which 109 abstracts were screened. Of these, 22 full-text papers were potentially relevant and assessed for eligibility. Nine papers were excluded for reasons listed in Figure 1. Three additional papers were found from the reference lists of other papers from the database search. This left 16 papers, 6 which were published since the most recent review (NICE, 2011) (Figure 1). For each paper, the percentage of participants with the specific outcome was provided according to the classification system outlined above.
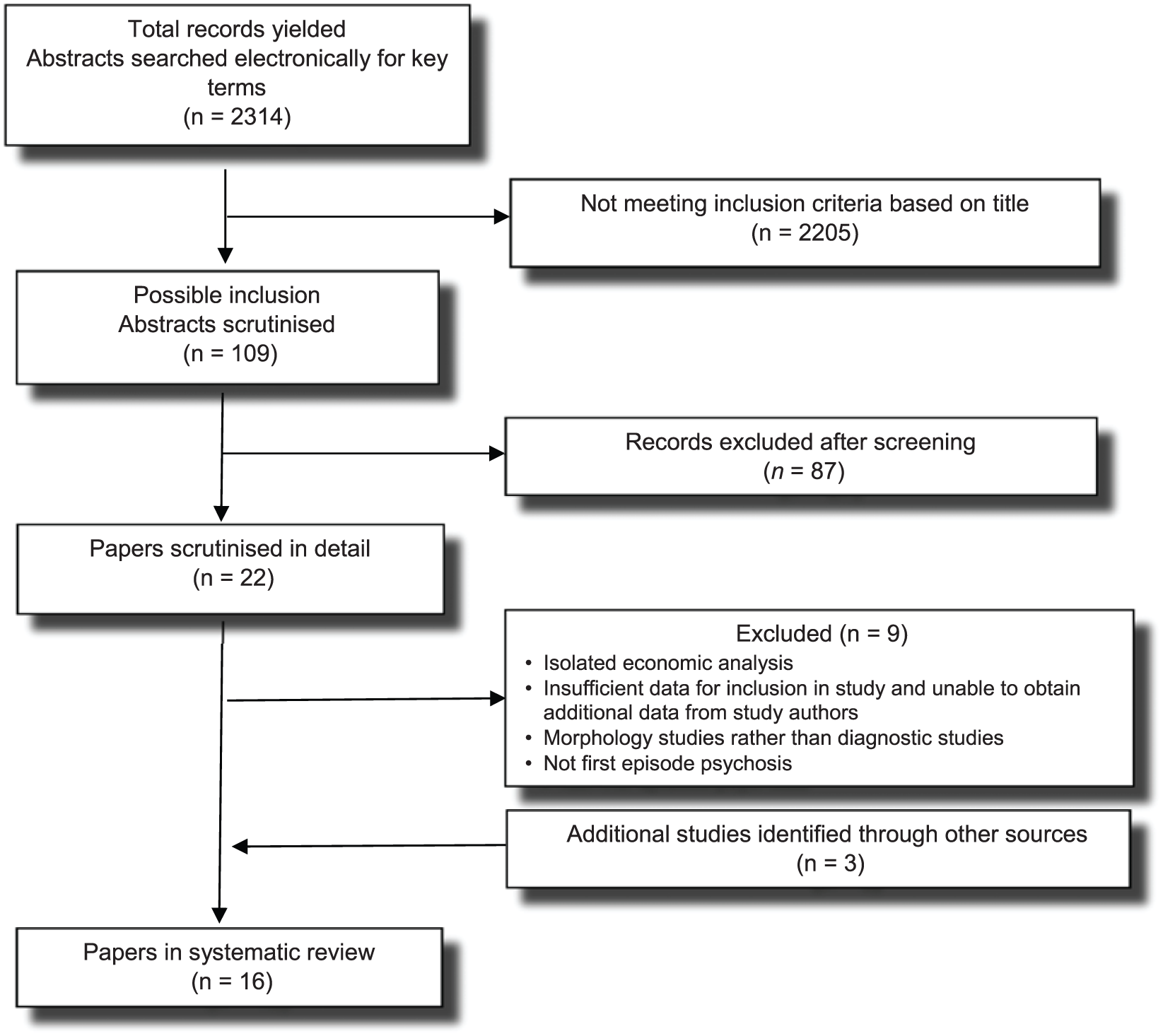
Search strategy.
