
Abstract
Objectives:
This study describes the development of a decision support tool to identify the combination of suicide prevention activities and service priorities likely to deliver the greatest reductions in suicidal behaviour in Western Sydney (Australia) over the period 2018–2028.
Methods:
A dynamic simulation model for the WentWest – Western Sydney Primary Health Network population-catchment was developed in partnership with primary health network stakeholders based on defined pathways to mental health care and suicidal behaviour, and which represented the current incidence of suicide and attempted suicide in Western Sydney. A series of scenarios relating to potential suicide prevention activities and service priorities identified by primary health network stakeholders were investigated to identify the combination of interventions associated with the largest reductions in the forecast number of attempted suicide and suicide cases for a 10-year follow-up period.
Results:
The largest number of cases averted for both suicide and attempted suicide was associated with (1) post-suicide attempt assertive aftercare (6.1% for both attempted suicide and suicide), (2) improved community support and reductions in psychological distress in the community (5.1% for attempted suicide and 14.8% for suicide), and (3) reductions in the proportion of those lost to services following a mental health service contact (10.5% for both attempted suicide and suicide). In combination, these interventions were forecast to avert approximately 29.7% of attempted suicides and 37.1% of suicides in the primary health network catchment over the 10-year period.
Conclusion:
This study demonstrates the utility of dynamic simulation models, co-designed with multi-disciplinary stakeholder groups, to capture and analyse complex mental health and suicide prevention regional planning problems. The model can be used by WentWest – Western Sydney Primary Health Network as a decision support tool to guide the commissioning of future service activity, and more efficiently frame the monitoring and evaluation of interventions as they are implemented in Western Sydney.
Introduction
Suicide remains a significant public health problem in Australia and is associated with significant social, economic and health system costs (Australian Bureau of Statistics, 2014; Mendoza and Rosenberg, 2010). Following the recommendations of the 2014 review by the National Mental Health Commission (2014), there has been an increased focus on regional implementation of suicide prevention programmes and a more systematic national approach to programme evaluation. This has led, in part, to a devolution of funding and responsibility for the commissioning of suicide prevention initiatives from the Commonwealth level to regional primary health networks (PHNs), with a view to provide local and context-specific interventions.
This presents challenges for local communities to identify the most appropriate combination of interventions and services to prevent suicidal behaviour, and implement these interventions with finite resources and capacity. Challenges include the complex aetiology of suicidal behaviour, the range of available evidence-based approaches for intervening (Krysinska et al., 2016; Zalsman et al., 2016), geographic variation and changes over time in service capacity and population needs and the timely monitoring of suicide and suicidal behaviour. There are also different perspectives on what interventions might prevent suicide, particularly in local populations, and the extent to which evidence from studies in other contexts is applicable to a different context, and whether this aligns with local capacity, priorities and available resources.
In addition, understanding the likely impacts of interventions over time in different contexts, and how they perform in combination, is also a challenge. Standard programme evaluation approaches often have long lead times and take years to evaluate, which is incongruent with the timelines and priorities of service providers and policy makers (Atkinson et al., 2015a; Page et al., 2017). In instances where multiple interventions have been implemented employing community-level or whole-population approaches (Black Dog Institute, 2016; Hegerl et al., 2008), it is also difficult to ascertain which components of the programme have the biggest impact, or the extent to which some activities are extraneous, or where resources could be better used.
One approach to making decisions around the most effective combination of suicide prevention activity for a population is to employ dynamic simulation models, co-designed and developed by key stakeholders (Atkinson et al., 2015b, 2017; Loyo et al., 2013; Rouwette et al., 2002). Dynamic simulation modelling provides a method for bringing together a variety of sources of evidence such as research, expert and local knowledge; practice experience; and data to map and quantify complex problems. The resulting model is an interactive ‘what-if’ tool that allows decision makers to test the likely impacts of counterfactual situations and different combinations of a range of interventions and service planning options before they are implemented in the real world. These tools can be used to inform where best to target investments for suicide prevention, and with what intensity, in order to optimise the impact of limited resources and develop more effective, locally tailored strategies for reducing suicidal behaviour.
Accordingly, this study describes the development and application of a dynamic simulation model that aimed to inform the most appropriate combination of suicide prevention activity in the population catchment covered by WentWest – Western Sydney PHN (Sydney, Australia). Specifically, the study aimed to (1) conceptualise a model of the Western Sydney population, with particular emphasis on pathways to mental health care and suicidal behaviour; (2) operationalise this model and calibrate outputs to represent current incidence of suicide and attempted suicide in Western Sydney; and (3) incorporate a range of potential suicide prevention activities and service priorities to identify the combination of services and activities associated with the greatest potential reductions in suicide over the period 2018–2028.
