
Abstract
Objective:
The treatment of bipolar disorder is challenging because of its clinical complexity and availability of multiple treatment options, none of which are ideal mood stabilizers. This survey studies prescription practices of psychiatrists in India and their adherence to guidelines.
Method:
In total, 500 psychiatrists randomly selected from the Indian Psychiatric Society membership directory were administered a face-to-face 22-item questionnaire pertaining to the management of bipolar disorder.
Results:
For acute mania, most practitioners preferred a combination of a mood stabilizer and an atypical antipsychotic to monotherapy. For acute depression, there was a preference for a combination of an antidepressant and a mood stabilizer over other alternatives. Electroconvulsive therapy was preferred in the treatment of severe episodes and to hasten the process of recovery. Approximately, 50% of psychiatrists prescribe maintenance treatment after the first bipolar episode, but maintenance therapy was rarely offered lifelong. While the majority (85%) of psychiatrists acknowledged referring to various clinical guidelines, their ultimate choice of treatment was also significantly determined by personal experience and reference to textbooks.
Limitations:
The study did not study actual prescriptions. Hence, the responses to queries in the survey are indirect measures from which we have tried to understand the actual practices, and of course, these are susceptible to self-report and social-desirability biases. This was a cross-sectional study; therefore, temporal changes in responses could not be considered.
Conclusion:
Overall, Indian psychiatrists seemed to broadly adhere to recommendations of clinical practice guidelines, but with some notable exceptions. The preference for antidepressants in treating depression is contrary to general restraint recommended by most guidelines. Therefore, the efficacy of antidepressants in treating bipolar depression in the context of Indian psychiatrists’ practice needs to be studied systematically. Not initiating maintenance treatment early in the course of illness may have serious implications on the long-term outcome of bipolar disorder.
Introduction
Bipolar disorder often starts in adolescence or early adulthood and typically runs an episodic course (Angst and Sellaro, 2000), but many patients do not remit completely and continue to have persistent mood symptoms (Judd and Schettler, 2010). Over the course of a lifetime, the illness is associated with significant disability and high suicide risk (Malhi et al., 2018a). Therefore, aggressive treatment of acute episodes and prevention of recurrences have become major treatment goals (Novick et al., 2010).
Numerous pharmacological options are now available to treat bipolar disorder although no one drug can fully satisfy the definition of an ideal mood stabilizer (MS) (Malhi et al., 2018b). Several classes of drugs are used to treat bipolar disorder, namely, MSs, antipsychotics and antidepressants. Some of these are effective antimanic drugs, but not all are equally effective in treating bipolar depression (Malhi et al., 2012). There is also a great deal of uncertainty as to whether antidepressants are effective and safe in the treatment of bipolar depression (Gijsman et al., 2004; McGirr et al., 2016; Malhi, 2015; Sidor and MacQueen, 2011).
In view of the complexities involved in treating bipolar disorder, several guidelines have been developed to help clinicians make appropriate treatment decisions with the aim of ensuring evidence-based care is provided to people suffering from the illness (American Psychiatric Association (APA), 2002; Grunze et al., 2009, 2010, 2013; Goodwin et al., 2016; Licht et al., 2003; Malhi et al., 2015a; National Institute for Health Clinical Excellence (NICE), 2014; Shah et al., 2017; Yatham et al., 2018). The recent Canadian Network for Mood and Anxiety Treatments/International Society for Bipolar Disorders (CANMAT-ISBD) guidelines, in addition to grading the level of evidence, have also introduced hierarchical recommendations for treatment based on the efficacy of each treatment across all phases, as well as acute and maintenance safety and tolerability and the risk of a treatment emergent switch. For example, if two treatments are similarly effective in treating acute bipolar depression, but only one of these is effective in preventing both depressive and manic relapses, or has better safety or tolerability, then the treatment with a broader profile and/or better tolerability is ranked higher.
In practice, adherence to clinical guidelines may improve treatment outcomes in bipolar disorder (Bauer et al., 2009). However, there are data from North America (Bauer, 2002; Bauer et al., 2009; Lim et al., 2001; Perlis, 2007; Smith et al., 2008) and Europe (Morriss, 2008; Samalin et al., 2011; Vieta and Morralla, 2007), which suggest that despite the availability of many evidence-based guidelines, treatment decisions of practising physicians are not always guideline-based. In this regard, there is no data from India on the prescription patterns of psychiatrists in bipolar disorder. Therefore, this study explores the prescription practice and adherence to guidelines among practicing psychiatrists in India by directly questioning practitioners using a questionnaire specially developed for the study.
Method
Study design
We conducted a questionnaire-based survey of psychiatrists with at least 3 years of clinical practice experience in India after completing post graduation in psychiatry. This was a collaborative research project undertaken by the Society for Bipolar Disorders, India (SBDI) with support from GlaxoSmithKline (GSK).
Data collection
Ipsos Healthcare (Mumbai), an international Clinical Research Organization (CRO), executed the study. Specifically, Ipsos Healthcare recruited psychiatrists and administered the survey face-to-face through field executives. An Independent Ethics Committee (IEC) approved the protocol, the questionnaire and the consent form. Participation of the psychiatrists was voluntary. All participants provided prior written informed consent. Participants were not paid any fee/honorarium for their participation in the study.
Considering that approximately 5000 psychiatrists are practising in India, a sample size of 500 (approximately 10% of psychiatrists practising in India) was considered sufficient to give a fair representation of each of the various geographic locations within the population of interest. To get completed questionnaires from 500 participants, it was planned to contact 1000 psychiatrists meeting eligibility criteria. A computer-generated randomization table was used to select the names of participants from the directory of the Indian Psychiatric Society (IPS) and from the database of the CRO for some north-eastern regions of the country. Names of the participants were distributed to the respective telecallers. CRO divided equally the names of psychiatrists into 4–5 parts (depending upon the number of telecallers), and each of the telecallers approached and contacted these psychiatrists until the sample size for that particular location was achieved. The sample of 500 participants included equal representation of 125 participants from each of the four zones of the India (North, South, East and West). For a comprehensive coverage of the psychiatrists across a zone, 80 psychiatrists were selected from metropolitan cities (⩾1 million population) and the remaining 45 from urban (>100,000, but less than a million) areas. The total number of interviews achieved was monitored on a daily basis. Once the number of interviews per city achieved a target sample size, fieldwork for that city was stopped.
The CRO personnel went through the questionnaires and collected the missing and/or incomplete data from the participants. A study coordinator performed quality control of approximately 20% of the completed questionnaires. Queries related to inconsistent/missing data from a particular participant were resolved by seeking further clarification from the survey participant through the designated field executive. GSK reviewed only fully anonymized completed data collection forms. GSK had no access to any personally identifiable participant information. Confidentiality of study participants was maintained throughout the conduct of the study.
