
Abstract
Objective:
We examined associations between developmental vulnerability profiles determined at the age of 5 years and subsequent childhood mental illness between ages 6 and 13 years in an Australian population cohort.
Methods:
Intergenerational records from New South Wales (NSW) Government Departments of Health and Child Protection spanning pre-birth to 13 years of age were linked with the 2009 Australian Early Development Census records for 86,668 children. Mental illness indices for children were extracted from health records between 2009 and 2016 (child’s age of 6–13 years). Associations between mental disorder diagnoses and membership of early childhood risk groups, including those with established ‘special needs’ (3777, 4.3%) at school entry, or putative risk classes delineated via latent class analysis of Australian Early Development Census subdomains – referred to as ‘pervasive risk’ (N = 3479; 4.0%), ‘misconduct risk’ (N = 5773; 6.7%) or ‘mild generalised risk’ (N = 9542; 11%) – were estimated using multinomial logistic regression, relative to children showing ‘no risk’ (N = 64,097; 74%). Poisson regression models estimated the relative risk of a greater number of days recorded with mental health service contacts among children in each Australian Early Development Census risk group. Adjusted models included child’s sex, socioeconomic disadvantage, child protection contacts and parental mental illness as covariates.
Results:
The crude odds of any mental disorder among children aged 6–13 years was increased approximately threefold in children showing pervasive risk or misconduct risk profiles at the age of 5 years, and approximately sevenfold in children with special needs, relative to children showing no risk; patterns of association largely remained after adjusting for covariates. Children with special needs and the misconduct risk class used mental health services over a greater number of days than the no risk class.
Conclusion:
Patterns of early childhood developmental vulnerability are associated with subsequent onset of mental disorders and have the potential to inform interventions to mitigate the risk for mental disorders in later childhood and adolescence.
Introduction
Early indicators of emerging childhood psychopathology may be risk factors for adult mental disorders (Althoff et al., 2010; Copeland et al., 2009; Costello et al., 2003; Kim-Cohen et al., 2003) and up to half of all adult psychiatric diagnoses could be averted with effective treatment provided to those showing signs of risk before the age of 15 years (Kim-Cohen et al., 2003). Putative risk for mental disorder can be identified via latent patterns of vulnerability across a range of early childhood developmental competencies, and may represent intermediate and potentially modifiable stages on developmental pathways to later psychopathology (Green et al., 2018b). Here, we examined the utility of early childhood developmental risk profiles as potential indicators of the likelihood of later childhood mental illness in a longitudinal population cohort study of children for whom intergenerational (child and parent) records from health, education and child protection services (from pre-birth to age ~13 years) were linked with an assessment of developmental vulnerability at the age of 5 years (Green et al., 2018a).
The utility of putative risk classes delineated at school entry for predicting later childhood-onset mental disorders has yet to be examined at a population level. Previous studies using similar methods to determine latent classes of early childhood risk for mental illness (encompassing multiple developmental indicators) have been predominantly derived in smaller population samples ranging in size from around 900 to 7000 children; in these studies, between three and five latent classes of internalising and externalising behaviours have typically emerged in early childhood on the basis of clinical ratings on the Child Behavior Checklist (CBCL; Achenbach, 1991; Basten et al., 2013; Davis et al., 2015; Fanti and Henrich, 2010). Longitudinal follow-up of child clusters defined by clinical features has demonstrated both homotypic and heterotypic continuity of psychopathology across the life course; that is, patterns of psychopathology appear to be relatively stable within diagnosis (homotypic) from early to middle childhood, and from middle childhood to adolescence (Achenbach, 1991; Basten et al., 2013; Davis et al., 2015; Fanti and Henrich, 2010; Whalen et al., 2016), with some evidence of heterotypic diagnostic patterns between childhood and adult diagnoses (Althoff et al., 2010).
Consideration of other individual and familial risk factors operating during the life course is also important in estimating the risk for the development of mental disorder. For example, exposure to early life stress (such as childhood maltreatment) is an important, potentially modifiable risk factor for childhood psychopathology (Cicchetti and Toth, 2015) that has been consistently associated with mental disorders in adulthood (Kessler et al., 2010; Spinazzola et al., 2014; Van Nierop et al., 2015), including psychotic disorders (McGrath et al., 2017). Childhood maltreatment has also shown pervasive effects on early childhood developmental functioning assessed at school entry (Green et al., 2018b, 2018c). In addition, exposure to familial mental illness is well known to increase the risk of offspring mental disorder, and may reflect genetic influences and/or related familial (Davis et al., 2015) or social factors (Paksarian et al., 2018) that increase the risk of developing mental illness.
In this study, we examined associations between early childhood developmental risk class-membership at the age of 5 years (Green et al., 2018b) and childhood-onset mental disorders treated in public health care settings. We first delineated a set of mutually exclusive classes of children at putative developmental risk for mental illness (based on patterns of early developmental vulnerability) and then examined associations between membership in each of these putative risk classes and subsequent treatment for mental disorders according to a number of indices including (1) any childhood mental disorder, (2) specific childhood mental disorders and (3) the number of days on which the child had a record of being in contact with mental health services for a mental disorder. All associations were examined in the context of the contribution of parental mental illness or child protection contacts up to the age of 13 years.
Methods
Participants and procedures
We included 82,891 children (50.8% male) from the Wave 2 Linkage of the New South Wales Child Development Study (NSW-CDS) (Green et al., 2018a); mean child age at the time of linkage was 13.15 years (SD = 0.4, range = 11.6–14.9 years). The NSW-CDS is a longitudinal study that combines data from multiple agencies for a population cohort of Australian children who were assessed by their kindergarten teachers on entry to school in the state of New South Wales (NSW) in 2009 (Carr et al., 2016) using the Australian Early Development Census (AEDC; Brinkman et al., 2007). From the full Wave 2 Linkage AEDC sample of 87,037 children, for the purpose of conducting the latent class analysis (LCA), we excluded 369 children for whom AEDC subdomain indicator variables were unavailable and 3777 children designated as having established special needs at school entry (i.e. with an established, diagnosed chronic medical, physical or intellectually disabling condition such as autism, cerebral palsy or Down syndrome). The LCA was thus conducted on 82,891 children with valid AEDC subdomain data. In subsequent analyses of associations with mental illness, we included the group of 3777 children with established special needs as an additional risk group of interest (see O’Connor et al. [2018] for information about the proportion of children identified with particular medical diagnoses in the national 2009 AEDC cohort). Among the total AEDC cohort of 86,668 children included in the regression analyses, 72,731 (83.9%) had births registered in NSW to enable linkage to parental administrative records and 1561 had a mental illness diagnosed prior to the AEDC assessment (these children were excluded in sensitivity analyses presented in Supplementary Tables S6–S8).