Methods
Context
WentWest PHN is responsible for delivery of programmes and primary care services for the geographic area covering the Local Government Areas of Blacktown, Parramatta, Cumberland and The Hills in the western suburbs of Sydney. This population catchment (N = ~971,000) is one of Australia’s fastest growing urban populations, and is characterised by a range of socio-economic circumstances, a range of ethnic and non-Australian born backgrounds, a range of social and health services (provided by both government and non-government sectors) and varying geography (urban, peri-urban and rural) (WentWest Primary Health Network, 2016). It has been estimated that 20% of the population have experienced a mental health issue in the last 12 months, of whom almost 15% were classified as severe (WentWest Primary Health Network, 2016). There is also an increasing trend in hospitalisations for mental disorder placing pressure on tertiary services in the population catchment (WentWest Primary Health Network, 2016).
The extent to which investments in current mental health and suicide prevention programmes and service capacity will contribute to reductions in suicidal behaviour in this population catchment is unknown, nor is it clear what additional interventions might be required. Thus, the purpose of the dynamic simulation model was to identify the combination of mental health programmes, services and specific suicide prevention interventions, that would potentially deliver the largest reductions in suicide and hospital attempted suicide in Western Sydney over the next 10 years (2018–2028).
Approach and model development
The model was developed in partnership with WentWest – Western Sydney PHN and in collaboration with local stakeholders (Supplementary Table 1). A participatory model building approach was undertaken, drawing iteratively on the deep tacit knowledge these stakeholders possess of the local context, issues and priorities, and which employed a broad systems perspective to draw this knowledge together. Participating stakeholders included representation from health and social policy agencies, local councils, non-government organisations, emergency services, primary care providers, programme planners, research institutions, community groups and those with lived experience of suicide. Oversight of model development was provided by a core team consisting of dynamic modellers and content experts.
Input from stakeholders was provided through a series of workshops and meetings between April and November 2017. The workshops mapped key suicide and mental health service pathways, the factors that influenced the flow of the population along these pathways, and the mechanisms by which selected interventions were hypothesised to have their effect. Findings from this mapping exercise were developed into a conceptual model (Supplementary Figure 1A) based on current policy priorities identified by the PHN, which included a ‘stepped care’ approach to the provision of mental health care in primary health settings (Cross and Hickie, 2017). The conceptualised model, incorporating research evidence and local secondary data sources, facilitated the construction, quantification, calibration and validation of the computational model (Supplementary Figure 1B) using standard approaches for system dynamics models (Andersen and Richardson, 1997; Bérard, 2010; Hovmand, 2014; Vennix et al., 1992; Voinov et al., 2016; Voinov and Gaddis, 2017). Additional detail describing the co-design and participatory simulation modelling process applied in this study has been more fully described elsewhere (Atkinson et al., 2017; Freebairn et al., 2016). The computational model was developed using Stella Architect® software (www.iseesystems.com/).
Model structure, inputs and outcome indicators
The model was defined to have an open population with births and migration contributing to the population, and deaths (from causes other than suicide) subtracting from the population. The model of the WentWest – Western Sydney PHN population-catchment captures (1) the pathway from vulnerability, to psychological distress and to mental disorder; (2) mental health service pathways, including assessment of care needs and delivery of low, moderate and high intensity services based on changing individual needs (Cross and Hickie, 2017); (3) pathways to suicidal behaviour (attempted suicide and suicide) either with, or without contact with mental health services; and (4) mental health recovery pathways with and without contact with mental health services (Supplementary Figure 1B).
The structure and parameterisation of the model drew on a range of data sources including population survey data, systematic reviews (and meta-analyses), administrative data and expert knowledge of the multidisciplinary stakeholders. This process has been described in detail elsewhere (Atkinson et al., 2017; Freebairn et al., 2016), and in the present study involved a series of stakeholder workshops to co-design the structure and key parameters of the model (Supplementary Table 2). Demographic data, psychological distress data, mental health hospitalisations, suicide attempts and completed suicides for Western Sydney were sourced from NSW Health administrative datasets (Centre for Epidemiology and Evidence, 2017). Prevalence of mental disorder and service capacity and use data were sourced from a WentWest – Western Sydney PHN needs assessment conducted in 2016 (WentWest Primary Health Network, 2016) and data from the Medicare Benefits Schedule (MBS) relating to mental health services in the WentWest – Western Sydney PHN population catchment. These data were used for model initialisation, calibration and validation purposes. In instances where data were not available, estimates were reached by consensus and the ability to test the impact of alternative values for those parameters provided in the model interface. Model assumptions and variable inputs are provided in supplementary material (Supplementary Box 1, Supplementary Table 3). The model was calibrated using historical and projected population data (2016–2030) for WentWest – Western Sydney PHN (Centre for Epidemiology and Evidence, 2017; WentWest Primary Health Network, 2016) and suicide attempts (based on hospital separations for self-harm) and completed suicide for the period (2001–2013) (Centre for Epidemiology and Evidence, 2017). Hospital-based suicide attempts were selected as these data could be readily accessed and represented an objective measure of non-fatal suicidal behaviour. However, this measure of suicide attempts is likely an under-enumeration of the total burden of non-fatal suicidal behaviour in the population catchment (excluding those cases that do not present to hospital services). The model projects the primary outcome indicators (hospital suicide attempts and suicide deaths) to 2030.