Questionnaire
A committee of experts comprising members of the SBDI, an affiliate of the International Society for Bipolar Disorders (M.S.R., Y.C.J.R., V.J., R.N. and N.S.) developed a 22-item questionnaire, in collaboration with GSK India. The committee deliberated in detail the content of the questionnaire keeping in mind the practice environment in India and the results of some of the surveys conducted elsewhere in the world (Bauer, 2002; Bauer et al., 2009; Lim et al., 2001; Morriss, 2008; Perlis, 2007; Samalin et al., 2011; Smith et al., 2008). The questionnaire included the following aspects pertaining to the treatment of bipolar disorder: treatment of acute mania, depression (bipolar disorder type I and bipolar disorder type II) and rapid cycling; use of antidepressants in bipolar disorder type I and bipolar disorder type II; initiation and duration of prophylaxis/maintenance treatment; choice of medications for prophylaxis; use of electroconvulsive therapy (ECT); and utility of guidelines in the routine treatment of bipolar disorder. For questions on medication dose/combinations, we provided an exhaustive list of options to choose from. Respondents were expected to fill in their first, second and third preferences for a given indication (e.g. acute mania) from the options provided. For example, for treatment of acute mania, the following options were provided: lithium alone, lithium with benzodiazepine, valproate alone, valproate with benzodiazepine, carbamazepine/oxcarbamazepine with and without benzodiazepine, MS (lithium, valproate, carbamazepine/oxcarbamazepine) + atypical antipsychotic, MS + typical antipsychotic, antipsychotics alone, ECT + antipsychotics and ECT + MS + antipsychotic. For certain questions such as indication for prophylaxis (after first episode/second episode/multiple episodes), use of ECT and indications for ECT, we asked the respondents to choose one of the five options provided (always, mostly, sometimes, rarely and never). For example, how often do you use ECT in bipolar disorders was followed by the aforementioned five choices.
Data analysis methods
Descriptive statistics using the frequency counts of the responses to each question of the interview were generated. No formal statistical modeling was performed for data analysis.
Results
The study included 500 practicing psychiatrists (male = 402 [80%] and female = 98 [20%]). The majority came from metropolitan cities (n = 396, 79%) and the remainder from urban areas. Mean and median years of practice was 14.74 (SD 10.49) and 10 years, respectively. A total 231 psychiatrists (n = 231, 46%) were in clinical practice for less than 10 years.
Acute mania
For the treatment of acute mania, a combination of an MS (lithium, valproate and carbamazepine/oxcarbamazepine) and an antipsychotic (particularly an atypical antipsychotic) was the preferred choice for the majority (65%), followed by an MS with or without a benzodiazepine (24%), while an antipsychotic alone was the third preference (8%) (Table1).
Treatment of acute mania (N = 500).
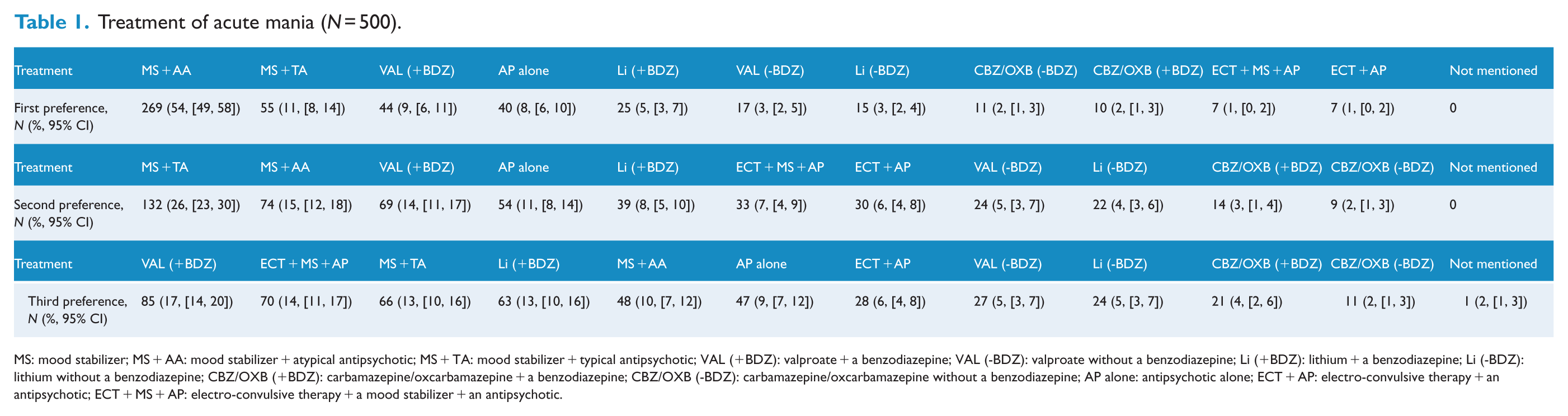
MS: mood stabilizer; MS + AA: mood stabilizer + atypical antipsychotic; MS + TA: mood stabilizer + typical antipsychotic; VAL (+BDZ): valproate + a benzodiazepine; VAL (-BDZ): valproate without a benzodiazepine; Li (+BDZ): lithium + a benzodiazepine; Li (-BDZ): lithium without a benzodiazepine; CBZ/OXB (+BDZ): carbamazepine/oxcarbamazepine + a benzodiazepine; CBZ/OXB (-BDZ): carbamazepine/oxcarbamazepine without a benzodiazepine; AP alone: antipsychotic alone; ECT + AP: electro-convulsive therapy + an antipsychotic; ECT + MS + AP: electro-convulsive therapy + a mood stabilizer + an antipsychotic.
Acute bipolar depression
For the treatment of acute bipolar I depression, a combination of an MS and a selective serotonin reuptake inhibitor (SSRI) was the preferred option followed by an MS + quetiapine and olanzapine + fluoxetine combination (OFC) (Table 2). Almost a similar pattern is noted for bipolar II depression with a preference for OFC and MS + SSRI over MS + quetiapine (Table 3). Very few respondents preferred to use antidepressants alone in the treatment of acute bipolar depression.
Treatment of acute bipolar I depression (N = 500).