Record linkage of multi-agency data for child and parent cohorts of the NSW-CDS was conducted by the Centre for Health and Record Linkage in 2016, using probabilistic record linkage methods across a set of minimal identifiers, with ethical approval from the NSW Population & Health Services Research Ethics Committee (PHSREC AU/1/1AFE112) and data custodian approvals granted by the relevant government departments. The linkage process maintained the separation of personal identifiers from research content (e.g. health information) to preserve privacy and confidentiality for all persons in the linked datasets, who remained anonymous to the research team.
Exposures
Early childhood risk profiles
LCA (Collins and Lanza, 2010) conducted on 82,891 children with valid AEDC subdomain data determined four classes of children on the basis of patterns of vulnerability on 16 AEDC subdomains (Figure 1); LCA was conducted using SAS® 9.4 with the PROC LCA macro (Lanza et al., 2007; SAS, 2015). The AEDC uses 96 items to measure 16 subdomains of child functioning (see Supplementary Table S1), conceived within five broad domains of function, each with acceptable reliability (Cronbach’s α): social competence (α = 0.95), emotional maturity (α = 0.93), physical health and well-being (α = 0.80), language and cognition (α = 0.91) and communication and general knowledge (α = 0.90) (Brinkman et al., 2007; Janus et al., 2011). Children are considered developmentally vulnerable if they score in the lowest 10% of the national population distribution (Brinkman et al., 2014). Class membership was determined via probability indicators (γ) and the associated item-response probabilities (ρ) for vulnerability indicators (see Supplementary Tables S2 and S3). The prevalence of the four putative early childhood risk classes in the current NSW sample is shown in Table 1, confirming our previously published solution in an earlier stage of NSW-CDS record linkages, where the initial LCA was limited to (n = 67,353) children with available parent data (Green et al., 2018b).
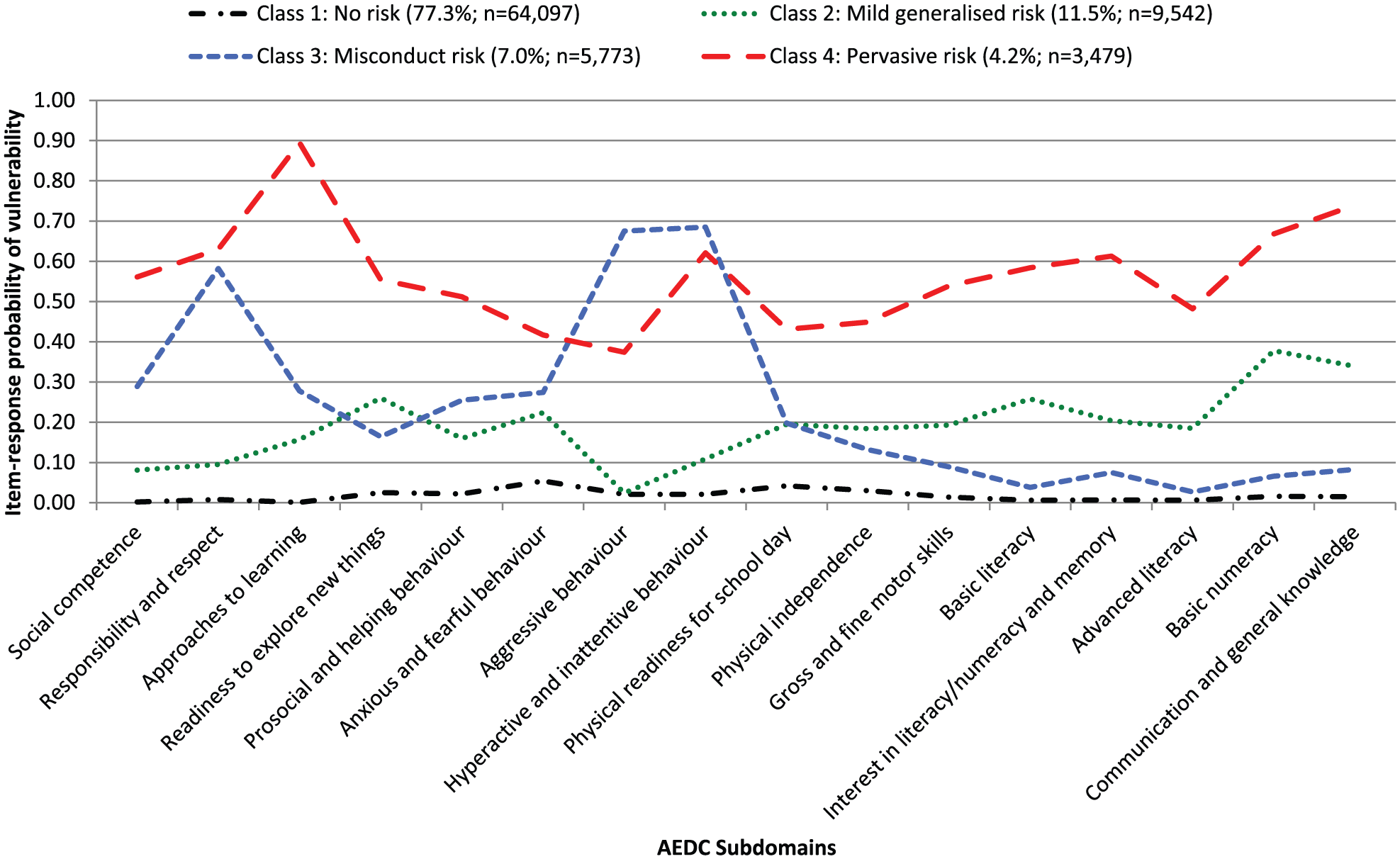
Four latent classes of children (n = 82,891) derived from latent class analyses of 16 Australian Early Development Census (AEDC) subdomains.
Prevalence of early childhood (AEDC) risk categories, diagnosed mental disorder (between ages 6 and 13 years), and covariates for the sample of 86,668 children within AEDC childhood risk categories.
