
Abstract
The purpose of the present paper was to compare currently available diagnostic guidelines for juvenile bipolar disorder with respect to utility in research and clinical practice. A systematic search of psychiatric, medical and psychological databases was conducted using the terms ‘juvenile bipolar disorder’, ‘paediatric bipolar disorder’ and ‘guidelines’. Three main sets of guidelines issued by the National Institute of Health and Clinical Excellence (UK), The National Institute of Mental Health (USA) and Child Psychiatric Workshop (USA) were found. There were key differences in the recommendations made by each regarding the diagnosis and symptomatic presentation of juvenile bipolar disorder. Although the diagnosis of juvenile bipolar disorder is gaining increased recognition, its definition remains controversial. It is recommended that clinicians and researchers need to develop diagnostic guidelines that have clinical salience and can be used for future research by incorporating key features of those that are currently available.
Juvenile bipolar disorder (JBD) is the term most commonly used when children and adolescents aged 6–18 years meet criteria for the diagnosis of bipolar disorder (BD). Alternative terms that are used in practice to describe JBD include paediatric BD, childhood-onset BD, early onset BD and prepubertal BD. These differing terminologies both reflect and contribute to a lack of consensus as regards the diagnosis of BD in this age group. The diagnostic threshold of JBD is a matter of considerable debate among psychiatrists, paediatricians and other mental health professionals, added to which BD is difficult to diagnose in children and adolescents owing to developmental factors that impact upon symptom presentation.
Adults with BD commonly report that their symptoms commenced before the age of 16 years [1, 2]. However, there is typically a delay of 11–19 years before a definitive diagnosis of BD is conferred [3–5]. Akin to this, there is a significant delay between the onset of symptoms and subsequent accurate diagnosis of JBD. Robust diagnosis permitting effective implementation is desirable at any stage of the illness, and across all bipolar age groups, but is perhaps most critical in younger individuals [6].
Interestingly, the diagnosis of JBD is on the increase, possibly due to growing awareness of younger patients presenting with dysphoric mania, and the identification of shorter episodes of mania/hypomania, mixed episodes and rapid cycling [7]. Clinically, an important question is whether the patterns of illness encountered in JBD evolve into the classic adult form, characterized by a biphasic pattern of depression and mania, or whether atypical presentations are a more likely outcome.
Some authorities recommend that the diagnosis of JBD should be limited to children aged ≥6 years [8, 9] and yet the Great Smoky Mountain study that examined a sample of 9-, 11- and 13-year-olds found no cases of mania, and only rare occurrences of hypomania (0.07%) [9]. It is only in older adolescents that the prevalence of BD approaches that found in adults, with one community survey reporting 1% of older adolescents satisfying criteria for JBD and a further 3–4% having subthreshold disorder [10].
The diagnosis of JBD is also considered to be controversial because of similarities in presentation to attention-deficit–hyperactivity disorder (ADHD), oppositional defiant disorder (ODD), conduct disorder (CD), substance misuse disorders and anxiety disorders. The diagnosis of JBD is further complicated by considerable comorbidity that is prevalent in all of the aforementioned diagnoses [11].
Diagnostic guidelines
Recently, guidelines to assist the diagnosis of JBD have been issued in the USA and UK. However, there is significant disparity between them, suggesting that the underlying mechanisms mediating bipolar are perhaps apportioned different emphasis in the two countries. In practice, it is vital that professionals working with children and adolescents are familiar with the current debate and the contentious viewpoints and approaches surrounding the diagnosis of JBD. Hence, in this review, three different sets of diagnostic guidelines, two from the USA (from the National Institute of Mental Health and the Child Psychiatric Workshop) [8, 9, 12] and one from the UK (from the National Centre for Health and Clinical Excellence) [13] are succinctly summarized and compared.
The American Psychiatric Association, the Royal Australian and New Zealand Clinical Practice Guidelines Team for Bipolar Disorder and, more recently, the Canadian Network for Mood and Anxiety Treatments (CANMAT) have each highlighted some of the difficulties with the diagnosis of JBD, including the problem of high comorbidity [14–16]. However, the focus of the latter guidelines is treatment within adult populations, and therefore these are not considered in this discussion.