Of the 16 studies, 13 were retrospective audits of medical records, 2 were prospective case series and 1 was a case-control study (Table 3). Sample sizes ranged from 30 to 349, and overall, they examined 2312 patients. Two studies considered the diagnostic characteristics of tests (sensitivity and specificity) and the costs of potentially unnecessary scans but none provided details or an economic analysis. None of the studies gave follow-up data and none were randomised controlled trials or before–after studies. Six papers came from the United States, three from Australia, two each from the United Kingdom and Canada, and one from Switzerland, the Netherlands and Portugal.
Radiological findings.
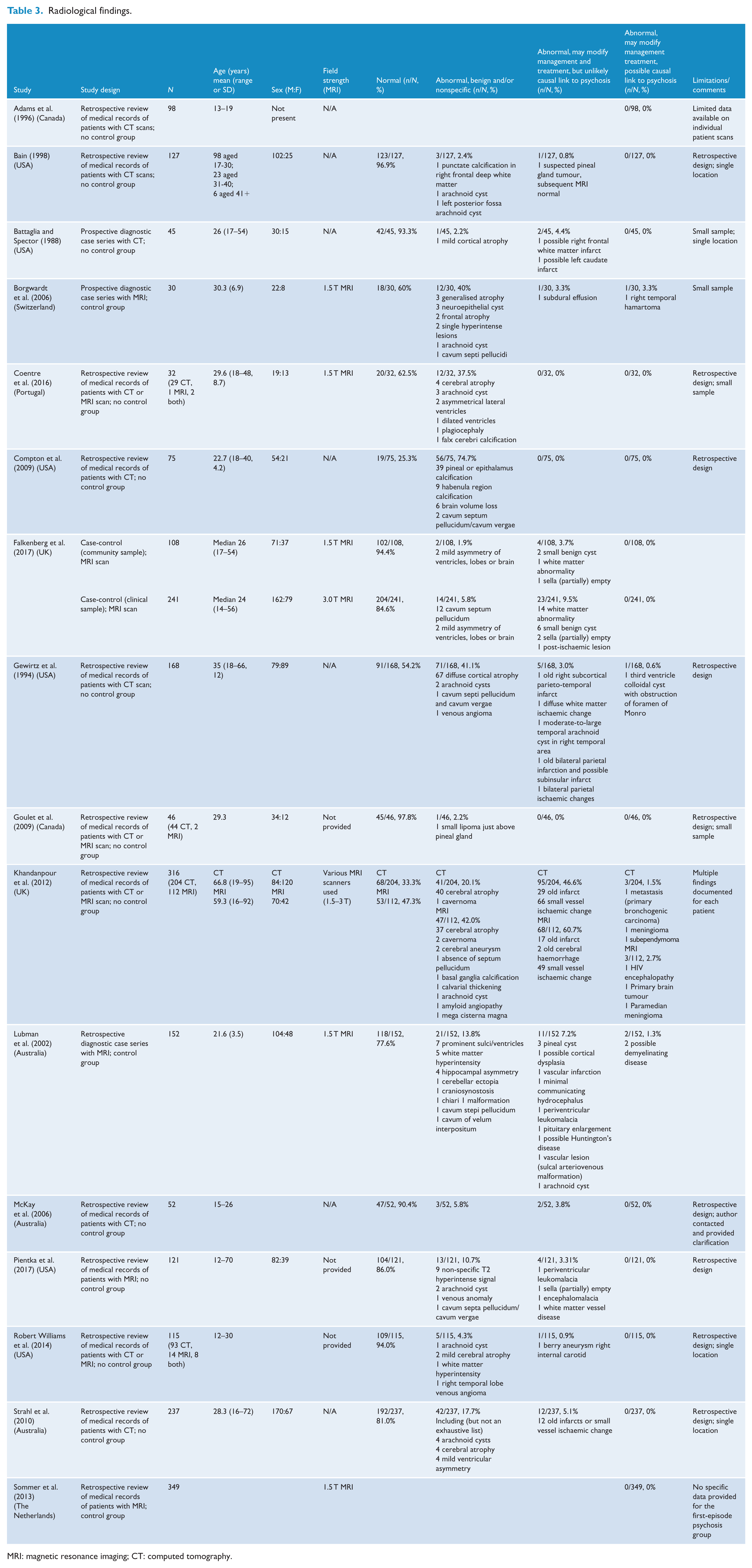
MRI: magnetic resonance imaging; CT: computed tomography.