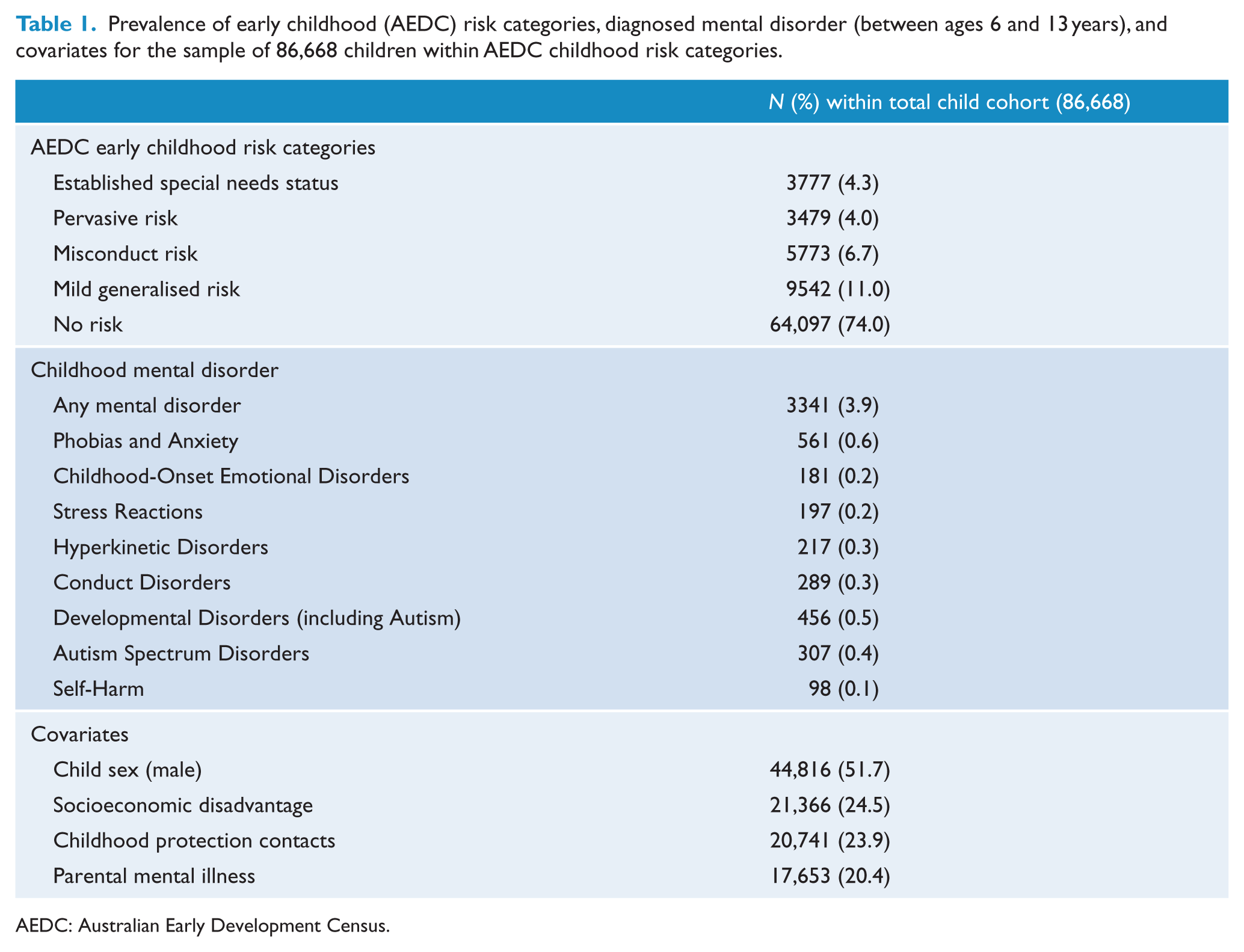
AEDC: Australian Early Development Census.
Child protection contact
A binary indicator of child protection contact in the years 2000–2016 was created using data from the Department of Family & Community Services (FACS) Case Management System – Key Information Directory System (KIDS). There were 20,741 children (23.9%) with valid AEDC data who had at least one child protection report or placement in Out of Home Care (OOHC) prior to the age of 13 years (Table 1). Among these 20,741 children, 2056 (9.9%) had at least one OOHC placement, 17,556 (84.6%) had at least one child protection report that met the threshold for risk of significant harm (i.e. suggesting the need for follow-up by case-workers) and 3114 (15.0%) had a report that did not require follow-up for risk assessment.
Parental mental illness
A binary indicator representing any parental mental illness was determined using International Statistical Classification of Diseases and Related Health Problems (10th rev.; ICD-10) codes representing any type of psychiatric disorder recorded in the NSW Ministry of Health Mental Health Emergency Department Data Collection (EDDC; 2005–2016), Admitted Patients Data Collection (APDC; 2001–2016) and Mental Health Ambulatory (MHAMB; 2001–2016) records, spanning the period from approximately 3 years prior to the child’s birth, up to the child’s age of 13 years. There were 20,741 children who had a parent with any mental disorder in health records, diagnosed according to ICD-10 codes (see Supplementary Table S4).
Child’s sex
A binary indicator of the child’s sex was obtained from a combination of all available record sets for the child (female sex was used as the reference group).
Socioeconomic disadvantage
A binary indicator of socioeconomic disadvantage was computed using the Socio-Economic Indexes for Areas (SEIFA; Pink, 2013) available in AEDC records (see Table 1); quintiles were dichotomised into ‘disadvantaged’ (quintile 1) and ‘not disadvantaged’ (quintiles 2–5; this was used as the reference group).
Outcome variables
Childhood mental disorders
Mental disorder diagnoses were determined for 3341 children with valid AEDC data (See Table 1). Mental disorder diagnoses were determined from ICD-10 codes recorded in primary or secondary diagnoses of the EDDC, APDC and MHAMB records available for the child from 2009 to 2016 (i.e. approximate child age is 6–13 years). These record sets contain administrative data obtained via the Australian (state-based) public health service delivery system; only the APDC includes both public and private hospital admissions. The MHAMB contains records of public ambulatory (i.e. community-based or outpatient) mental health services and does not include ambulatory services provided in the private sector, such as by general practitioners and private psychiatrists or psychologists. The EDDC details diagnoses and procedures provided for emergency department presentations in public hospitals, and the APDC details diagnoses, procedures and services provided for admitted patients to all NSW public general hospitals, public psychiatric hospitals, and private hospitals and day procedure centres.
Binary indicators of any mental disorder (Table 1), as well as non-mutually exclusive indicators of any previous diagnosis of anxiety and neurotic disorders (including Phobias and Anxiety, Stress Reactions), Hyperkinetic Disorders (i.e. Attention-Deficit/Hyperactivity Disorder [ADHD]), Conduct Disorders, Childhood Emotional Disorders, Developmental Disorders and Self-Harm behaviours were derived for use in focal analyses. The ICD-10 AM codes used to define specific childhood-onset mental disorders are summarised in Supplementary Table S5.
