
Abstract
Objective:
Detecting the early emergence of childhood risk for adult mental disorders may lead to interventions for reducing subsequent burden of these disorders. We set out to determine classes of children who may be at risk for later mental disorder on the basis of early patterns of development in a population cohort, and associated exposures gleaned from linked administrative records obtained within the New South Wales Child Development Study.
Methods:
Intergenerational records from government departments of health, education, justice and child protection were linked with the Australian Early Development Census for a state population cohort of 67,353 children approximately 5 years of age. We used binary data from 16 subdomains of the Australian Early Development Census to determine classes of children with shared patterns of Australian Early Development Census–defined vulnerability using latent class analysis. Covariates, which included demographic features (sex, socioeconomic status) and exposure to child maltreatment, parental mental illness, parental criminal offending and perinatal adversities (i.e. birth complications, smoking during pregnancy, low birth weight), were examined hierarchically within latent class analysis models.
Results:
Four classes were identified, reflecting putative risk states for mental disorders: (1) disrespectful and aggressive/hyperactive behaviour, labelled ‘misconduct risk’ (N = 4368; 6.5%); (2) ‘pervasive risk’ (N = 2668; 4.0%); (3) ‘mild generalised risk’ (N = 7822; 11.6%); and (4) ‘no risk’ (N = 52,495; 77.9%). The odds of membership in putative risk groups (relative to the no risk group) were greater among children from backgrounds of child maltreatment, parental history of mental illness, parental history of criminal offending, socioeconomic disadvantage and perinatal adversities, with distinguishable patterns of association for some covariates.
Conclusion:
Patterns of early childhood developmental vulnerabilities may provide useful indicators for particular mental disorder outcomes in later life, although their predictive utility in this respect remains to be established in longitudinal follow-up of the cohort.
Introduction
Adult mental disorders emerge from multiple cumulative and interactive effects of inherited genetic vulnerability and negative exposures that occur over the life course (Shonkoff et al., 2012) and are often preceded by observable childhood psychopathology (Althoff et al., 2010; Copeland et al., 2009; Costello et al., 2003; Kim-Cohen et al., 2003) that may provide critical windows of opportunity for preventative intervention (Marin, 2016). Recent Australian population-based studies using the Longitudinal Study of Australian Children (LSAC) have estimated a high prevalence of risk for mental disorder in 10,000 Australian children (aged 3 months to 13 years) using a wide array of indices spanning familial factors and childhood antecedents (Guy et al., 2016). The current challenge to prevent adult mental disorders is thus to determine early indicators of risk that may be responsive to universal support programmes or to more targeted interventions for particularly vulnerable children. In this study, we set out to identify early childhood developmental vulnerability profiles within the general population that may confer risk for later mental disorders.
In the first 5 years of life, key brain networks are established to support future social, emotional and cognitive capacities (Giedd et al., 2015; Gogtay et al., 2004; Lyall et al., 2015). The plasticity of the brain during these critical periods of development makes it highly sensitive to stress (Hanson et al., 2012; Panzer, 2008). Exposure to physical (e.g. perinatal complications) or psychological trauma (e.g. child maltreatment) can disrupt healthy development, with cascading effects throughout the life course (Healy, 2004; Hodel et al., 2015; Shonkoff et al., 2012). For example, early childhood maltreatment negatively affects various domains of psychosocial development (Cicchetti, 2016) and is also associated with emerging psychopathology in middle childhood and adolescence (Cicchetti and Toth, 2015; Natsuaki et al., 2009; Oshri et al., 2013; Pears et al., 2008; Rogosch and Cicchetti, 2004), extending to mental health problems in adulthood (Dunn et al., 2013; Kaplow and Widom, 2007). The psychological effects of stress may also be influenced by inherited (e.g. genetic) susceptibilities to particular mental disorders and adverse event exposures during gestation.
For example, exposure to familial mental illness is a strong risk factor for mental illness in offspring that does not respect psychiatric classification systems (Lichtenstein et al., 2009). Parental criminal offending and exposure to family violence are also associated with later mental illness (e.g. personality and other disorders) as well as the intergenerational transmission of criminality and victimisation (Leschied et al., 2008). Such exposures may contribute to the development of early childhood susceptibility profiles that may themselves signify intermediate and potentially modifiable stages on the pathways to later mental disorder. The effects of these exposures may equally interact with other (e.g. stress-related) mechanisms to increase the likelihood that particular cognitive and behavioural vulnerability patterns persist throughout development into adulthood. Finally, pregnancy-related factors (e.g. maternal smoking during pregnancy, young maternal age) and birth complications (e.g. gestational diabetes, low birth weight) are known risk factors for severe mental disorders such as affective and non-affective psychoses (Laurens et al., 2015) and have been shown to affect developmental functioning in childhood (Anthopolos et al., 2013).
Statistical approaches to determine latent profiles of risk encompassing multiple indicators, such as latent trajectory modelling, are increasingly used to investigate the developmental origins of mental illness. Using population samples ranging in size from around 900 to 7000 children, four latent classes of internalising and externalising behaviours have typically emerged in early childhood on the basis of clinical ratings on the Child Behavior Checklist (CBCL; Achenbach, 1991; Basten et al., 2013; Davis et al., 2015), with both homotypic and heterotypic continuity of psychopathology evident from early to middle childhood (Basten et al., 2016). One study of just over 2000 individuals has deviated from this pattern of findings, using overlapping CBCL assessment waves from multiple longitudinal birth cohort studies of children spanning the ages of 4–16 years (Althoff et al., 2010); in this study, seven latent classes of psychopathology emerged at time 1 (early childhood), and these classes were relatively stable across middle childhood and adolescence, but showed heterotypic diagnostic patterns between childhood psychopathology and adult Diagnostic and Statistical Manual of Mental Disorders (DSM) diagnoses at age 18–32 years (Althoff et al., 2010). The determination of risk factors for adult mental disorder thus requires understanding these complex patterns of emerging psychopathology beginning in early childhood, in the context of influences by a range of external factors operating throughout development into adult life.
Here, we used latent class analysis (LCA) to determine a set of mutually exclusive classes of children in the general population, which may represent putative risk states for later mental disorders. This was conducted using measures of early childhood developmental vulnerability across a range of domains, as assessed by the Australian Early Development Census (AEDC) of 2009, in a general population cohort of 67,353 children within the New South Wales Child Development Study (NSW-CDS; Carr et al., 2016). Unlike previous studies that used clinical information to classify children, our assessment at age 5 years included unique indices of language and cognitive functioning, offering the potential to disaggregate children at risk of learning disorders from those with affective dysregulation. We were also able to examine the extent to which exposure to specific familial factors, including child maltreatment, parental mental illness and parental criminal offending, and other perinatal factors were associated with membership in each of the risk profiles, while taking into account the effects of demographic factors (sex and socioeconomic status).
Methods
Study context
The NSW-CDS is a prospective, longitudinal, population-based study that combines data from multiple agencies via probabilistic linkage undertaken by the Centre for Health Record Linkage (www.cherel.org.au; Carr et al., 2016). The full NSW-CDS sample of 87,026 children represents 99.7% of NSW children who were assessed by their kindergarten teachers on entry to school in 2009 using the AEDC, a validated measure of childhood developmental vulnerability on multiple domains of functioning (Brinkman et al., 2007).