Methods
We conducted a systematic search of several databases including PyschLit, MEDLINE and PubMed and also the Google Internet Search Engine on 29 November 2006 and 19 December 2006 using the terms ‘juvenile bipolar disorder’, ‘paediatric bipolar disorder’ and ‘guidelines’ to gather the necessary literature in addition to drawing upon data known to each of the authors. We identified six guidelines in total, three that focused on diagnosis [11–13], and three that were excluded from this review because they centered solely on treatment [14–16].
Results
National Institute of Mental Health Guidelines
The National Institute of Mental Health (NIMH) guidelines explicitly state that mania during childhood and adolescence more commonly presents with irritability, alongside destructive outbursts [12]. The guidelines focus on behaviours that may reflect mood symptoms, and suggest that symptoms of other disorders frequently characterize the initial presentation of JBD. It is suggested that physical complaints, school difficulties, running away from home, excessive complaining and crying, interpersonal sensitivity and poor socializing may all be indicative of JBD.
The NIMH guidelines highlight that, in contrast to the presentation of mania in adult BD, juvenile mania typically assumes a rapid cycling or chronic pattern, and is highly comorbid with other conditions such as ADHD and CD [12]. Onset in late adolescence, however, is more likely to pursue an adult pattern of BD with discrete phases of depression and mania/hypomania.
The NIMH subsequently amended the guidelines and their recommendations following a round table meeting of experts [17]. The participants agreed that while DSM-IV-TR [18] criteria may apply to some prepubertal children, there is a group who clearly do not meet these criteria and are placed in the category of BD not otherwise specified (BD-NOS). The most frequent presentation of BD in children and adolescents was described as long episodes of mood instability with rapid cycling and mixed mood states [17].