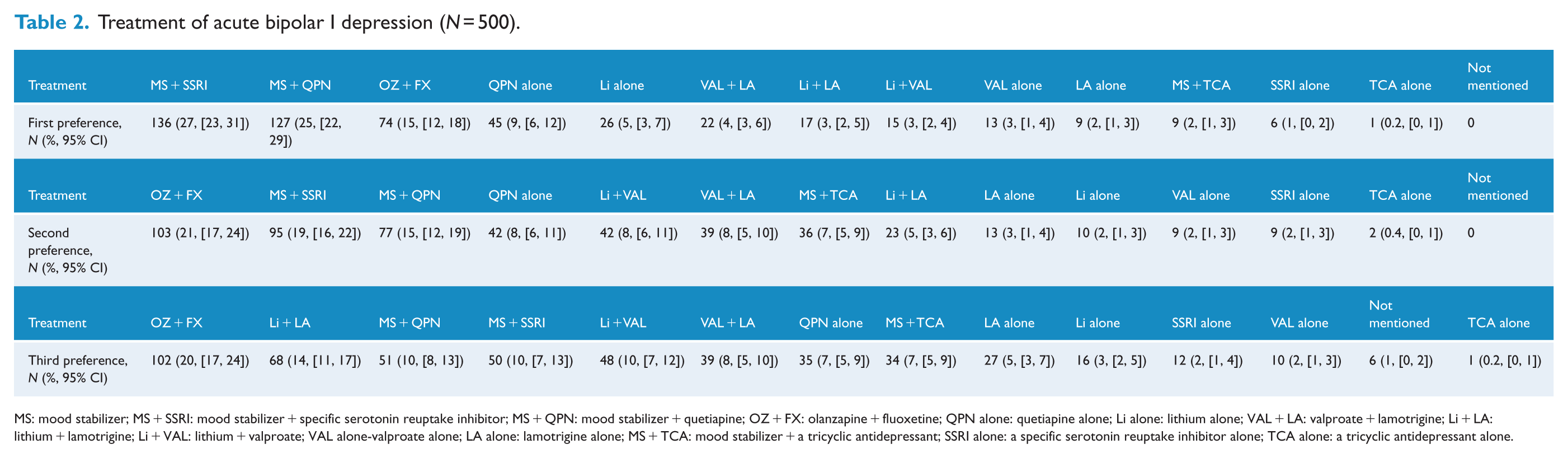
MS: mood stabilizer; MS + SSRI: mood stabilizer + specific serotonin reuptake inhibitor; MS + QPN: mood stabilizer + quetiapine; OZ + FX: olanzapine + fluoxetine; QPN alone: quetiapine alone; Li alone: lithium alone; VAL + LA: valproate + lamotrigine; Li + LA: lithium + lamotrigine; Li + VAL: lithium + valproate; VAL alone-valproate alone; LA alone: lamotrigine alone; MS + TCA: mood stabilizer + a tricyclic antidepressant; SSRI alone: a specific serotonin reuptake inhibitor alone; TCA alone: a tricyclic antidepressant alone.
Treatment of acute bipolar II depression (N = 211). a
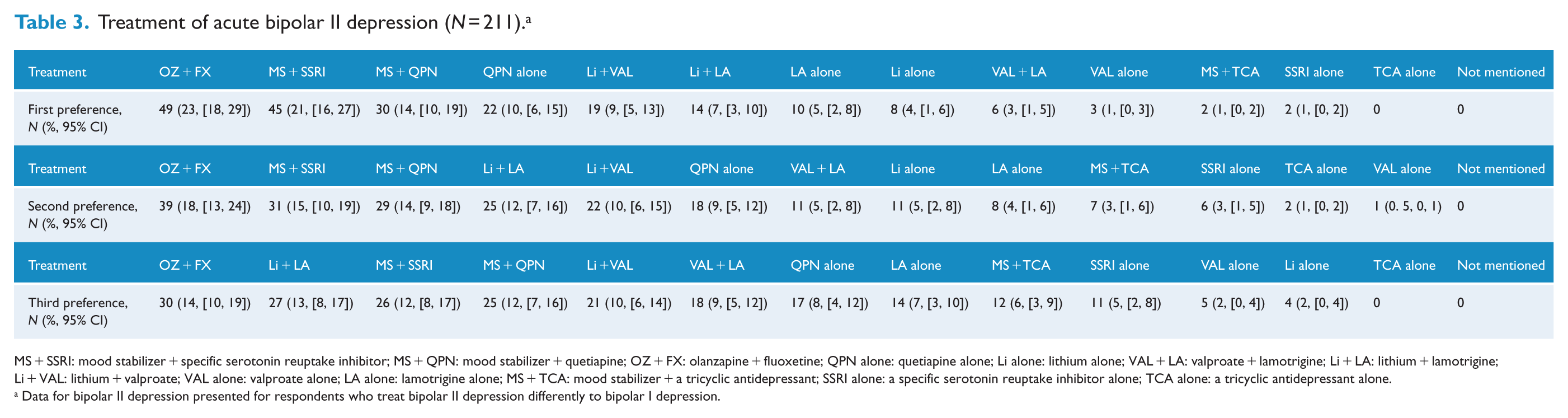
MS + SSRI: mood stabilizer + specific serotonin reuptake inhibitor; MS + QPN: mood stabilizer + quetiapine; OZ + FX: olanzapine + fluoxetine; QPN alone: quetiapine alone; Li alone: lithium alone; VAL + LA: valproate + lamotrigine; Li + LA: lithium + lamotrigine; Li + VAL: lithium + valproate; VAL alone: valproate alone; LA alone: lamotrigine alone; MS + TCA: mood stabilizer + a tricyclic antidepressant; SSRI alone: a specific serotonin reuptake inhibitor alone; TCA alone: a tricyclic antidepressant alone.
Data for bipolar II depression presented for respondents who treat bipolar II depression differently to bipolar I depression.
Use of antidepressants in bipolar disorder
One section of the questionnaire elicited responses concerning the use of antidepressants in bipolar depression. This section first elicited whether antidepressants are used at all. A majority of respondents used antidepressants to treat bipolar depression, type I (95%) and type II (93%). Most preferred SSRIs (88%) over other antidepressants to treat bipolar depression, both type I and type II. They preferred to use antidepressants ‘under the cover’ of MSs to treat bipolar depression, type I (93%) and type II (91%). None believed that antidepressants were ineffective in treating bipolar depression, although 66% of those using antidepressants to treat bipolar I depression and 54% of those using them to treat bipolar II depression opined that they have lesser efficacy than in major depressive disorder.