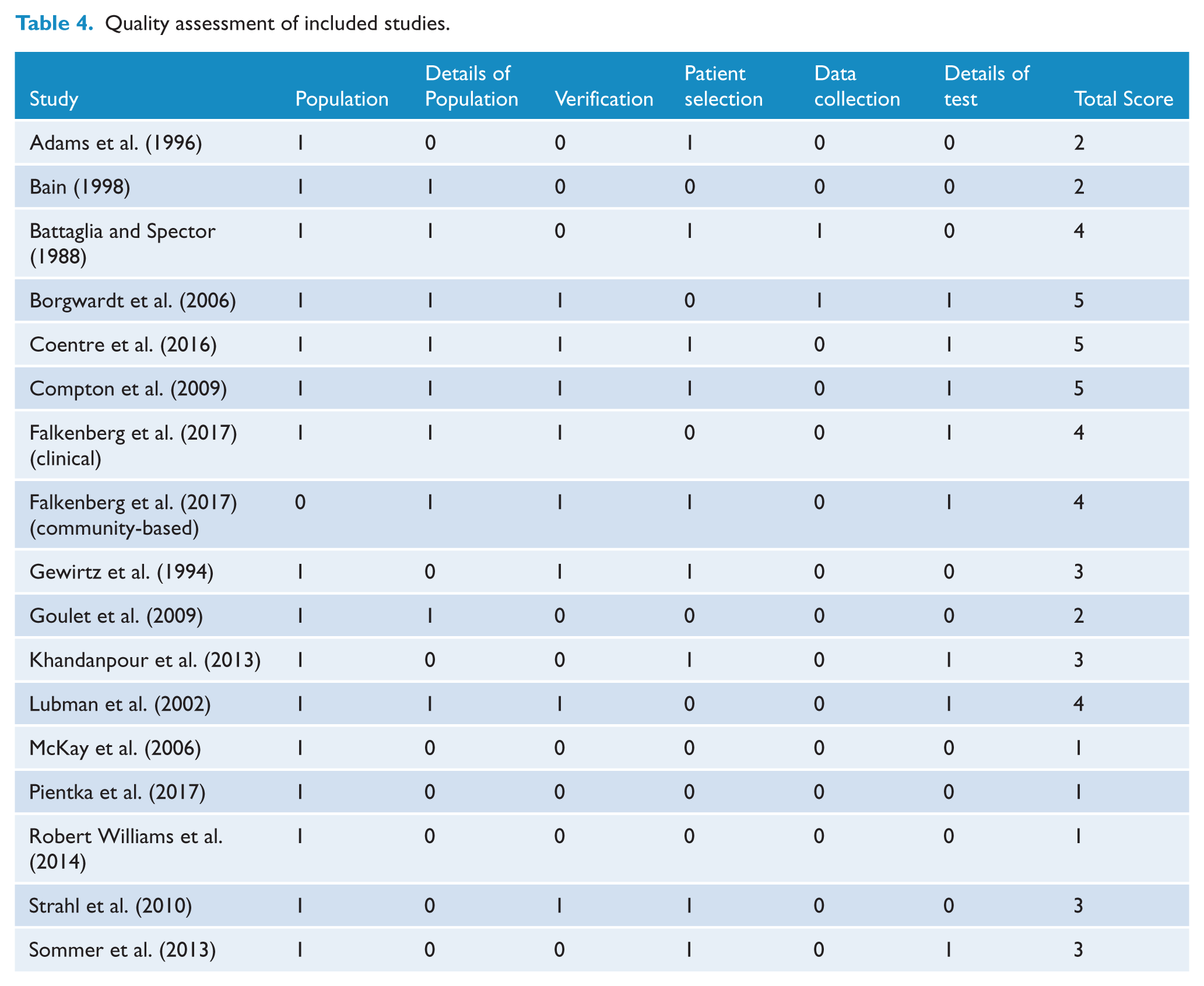
The included studies were of variable quality. From the maximum possible quality score of 6 points, seven studies scored 4 or 5 and were considered as adequate or high quality. However, six of the reviewed studies had an overall score of 1 or 2, suggesting low quality (Table 4).
Quality assessment of included studies.
CT
In one retrospective analysis (Bain, 1998), there were four incidental radiological abnormalities of 127 individuals scanned, none of which were causally related to psychosis, while in another of 52 patients with first-episode psychosis (McKay et al., 2006), none had abnormalities potentially related to psychosis. The same finding was made in a retrospective analysis of 75 patients (Compton et al., 2009) and of 98 patients (Adams et al., 1996). Furthermore, Strahl et al. (2010) reviewed 237 consecutive patients who had CT scans for first-episode psychosis with no focal neurological signs. None of those scanned had abnormalities related to psychosis.