However, under the amended NIMH guidelines [17], BD-NOS becomes a catch-all category for patients under 18 years of age who do not meet the adult duration criteria for BD. Thus the round table recommendations suggest that BD-NOS be viewed as a working diagnosis with well-described comorbidities and symptoms. Furthermore, they proposed the addition of the Child Behavior Check List–Parent Report (CBCL-PR) [19], in order to provide an evaluation of the dimensions of common and overlapping symptoms in diagnostically problematic children and adolescents (Table 1). Better mapping of comorbid disorders was advised so as to track the course of bipolar I disorder (BDI) and bipolar II disorder (BDII) as compared to BD-NOS, and to ultimately evaluate outcome. This is important because many cases of BD-NOS eventually convert to BDI or BDII, suggesting that in some cases this may be a prodromal phase that serves as precursor to the illness. The NIMH round table discussions also advocated the use of additional assessments in the case of children under 6 years of age, so as to confirm a diagnosis of BDI or BDII [12]. In this age group ‘mood lability’ was thought to be of uncertain significance and so the Washington University (St Louis), Kiddie Schedule for Affective Disorders and Schizophrenia (WASH-U-KSADS), [20] was recommended as principal tool for diagnosis.
Assessment tools recommended for use by NICE guidelines [13]
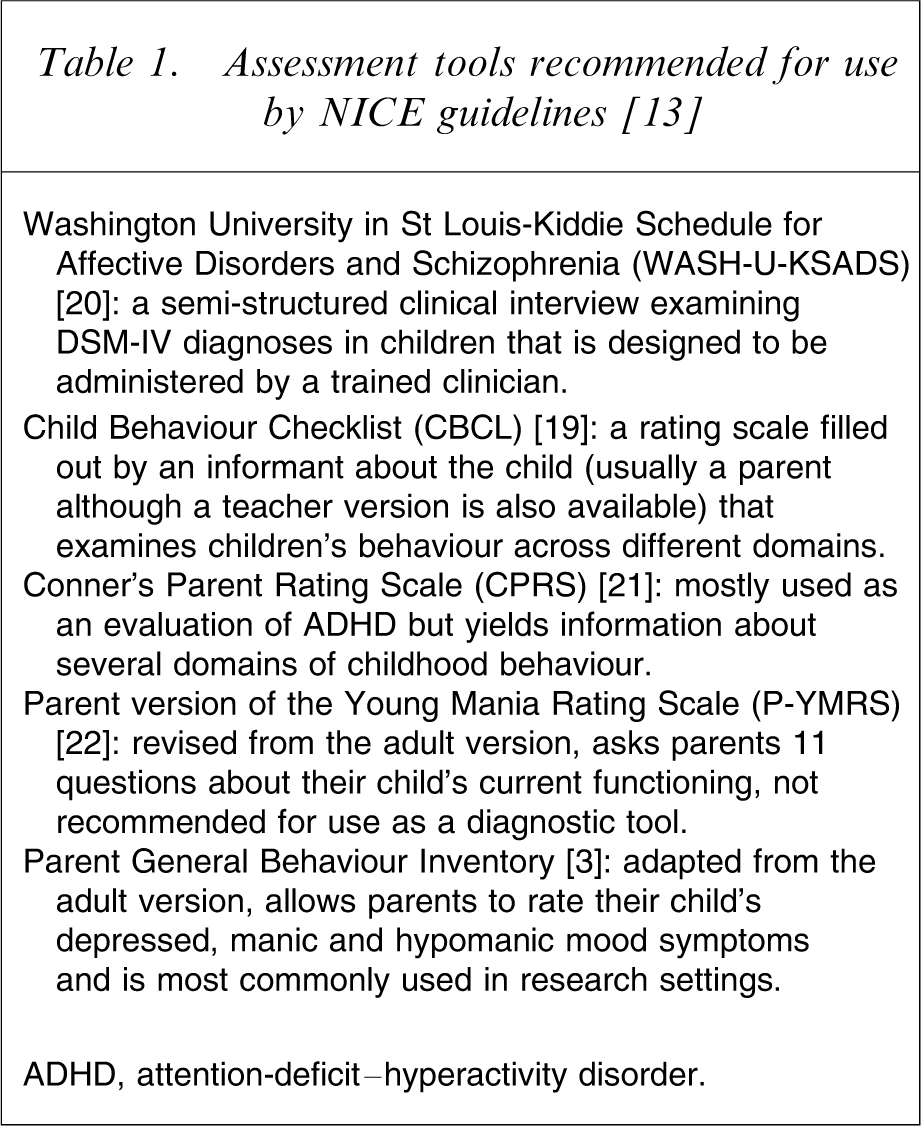
ADHD, attention-deficit–hyperactivity disorder.
Child Psychiatric Workshop
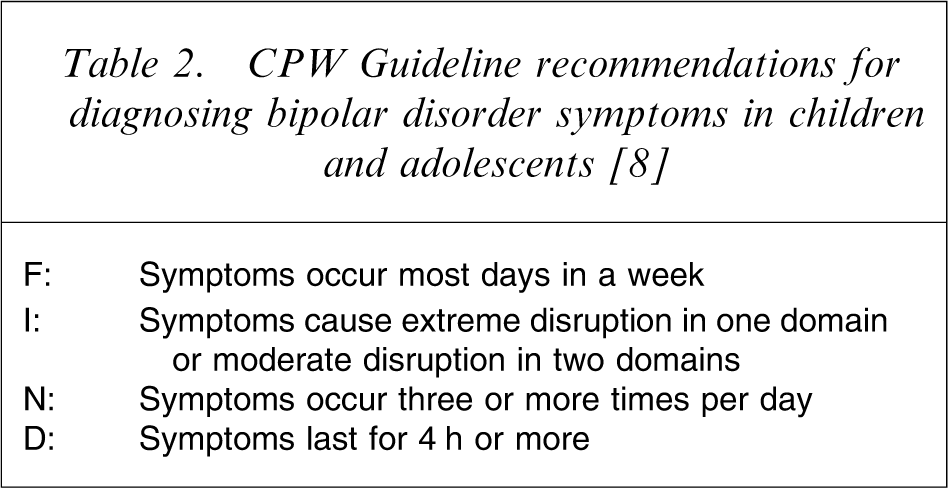
More recent guidelines for JBD have been issued by the Child Psychiatric Workshop (CPW), in response to the needs of clinicians [9]. The workshop acknowledged the limitations of DSM-IV-TR [18] criteria for children and adolescents and reiterated that many children with JBD have daily mood swings over periods of days, weeks or months. As a result of this variable and rapidly changing clinical picture, BD-NOS is the largest subgroup within JBD because it accommodates all the children who fail to meet duration criteria for DSM-IV-TR BDI or BDII. In keeping with NIMH recommendations, the CPW guidelines recognize BDII as a valid diagnosis in children, but in order to determine the presence or absence of mania the CPW guidelines recommend using a frequency, intensity, number, duration (FIND) strategy, noting several characteristics of symptoms that commonly reflect bipolarity in this age group (Table 2). Although not validated, this strategy offers a framework for considering whether symptoms are within normal parameters.