Participants
The present sample of 67,353 children (mean age = 5.6 years; standard deviation [SD] = 0.4) was derived from the first wave of record linkage from the NSW-CDS (nsw-cds.com.au) conducted in 2013–2014 (Carr et al., 2016), with ethical approval from the NSW Population Health Services Human Research Ethics Committee (PHSREC/11/CIPHS/14). From the full NSW-CDS child sample of 87,026, we excluded 14,781 children whose births were not registered in NSW (i.e. those with no linked parental records) and 3129 children with special needs (based on AEDC records denoting chronic medical, physical or intellectually disabling conditions), 1588 children who were not the first-born among twins, triplets or quadruplet births (i.e. we retained singletons and first-born children for analyses) and 175 children with no AEDC subdomain data available in AEDC records.
Measures
Child vulnerability
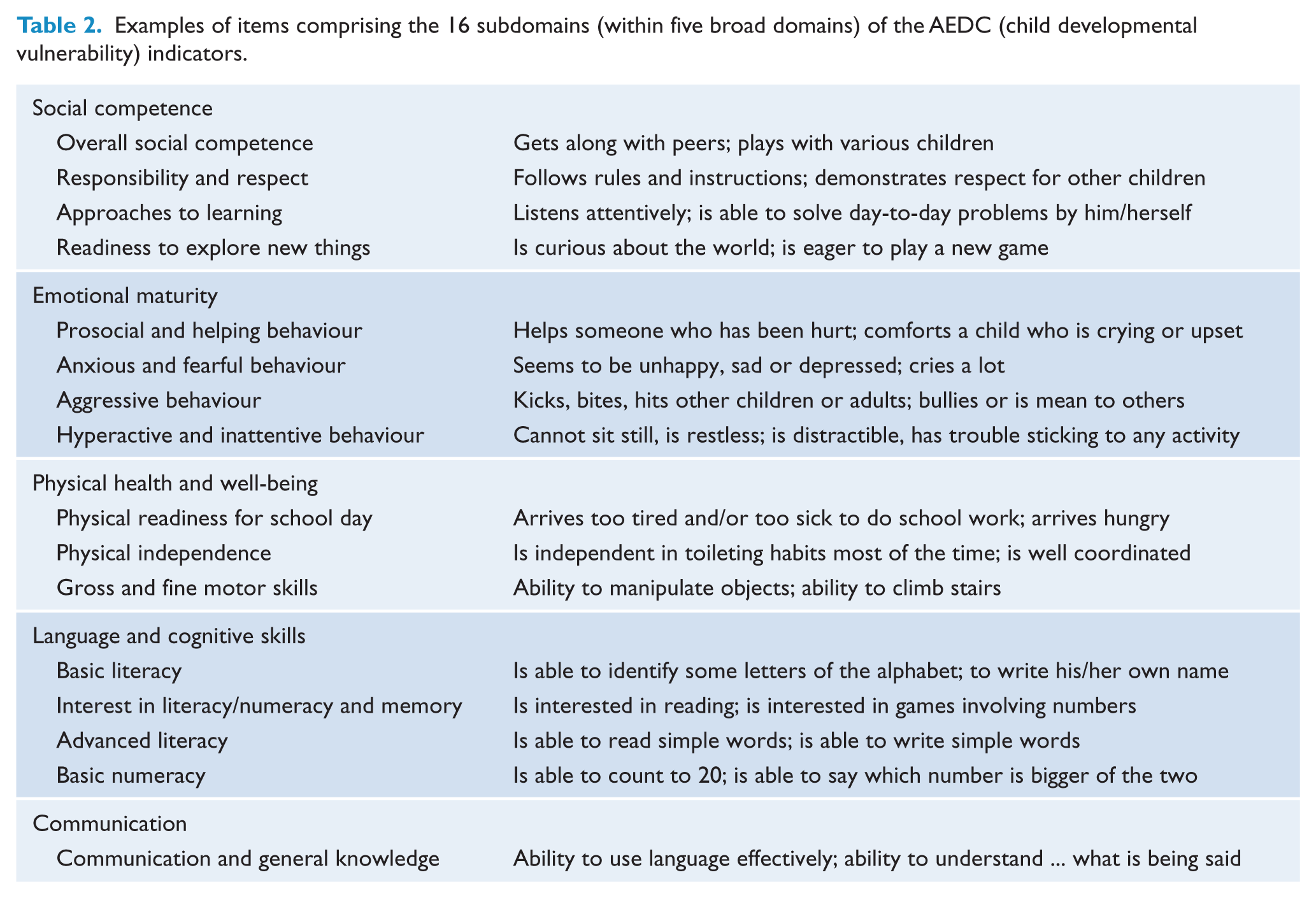
A total of 16 indicators from the AEDC were used to index children’s developmental vulnerability at age 5 years. The AEDC is a 104-item population measure of developmental competencies, from which 96 items are used to summarise 16 subdomains of child functioning (conceived within five broad domains of function that span social, emotional, physical, cognitive and communication competencies). Children were considered developmentally vulnerable on any subdomain if they scored in the bottom 10% of the national AEDC population distribution (Brinkman et al., 2014). Table 1 shows that the prevalence of developmentally vulnerable children in the current NSW sample varies from 5.5% to 10.7% across the 16 indicators (Brinkman et al., 2014), and Table 2 presents example items for the 16 AEDC subdomains.
Prevalence of early childhood developmental vulnerability and covariates in the sample of 67,353 children and their parents.