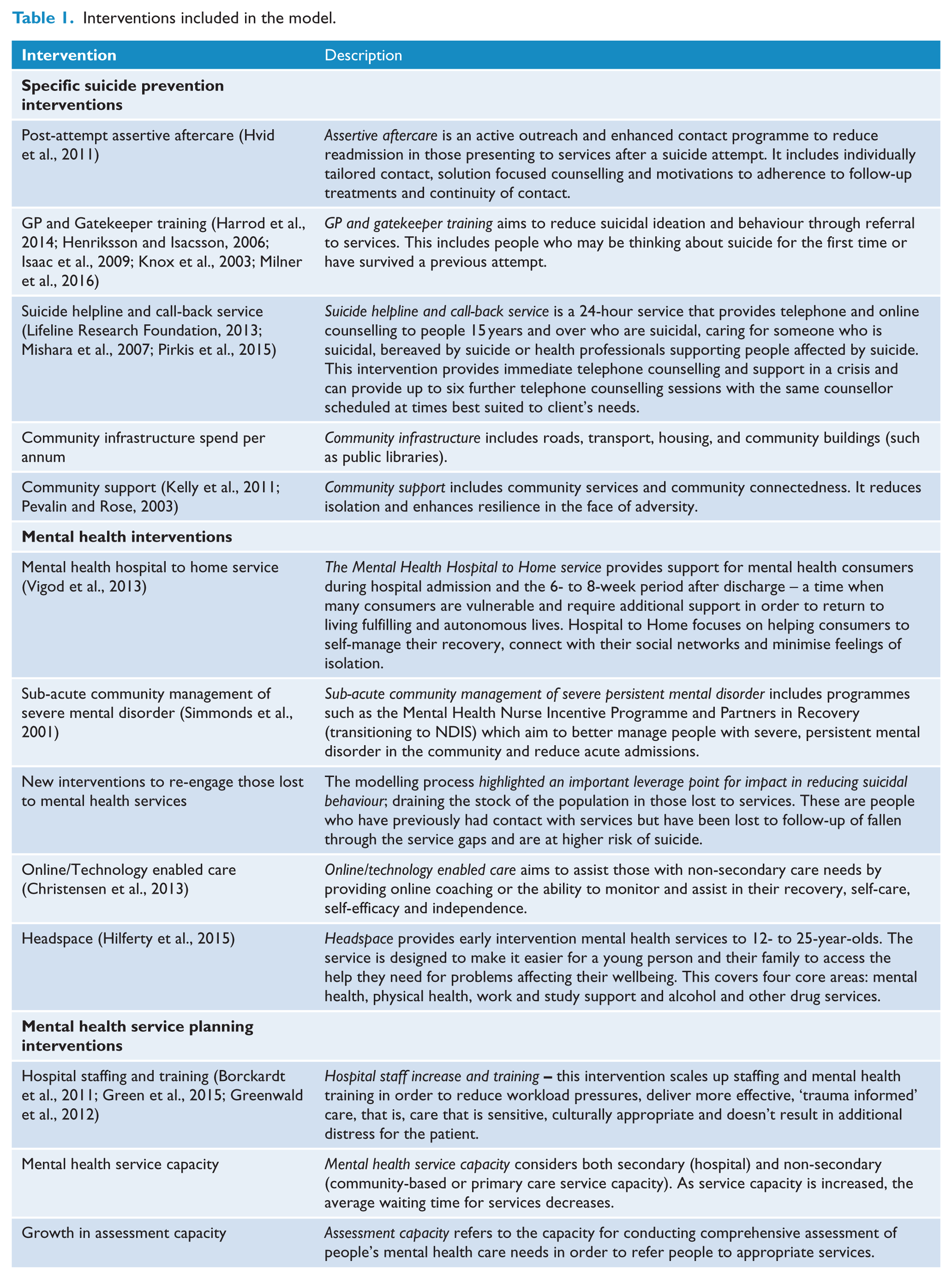
The model also incorporated a series of interventions identified by the WentWest – Western Sydney PHN stakeholder group for inclusion, relating to (1) specific suicide prevention interventions, (2) mental health interventions and (3) mental health service interventions (relating to capacity and infrastructure) (Table 1). Estimates of the effects of selected interventions, and the specific mechanism of action in the model, were based on evidence from the literature, and informed by stakeholder feedback for local application (Supplementary Table 2). A detailed exposition of how each intervention acts in the model is provided in Supplementary Table 3. Each of these interventions were incorporated at specific points in the model to modify pathway flows (demonstrated graphically in Supplementary Figure 1B). The final model can be used as an interactive ‘what-if’ tool (Figure 1) to test the likely impacts of counterfactual situations and different combinations of the range of interventions and service planning options to maximise reductions in attempted suicide and suicide in Western Sydney over a 10-year period.
Interventions included in the model.