CPW Guideline recommendations for diagnosing bipolar disorder symptoms in children and adolescents [8]
As regards irritability, the CPW guidelines acknowledge that it is ubiquitous in childhood psychopathology and agree that episodic manifestations of this symptom may be indicative of future development of BD [8]. The guidelines also expand on the assessment of manic symptoms in children, giving examples of how grandiosity, racing thoughts, and decreased need for sleep may be appropriately assessed.
As regards the accuracy of assessment of JBD symptoms, these guidelines make several recommendations, namely that the assessment should include the child, at least one parent, and input from school staff [8]. Furthermore, they advocate that information about mood, sleep and energy levels is collected for 2 weeks prior to the first assessment and that information providing a timeline of mood disturbance along with medical history, psychosocial history and the child's current level of functioning be collated [8].
National Institute of Health and Clinical Excellence Guidelines
In 2006 the National Institute of Health and Clinical Excellence (NICE) in the UK issued guidelines for the diagnosis and treatment of BD [13]. These guidelines, while acknowledging the limitations of the adult criteria when applied to children and adolescents, suggested that the diagnosis could be made in this population. The NICE guidelines (2006) recommend that in order to diagnose BD in children or adolescents mania should be present and that euphoria should be present most days, for most of the time over a 7 day period [13]. These guidelines also advocated that irritability in this population should not be considered a core diagnostic criterion and that in the case of adolescents presenting with symptoms of BD, irritability may be helpful diagnostically, but only if it is episodic, severe and out of character for the adolescent and has a negative impact upon functioning.
Thus, the NICE guidelines permit a diagnosis of BDI in children where DSM-IV-TR criteria [18] are met, but a diagnosis of BPII in children and adolescents is not supported because it is argued that the diagnostic criteria are not sufficiently validated for routine use [13]. These guidelines also err on the side of caution in cases in which a child or adolescent with recurrent major depressive episodes has a family history of BD [18]. In these instances the NICE guidelines recommend that BDI is not diagnosed and that instead careful follow up is instituted.
With respect to differential diagnoses, the NICE guidelines suggest that clear mood episodes and cycling of mood with features of elation and grandiosity should be used to differentiate BD from ADHD, CD and schizophrenia [13]. Clinicians are also urged to consider broader issues such as child abuse, substance misuse, undiagnosed learning disabilities and organic causes as possible causes of unusual behaviour and symptoms.
Finally, the guidelines recommend that a diagnosis should be made only by a specialist clinician. The instruments suggested for use include a semi-structured diagnostic interview such as the WASH-U-KSADS [20] and parent report questionnaires such as the CBCL-PR [19] (Table 1). These instruments are used in combination with a Mental State Examination (MSE), medical evaluation, neuropsychological and neurological evaluation, and full clinical assessment of the child, as well as obtaining history from the parents/carers and teachers [13].
Discussion
The three guidelines that have clearly adopted differing approaches and place varying emphasis on specific symptoms, all support the diagnosis of JBD. Key differences between each set are presented in summary form in Table 3. The NIMH and CPW guidelines for instance emphasize irritability as a manic symptom in JBD [9, 12, 17], whereas the NICE guidelines do not [13]. With respect to age the guidelines differ such that diagnosis of BD in children under 6 years of age is not specifically addressed by the NICE guidelines that allow only BDI as a diagnosis in patients under 18 years of age [13]. The NIMH guidelines require additional assessments in children under 6 years in order to assign a diagnosis of BD, although BDI, BDII and BD-NOS are all permitted [12, 17]. This is in marked contrast to the CPW guidelines, which do not support any bipolar diagnosis in this age group [8].