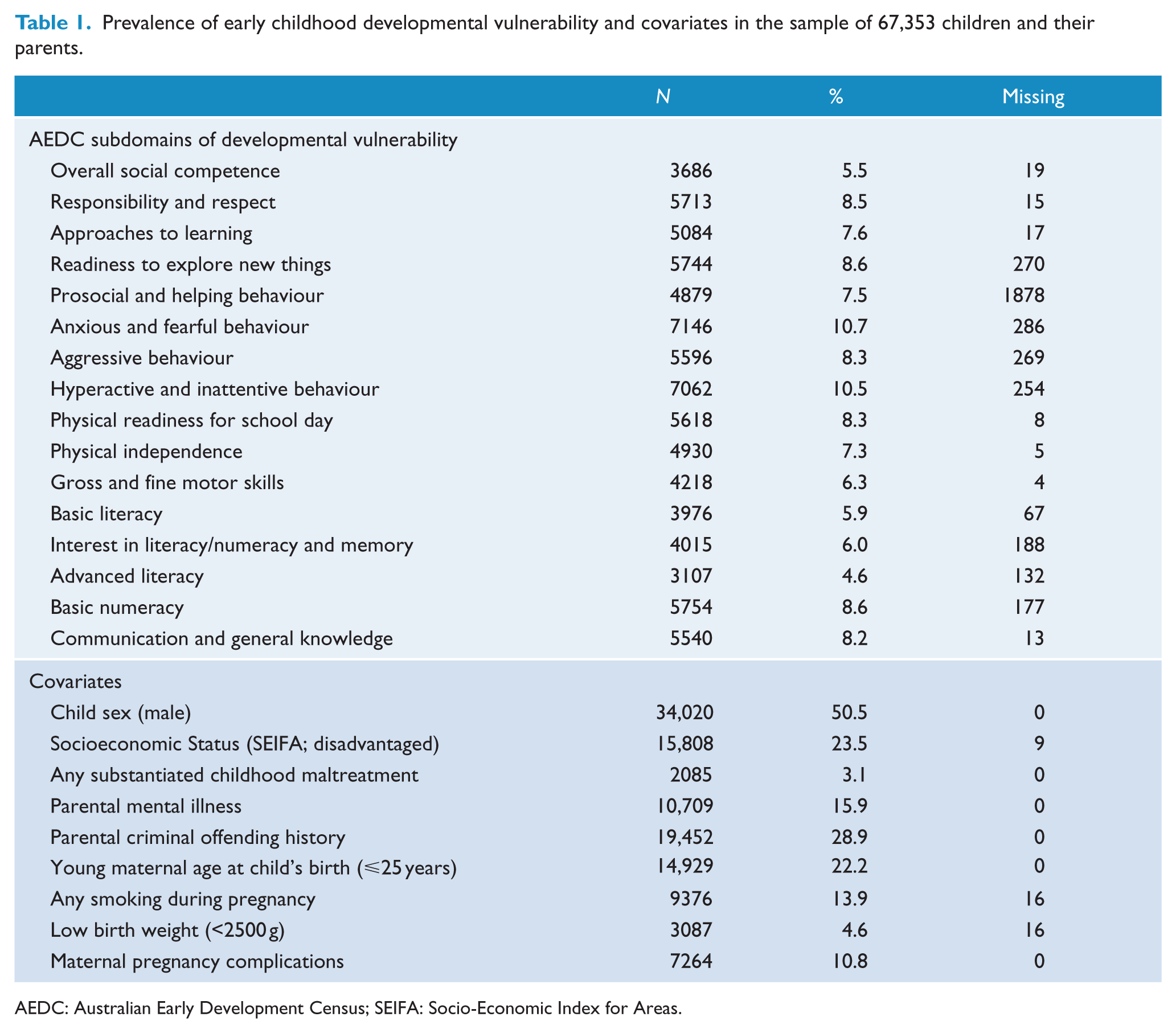
AEDC: Australian Early Development Census; SEIFA: Socio-Economic Index for Areas.
Examples of items comprising the 16 subdomains (within five broad domains) of the AEDC (child developmental vulnerability) indicators.
Demographic indicators
Indicators for the children’s sex and socioeconomic status were obtained from the AEDC data collection. A binary indicator of socioeconomic disadvantage was computed based on the Socio-Economic Index for Areas (SEIFA; Pink, 2013) by recoding the national quintiles into those most disadvantaged (i.e. lowest quintile) and the least disadvantaged (four remaining quintiles). Approximately half of the sample was male (50.5%) and less than a quarter were considered to be socioeconomically disadvantaged (23.5%).
Child maltreatment
A binary indicator of child maltreatment (spanning the years 2000–2009) was created using data from the Department of Family and Community Services (FACS) Case Management System – Key Information Directory System (KIDS). Children with substantiated records of childhood maltreatment were considered exposed to maltreatment (3.1%, Table 1). This represents instances of actual harm, or risk of significant harm, that were substantiated by child protections case-workers during safety and risk assessments. A number of maltreatment types were recorded for individuals represented in FACS records. Of the 2085 children exposed to maltreatment, 60.1% (n = 1253) had been first reported for maltreatment before age 3 years (0–18 months: 34.5%; 19–36 months: 25.6%), and 77.9% (n = 1625) had been exposed to a single maltreatment type, while 22.1% (n = 460) were exposed to more than one type of maltreatment. For those exposed to a single maltreatment type, emotional abuse was the most frequently reported (n = 762; 46.9%), followed by neglect (n = 425; 26.2%), physical abuse (n = 260; 16%) and sexual abuse (n = 178; 11%). Among those experiencing multiple types of maltreatment, the combination of emotional abuse and neglect was most common (n = 182; 39.6%), followed by physical and emotional abuse (n = 87; 18.9%), physical abuse and neglect (n = 52; 11.3%), emotional and sexual abuse (n = 42; 9.1%), physical and sexual abuse (n = 14; 3.0%), sexual abuse and neglect (n = 11; 2.4%) or the combination of sexual, physical and emotional abuse (n = 8; 1.7%); less than 1% of children (n = 4) experienced all four types of maltreatment.
Parental mental illness
Parental history of mental illness was determined using International Classification of Disease (ICD-10) codes representing any type of psychiatric disorder recorded in the NSW Ministry of Health Mental Health Admitted Patients (APDC, that is, public and private hospitals) and Mental Health Ambulatory (MHAMB, that is, public only ambulatory services) records that were obtained for parents of the child cohort for the period of 2001–2009 (i.e. approximately 3 years prior to the child’s birth up to age 5 years). Using methods for longitudinal coding of mental health diagnoses developed previously by our group (Sara et al., 2014), we computed a binary indicator of any parental mental disorder (15.9%; Table 1). We noted that 54.2% of parents with a history of mental illness also had a history of criminal offending.
Parental offending
Parental criminal offending histories were obtained from the NSW Bureau of Crime Statistics and Research court appearance data from 1994 until 2009 and included information on criminal court appearances for charges before the Local, District, Supreme and Children’s Criminal Courts. A binary indicator was created to reflect the appearance in court for any type of criminal offence (28.9%; Table 1). We noted that 29.8% of parents with offending histories also had a history of mental illness.
Perinatal risk factors
Four perinatal risk factors to be investigated as covariates included binary indicators of young maternal age at the child’s birth (⩽25 years), derived from Australian Bureau of Statistics’ Registry of Births, Deaths, and Marriages (RDBM), and prenatal smoking exposure (coded ‘yes/no’), maternal pregnancy complications (coded ‘yes/no’, and including any history of maternal diabetes, gestational diabetes, hypertension and pre-eclampsia) and low birth weight (<2500 g), derived from the NSW Ministry of Health’s Perinatal Data Collection (PDC).
Statistical analyses
LCA was used to determine subtypes of individuals that show similar patterns of vulnerability characteristics on AEDC subdomains (Collins and Lanza, 2010). LCA was conducted in SAS® 9.4 with the PROC LCA macro (Lanza et al., 2007; SAS, 2015). A baseline model was identified determining the number of classes of children based on the 16 AEDC subdomains of developmental vulnerability. Class membership probabilities (γ) were identified for the children, as well as the associated item-response probabilities (ρ) on the vulnerability indicators. To describe characteristics of the emerging classes, covariates were included in the LCA to predict class membership (incorporating multinomial logistic regression [MLR]). This step was conducted first for each covariate separately (i.e. unadjusted effects), and then a series of hierarchical models started with the demographic indicators (i.e. sex and socioeconomic disadvantage) and child maltreatment (Model 1), followed by the addition of parental history of mental illness (Model 2), parental history of criminal offending (Model 3) and perinatal risk factors (Model 4).