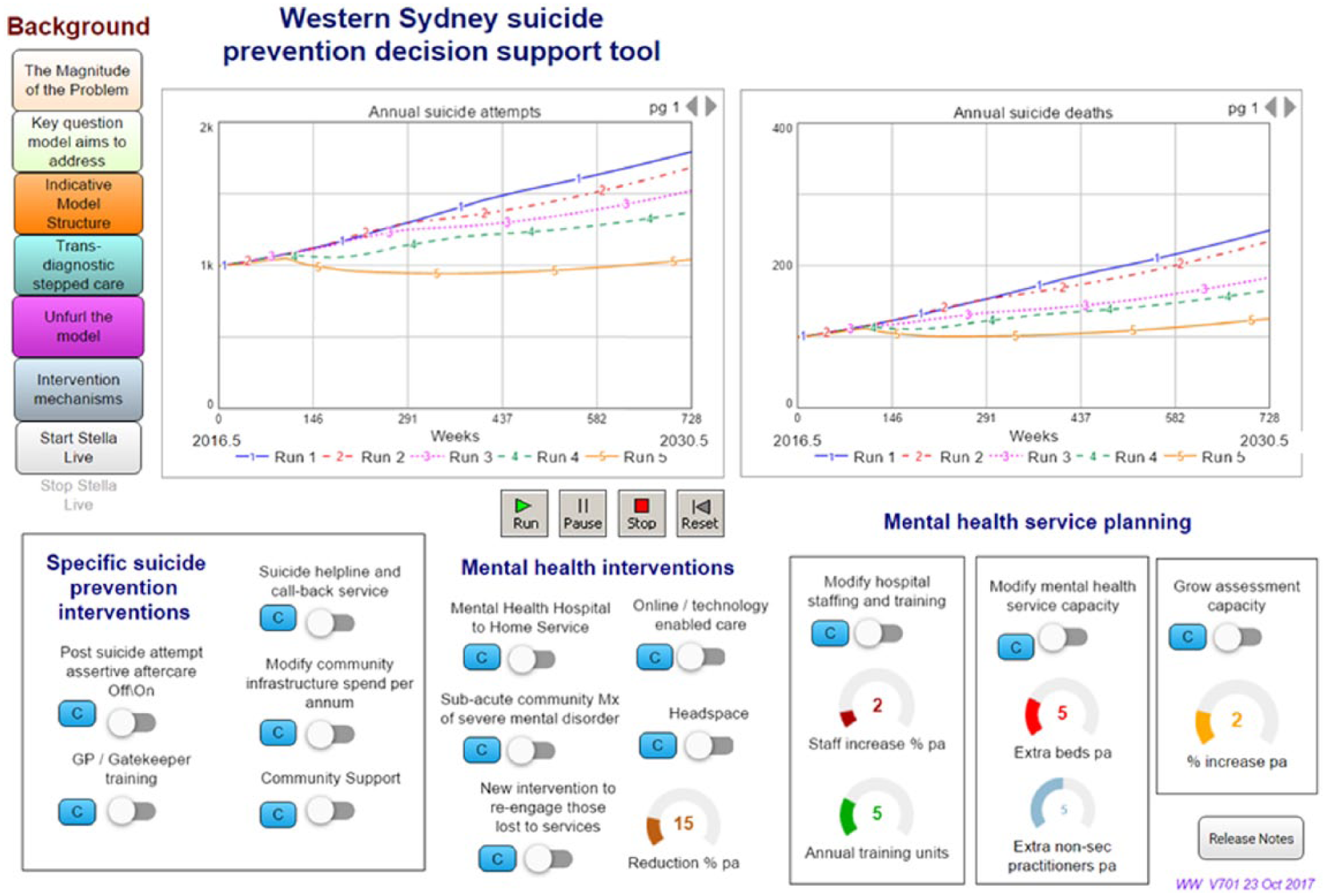
Interactive model interface displaying the impact of different intervention scenarios against a baseline of business as usual.
Modelling the impact of interventions
A series of scenarios were modelled to identify the combinations of interventions associated with the largest forecast reductions in attempted suicide and suicide in the WentWest – Western Sydney PHN population catchment over a 10-year period (2018–2028). First, the impact over time of each intervention was assessed individually, with default assumptions as specified by stakeholders (Supplementary Table 3). The optimal combination to avert the largest forecast number of attempted suicides and suicides was then simulated for (1) specific suicide prevention interventions, (2) mental health programmes and services and (3) mental health service capacity and infrastructure. A final scenario considered the combination of interventions associated with the largest reductions in suicide and attempted suicide across all three intervention types.
Sensitivity analysis was also conducted to estimate the potential variability around the forecast estimates of suicide and attempted suicide in each scenario. Due to the large number of parameters in the model, exhaustive analysis combining every variable in the model with estimated ranges of values was not feasible. Accordingly, in the current model, two key variables were identified as having the most uncertain baseline assumptions and the greatest likely impact on the outcome of interest, and were the focus of sensitivity analyses: (1) the proportion of the population that become vulnerable each year (default value 2%; estimated variation of 1–5%; step-change for each run of 0.5%) and (2) the initial value of non-secondary mental health service staff (default value 100 practitioners, estimated variation of 90–110 practitioners step-change for each run of 2 practitioners). Comparison of simulation results between baseline and intervention scenarios were presented as the mean number of cases averted across 100 model runs, and the absolute difference in mean number of cases with the associated margin of error.