Number of days treated for mental health conditions
A count of the total number of days with mental health contacts was computed for each child, using all available health data from birth to the age of 13 years. This index of mental health service uses the included days that a child had been admitted to hospital (APDC or EDDC) for a primary mental health condition, or treated by mental health ambulatory services (i.e. recorded in the MHAMB records) for any mental disorder.
Statistical analyses
Children were assigned to risk categories for the purpose of conducting focal regression analyses; children included in the LCA were assigned to their most likely class, and those with established special needs were included as an additional risk group. Two sets of regression analyses were performed using SPSS v24 (IBM, 2016) to estimate unadjusted and adjusted associations between early childhood risk category membership and (1) ‘any’ and (2) specific mental disorder diagnoses and (3) the number of days treated for mental disorders up to the age of 13 years. Covariates examined in adjusted models included exposure to child protection contacts, parental mental illness, socioeconomic disadvantage and the child’s sex. The first series of analyses used multinomial logistic regressions (MLRs) to examine unadjusted and adjusted associations between early childhood risk classes and (1) any mental disorder diagnosis and (2) any specific mental disorder for the child between 2009 and 2016, using the group of children with no recorded mental illness as the reference group. Sensitivity analyses were repeated for a subcohort of the population (n = 85,107) to exclude 1561 children with evidence of a diagnosis of mental disorder prior to AEDC administration (i.e. in health records up to December 2008, which included 457 children who had also been diagnosed with a mental disorder aged 6–13 years); these results are presented in Supplementary Tables S6–S8. A final series of analyses estimated crude and adjusted relative risk of the number of days with mental health service contacts across the early developmental risk classes, using Poisson regression for negative binomial distribution.
Results
Descriptive statistics
The prevalence of AEDC risk groups and covariates, and the number of children with any diagnosis of specific mental disorders between ages 6 and 13 years, are presented in Table 1 for the total sample of 86,668 children included in regression analyses. The mean number of days with mental health contacts was 19.59 (SD = 49.12) among a total of 4034 children represented in health records with any type of mental health contact (median = 6 days; mode = 1 day; range = 1–755); this reflects more children than those with specific mental disorder diagnoses because of the large number MHAMB contacts where the diagnosis of mental disorder was ‘not otherwise specified’ (i.e. F99).
Latent risk classes
Four classes (Figure 1) were identified among the cohort of 82,891 children included in the LCA, characterised by (1) high probability of developmental vulnerabilities spanning all AEDC domains (social, emotional, physical, cognitive and communication), labelled ‘pervasive risk’ (N = 3479; 4.2%); (2) high probability of disrespectful and aggressive/hyperactive behaviour against a background of low probability for any other type of vulnerability, labelled ‘misconduct risk’ (N = 5773; 7.0%); (3) low probability of vulnerability across the entire spectrum of developmental domains, ‘mild generalised risk’ (N = 9542; 11.5%); and (4) a class showing virtually ‘no risk’ (N = 64,097; 77.3%).
Associations between mental disorder diagnoses and early childhood risk categories
Fit statistics and odds ratios (ORs; with 95% confidence intervals [CIs]) for all MLR models examining the unadjusted odds of any mental disorder among early childhood risk categories are summarised in Table 2. The odds of any mental disorder were higher for pervasive (OR = 3.07; 95% CI = [2.68, 3.51]) and misconduct risk groups (OR = 3.09; 95% CI = [2.77, 3.45]) than for children with mild generalised risk (OR = 1.47; 95% CI = [1.31, 1.66]), when each was compared to the no risk group. The odds of any mental disorder were highest in the group with established ‘special needs’ at school entry (OR = 7.12; 95% CI = [6.44, 7.86]), relative to the no risk class. Models examining associations between specific types of mental disorder and early developmental risk categories revealed large, crude associations for the pervasive and misconduct risk classes and diagnoses of Hyperkinetic Disorders (i.e. ADHD), Developmental Disorders (including Autism Spectrum Disorder) and, to a lesser extent, Conduct Disorders, relative to children with no risk (Table 2). The pervasive and misconduct risk classes also showed weak-to-moderate unadjusted associations with emotional disorders, stress reactions and self-harm, while the mild generalised risk class showed only low-to-medium associations with Hyperkinetic and Developmental Disorders, relative to the no risk group. There were extremely high crude odds of diagnoses of Hyperkinetic, Conduct and Developmental Disorders for children with special needs (see Table 2), likely reflecting existing medical diagnoses among these children prior to school entry (see O’Connor et al., 2018).
Unadjusted odds ratios (and 95% confidence intervals) for ‘any’ and specific mental disorder diagnoses in association with early childhood developmental risk categories (‘pervasive’, ‘misconduct’ and ‘mild generalised’ risk) or those with established ‘special needs’, relative to the ‘no risk’ category.