In a retrospective analysis (Gewirtz et al., 1994), 1 of the 168 individuals scanned (0.6%) had incidental findings that may have been causally related to psychosis. Individuals were examined but it is unclear whether neurological findings on clinical examination were present in the individuals with psychosis. In another study, this time a prospective diagnostic case series (Battaglia and Spector, 1988), 3 of 45 individuals had incidental abnormalities although none of these abnormalities were considered implicated in psychosis. This study excluded individuals with drug-induced psychosis, thus the ‘hit rate’ for identifying lesions responsible for psychosis was likely higher than studies that did not exclude this group.
MRI
Borgwardt et al. (2006) used MRI to assess the prevalence of radiological abnormalities in individuals with first-episode psychosis and compared this to individuals at high risk of schizophrenia. The rate of radiological abnormality in the first-episode psychosis group was 40%, but only 2 of the 30 individuals with first-episode psychosis had clinically relevant pathology – a subdural effusion and right temporal hamartoma. The authors did not identify whether these individuals had findings on neurological examination.
Similarly, a case-control study of a clinical and community-based sample found radiological abnormalities in 15% of the former and 6% of the community-based sample although none of the abnormalities required intervention or were related to psychosis (Falkenberg et al., 2017). Despite this finding, the authors concluded by recommending routine MRI in the clinical assessment of all patients presenting with first-episode psychosis.
A further study used a research sample that excluded individuals with a history of head injury, seizures, neurological disease, and alcohol or substance use disorder (Lubman et al., 2002). The authors classified abnormalities as requiring no referral, routine referral or urgent referral. In re-examining the cases identified in their sample, 2 of 152 cases (1.3%) may have potentially been casually related to psychosis.
Finally, retrospective reviews of the medical records of 349 (Sommer et al., 2013) and 121 (Pientka et al., 2017) patients with first-episode psychosis found no abnormalities related to psychosis.
Both imaging modalities (CT and MRI)
Khandanpour et al. (2013) retrospectively reviewed 112 consecutive MRI scans and 204 consecutive CT scans for individuals with first-episode psychosis but no neurological signs. Three of 112 (2.7%) individuals who had MRI and three of 204 (1.5%) individuals who had CT had incidental brain lesions potentially accountable for psychosis. This study included older patients who were more likely to have an organic cause for psychosis. A second retrospective review of 32 consecutive admissions who received a CT, MRI or both found none had incidental brain abnormalities potentially accountable for psychosis (Coentre et al., 2016). Two further retrospective reviews of 46 (44 CT and 2 MRI; Goulet et al., 2009) and 115 individuals (Robert Williams et al., 2014) with first-episode psychosis reported similar negative findings.
Discussion
Clinicians order brain imaging to exclude neurological abnormalities in individuals with first-episode psychosis. However, the available data suggest a disappointing yield from routine neuroimaging in individuals at low risk of a specific brain abnormality.
This systematic review includes 2312 individual patients who were scanned with CT or MRI. While structural abnormalities were a relatively common finding, these rarely required clinical intervention (range across studies: 0–60.7%; median: 3.5%) and were very rarely the cause of the psychotic symptoms (range: 0–3.3%; median: 0%). Across all studies, only 10 of the 2312 individual subjects had abnormalities that may have been causally related to psychosis (0.4%). It is apparent that incidental radiological abnormalities are more common in older individuals, as has been identified in a large meta-analysis of 20,000 individuals (Morris et al., 2009). This review therefore supports the conclusion by Hollister and Boutros (1991) that older age is most predictive of abnormalities in individuals with first-episode psychosis.
The clinical utility of a test is related to its diagnostic utility. The diagnostic utility of a screening test, such as brain imaging in first-episode psychosis, depends on a number of variables including the sensitivity and specificity of the test, the prevalence of the disease being tested for and the positive predictive value of the test (Adams et al., 1996). The imaging modality used will thus have an impact on the number and type of abnormalities detected. This is demonstrated in Khandanpour et al. (2013), where more lesions were detected with MRI versus CT and in Falkenberg et al. (2017), where the group scanned with 3 T MRI had more abnormal scans than those scanned with 1.5 T MRI scans. Other factors which may explain the wide variation of abnormalities reported across studies are the prevalence of the abnormalities being tested for and the variation in training, experience and reporting methods of the reporting radiologist(s). As outlined, the prevalence of neurological conditions explaining psychosis is low, although it increases in older individuals. Given the low positive predictive value in first-onset psychosis in adolescents, false-positive tests will be more common than true-positive tests (Adams et al., 1996). In 1000 healthy volunteers, 82% of MRI scans were completely normal. Of the ‘abnormal scans’, only 1.1% required urgent referral, with the remainder representing false-positive tests that may have caused worry (Katzman et al., 1999).