Results
LCA baseline model identification
LCA models with one through six latent classes were computed to identify the optimal number of latent classes of child vulnerability on the basis of fit statistics. The G2 statistic, the Akaike information criterion (AIC), the Bayesian information criterion (BIC), the adjusted Bayesian information (aBIC) and entropy values were all examined in determining the baseline model. Model fit statistics are presented in Table 3, and their decreasing values suggested an improved model as the number of classes increased, up to a four-class model; models with five and six classes did not differ substantively from the four-class solution other than identifying additional small classes (2–4% of the sample) which were not meaningful. Therefore, the four-class model was selected on principles of parsimony and interpretability. Average posterior probabilities of class membership were examined for the four-class model to assess classification accuracy. Across the four classes, the mean probability of being assigned to the correct class was high (0.82–0.96), and the mean probability of being assigned incorrectly was low (0.00–0.10; see Table 4).
Model fit statistics for identifying the latent class baseline model (N = 67,353).
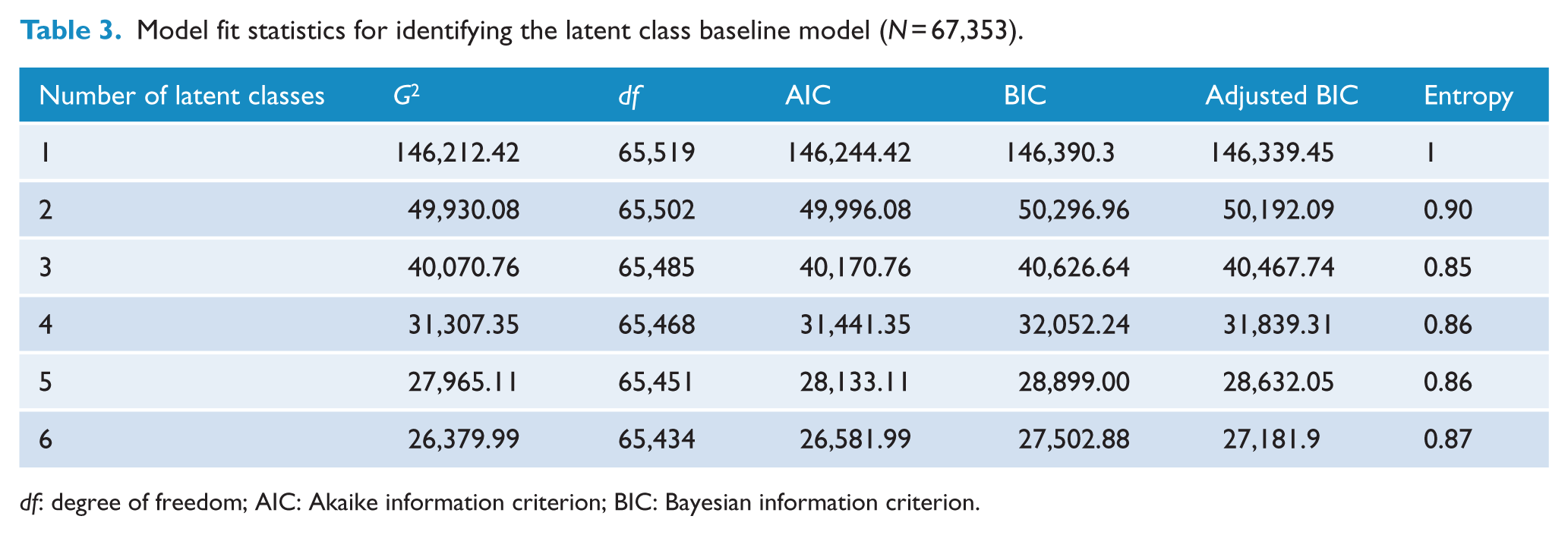
df: degree of freedom; AIC: Akaike information criterion; BIC: Bayesian information criterion.
Mean posterior probabilities and item-response probabilities for the four-class model of children’s developmental vulnerability.
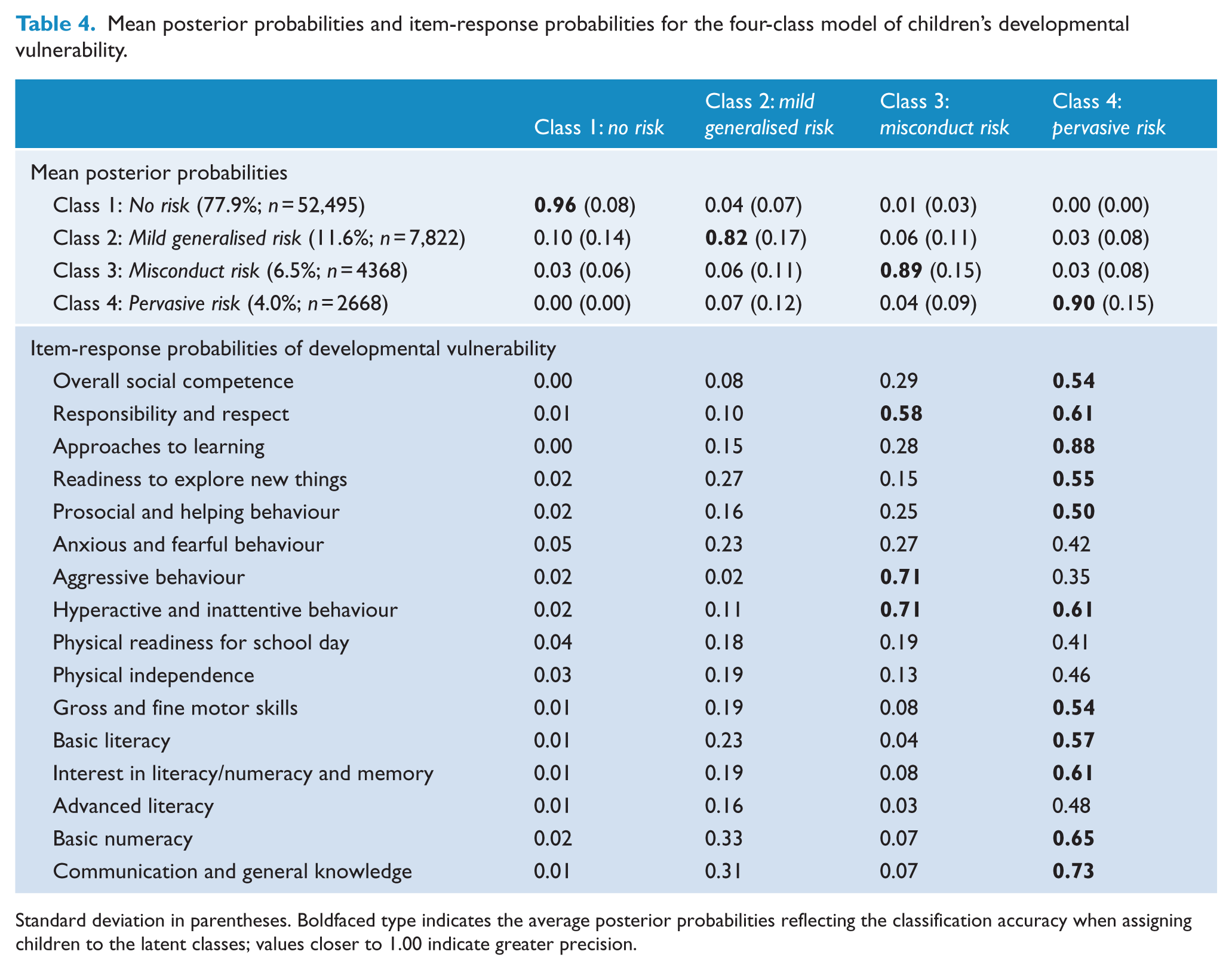
Standard deviation in parentheses. Boldfaced type indicates the average posterior probabilities reflecting the classification accuracy when assigning children to the latent classes; values closer to 1.00 indicate greater precision.