ECT
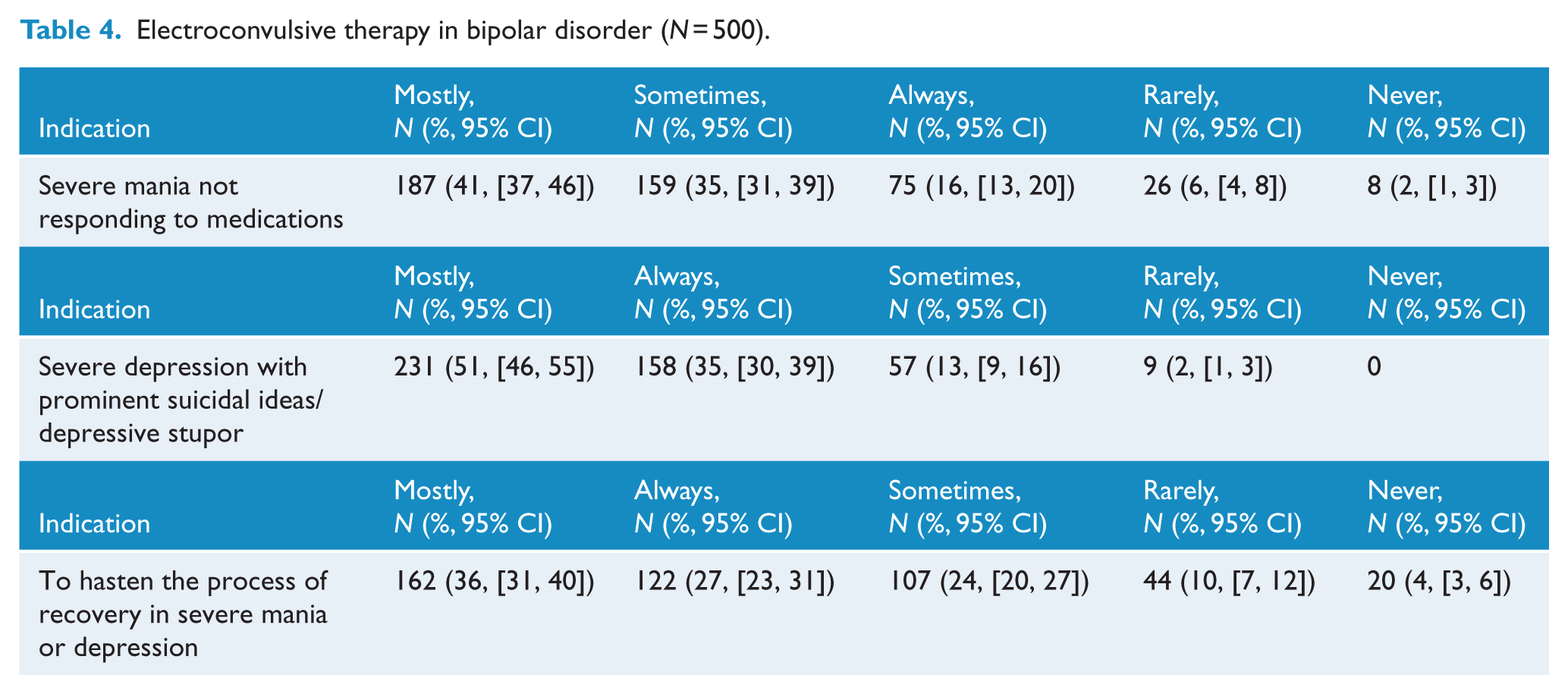
Assessing the use of ECT with the question ‘how often do you use ECT in bipolar disorder?’, 9% answered ‘never’, 22% ‘rarely’, 56% ‘sometimes’, 13% ‘mostly’ and 0% ‘always’. The pattern of ECT preference for three major indications is shown in Table 4. It is evident psychiatrists mostly or always use ECT for severe mania that has not responded to medications (57%), for severe depression with suicidal ideas/stupor (86%) and to hasten the process of recovery in both mania and depression (63%).
Electroconvulsive therapy in bipolar disorder (N = 500).
Maintenance treatment
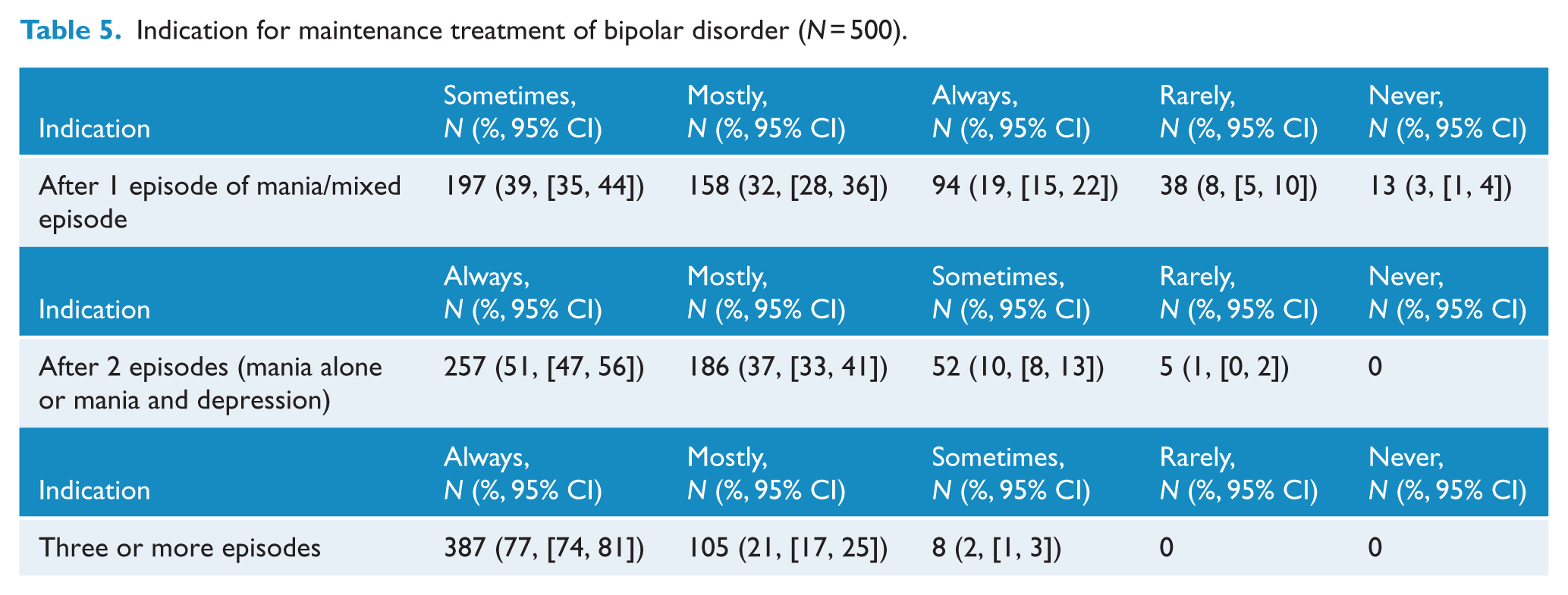
Following the first episode of bipolar disorder, 51% of participants prescribe maintenance treatment ‘mostly’ or ‘always’ (Table 5). With subsequent episodes, the tendency to prescribe for maintenance increases. To a question ‘how long do you recommend maintenance treatment?’, 29% recommended for ⩽2 years, 43% for 5 years, 20% for >5 years (but not lifelong) and only 8% advocated lifelong treatment. Participants felt that only 2% of their patients adhered to prophylactic medication(s) for at least 75% of the time prescribed. Lithium alone, valproate alone, and a combination of an MS and an atypical antipsychotic were the preferred maintenance treatment options (Table 6).