Summary of differences across JBD guidelines
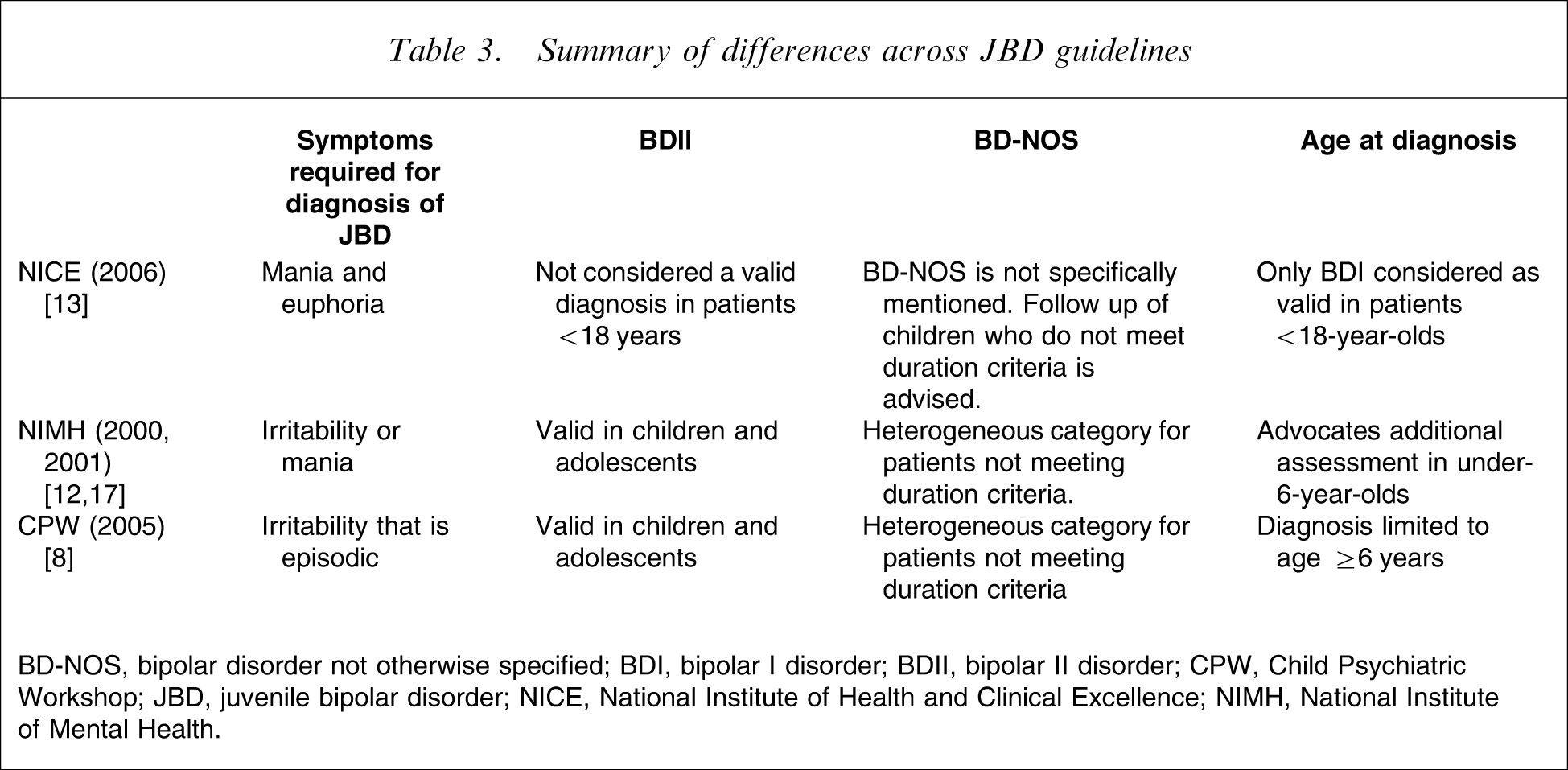
BD-NOS, bipolar disorder not otherwise specified; BDI, bipolar I disorder; BDII, bipolar II disorder; CPW, Child Psychiatric Workshop; JBD, juvenile bipolar disorder; NICE, National Institute of Health and Clinical Excellence; NIMH, National Institute of Mental Health.
Of note, in addition to the many discrepancies outlined here in the main diagnostic guidelines, cultural differences are also becoming increasingly apparent in the diagnosis of JBD. For example, JBD is more likely to be diagnosed in the US than in Holland [23] and children and adolescents with JBD in India have a better outcome, experience less comorbidity, have less substance misuse and are less likely to be rapid cycling as compared to their contemporaries with JBD in the USA [24–26].
In essence, the three sets of criteria described reflect a conservative, a liberal and a compromise viewpoint. However, in practice clinicians have many more considerations to contend with in diagnosing JBD. In addition to multiple sets of criteria, there are issues related to their own biases, level of training and experience, pressure from the patient's family and school, not to mention the significant psychosocial adversity that faces many of these children.