The four-class solution is presented in Figure 1 (see Table 4 for the item-response probabilities associated with vulnerability on each of the 16 AEDC subdomains). The largest class identified comprised 77.9% of the cohort (n = 52,495) and was labelled ‘no risk’ since there was a close to zero probability of being vulnerable on any of the 16 indicators (ρ range: 0.00–0.04). The second largest class identified was called ‘mild generalised risk’ and comprised 11.6% of the cohort (n = 7822) with modestly increased probabilities of early childhood developmental vulnerability across nearly all 16 subdomain indicators (ρ range: 0.02–0.33), other than the ‘aggressive behaviour’ domain. The third class, termed ‘misconduct risk’, comprised 6.5% of the cohort (n = 4368) and showed high probabilities of being vulnerable on the indicators of responsibility and respect (ρ = 0.58, standard error [SE] = 0.01), aggressive behaviour (ρ = 0.71, SE = 0.01) and hyperactive and inattentive behaviour (ρ = 0.71, SE = 0.01), with low probabilities of vulnerability on the physical health, language, cognitive and communication indicators (ρ ranging from 0.03 to 0.29). The fourth and smallest class comprised 4.0% of the cohort (n = 2668) and showed a pattern we described as ‘pervasive risk’. In this class, the probability of being developmentally vulnerable was greater than 0.50 for 11 of the 16 indicators, and the indicators with the highest probabilities of vulnerability were approaches to learning (ρ = 0.88, SE = 0.01) and communication and general knowledge (ρ = 0.73, SE = 0.01).
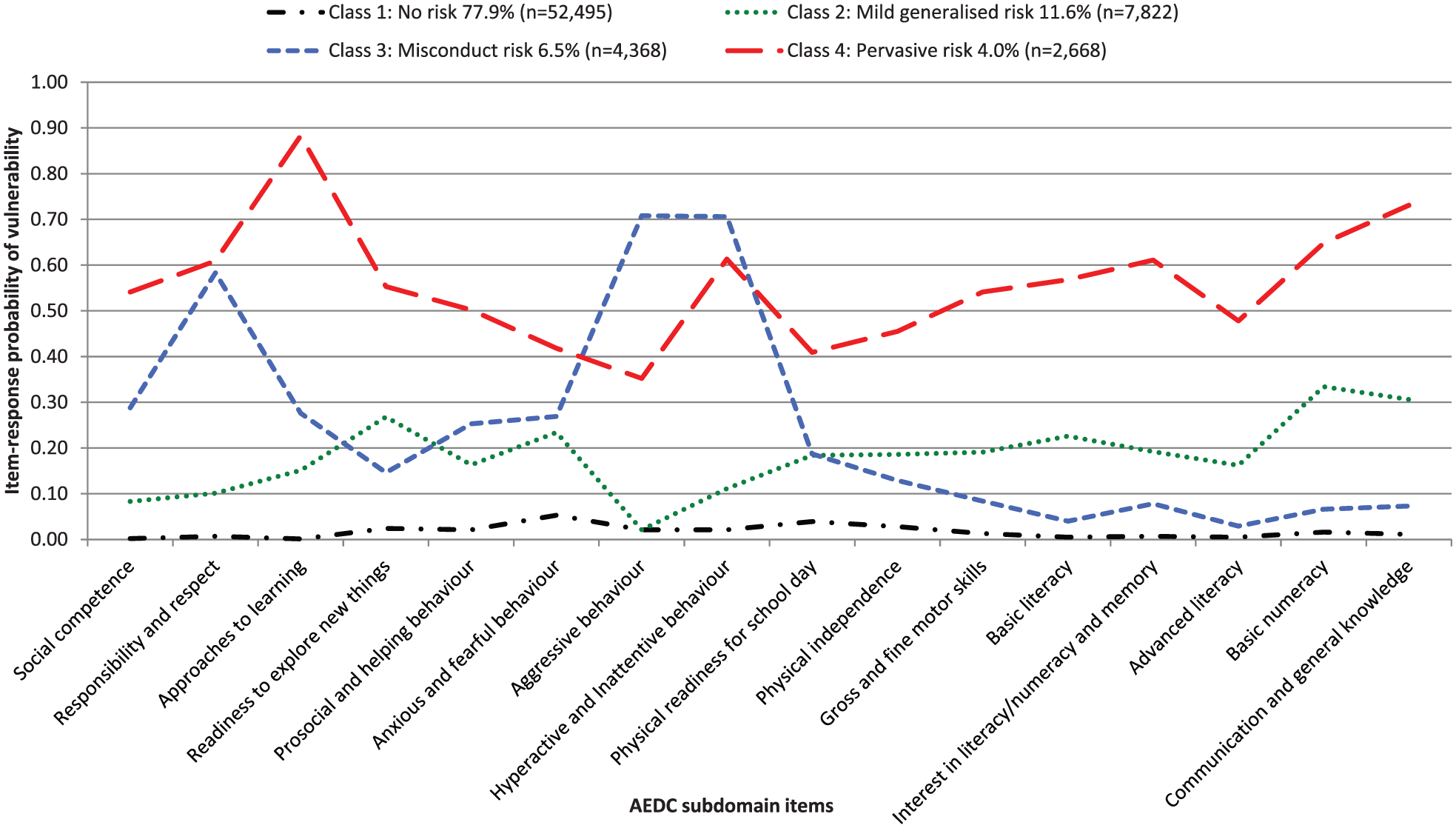
Four latent classes of children (N = 67,353) emerging from latent class analyses of 16 AEDC subdomains.
The Missing Completely At Random (MCAR) test for the four-class model was not significant (G2 = 6199.85, degree of freedom [df] = 900,567) suggesting that the missing data were a random set of all observations. Missing data for AEDC indicators were imputed automatically within the PROC LCA macro using a full-information maximum likelihood technique that assumes that data are missing at random (MAR); even when the MAR assumption is not met, this missing data procedure performs better than case-wise deletion.
Characteristics of the latent classes
We first present the unadjusted associations for all covariates investigated to characterise the latent classes (Table 5), using a series of MLRs with no risk (Class 1) as the reference class. All covariates were statistically significant at p <0.001. When covariates were examined independently, the strongest associations were revealed for child maltreatment: the odds of membership in any of the three classes (mild generalised, misconduct or pervasive risk) were three to six times higher for children exposed to maltreatment.
Latent class analysis with unadjusted covariate effects: odds ratios (95% confidence intervals).