Indication for maintenance treatment of bipolar disorder (N = 500).
Preferences for maintenance treatment of bipolar disorder (N = 500).
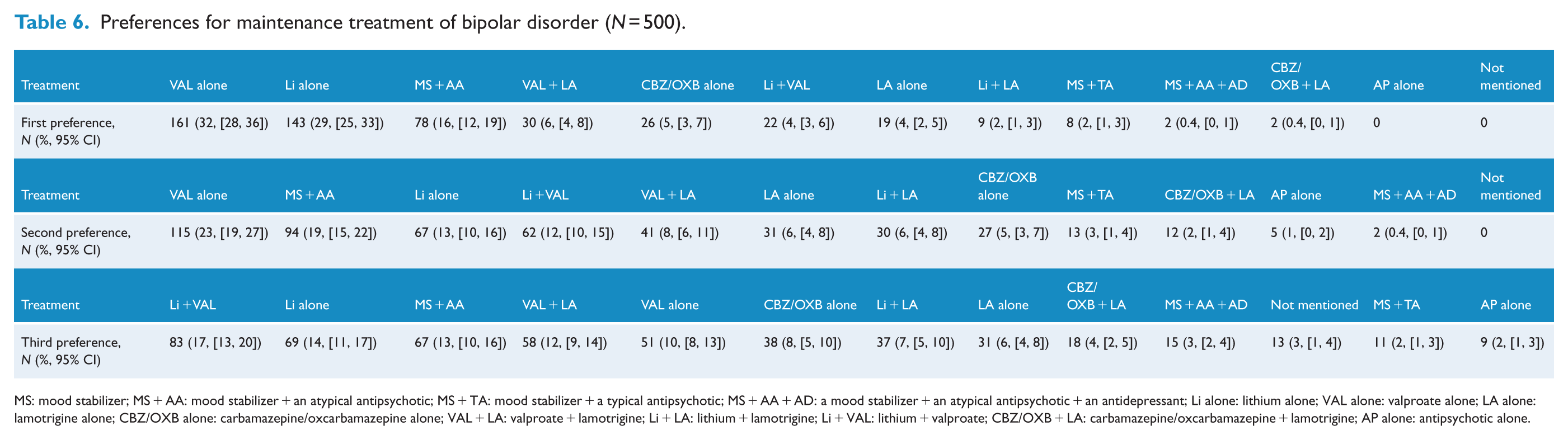
MS: mood stabilizer; MS + AA: mood stabilizer + an atypical antipsychotic; MS + TA: mood stabilizer + a typical antipsychotic; MS + AA + AD: a mood stabilizer + an atypical antipsychotic + an antidepressant; Li alone: lithium alone; VAL alone: valproate alone; LA alone: lamotrigine alone; CBZ/OXB alone: carbamazepine/oxcarbamazepine alone; VAL + LA: valproate + lamotrigine; Li + LA: lithium + lamotrigine; Li + VAL: lithium + valproate; CBZ/OXB + LA: carbamazepine/oxcarbamazepine + lamotrigine; AP alone: antipsychotic alone.
Rapid cycling
For rapid cycling bipolar disorder, valproate alone, a combination of MS and an atypical antipsychotic, and lithium + valproate were the preferred options (Table 6).
Modalities of decision-making
A majority of the participants (85%) acknowledged referring to treatment guidelines routinely (American Psychiatric Association [APA] guidelines, 75%; Indian Psychiatry Society [IPS] guidelines, 70%; British Association for psychopharmacology [BAP], 35%; Canadian Network for Mood and Anxiety Treatments [CANMAT], 22%; World Federation of Society for Biological Psychiatry [WFSBP], 18%; and National Institute for Health and Clinical Excellence [NICE], 4%), but to a question ‘which of the following convinces you of your choice of treatment?’, the responses were as follows: international guidelines (46%), personal experience (25%), Indian Psychiatric Society guidelines (13%), text books (13%), industry educational material (2%), and information from conferences and congresses (1%).
Discussion
The main findings of this survey of prescribing practices of Indian psychiatrists for the treatment of bipolar disorder are as follows:
A combination of an MS and an atypical antipsychotic is the preferred treatment option for acute mania.
To treat acute bipolar I depression, a combination of an MS and an SSRI is the preferred option, followed by MS + quetiapine and OFC. The preferences are similar for bipolar II depression.
Antidepressants, in particular the SSRIs, are widely used in the treatment of bipolar depression and often co-administered with MSs.
It appears that ECT is used more often in practice than recommended by guidelines.
Approximately, 50% of psychiatrists prescribe maintenance treatment after the first bipolar episode; lifelong maintenance treatment is rare.
The majority of psychiatrists make use of guidelines, but personal experience and other resources also influence their choice of treatment.
Acute mania
It is evident from our findings that prescription preferences for acute mania are not entirely in accordance with clinical guidelines (APA, 2002; Goodwin et al., 2016; Grunze et al.,2009, 2010, 2013; Licht et al., 2003; Malhi et al., 2015a; NICE, 2014; Shah et al., 2017; Yatham et al., 2018). Monotherapy with MSs (lithium and valproate) and atypical antipsychotics are the typical first-line strategies recommended for acute mania, but in clinical practice, most Indian psychiatrists tend to use a combination of an MS and an antipsychotic, prescribing predominantly an atypical antipsychotic to hasten the process of recovery (Ogawa et al., 2014). Although most guidelines recommend monotherapy with an MS or an atypical antipsychotic as first-line treatment for acute mania (APA, 2002; Goodwin et al., 2016; Grunze et al., 2009; NICE, 2014), the CANMAT/ISBD guidelines (Yatham et al., 2018), the Royal Australian and New Zealand College of Psychiatrists (RANZCP) clinical practice guidelines for mood disorders (Malhi et al., 2015a) and the clinical practice guidelines of the Indian Psychiatric Society (IPS) (Shah et al., 2017) recommend combination treatment as a possible first line option. The latest CANMAT/ISBD guidelines note that a combination therapy with the atypical antipsychotics (quetiapine, aripiprazole, risperidone or asenapine) and lithium/valproate may have greater efficacy than monotherapy with lithium, or valproate alone, especially in severe episodes; about 20% more patients may respond to combination therapy than monotherapies, but with a greater risk for adverse effects (Yatham et al., 2018). Treatment with olanzapine is downgraded to a second-line treatment option, both as a monotherapy and as a combination treatment with lithium/valproate by the CANMAT/ISBD guidelines because of safety and tolerability issues, whereas other guidelines recommend treatment with olanzapine as one of the first-line options.