Age and mode of onset seems to be an important clue to diagnosis especially because it not yet clear whether BD is a developmental disorder [27]. Usually it has a discernible onset that coincides with a definite worsening of symptoms (and or development of new symptoms) and confers significant functional disability. The NICE guidelines seem to be the easiest to follow and if a child satisfies the necessary criteria, there is usually no hesitation in making a diagnosis of BD. Naturally, in practice chronicity, irritability, ultradian cycling and an absence of clearly defined episodes decrease diagnostic certainty. However, in a subset of children who manifest dysregulated affect in addition to disruptive behaviour, the CPW guidelines are potentially more useful in differentiating those with severe disruptive disorders from those who have putative JBD.
Whether JBD is episodic or chronic divides the opinions of researchers and clinicians and in practice partitioning of BD from an associated comorbidity is achieved by observing whether the comorbid symptoms persist during euthymia. However, in cases in which there is no clearly distinguishable period of euthymia this becomes problematic [28]. Recent research indicates that mania is characterized by euphoria and an expansive mood and that this differentiates it from all other psychiatric disorders, whereas irritability is common to many disorders, making it difficult to decide when it is pathological [28]. Further, the measurement of irritability is complicated because the assessment tools routinely used vary considerably in terms of anchor points. Another parameter that warrants further consideration is age, because adolescents usually have a more classic adult-like profile with acute episodes of illness, fewer and less severe comorbidities and an episodic course, whereas in the prepubertal population BD remains a much more difficult entity to define and diagnose [29].
Clearly, on all fronts, further refinement of the phenotype is necessary and this will no doubt help better predict the course of the disorder [28]. In this context Dickstein and Leibenluft have identified four phenotypes of JBD [28]. The first is a narrow phenotypic group that meet DSM-IV-TR [18] criteria and further, have clearly defined episodes of euphoria for at least 4 days in the case of hypomania, or 7 days in the case of mania. Eliminating irritability makes the patients in this group much more homogenous. The second phenotypic group does not meet duration criteria for mania because their symptoms typically last between 1 and 3 days. The third group have mood disturbance with distinct episodes that last at least 4 days but the disturbance is characterized by irritability rather than euphoria. Members of the final phenotypic group experience severe mood dysregulation and present with chronic irritability as the aberrant mood state. These four phenotypes are recommended for use, particularly in research, in order to draw comparisons with healthy controls and other child patient groups, although the usefulness of phenotypic differentiation can be proved only with long-term outcome studies of each subtype and their eventual underpinning by neurobiological markers.
Conclusion
JBD is attracting growing interest and drawing controversy from all quarters but in particular from clinicians across a number of specialties. It is clear that in regards to JBD, researchers and clinicians are currently disadvantaged by a lack of knowledge as concerns long-term outcome both in this clinical population and beyond. Consequently, there is widespread uncertainty about which guidelines are best suited for use in clinical practice and marked disagreement between researchers in the field as to the inclusion and exclusion criteria for JBD.
However, given the urgent need for progress in this field, a wait-and-see policy to determine which guidelines prevail is an approach we can ill-afford. Instead, we propose that researchers and clinicians adopt the most pertinent features of each of the three guidelines. For instance, the NIMH guidelines give useful anchors to clinicians struggling with ambiguous presentations of JBD, whereas the NICE guidelines, with an emphasis on follow up and continued observation of children with BD, as well as at-risk children, are likely to maximize the information that can be obtained relating to differing manifestations. Further, acknowledging that like adults, where BD commonly presents with mixed states [30], children and adolescents may also present with a variety of symptoms, allows conceptualizing of the disorder outside of criteria for a non-specific category. Even if applied empirically this could eventually yield a better definition of a bipolar prodrome [31]. Finally, the CPW guidelines [9]have drawn on the extensive first-hand experience of many clinicians and researchers with expertise in the area of JBD, and thus provide practical descriptors of commonly occurring symptoms in this disorder. Elements of each of these guidelines provide a useful framework for research and application in clinical practice and should form the basis of much-needed long-term outcome studies of JBD. Ultimately, a better understanding of JBD, beyond aiding diagnosis and improving the management of BD in juveniles, is important because it is likely that individuals in this age group also hold the key to determining the aetiology of BD – an advance that would potentially affect all aspects of the illness.