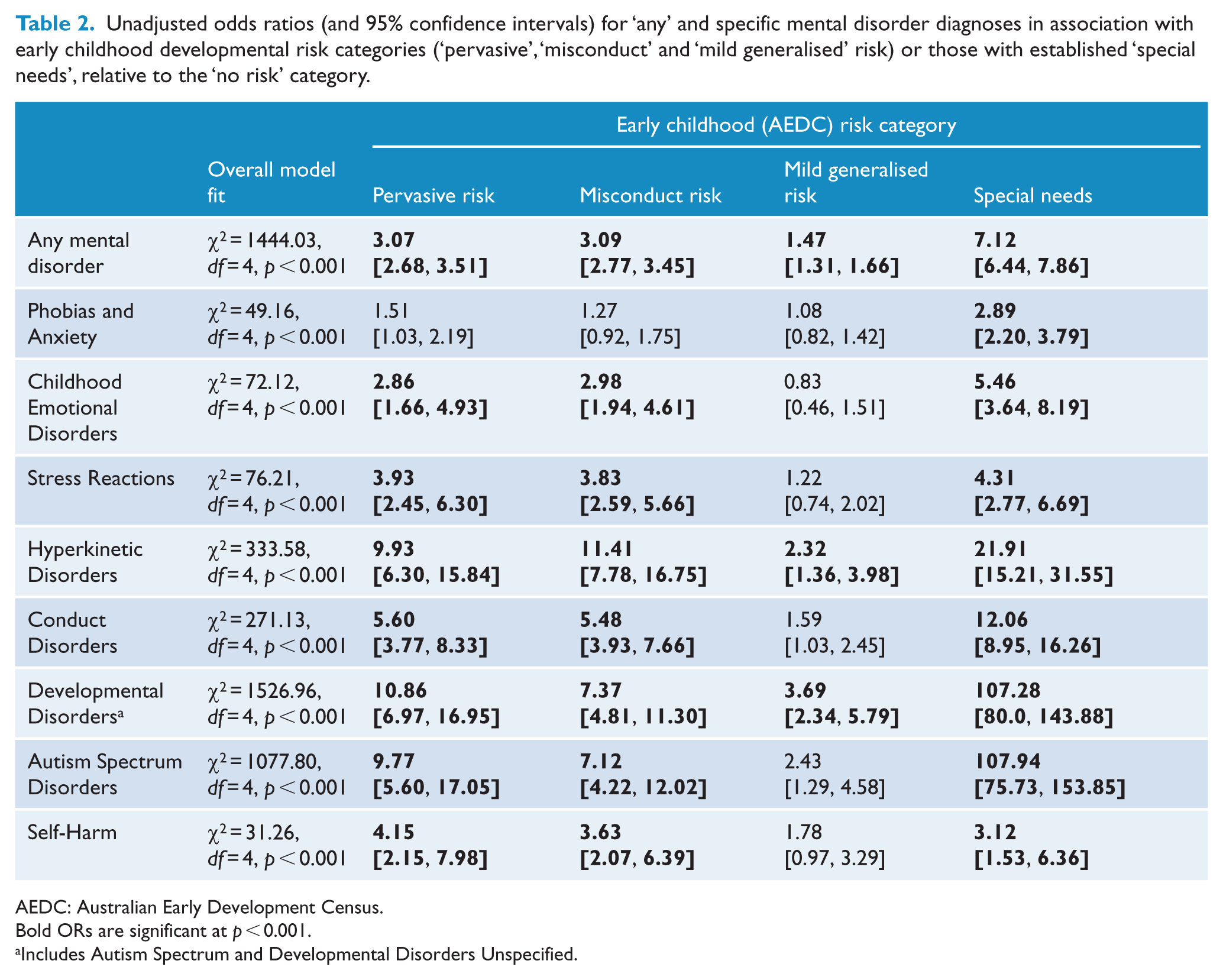
AEDC: Australian Early Development Census.
Bold ORs are significant at p < 0.001.
Includes Autism Spectrum and Developmental Disorders Unspecified.
Subsequent models including the covariates of child protection contact, parental mental illness, socioeconomic disadvantage and male sex reduced the magnitude of the ORs for all mental disorder indices (Table 3). However, the pattern of associations between early childhood developmental risk categories and specific mental disorders largely remained after adjusting for covariates, with the large effects evident for associations between pervasive risk and Developmental Disorders (including Autism), and between misconduct risk and Hyperkinetic Disorders (Figure 2). There were no significant associations between pervasive risk and the internalising disorders (Phobias and Anxiety, Childhood Emotional Disorders, Stress Reactions and Self-Harm) in adjusted models, suggesting some degree of specificity for externalising and developmental disorders for this risk class. Child protection contact was consistently and strongly associated with all mental disorders, with the largest effects for Stress Reactions, Conduct Disorders and, especially, Self-Harm. The odds of being diagnosed with all types of mental disorder (except for self-harm) were greatest for children with special needs.
Adjusted odds ratios (ORs) and 95% confidence intervals (CI) estimating risk for mental disorder diagnoses (relative to no mental disorder) in association with early childhood developmental risk profiles (‘pervasive’, ‘misconduct’ and ‘mild generalised risk’) or those with established ‘special needs’, relative to the no risk profile (adjusted for male sex, socioeconomic disadvantage, parental mental illness history and child protection contacts).
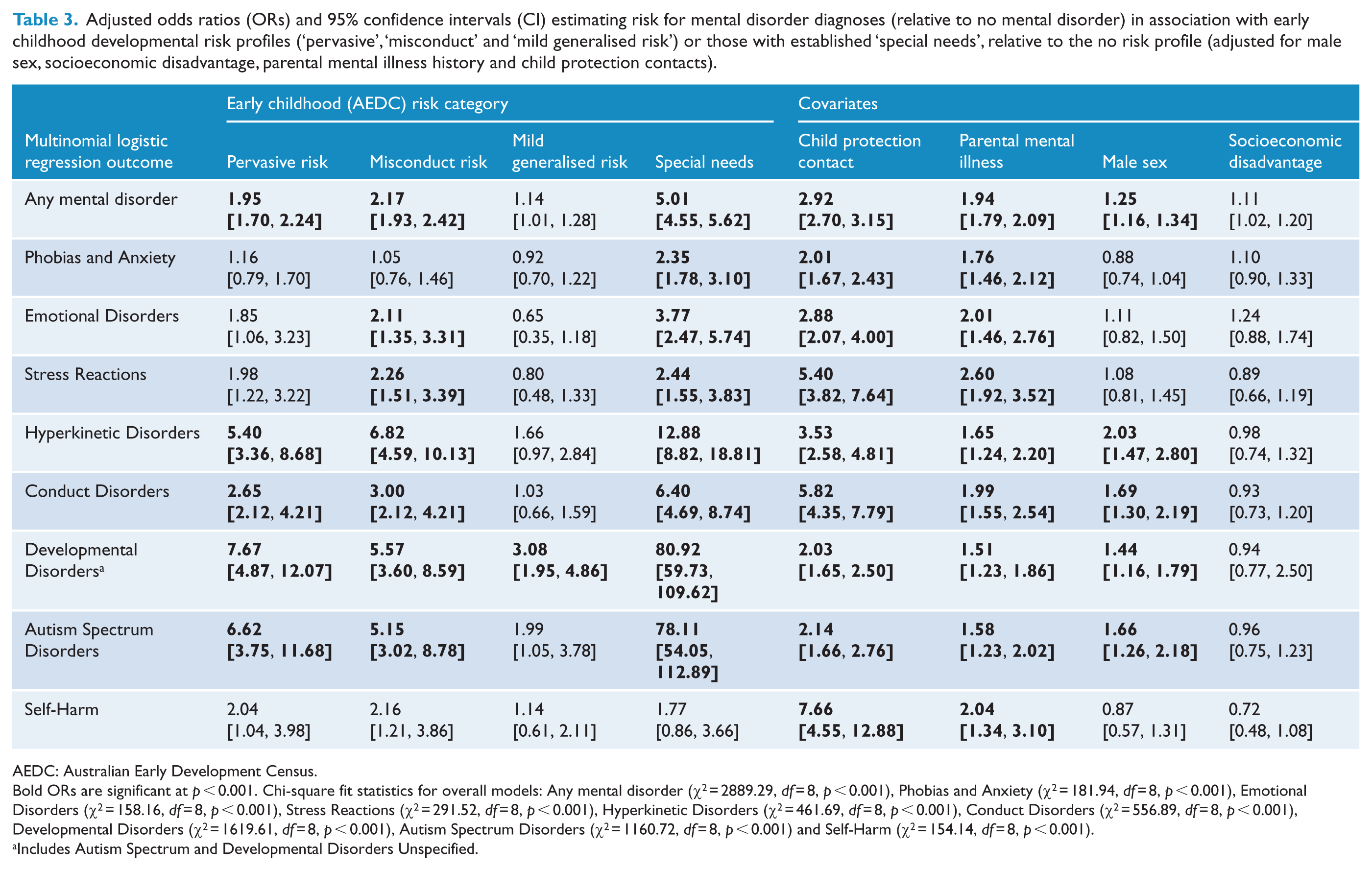
AEDC: Australian Early Development Census.