The management of acute mania in clinical practice is directed at rapid resolution of symptoms because of hyperarousal and attendant irritability, aggression, impulsivity, agitation and psychosis. Amelioration of these symptoms is best achieved by a combination of an MS and an antipsychotic. A recent meta-analysis of 19 randomized controlled studies comparing a combination (or augmentation) of an MS and an antipsychotic versus an MS alone or an antipsychotic alone demonstrated that the combination was more efficacious than either of them alone, but caused greater side-effects, especially somnolence and lesser tolerability (Ogawa et al., 2014). While the CANMAT/ISBD (Yatham et al., 2018), the IPS (Shah et al., 2017) and the RANZCP (Malhi et al., 2015a) guidelines consider adjunctive/combination therapy of atypical antipsychotics with lithium or valproate as one of the first-line therapies in addition to monotherapy, the WFSBP guidelines strongly encourage monotherapy before switching to combinations to minimize side-effects and medical risks (Grunze et al., 2009).
It must be emphasized that, in studies examining the efficacy of a combination of an MS plus an antipsychotic versus an MS alone, only the patients who experience insufficient response to monotherapy with an MS were included. There is no robust evidence to show that a combination treatment from the beginning (a de novo combination) is better than monotherapy. Irrespective of the guidelines’ recommendations and evidence base, in clinical practice, combination treatments are preferred over monotherapy shown also by our findings (Ghaemi et al., 2006). In view of the fact that only a minority of the naturalistic patients are eligible for controlled trials (Licht et al., 1997), there is an understandable gap between the evidence and practice. The IPS guidelines also acknowledge routine use of typical antipsychotics like haloperidol, chlorpromazine and trifluoperazine in the treatment of acute mania, which again is reflected in our finding that they are often used in combination with an MS (Shah et al., 2017).
Acute depression
Quetiapine, OFC and lurasidone are approved by the Food and Drug Administration (FDA) for the treatment of acute bipolar depression. Guidelines uniformly recommend quetiapine and lithium (APA, 2002; Goodwin et al., 2016; Grunze et al., 2009, 2010, 2013; Licht et al., 2003; Malhi et al., 2015a; NICE, 2014; Shah et al., 2017; Yatham et al., 2018) as one of the first-line options. A few guidelines recommend lamotrigine (Goodwin et al., 2016; Malhi et al., 2015a; Shah et al., 2017; Yatham et al., 2018) as a first-line therapy while others do not (Grunze et al., 2010; NICE, 2014). The latest revisions of certain guidelines also include lurasidone as a first-line option (Goodwin et al., 2016; Malhi et al., 2015a; Yatham et al., 2018). Although quetiapine and OFC were a popular option in our survey, the combination of an SSRI with an MS was the most preferred, particularly in bipolar I depression (Table 2). In fact, the majority of respondents admitted to widespread use of SSRIs, mostly under the cover of MSs. The widespread use of antidepressants in treating bipolar depression is not in tune with the general recommendations of most guidelines, and, while a few guidelines support the use of antidepressants under the cover of MSs, this is not usually a first-line treatment option (Goodwin et al., 2016; Malhi et al., 2015a; Yatham et al., 2018). Some pivotal studies on acute bipolar depression strongly discourage the use of antidepressants in bipolar depression (McElroy et al., 2010; Sachs et al., 2007). Experts have cautioned clinicians about the potential disruptive effects of antidepressants on the course of bipolar disorder (Ghaemi, 2012; Malhi, 2012; Malhi et al., 2015b). One older meta-analysis supported the use of antidepressants (Gijsman et al., 2004), whereas recent meta-analyses do not report beneficial effects of antidepressants (McGirr et al., 2016; Sidor and MacQueen, 2011). Irrespective of the findings of these studies, our survey reveals that most psychiatrists believe that antidepressants are effective in bipolar disorder and therefore they are widely used in clinical practice. The ISBD task force on the use of antidepressants in bipolar disorder points out the incongruence between widespread use of antidepressants and the weak evidence base supporting efficacy and safety, but also recognizes that some patients may actually benefit from the use of antidepressants (Pacchiarotti et al., 2013). This underscores the need for well-designed studies with a translational approach designed to examine the efficacy of antidepressants in the acute and maintenance treatment of bipolar depression.
The OFC combination was widely preferred in treating both bipolar I and II disorders (Tables 2 and 3), but some recent guidelines do not recommend it as one of the first-line treatment options because of safety and tolerability concerns (Malhi et al., 2015a; Yatham et al., 2018) and a lack of evidence for any prophylactic properties (Yatham et al., 2018). However, the IPS guidelines consider the OFC combination as one of the first-line treatment options (Shah et al., 2017).
ECT
Generally, it appears that ECT is used more often than recommended by guidelines (Table 4). Some guidelines recommend the use of ECT in severe/resistant mania, severe depression with psychosis/stupor/high suicide risk and in severe mania or depression during pregnancy as one of the first-line options (Goodwin et al., 2016; Shah et al., 2017), but the CANMAT/ISBD (Yatham et al., 2018) and the RANZCP (Malhi et al., 2015a) guidelines recommend that ECT be considered as a second-line option. The IPS guidelines provide a few additional indications such as the need for rapid control of symptoms, severe agitation or violence and refusal to eat that puts the life of the patient at risk (Shah et al., 2017). Our findings are in accordance with the observation made in a narrative review that ECT is used frequently in India to treat both manic and depressive phases of bipolar disorder (Thirthalli et al., 2012). An interesting observation is that many practitioners use ECT to hasten the process of recovery (63%), although this is not an indication usually recommended by guidelines. It is possible that local practice situations such as limited infrastructure (e.g. fewer beds), fewer mental health professionals and the cost of prolonged hospitalization, coupled with an expectation of a quick recovery from families, persuade psychiatrists to employ ECT earlier in the course of illness to curtail episode duration. ECT is effective in severe and treatment-resistant depression and mania and has the potential to induce quick recovery and shorten the duration of mood episodes (Versiani et al., 2011).