Results
There were three main points in the model where identified interventions had the largest potential impacts on the number of cases averted for attempted suicide and suicide over the 10-year forecast period (2018–2028) (Table 2; Figure 2). The largest number of cases averted for both suicide and attempted suicide was associated with (1) post-suicide attempt assertive aftercare (6.1% for attempted suicide and suicide), (2) improving community support and reducing psychological distress in the community (5.1% for attempted suicide and 14.8% for suicide) and (3) reducing the proportion of those lost to services following a mental health service contact (10.5% for both attempted suicide and suicide).
Summary of estimated reductions in suicide and attempted suicide in Western Sydney for selected interventions (10-year forecast period; 2018–2028).
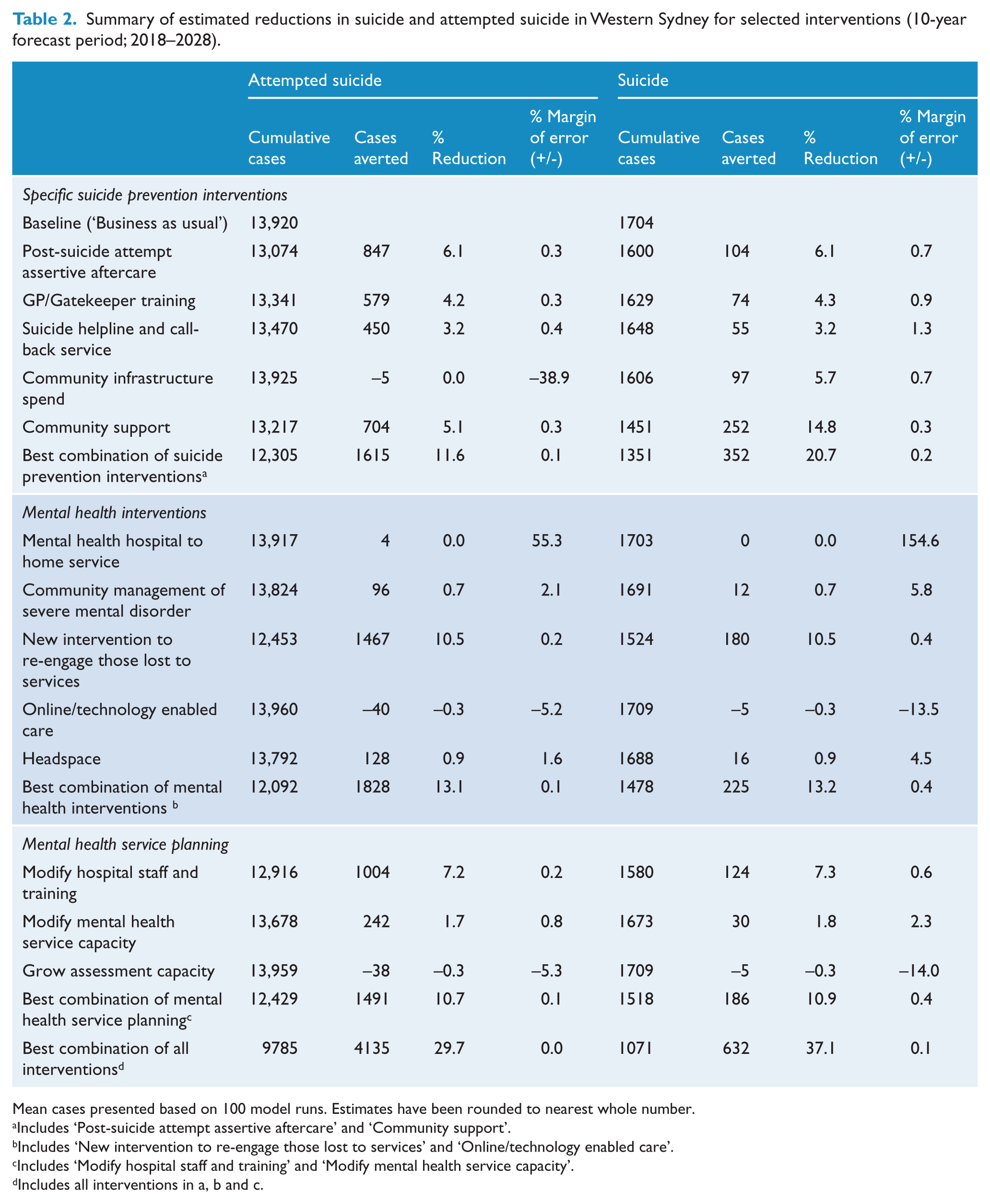
Mean cases presented based on 100 model runs. Estimates have been rounded to nearest whole number.
Includes ‘Post-suicide attempt assertive aftercare’ and ‘Community support’.
Includes ‘New intervention to re-engage those lost to services’ and ‘Online/technology enabled care’.