Bold ORs are significant at p < 0.001. Chi-square fit statistics for overall models: Any mental disorder (χ2 = 2889.29, df = 8, p < 0.001), Phobias and Anxiety (χ2 = 181.94, df = 8, p < 0.001), Emotional Disorders (χ2 = 158.16, df = 8, p < 0.001), Stress Reactions (χ2 = 291.52, df = 8, p < 0.001), Hyperkinetic Disorders (χ2 = 461.69, df = 8, p < 0.001), Conduct Disorders (χ2 = 556.89, df = 8, p < 0.001), Developmental Disorders (χ2 = 1619.61, df = 8, p < 0.001), Autism Spectrum Disorders (χ2 = 1160.72, df = 8, p < 0.001) and Self-Harm (χ2 = 154.14, df = 8, p < 0.001).
Includes Autism Spectrum and Developmental Disorders Unspecified.
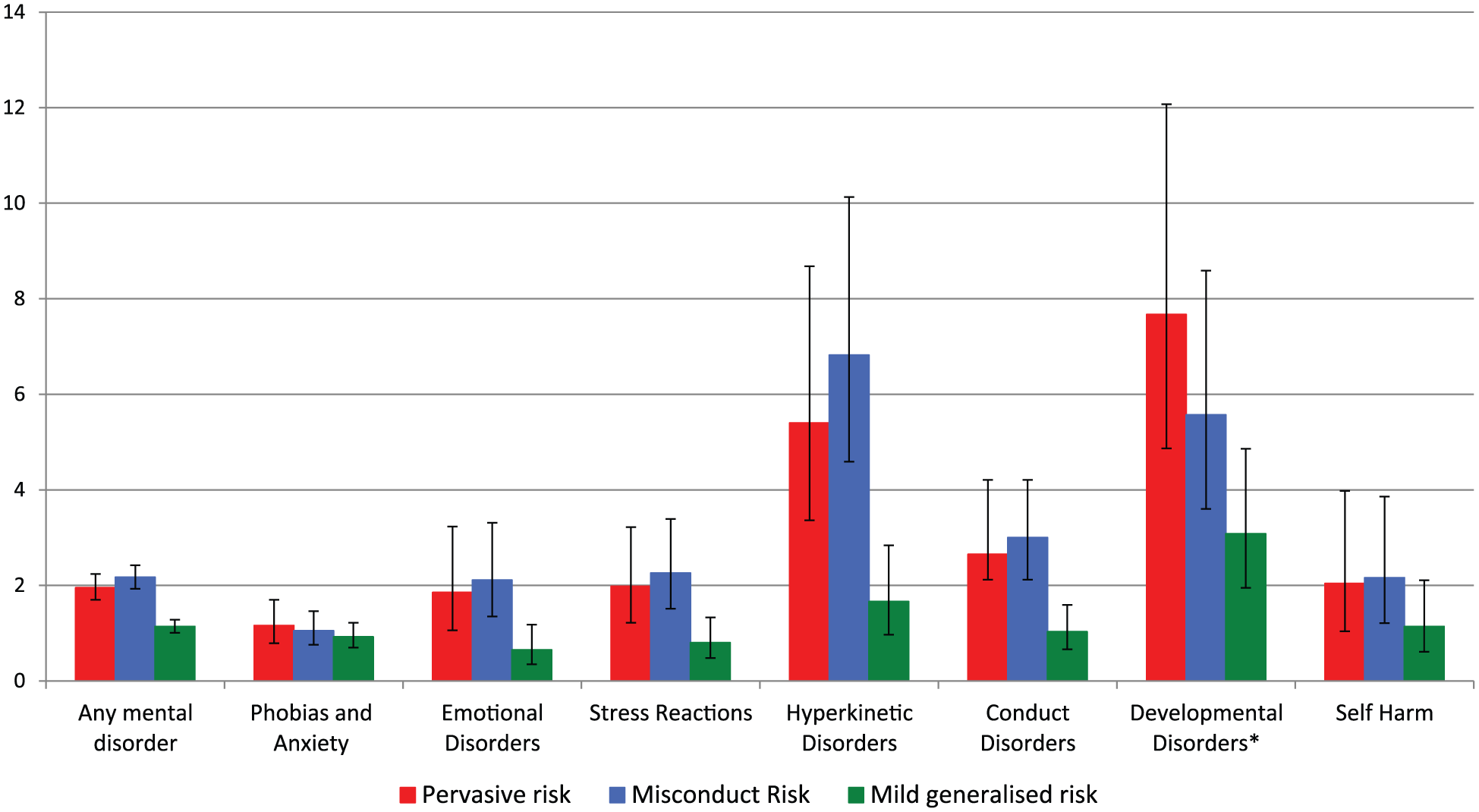
Adjusted associations (odds ratios with 95% confidence intervals) between early childhood risk categories (derived from the latent class analysis of the Australian Early Development Census) and mental illness diagnoses in children aged 6–13 years.
Sensitivity analyses conducted on a subcohort of 85,107 children (i.e. excluding 1561 children with mental illness diagnoses prior to AEDC assessment at the age of 5 years) revealed only subtle changes in the magnitude of findings for the primary risk-classes of interest derived from the LCA. In contrast, the associations for the class of children designated as special needs were more significantly reduced in this subcohort, as expected, since these children had been formally diagnosed with some type of disorder prior to school entry, in order to be rated on the AEDC as having special needs in the classroom.