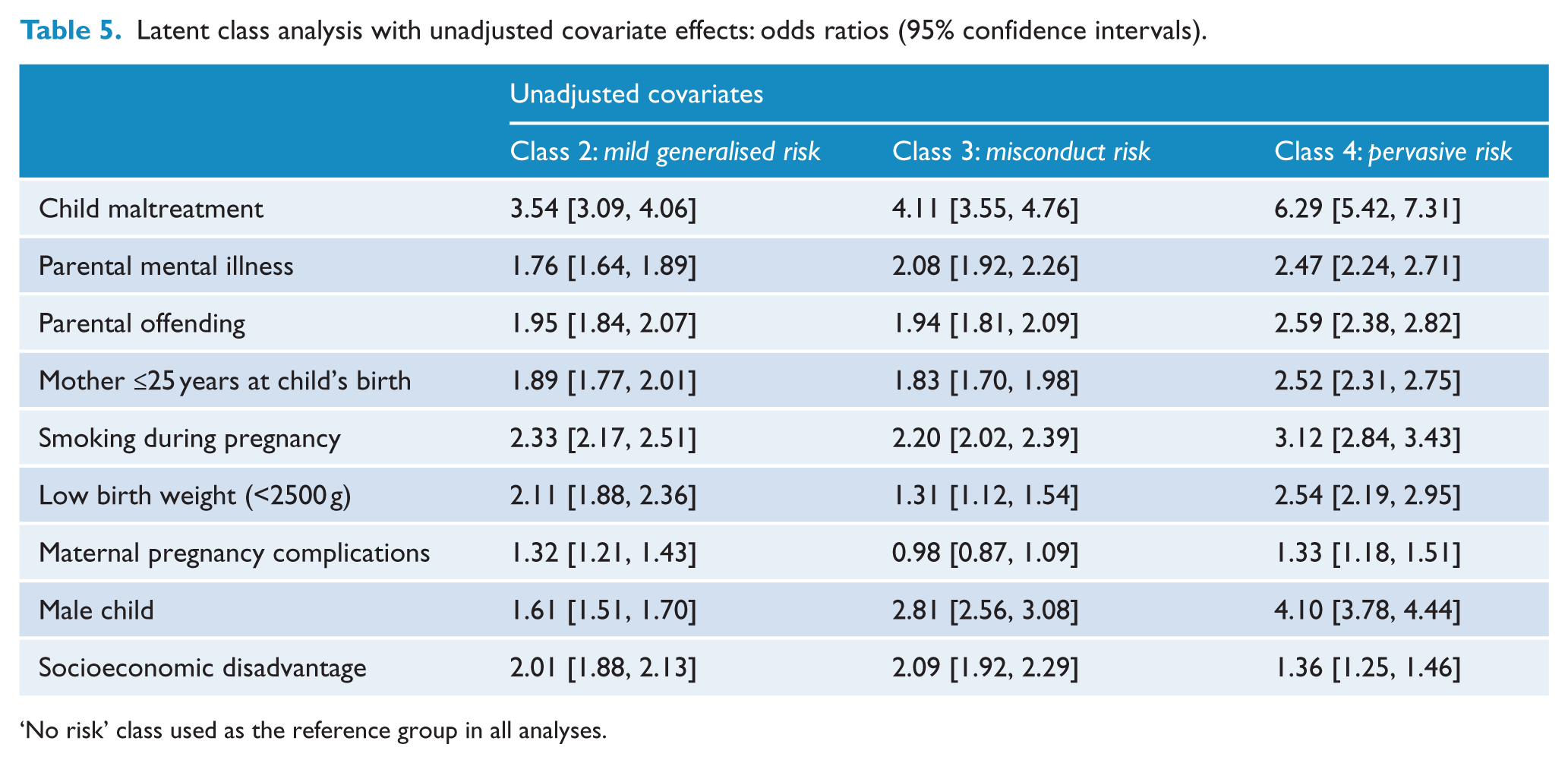
‘No risk’ class used as the reference group in all analyses.
The four MLR models that examined the covariates of interest together (in a step-wise, hierarchical fashion) are presented in Table 6, using no risk (Class 1) as the reference class. All covariates were statistically significant at p <0.001. In Model 1, child sex, socioeconomic disadvantage, and maltreatment were added as covariates to the LCA. Higher odds ratios (ORs) for male sex and exposure to maltreatment showed a pattern of increasing strength in association with mild generalised, misconduct and pervasive risk, while socioeconomic disadvantage did not follow this pattern and was weakest for the misconduct risk group. The odds of maltreatment were highest for the pervasive risk class (OR = 6.35; 95% CI = [5.45, 7.40]), followed by the misconduct risk class (OR = 4.43; 95% CI = [3.80, 5.15]) and then the mild generalised risk class (OR = 3.41; 95% CI = [2.97, 3.92]) compared to the no risk class. In Model 2, the addition of history of parental mental illness as a covariate reduced the magnitude of the ORs for child maltreatment (ranging from 2.74 for mild generalised risk to 4.48 for pervasive risk), while the ORs for sex and socioeconomic disadvantage remained stable; in this model, the ORs for parental mental illness were similar for the three risk classes (ranging from 1.52 for mild generalised risk, to 1.96 for pervasive risk). Parental history of offending was added in Model 3, which further reduced the ORs for child maltreatment and only slightly reduced the ORs for parental mental illness. The ORs for parental offending were relatively consistent across all risk classes (ranging from 1.64 to 2.01), though slightly higher for pervasive risk (OR = 2.01; 95% CI = [1.84, 2.20]). Finally, in Model 4, perinatal risk factors were added, reducing again the ORs for child maltreatment but leaving stable the pattern of increasing magnitude across the latent classes (mild generalised risk < misconduct risk < pervasive risk) for parental mental illness and parental offending. Of the perinatal risk factors, the strongest association was for low birth weight, increasing the odds of membership in the pervasive risk class (OR = 2.13; 95% CI = [1.83, 2.49]), while weak to moderate effects of young maternal age (ORs ranging from 1.42 to 1.73) and maternal smoking during pregnancy (ORs ranging from 1.55 to 1.81) were relatively consistent for all risk classes.
Latent class analysis with covariates: odds ratios (95% confidence intervals).