Includes ‘Modify hospital staff and training’ and ‘Modify mental health service capacity’.
Includes all interventions in a, b and c.
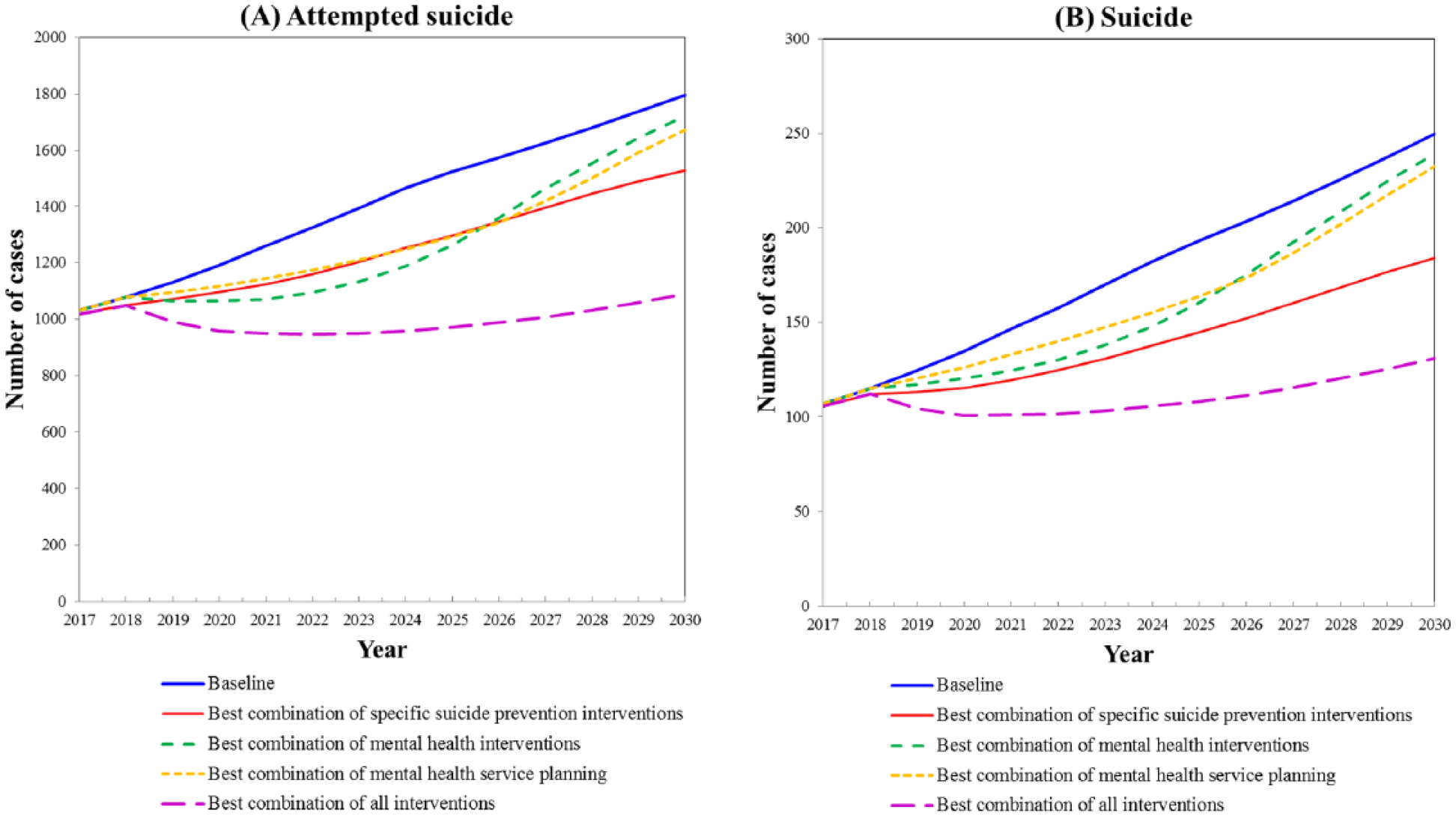
Optimal modelled combinations of suicide prevention and mental health service capacity interventions. (A) Attempted suicide (B) Suicide.*
Infrastructure and workforce capacity interventions were also associated with a significant number of cases averted over the forecast period (Table 2). Increased spending on community infrastructure (relating to improved access to services, employment, transport and housing) was estimated to result in a 5.7% reduction in suicide cases; however, this had limited impact on attempted suicide cases. Also, increased staff (approximately 2% per annum) and training relating to trauma-informed care was also estimated to avert approximately 7% of attempted suicide and suicide cases (Table 2).
Interventions relating to post-suicide attempt assertive aftercare, reducing psychological distress in the community, and re-engaging those lost to follow-up from mental health service, when combined with increased staff, staff training and community infrastructure, resulted in the largest potential number of cases of attempted suicide and suicide averted over the follow-up period (29.7% and 37.1%, respectively) (Table 2; Figure 2).