Number of days with mental health contacts
Unadjusted Poisson regression revealed a greater relative risk of days in mental health care, in the misconduct risk (risk ratio [RR] = 1.73; 95% CI = [1.38, 2.18]; p < 0.001) and the pervasive risk classes (RR = 1.43; 95% CI = [1.14, 1.79]; p = 0.002) relative to the no risk group, but the effects for mild generalised risk were not significant (RR = 1.02; 95% CI = [0.81, 1.28]; p = 0.90). Children with established special needs at school entry also showed greater unadjusted relative risk of days in mental health care (RR = 15.27; 95% CI = [14.03, 16.63]), relative to the no risk group. Among the AEDC LCA risk classes, only the association with the misconduct risk class remained significant (RR = 1.63; 95% CI = [1.28, 2.07]; p < 0.001) in adjusted models, as did the association with the group with established special needs (RR = 1.89; 95% CI = [1.48, 2.4]; p < 0.001). There were also significant effects of parental mental illness (RR = 1.24; 95% CI = [1.08, 1.43]; p < 0.001) and child protection contacts (RR = 1.56; 95% CI = [1.35, 1.81]; p < 0.001), but not male sex (RR = 1.00; 95% CI = [0.87, 1.15]; p = 0.97) or socioeconomic disadvantage (RR = 1.14; 95% CI = [0.98, 1.32]; p = 0.07). The mean number of days with mental health contacts was estimated as 18.34 days for the pervasive risk class (standard error [SE] = 1.90), 24.44 days for the misconduct risk class (SE = 2.83), 13.96 days for the mild generalised risk class (SE = 1.33), 28.53 days for the group with special needs (SE = 3.29) and 15.05 days for the no risk class (SE = 0.71) groups, when accounting for the effects of covariates in the adjusted model.
Discussion
In a large representative population of Australian children, we confirmed our previous typology of putative risk for mental disorders based on early childhood developmental vulnerability indicators at the time of school entry (age of 5 years; Figure 1). Two of these risk classes, pervasive and misconduct risk, which accounted for 10–11% of the population, showed strong and consistent associations with mental disorders recorded in administrative hospital inpatient and ambulatory mental health records from middle childhood (~6 years) to late childhood (~13 years), relative to those showing virtually no developmental risk (77% of the child population) at the age of 5 years. The mild generalised risk class showed small-to-moderate associations with developmental disorders only. Extremely large odds of being diagnosed with a mental disorder were observed for children designated as having special needs at school entry, consistent with their definition as a group with established medical issues that require special assistance in the classroom; these children may already have been diagnosed with developmental or other behavioural disorders, or else had recognised physical or intellectual disability, prior to starting school (O’Connor et al., 2018). The strongest covariate effects were observed for child protection contacts, while parental mental disorders showed small but consistently significant associations with childhood mental disorders in all models. Among children in risk classes defined by the LCA, the number of days treated for mental disorder was highest in children classed as misconduct risk; this is consistent with the evidence of higher utilisation of specialist child mental health services among children with conduct disorder in the United Kingdom (Shivram et al., 2009).
These findings demonstrate strong evidence for homotypic continuity of putative developmental risk profiles and the diagnoses of mental disorders in middle childhood and very early adolescence, in line with previous evidence (Fanti and Henrich, 2010; Whalen et al., 2016). In particular, children classified as misconduct risk at the age of 5 years (owing to externalising behaviours including aggression, hyperactivity and inattention that would be disruptive in the classroom) showed very strong odds of being diagnosed with Hyperkinetic or Conduct Disorders, as well as Developmental Disorders (including Autism), by the age of 13 years. At the age of 5 years, the misconduct risk group of children most closely resembled those referred to as having ‘dysregulation syndrome’ in smaller longitudinal studies of children of comparable age, but were not rated by teachers as having overt emotional (internalising) vulnerabilities that are seen when risk classes are determined on the basis of CBCL data (Basten et al., 2013; Davis et al., 2015); this fits with the observation of relatively small associations with internalising disorders in the misconduct risk class, but might also reflect the limited capacity of teachers to identify internalising vulnerability in the classroom (relative to overt externalising behaviours). Of course, it is possible that this pattern of findings for the misconduct risk class reflects the greater propensity for these children to be treated in the public sector, given the familial risk factors (child protection contacts and parental mental illness) that were also strongly associated with childhood conduct, hyperkinetic and developmental disorders. Recent Australian data shows that 72.5% of children with moderate forms of disorder and 87.6% of children with severe mental disorders access public health services in a 12-month period (Johnson et al., 2016).
Children deemed at pervasive risk of mental disorders at the age of 5 years showed the highest odds of Developmental Disorders and Hyperkinetic Disorders in middle childhood, but no significant associations with internalising disorders. This is consistent with the characteristics of the pervasive risk class at the age of 5 years, indicative of widespread neurodevelopmental dysfunction associated with learning difficulties and impaired cognitive functioning; these children may be in need of targeted neurocognitive as well as behavioural remediation from an early age. Finally, children in the mild generalised risk class at the age of 5 years (showing modest peaks on literacy and numeracy vulnerabilities) also showed a small-to-moderate increase in the odds of being diagnosed with a Developmental Disorder, but no other type of mental disorder, after adjusting for the contribution of other covariates (childhood protection contacts, parental mental illness and male sex). These findings highlight the value of including language and cognitive vulnerabilities in addition to the internalising and externalising variables typically used in the derivation of early childhood risk profiles via latent modelling.
There were strikingly large associations between child protection contacts and mental disorders in middle-to-late childhood (medium-to-large effect sizes), with the strongest association reflected in a sevenfold increase in the odds of self-harm among children with a history of protection contacts. These findings are consistent with considerable evidence for the role of stress-related processes in the development of childhood psychopathology and later mental disorders (Spinazzola et al., 2014; Van Nierop et al., 2015). Importantly, not all contacts with child protection services necessarily reflected severe or prolonged child maltreatment, since we considered all levels of child protection reports as a risk indicator. That is, while the majority of child protection reports had been substantiated, others had not been followed-up by case-workers to enable substantiation owing to resource limitations (despite having met thresholds for ‘risk of significant harm’ according to decision-making tools), while other reports were not regarded as representing a significant risk of harm that would typically require follow-up. Our findings thus suggest that any level of reporting to child protection services indicates a potential threat to child safety, or at least a significantly stressful environment for the child. Cross-agency communication of all levels of child protection reporting may enable appropriate school-based interventions to prevent the development of mental disorders in childhood in the context of observable developmental risk at school entry, or via health services offered to vulnerable mothers in postnatal and early childhood periods.