Clinicians continue to order neuroimaging because of clinical practice guidelines, the desire to establish the ‘functional’ character of the psychosis, and a fear of missing a potentially treatable cause of psychosis or serious neurological illness, which may result in medicolegal risk (Freudenreich et al., 2009). This may relate to availability bias in the clinician due to a misperception of how common causative ‘organic’ findings are, in part due to case reports that resonate with clinicians (Kasinathan et al, 2017; Kuehn, 2014).
Given the growing amount of data demonstrating the low clinical yield of neuroimaging in first-episode psychosis, the Canadian Psychiatric Association has recently modified its guidelines from an earlier recommendation that brain imaging be considered as part of a routine investigation of all patients with first-episode psychosis (Addington et al., 2017). The Canadian guidelines now state that ‘imaging is indicated in the presence of signs and symptoms suggestive of intracranial pathology including headaches, nausea and vomiting, seizure-like activity, and later age at the onset of symptoms’ (Addington et al., 2017). This is reflected in the recommendations of Choosing Wisely in both Canada and the United Kingdom that clinicians do not routinely order neuroimaging in first-episode psychosis in the absence of signs or symptoms suggestive of intracranial pathology (Choosing Wisely Canada, 2017; Choosing Wisely UK, 2018). The recommendation of the American Psychiatric Association Practice Guidelines for the Psychiatric Evaluation of Adults is that, the decision to do laboratory studies and other clinical tests, such as imaging studies … should be based on the likelihood that the test result will alter diagnostic or treatment-related decision making. The costs of ‘routine’ testing, in financial terms and in unneeded evaluations for false positive results, are unlikely to offset the benefits of untargeted testing (APA, 2016).
Our results support this statement with respect to brain imaging in first-episode psychosis. Based on the available data, it should not be routinely performed. Prospective studies may provide further higher quality data to inform clinical practice (Jonsdottir and Briem, 2016).
The Royal Australian and New Zealand College of Psychiatrists (RANZCP) guidelines highlight the difference in opinion on the need for brain imaging (Galletly et al., 2016). In contrast to this uncertainty and the outright opposition to routine scanning in all cases of first-episode psychosis in the UK and Canadian guidelines, the Australian Orygen guidelines, updated in 2016, continue to recommend neuroimaging in first-episode psychosis (Orygen National Centre of Excellence in Youth Mental Health, 2016). This recommendation is not supported by the findings of this review.
While there are research indications for brain imaging in first-episode psychosis, these have only identified abnormalities at an aggregated population level rather than in clinical settings (Bartholomeusz et al., 2017; Fusar-Poli and Meyer-Lindenberg, 2016). There is no evidence to support the use of voxel-based morphology to diagnose schizophrenia in patients with first-episode psychosis (Palaniyappan et al., 2015).
Even with six more studies than earlier reviews, there were only 16 papers, a low number considering all MRI studies on first-episode psychosis. There were limitations in the available studies. Most had methodological problems, were of retrospective design and of heterogenous populations. It was not clear in several studies whether the same CT or MRI machine was used, what type of machine was used or whether scans were reported by the same neuroradiologist. There was a risk of selection bias in some studies where patients were included in a non-consecutive manner. There was also unclear documentation about whether a neurological examination was performed in all studies. No studies provided details of diagnostic measures (sensitivity, specificity or area under the curve) or economic analysis.
Conclusion
While clinicians must remain cognisant that patients presenting with first-episode psychosis have higher rates of underlying neurological abnormalities compared to healthy individuals, the available data do not support routine ordering of brain imaging for first-episode psychosis in the absence of clinical signs, symptoms or antecedents suggestive of an underlying medical or neurological disorder. The appropriate screening procedure for structural brain lesions is conventional history-taking, mental status and neurological examination. If intracranial pathology is suspected clinically, an MRI or CT scan should be performed depending on the clinical signs, the acuity and the suspected pathology.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.