Maintenance treatment
Not many psychiatrists prefer maintenance treatment following the first episode of mania, and only about a half of them prefer to use it after two episodes (Table 5). In essence, maintenance treatment is not routinely preferred by psychiatrists in India. Moreover, most did not prefer lifelong treatment. Our findings are in sharp contrast to a survey of French psychiatrists in which most (60%) offered long-term treatment from the first episode (Samalin et al., 2011). While most guidelines recommend early initiation of maintenance/prophylactic treatment, they fail to provide clear recommendations. Some guidelines (APA, 2002; Goodwin et al., 2016; Yatham et al., 2018) recommend lifelong prophylaxis after the first manic episode, whereas the NICE guidelines (NICE, 2014) do not specify when long-term treatment becomes necessary. Other guidelines recommend prophylaxis after the first episode if it is severe, or if it is associated with a family history (Malhi et al., 2009; Nolen et al., 2008). Danish guidelines recommend prophylaxis after two bipolar episodes within a span of 5 years (Licht et al., 2003). The RANZCP guidelines recommend prophylaxis after considering several factors (severity of episodes; relapse/recurrences/number of lifetime episodes; predictability of episodes; presence of subsyndromal symptoms; efficacy, side-effects and tolerability of treatment; and functioning and quality of life while on medications) and suggest reassessment every 12 months for continued prophylaxis (Malhi et al., 2015a).
What is consistent among guidelines is that the maintenance/prophylactic treatment is lifelong and not for an arbitrary duration. However, most Indian psychiatrists do not prefer lifelong maintenance treatment, and this is understandable considering the complexities involved; for example, low acceptance, poor adherence, tolerability issues, long-term side effects, negative attitudes toward medicines and the varying course of illness. Participants estimated that only 2% of their patients adhered to prophylactic medication(s) for at least 75% of the time prescribed. While we have not determined what participants considered to be reasons for poor adherence, we speculate that anticipation of poor adherence may itself contribute to less enthusiasm for prescribing lifelong maintenance treatment early in the course of illness.
Lithium or valproate monotherapy are the standard first-line monotherapies recommended by most guidelines. In this survey, most did not prefer atypical antipsychotic monotherapy despite accumulating evidence for their role in maintenance treatment and acceptance by guidelines (Goodwin et al., 2016; Grunze et al., 2013; Malhi et al., 2015a; NICE, 2014; Yatham et al., 2018). Although a combination of lithium and valproate is shown to be superior to valproate alone (Geddes et al., 2010), not many in this survey considered it a first preference. However, a combination of an MS and an atypical antipsychotic drug was preferred after valproate and lithium monotherapy (Table 6). It is possible that some psychiatrists prefer to continue the combination because it worked in the acute phase of the illness. The CANMAT/ISBD guidelines consider a combination of quetiapine and lithium or valproate as the best first-line adjunctive therapy (Yatham et al., 2018). Olanzapine is almost as effective as quetiapine, but is recommended as one of the several second-line maintenance treatments because of safety and tolerability issues (Yatham et al., 2018). A recent review suggests that a combination of an MS and an antipsychotic may be more effective than monotherapies in the long-term management of bipolar disorder (Buoli et al., 2014). One interesting observation is the limited preference for lamotrigine (Table 6) despite its purported efficacy in preventing depressive relapses (Goodwin et al., 2004) and its recommendation by many guidelines (APA Guidelines Watch; Goodwin et al., 2016; Grunze et al., 2013; Malhi et al., 2015a; Yatham et al., 2018).
Rapid cycling
As there is no evidence of superiority of any MS or atypical antipsychotic in the treatment of rapid cycling, a combination of MSs such as lithium or valproate, or a combination of an MS and an atypical antipsychotic such as quetiapine and olanzapine is recommended by some guidelines (APA, 2002; Goodwin et al., 2016; Shah et al., 2017; Yatham et al., 2005, 2018). The treatment of rapid cycling bipolar disorder is a challenge and there are not many controlled studies to guide therapeutic choice. Lithium and valproate are not as effective in rapid cycling as in non-rapid cycling bipolar disorder (Tondo et al., 2003), but are still considered first line options in some guidelines (Malhi et al., 2015a; Shah et al., 2017), although evidence supporting superiority of combination therapy is limited (Malhi et al., 2015a). The NICE guidelines note that rapid cycling bipolar disorder should be treated along the same lines as non-rapid cycling bipolar disorder since there is no definite evidence that treatment for rapid cycling and non-rapid cycling differ substantially (NICE, 2014).
Lamotrigine’s role in rapid cycling bipolar disorder, particularly in bipolar II disorder, is documented (Calabrese et al., 2000) and acknowledged by some guidelines (APA, 2002; Shah et al., 2017; Yatham et al., 2005), but in our survey, very few preferred lamotrigine for rapid cycling. The recent CANMAT/ISBD guidelines note that lamotrigine did not separate from placebo in the maintenance treatment of rapid cycling bipolar I disorder (Yatham et al., 2018). In our survey, most psychiatrists preferred either valproate or a combination treatment (Table 7), but curiously, lithium monotherapy was not preferred despite the evidence that it may not be inferior to valproate (Calabrese et al., 2005) and that a combination of lithium and valproate has no advantage over lithium alone (Geddes et al., 2010; Kemp et al., 2009). Preference for a combination of an MS and an atypical antipsychotic is supported by the evidence that the addition of risperidone to an MS may significantly reduce relapse rates (Macfadden et al., 2009).
Treatment preferences for rapid cycling bipolar disorder (N = 500).