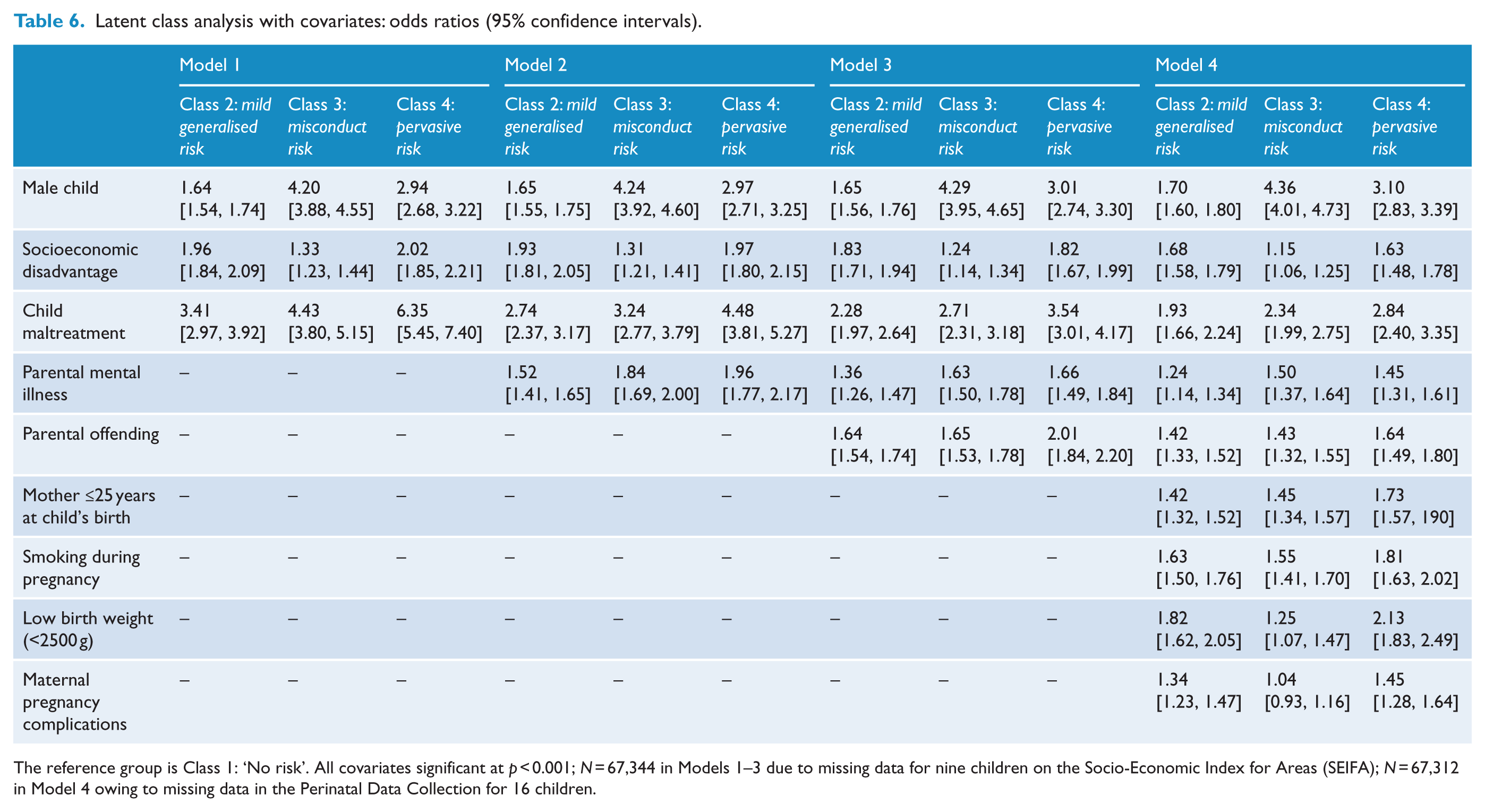
The reference group is Class 1: ‘No risk’. All covariates significant at p < 0.001; N = 67,344 in Models 1–3 due to missing data for nine children on the Socio-Economic Index for Areas (SEIFA); N = 67,312 in Model 4 owing to missing data in the Perinatal Data Collection for 16 children.
Discussion
In a large, nationally representative sample of 67,353 Australian children, we revealed four naturally occurring classes based on AEDC-defined early childhood developmental vulnerabilities at the time of school entry, which may represent putative risk states for subsequent mental disorders (Figure 1). These were termed pervasive, misconduct and mild generalised risk classes, which contrasted with a much larger no risk class (78%) having virtually no severe developmental vulnerabilities at age 5 years. The proportion of children represented in the two highest risk classes (i.e. approximately 10% of children represented in either the misconduct or pervasive risk classes) is comparable with a recent estimate of risk for adult mental disorders in 10,640 Australian children from the LSAC, in which approximately 10% of children were exposed to at least five risk factors by age 5 years (Guy et al., 2016). The estimated 12-month prevalence of mental disorders (13.9% of children age 4–17 years) in the 2013–2014 Australian national survey of mental health and well-being in children and adolescents (Lawrence et al., 2016) is also comparable to the proportion of the child population in this study showing putative risk for mental disorder, although we do not imply that children identified within these developmental risk classes are actually mentally ill. Longitudinal follow-up of these putative risk profile groups will be required to ascertain their utility in this regard.
The four classes revealed here using LCA methods appear robust according to fit statistics and are consistent with those established in the Dutch Generation R cohort (Basten et al., 2013; Davis et al., 2015), which has been followed up over time to reveal both homotypic and heterotypic outcomes in later childhood and adulthood (Basten et al., 2016). Consistent with these studies, we found a class with uniform spread of modestly increased probabilities of vulnerability across all AEDC subdomains (the mild generalised risk group), as well as a large majority class of children with virtually no AEDC-defined vulnerabilities at this age. Our group with misconduct risk was characterised by externalising vulnerabilities (i.e. responsibility and respect, aggression, hyperactivity and inattention) that would be conspicuous in the classroom as potential challenges to discipline and may suggest likelihood of externalising disorders. However, this class did not show peaks on literacy and numeracy vulnerabilities, suggesting that cognitive functioning is spared (and making attention-deficit/hyperactivity disorder [ADHD] less likely). This class of children present some similarities to those referred to as having ‘dysregulation syndrome’ in the Dutch longitudinal studies, in which males are more highly represented, but in this study the misconduct risk group did not show overt emotional (internalising) vulnerabilities that are characteristic of the CBCL-based dysregulation classes (Basten et al., 2013; Davis et al., 2015). We note that internalising (anxious/fearful) vulnerabilities do not feature especially in any of the vulnerability classes revealed at this age and speculate that internalising vulnerabilities may be less conspicuous in the classroom and potentially under-rated by teachers (particularly among boys) and/or that these internalising symptoms may emerge in later years of development in children whose vulnerabilities persist over time. Finally, while pervasive risk encompassed all domains assessed with the AEDC, the strength of probability on some vulnerability indicators was weaker than those for other classes. The widespread nature and magnitude of vulnerabilities in the pervasive risk class suggest possible global neurodevelopmental dysfunction that may be associated with learning difficulties and impaired cognitive functioning. This remains speculative, since none of the classes emerging from the LCA showed isolated cognitive vulnerability that might be expected to be associated with neurodevelopmental disorders (such as specific learning disorders); it is possible that other classes of this nature may have emerged if the children with ‘special needs’ were retained in the sample. However, the value of including language and cognitive vulnerabilities in our model provides a unique addition to the internalising and externalising variables typically used in the derivation of childhood risk profiles from clinical information, since early life cognitive difficulties may be important precursors to the development of mental illness in later life.
There was a strikingly high association between child maltreatment (medium to large effect sizes) and membership of all three classes of early childhood risk, especially pervasive risk. Even when taking sex and socioeconomic disadvantage into account, the children in the pervasive risk class were over six times more likely than the no risk class to be exposed to maltreatment, and children in the misconduct risk class were over four times more likely to have been exposed to maltreatment. While these odds of class membership in association with maltreatment were somewhat reduced with the inclusion of other familial risk factors that likely share variance with maltreatment exposure (e.g. parental mental illness, parental offending), this exposure remained the strongest among all covariates, with the most significant reduction in associations between child maltreatment and probability of membership in any risk class occurring when perinatal factors were included in the models. This pattern of findings accords with known associations between child maltreatment and developmental dysfunction in multiple developmental domains (Cheatham et al., 2010; Eigsti and Cicchetti, 2004; Font and Berger, 2015; Toth et al., 2011). Cross-agency communication of child maltreatment may thus be important for enabling appropriate school-based, community or health service interventions to prevent developmental lags and later potential consequences of membership in such risk classes.