By comparison, the strength of associations of parental mental illness and male sex were relatively modest after accounting for the contributions of early childhood risk profiles and child protection contacts. It is possible that stronger, disorder-specific familial risk may be elucidated with the use of more detailed exposure estimates for parental mental illness that were not investigated here, and that distinct familial patterns of risk may be associated with persistent mental health problems from childhood into adolescence (Moffitt, 1993, 2007). It is also possible that the small, observed effects of parental illness on childhood mental disorder may be at least partly mediated by early childhood developmental vulnerabilities. Investigation of more complex pathways to mental illness will require iterative modelling (e.g. testing hypothesised moderated mediation models) from birth to mental disorder diagnosis, with consideration of the potential contribution of other known risk factors for developmental vulnerabilities and/or mental disorders (e.g. perinatal adversities) that were not considered here. Notably, there were no significant effects of socioeconomic disadvantage in any models tested, and sensitivity analyses for a subcohort of the population that excluded children who had been diagnosed with mental disorders prior to the AEDC assessment demonstrated a robust pattern of findings for our LCA-derived risk classes; only the associations for the class of children designated as special needs were more significantly reduced, in line with these children having been formally diagnosed prior to school entry. Finally, the significantly higher odds of developing Hyperkinetic, Conduct and Developmental Disorders for males in the NSW-CDS cohort, though small in effect size relative to other risk factors, is consistent with higher rates of these disorders among males of this age group in the most recent Australian National Survey of Child and Adolescent Mental Disorders (Lawrence et al., 2016).
The present findings provide a framework for the early detection of risk for later mental disorders that could prevent a cascade of neurodevelopmental processes leading to poor mental health in later life (Marin, 2016). While it remains unclear as to whether early childhood risk profiles delineated via LCA represent early manifestations of emerging mental disorder evident in behavioural and cognitive development, or antecedent developmental vulnerabilities, the utility of these developmental risk profiles in providing a means for targeting preventive interventions remains of high significance. Later adverse outcomes may not be inevitable: some children may develop resources to recover from mental ill health (or other social and educational challenges) during later years of childhood (Shannon et al., 2007), while others may benefit from targeted interventions at critical periods of development (Bayer et al., 2009). Notably, previous longitudinal studies suggest that up to 25–50% of adult disorders are preceded by childhood conduct and oppositional behavioural disorders (Copeland et al., 2009; Kim-Cohen et al., 2003), and this accords with the present findings in which children identified as misconduct risks at the age of 5 years were more likely to present with a range of mental disorders before adolescence and had the greatest number of days receiving mental health treatment in hospital settings (among risk groups identified on the basis of AEDC LCA profiles); this group may thus be displaying a diagnostically non-specific signal indicating risk for a variety of adult mental disorders that may emerge in later years. Future waves of linkage will facilitate the investigation of complex pathways from early childhood risk factors, through emerging psychopathology to determine risk trajectories associated with adolescent-onset disorders such as affective and non-affective psychoses, or other adverse social outcomes (e.g. criminal justice contacts, education incompletion and unemployment).
The retrospective analysis of longitudinal data obtained via record linkage confers several advantages, including the avoidance of recall and minimisation of sampling biases, and the capacity to consider the temporal context of exposures and outcomes within discrete developmental periods. However, a number of limitations should also be considered. First, the administrative data used in the present analyses were not collected for these research purposes; potential errors in data entry or quality are therefore possible. The use of predominantly public-sector health records of mental illness may also underestimate the extent of less severe mental disorder in the population, given the inability to capture untreated mental disorders and those managed entirely in the private ambulatory sector. We also note the unavailability of linked child and parental health data for those not born in NSW or who may have since moved interstate. Second, we did not report models including risk factors related to perinatal adversities, despite their known associations with later onset mental illness (Fitzsimons et al., 2017; Tearne et al., 2015); we have already demonstrated the relatively small effects of these early life risk factors on age five developmental risk profiles (Green et al., 2018b). Third, we assigned children to their most likely LCA class for analysis, which can produce bias, although this is unlikely given the high probabilities with which children were originally classified by the LCA model. Finally, associations between early childhood physical illness and mental illness diagnoses were not examined here, despite evidence for their negative effects on early childhood developmental vulnerabilities (Bell et al., 2016), and both child (Neilsen et al., 2017) and adult mental disorders (Kohler et al., 2017).
In conclusion, this study shows that approximately 10% of children in the general population, identified via early developmental vulnerability profiles at the age of 5 years, are at high risk of developing early-onset mental disorders by the age of 13 years; these children are highly likely to have contact with child protection services, and longer periods of mental health care, relative to children showing no risk of mental disorder at the age of 5 years. Children with established special needs at school entry are also more likely to being treated for all types of mental disorders in the period between middle childhood and early adolescence. The provision of timely intervention for these children could mitigate poor mental health trajectories into adolescence and adulthood. These findings deserve the attention of government policy makers.
Supplemental Material
5._Green_AEDC-MH_Supplementary_Material_201018_clean – Supplemental material for Early developmental risk for subsequent childhood mental disorders in an Australian population cohort
Supplemental material, 5._Green_AEDC-MH_Supplementary_Material_201018_clean for Early developmental risk for subsequent childhood mental disorders in an Australian population cohort by Melissa J Green, Stacy Tzoumakis, Kristin R Laurens, Kimberlie Dean, Maina Kariuki, Felicity Harris, Sally A Brinkman and Vaughan J Carr in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
This research was conducted by the University of New South Wales (UNSW, Sydney), using population data owned by the Commonwealth Department of Education; NSW Education Standards Authority; NSW Department of Family & Community Services; NSW Ministry of Health; NSW Registry of Births, Deaths and Marriages; the Australian Bureau of Statistics; and the Bureau of Crime Statistics and Research. The information and views contained in this study do not necessarily, or at all, reflect the views or information held by these Departments.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was conducted by UNSW Sydney, with financial support from the Australian Research Council (Linkage Project LP110100150, with the NSW Ministry of Health, NSW Department of Education, and the NSW Department of Family and Community Services representing the Linkage Project Partners); the National Health and Medical Research Council (NHMRC Project Grants APP1058652 and APP1048055); and the Australian Rotary Health (Mental Health for Young Australians Research Grants 104090 and 162302). M.J.G. was supported by the NHMRC R.D. Wright Biomedical Career Development Fellowship (APP1061875); K.R.L. was supported by the ARC Future Fellowship (FT170100294). S.T. was supported by the NARSAD Young Investigator Grant from the Brain & Behavior Research Foundation.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.