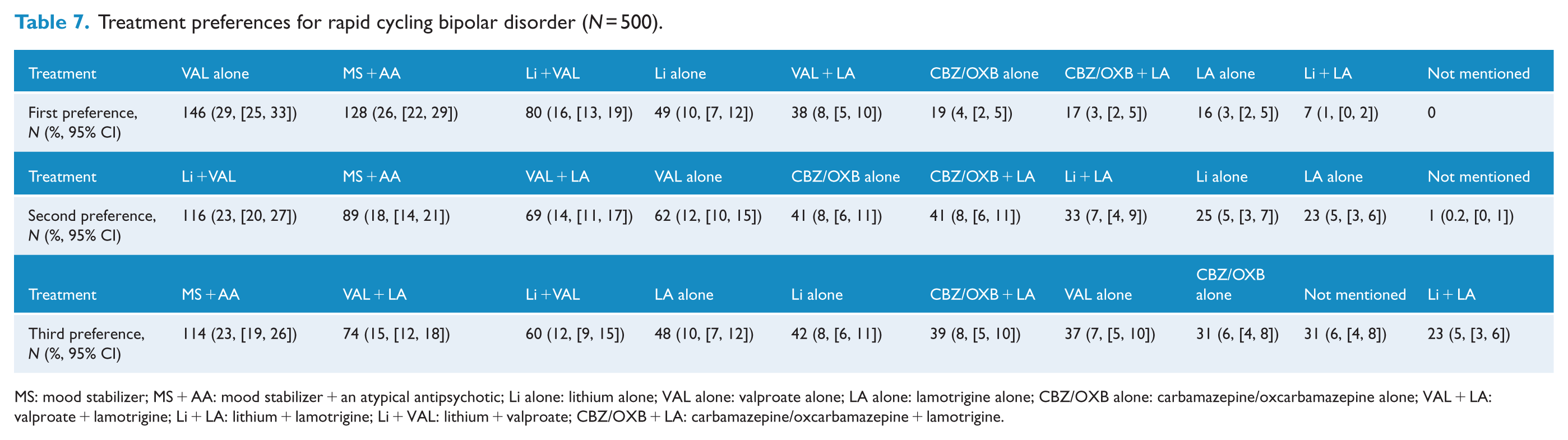
MS: mood stabilizer; MS + AA: mood stabilizer + an atypical antipsychotic; Li alone: lithium alone; VAL alone: valproate alone; LA alone: lamotrigine alone; CBZ/OXB alone: carbamazepine/oxcarbamazepine alone; VAL + LA: valproate + lamotrigine; Li + LA: lithium + lamotrigine; Li + VAL: lithium + valproate; CBZ/OXB + LA: carbamazepine/oxcarbamazepine + lamotrigine.
Decision-making
Results of our study show that most Indian psychiatrists refer to guidelines although personal experience and other sources also contribute significantly to their decision-making. These findings are reassuring and are in sharp contrast to the findings of a French survey of psychiatrists; which found that treatment guidelines were not widely implemented (12%) and that personal experience (41%) was the main factor contributing to decision-making (Samalin et al., 2011). A North American study also found that only 8% refer to guidelines while making treatment decisions and that they rely more on published clinical studies (43%) and information gleaned from relevant congresses and conferences (33%) (Perlis, 2007). It is interesting to know that for clinical decision-making, Indian psychiatrists seem to rely more on international guidelines (46%) and personal experience (25%) and less on the IPS guidelines (13%). This is possibly because the IPS guidelines are not updated regularly.
Implications
Although practitioners seem to broadly adhere to recommendations in clinical practice guidelines, there is an obvious gap between the research evidence and practice. This is despite the fact that the majority of practitioners report that they refer to guidelines. While this may lead to an obvious conclusion that more effort should be made to ensure adherence to guidelines, it also points to the fact that perhaps the recommendations in guidelines do not cater to the needs of the practitioners and that, in the real world, patients differ from the samples in clinical trials, the usual source for evidence that informs guidelines (Perugi and Fornaro, 2011). In other words, the survey points to the need to examine clinical questions in pragmatic clinical trials for greater generalisability.
The survey also raises pertinent clinical queries that need to be addressed with some urgency. Antidepressants are widely used to treat bipolar depression because they are perceived as effective (Gijsman et al., 2004; Pacchiarotti et al., 2013), but their efficacy and safety remain controversial (McGirr et al., 2016; Malhi et al., 2015b; Sidor and MacQueen, 2011). The role of antidepressants in the acute and maintenance treatment of bipolar depression clearly needs to be studied systematically.
ECT is often used to hasten the process of recovery and may potentially shorten the duration of acute severe mood episodes (Versiani et al., 2011); however, the efficacy of ECT in severe episodes of mania and depression needs to be established in comparison with other standard treatment options. In view of the highly recurrent and disabling nature of this illness and the high risk of suicide, there is an urgent need to further study the reasons for reluctance to prescribe long-term maintenance treatment, especially when it is increasingly being advocated as the norm in the treatment of bipolar disorder (Malhi et al., 2012) and not providing maintenance/prophylactic treatment could have grave implications.
Limitations
Findings of this study need to be considered in the context of certain limitations. The study surveyed the prescribing practices of Indian psychiatrists in the treatment of bipolar disorder by administering a questionnaire that elicited their preferences. The responses to queries in the survey are indirect measures that allow us to examine the actual practices; however, they are susceptible to self-report and social-desirability biases. Furthermore, the study did not examine prescription preferences in bipolar disorder comorbid with other disorders such as alcohol/substance dependence and anxiety disorders. Similarly, we did not explore prescribing preferences for relapses/recurrences of mood episodes in those who are already on maintenance treatment. Atypical antipsychotics are increasingly used to treat bipolar disorder, but we did not elicit preferences for individual drugs. Finally, this is a cross-sectional study, and therefore, temporal changes in views and practice cannot be considered.
Conclusion
Overall, Indian psychiatrists seem to broadly follow the recommendations of international and national guidelines. However, there are notable departures. Acute mania is managed mostly by a combination of an MS and an atypical antipsychotic and not by monotherapies. Although FDA-approved medications such as quetiapine and OFC are used for the treatment of bipolar depression, antidepressants co-administered with MSs are the preferred option. ECT is used commonly in the treatment of severe bipolar disorder and to hasten the process of recovery. What is most striking in this survey is that most psychiatrists did not adhere to the guidelines with respect to maintenance/prophylactic treatment of bipolar disorder and prescribed maintenance treatment only for a limited period of time.
Footnotes
Acknowledgements
The authors thank Professor Jagadisha Thirthalli, Department of Psychiatry, National Institute of Mental Health and Neurosciences (NIMHANS), Bangalore, for his suggestions during the course of development of the questionnaire used in this survey and for his comments on the earlier version of the manuscript. Participants in the study were not paid any fee.
Declaration of Conflicting Interests
Dr Y.C.J.R., Dr V.J., Dr R.N., Dr M.S.R. and Dr N.S. are members of Society for Bipolar Disorders, India (SBDI). Dr S.G. and Dr S.K. are full-time employees of GlaxoSmithKline.
Funding
The study was funded by GSK. All the authors including GSK employees conceptualized and drafted the study protocol. GSK funded the Ipsos Healthcare (Mumbai), an international Clinical Research Organization (CRO) which executed the study. GSK reviewed only fully anonymized completed data collection forms. GSK had no access to any personally identifiable participant information. All the authors had an access to raw data, and data analysis was performed as per the study protocol.