By comparison, the strength of associations of parental mental illness and parental criminal offending with putative risk classes was relatively small after child’s sex, socioeconomic status and child maltreatment were taken into account. These parental factors may be relevant in enabling broadly applicable interventions to be delivered by government agencies with this knowledge (e.g. child protection and health services). While there was a general lack of specificity in risk class associations with these parental factors, more distinct patterns of familial risk may differentiate particular risk profiles with the use of more detailed exposure estimates (e.g. for particular parental mental illness [e.g. schizophrenia] and/or specific types of offending [e.g. violent offending]), or when examined in the context of the emergence of persistent childhood mental health problems in later childhood and adolescence (Moffitt, 1993, 2007). Use of the CBCL to assess early psychopathology that may predict later adult mental health outcomes, as used in other longitudinal studies of fundamentally different (interview-based) methodology (Basten et al., 2016), may also provide more precise indices of later mental health risk that align more strongly with the familial and other risk factors examined here.
These emerging developmental profiles at age 5 years provide complementary information about early childhood developmental risk to that which is currently provided by the AEDC classifications of ‘vulnerability’, ‘at-risk’ and ‘on-track’ and should not be conflated or confused with those classifications. The prevalence of the putative risk classes for mental disorders found here is consistent with recent Australian population-based estimates using a combination of person-centred indices and other familial factors and childhood antecedents as assessed in the LSAC (Guy et al., 2016). Notably, the risk factors identified by Guy et al. largely overlap with adversity or disadvantage in Australian families (Gubhaju et al., 2013). This is consistent with our findings of small but stable associations between socioeconomic disadvantage and putative risk classes. Moreover, the associations with male sex detected here, which were robust across all four covariate models, are consistent with the higher rates of conduct disorders and neurodevelopmental dysfunction found among males of this age group (Lawrence et al., 2016), and with greater levels of early childhood vulnerability seen in males across the five broad domains of the AEDC in other national studies (Brinkman et al., 2014). The pervasive risk class, comprising 4% of the cohort, appears prima facie to be at greatest risk of long-term adverse mental health and social outcomes (e.g. education incompletion, unemployment) with features suggesting neurodevelopmental dysfunction (cognitive vulnerability) alongside social and emotional vulnerabilities. However, adverse outcomes may not be inevitable in any of these classes: some children may naturally develop resources to recover capacity during later years of childhood, while for others targeted interventions may assist them in catching up with their peers.
The significance of these findings is in providing a framework for the early detection of putative profiles of risk for later mental disorders that could be addressed early in life to prevent a cascade of neurodevelopmental processes leading to poor mental health and potentially other adverse outcomes in later life (e.g. criminal behaviour, poor educational and/or occupational achievement). The contribution of key perinatal indicators, familial mental health and offending characteristics and child maltreatment to these risk profiles at age 5 years suggests that cross-agency indicators (i.e. routine data collected by multiple government departments) could be used to flag the need for increased health and community services for high-risk families during the prenatal period and in the earliest years after child birth. Prospective longitudinal studies suggest that up to half of all adult psychiatric conditions could be averted with effective treatment provided to children with emerging psychopathology (Kim-Cohen et al., 2003). Notably, the widest range of adult cases (up to 25–50%; Copeland et al., 2009; Kim-Cohen et al., 2003) are preceded by child conduct and oppositional behavioural disorders, such that the group of children identified here as the misconduct risk class may be displaying a diagnostically non-specific signal indicating risk of developing a number of mental disorders that may emerge in adolescence and/or adulthood. Longitudinal study of these children will determine the predictive utility of these putative risk classes.
Advantages of the retrospective analysis of prospectively convened data via record linkage, as used here, include the avoidance of recall and minimisation of sampling biases and the capacity to consider exposures and outcomes in a temporal context within discrete developmental periods. The Australian Government has recently made significant investments to facilitate the coordinated linkage of State and Commonwealth data such that the longitudinal analysis of population records from multi-agency sources can now be harnessed to achieve national priority health goals. However, a number of limitations should also be considered with the use of such methods. First, these administrative data were not collected for research purposes; potential errors in data entry or quality are therefore possible. Second, linked parental data were unavailable for some children in the NSW population who were assessed with the AEDC; these children were not born in NSW to enable linkage of parental data, but the representativeness of the subcohort with linked parental data has been established elsewhere (Carr et al., 2016). Third, the maltreatment cohort in this study was restricted to children with substantiated harm or risk of significant harm that had been determined during a face-to-face child protection assessment. While this leaves open the possibility that some children categorised as ‘non-exposed’ were subject to maltreatment that was not substantiated by child protection workers, this possibility would tend to reduce rather than inflate associations between child maltreatment exposure and membership in particular risk classes. Finally, we did not examine the associations of early childhood physical illness with age 5 years risk classes, despite evidence for the negative effects of chronic illness on AEDC vulnerabilities (Bell et al., 2016).
In conclusion, we have identified putative risk classes for later mental disorders in a large (general population) cohort of Australian children, using data from the AEDC assessment that is currently administered triennially in all Australian schools. These observable patterns of developmental vulnerability on this population measure define classes of children who may be at risk of later mental disorder and are associated most strongly with substantiated child maltreatment before the age of 5 years, as well as with perinatal and parental risk factors. The capacity to distinguish a misconduct risk from a more pervasive risk class, the former not including prominent social and cognitive problems, suggests that it may be prudent to discern the existence of social or cognitive difficulties among children referred to clinicians for behavioural problems at an early age and to take these into consideration in choosing a suitable intervention. More broadly, the universal delivery of school-based interventions to promote prosocial behaviour and emotion regulation competencies may be useful in preventing or mitigating a variety of adverse mental health or other outcomes in later life to which the children in the risk classes might be susceptible. Follow-up of the cohort will address this question.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
This research was conducted by the University of New South Wales with financial support from the Australian Research Council (Linkage Project LP110100150, with the NSW Ministry of Health, NSW Department of Education and the NSW Department of Family and Community Services representing the Linkage Project Partners); the National Health and Medical Research Council (NHMRC Project Grant APP1058652); the Australian Rotary Health (Mental Health Research Grant 104090 and 162302) and the Australian Institute of Criminology (Research Grant CRG 19/14-15). K.R.L., M.K., F.H. and V.J.C. were supported by funding from the Schizophrenia Research Institute (Australia) using infrastructure funding from the NSW Ministry of Health; M.J.G. was supported by a NHMRC R.D. Wright Biomedical Career Development Fellowship (1061875). The research was conducted using population data owned by the Commonwealth Department of Education, the NSW Department of Family and Community Services, the NSW Ministry of Health and the NSW Registry of Births, Deaths and Marriages. The information and views contained in this study do not necessarily, or at all, reflect the views or information held by these Departments.