Interventions to identify those at risk of suicidal behaviour (GP/gatekeeper training; Headspace) had limited impact on averting cases of attempted suicide or suicide cases over the forecast period (Table 2), unless combined with a commensurate increase in capacity in mental health service pathways (including increased capacity for assessment and staff training) (not shown). This finding reflected a need for mental health services to have the capacity to assess the increased number of referrals that would result from this intervention, to avoid individuals becoming lost to services.
Interventions relating to mental health hospital to home service, and the community management of severe mental disorder also had limited impact on attempted suicide and suicide cases averted at the population level (Table 2). This is likely due to the small sub-population of those with acute or complex mental health needs targeted by these interventions.
Discussion
This study describes the co-design, development and application of a dynamic simulation model that aimed to inform the optimal combination of suicide prevention activity in the population catchment covered by WentWest – Western Sydney PHN (Sydney, Australia). The final model can be used by PHN stakeholders as an interactive ‘what if’ decision tool to compare and contrast different combinations of potential interventions to reduce suicidal behaviour in the PHN population catchment. The findings reported in the current study represent one set of scenarios (based on the default inputs developed in partnership with PHN stakeholders). There is also scope to investigate alternative scenarios related to the timing of implementation of interventions, scale up and level of participation and uptake, as well as the comparative costs of interventions, to provide a more nuanced investigation of potential intervention combinations.
Findings from the initial set of model scenarios suggested that the largest number of cases of attempted suicide and suicide could be averted by focussing on: (1) providing assertive aftercare and follow-up among those who have presented to services after a suicide attempt, (2) preventing disengagement from mental health services among those who have had mental health service contact and (3) reducing psychological distress and enhancing social connectedness in the general community. Providing assertive aftercare has been shown previously to be associated with reductions in recurrence of suicide attempts and subsequent suicide (Hvid et al., 2011) and has also been included in current community-level suicide prevention trials in Australia (Black Dog Institute, 2016), and was also an intervention of interest identified by PHN stakeholders.
For the other two scenarios, there were no specific interventions identified by stakeholders. This presents an opportunity to consider interventions that target community support and social connectedness; perhaps through modifications to social and community services and augmented by low intensity or online mental health interventions. Findings also suggested that if only a small proportion (15%) of those lost to mental health services could be re-engaged, a substantial number of cases of suicides and attempted suicides averted. No specific interventions were considered by PHN stakeholders for this intervention point in the model, but there appears to be a role for system strengthening and potentially the use of technology to ensure that services remain more effectively connected with individuals who have previously made contact with mental health services.
An additional finding from the model was that interventions that identify those at suicide risk (for example via GP or gatekeeper training, [Isaac et al., 2009; Knox et al., 2003; Milner et al., 2016] or Headspace [Hilferty et al., 2015]) had little impact on the potential number of attempted suicide and suicide cases averted, unless there was also an increase in mental health service capacity (in terms of assessment, staffing and staff training). This finding suggests that where interventions refer those at risk of suicide to existing mental health services, but there is not sufficient workforce and service capacity to absorb additional referrals, this may lead to increases, not decreases, in suicidal behaviour in communities. In the case of Headspace, this may also reflect that Headspace provides a range of services relating to mental health, physical health, work and study support and alcohol and other drug services, and not solely identifying those at suicide risk.
There are a number of limitations that require consideration when interpreting the findings of this paper. First, the model presented is a system dynamics model–an approach that models populations in aggregate. The model accounts for behavioural and population dynamics that impact mental health service capacity, suicidal behaviour and suicide outcomes. Aggregate systems models cannot consider the complex mechanisms and trajectories that affect the behaviours and outcomes for individuals. For example, it is not possible to assess the potentially differential impact of identified interventions on individuals with a particular combination of socio-economic position, migrant status or Indigenous status. Agent-based models are better placed to capture these mechanisms and can better capture causal inferences regarding the heterogeneity of individual behavioural trajectories (Marshall and Galea, 2014). However, system dynamics models offer significant value in informing strategic planning in timeframes that are more congruent with the timelines and priorities of service providers and policy makers. In addition, they are suited to analysis and improved understanding of the dynamics of complex problems, the non-additive effects of intervention combinations, the identification of leverage points where interventions can deliver greater than anticipated returns, and strategic directions for achieving population-level reductions in suicidal behaviour.
Second, there is potential measurement bias in the range of secondary data used to parameterise the model. Where possible, routinely collected local health service information was obtained to estimate population-based estimates of psychological distress, mental health service contacts (via MBS data), workforce information (in terms of numbers of general physicians [GPs], psychologists, psychiatrists, and allied health professionals) and primary, secondary and tertiary service capacity (in terms of numbers of beds, available appointments, and waiting times) from PHN and Local Health District datasets, hospital-based suicide attempts (from LHD data), and suicide data (from the ABS). There were also a number of population stocks, and information relating to rates of flow between population stocks, where routinely collected data sources were not available. In these instances, for example, the prevalence of psychological distress among the general population in comparison to the ‘vulnerable’ population, a combination of estimation and stakeholder consensus was used to identify plausible estimates.
The model acknowledges these potential sources of measurement bias, and a number of commonly used strategies were employed to address them, including the triangulation of multiple data sources, calibration to refine parameter estimates and the engagement of stakeholders with detailed knowledge of the limitations and likely direction and size of potential measurement biases in key data sources. In addition, interactive ‘sliders’ were added to the model interface to allow default input estimates to be varied across the model structure by end-users, enabling the testing of alternative parameter scenarios and assumptions. This function allows exploration of which parameter estimates the model outputs are most sensitive to change, and can guide priorities for new data collection and quality improvement of existing data collection.
There is potentially an under-enumeration of suicide cases used to calibrate the model, due to the misclassification of suicides to International Statistical Classification of Diseases and Related Health Problems (ICD) codes relating to unintentional injury and events of ‘undetermined intent’. However, this does not preclude the use of these data particularly in studies of time-series analyses. In addition, hospital suicide attempts (from hospital admissions) capture only those cases serious enough to warrant medical intervention, and will under-enumerate the total population burden of attempted suicide in the WentWest – Western Sydney PHN population catchment.
Finally, the interventions included in the model represent a limited set of potential suicide prevention interventions. These interventions were included in the model based on consultation with local stakeholders, and guided by Commonwealth priorities for PHNs (Department of Health, 2017; National Mental Health Commission, 2014). This led to a focus on mental health service interventions, conceptualised according to a stepped care model of mental health service provision (Cross and Hickie, 2017). Other whole-of-population interventions relating to, for example, restricting access to means, communication campaigns, education or employment may be of importance in the prevention of suicidal behaviour, but have not been explicitly included. While there is scope within the model to consider the impact of interventions relating to broader social determinants of suicidal behaviour in general terms (e.g. via investigations of transitions to ‘vulnerable’ populations, and populations in ‘psychological distress’), the model provides more detailed insights relating to primary health care and mental health service settings.
In addition, the findings of the present study represent one set of scenarios for the identified interventions. Alternative scenarios and combinations of interventions may result in different impacts on forecast attempted suicide and suicide cases (as noted above). For example, the model also allows for alternative scenarios that investigate the timing of the onset of interventions, the level of participation and uptake and changes to workforce structure and capacity. These alternative scenarios allow a more sensitive investigation of how interventions might be implemented in reality in terms of competing priorities and logistical constraints, but may lead to alternative conclusions regarding the most appropriate combinations of interventions to maximise reductions in suicidal behaviour.
Diverse local perspectives and interests often provide decision makers with conflicting advice regarding the best course of action. Data limitations, insufficient local analytic capacity and inadequate tools to support longer term planning in a context of changing local needs, contribute to the persistence of a trial and error approach and levels of programme turnover that may delay or prevent the realisation of significant impacts on suicide and suicidal behaviour. The modelling approach described in the present study is one way to address some of these challenges, and can also contribute to prioritising data sources and infrastructure to better support integrated and longer-term programme evaluation and continuity of care.
This study demonstrates the utility of dynamic simulation models, co-designed with multi-disciplinary stakeholder groups, to capture a complex model of primary mental health service provision and suicidal behaviour, and to identify potential points for intervention activity. This system approach applied to suicidal behaviour can be used to develop policy decision support tools, provide a process for consensus building and the development of partnerships in contentious areas of population health and provide evidence to guide the prioritisation of services, interventions and programme evaluation for a given population.
The present study suggests that the most effective combination of interventions to reduce suicidal behaviour in the WentWest – Western Sydney PHN population catchment relates to the provision of assertive aftercare among those with a previous suicide attempt, the re-engagement of individuals previously in mental health services and the reduction of psychological distress in the general community. This information can be used by the PHN to guide decisions on the commissioning of future service activity, and more efficiently frame the future monitoring and evaluation of interventions as they are implemented in Western Sydney.
Supplemental Material
anzjp_submission19Feb2018_supplementarymaterial – Supplemental material for A decision support tool to inform local suicide prevention activity in Greater Western Sydney (Australia)
Supplemental material, anzjp_submission19Feb2018_supplementarymaterial for A decision support tool to inform local suicide prevention activity in Greater Western Sydney (Australia) by Andrew Page, Jo-An Atkinson, William Campos, Mark Heffernan, Shahana Ferdousi, Adrian Power, Geoff McDonnell, Nereus Maranan and Ian Hickie in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
This model was developed by Decision Analytics (Sax Institute) and the Translational Health Research Institute (Western Sydney University) in partnership with WentWest–Western Sydney Primary Health Network and the Brain and Mind Centre, University of Sydney. Importantly, this work was made possible by the generous contributions of local expert knowledge and data by representatives of the following stakeholder agencies: Western Sydney Local Health District, Hills Shire, Parramatta, Blacktown and Cumberland City councils, the Western Sydney Regional Organisation of Councils, NSW Police Force, Headspace, WESTIR Ltd., and consumer representatives.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
This research was supported by a Western Sydney University Partnership Grant, and in-kind contributions from WentWest–Western Sydney (in part with the Commonwealth Department of Health) and Western Sydney Local Health District.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.