
Abstract
Objective:
This study intended to classify subtypes of Korean adolescents with suicidal ideation based on mental health problems and to explore the relationship between such subtypes and individual-, school- and community-level factors.
Method:
Data from high school freshmen who participated in the 2013 school-based mental health screening test and data about school and community variables obtained from public sources were combined and analyzed. A multilevel latent profile analysis using mental health issues as class indicators that included several predictors was conducted.
Results:
Three latent profiles were identified: Group 1 (6.5%) had high scores for both the internalizing and externalizing problems; Group 2 (40.2%) had high scores for internalizing problems, such as depression and mood related symptoms; and Group 3 (53.3%) had lower scores for all mental health problems compared to Groups 1 and 2. Gender, peer conflict, family conflict and academic problems were significant predictors at the individual level; school dropout rate was a significant school-level variable; and percent of youth in the total population, availability of mental health services, number of social welfare facilities and percentage of the total budget devoted to education/welfare were significant community-level variables.
Conclusion:
The present findings suggest that adolescents with suicidal ideation can be classified into several distinct subtypes based on mental health problems. These profiles and their associated covariates will aid in the establishment of youth suicide prevention policies.
Introduction
Approximately 1.3 million young people died from suicide in 2012, making suicide the third leading cause of death among adolescents (World Health Organization, 2012). The significant loss of productivity due to suicide renders the need to reduce the suicide rate of adolescents an important nationwide task (Nock et al., 2008b). Therefore, many countries have implemented suicide intervention and prevention policies targeted at youth. Studies investigating the factors associated with suicidal behavior have found that suicidal ideation, which is a major risk factor for attempted and completed suicide (Nock et al., 2008a; Scott et al., 2015), is relatively common among adolescents (Bridge et al., 2006; Gould et al., 2003; Nock et al., 2008b). Although there are differences among countries, the prevalence of suicidal ideation among adolescents is reported to be approximately 20–30% (Evans et al., 2005; Kokkevi et al., 2012).
A systematic review of the literature revealed that various psychiatric disorders and psychological, personal, family and social factors are associated with suicidal ideation in adolescents (Evans et al., 2004). Although depressive disorders are the most influential factor in suicidal ideation (Gould et al., 2003; Kandel et al., 1991; Nock et al., 2013), anxiety disorders (Hill et al., 2011; O’Neil Rodriguez and Kendall, 2014), mood disorders (Gould et al., 1998; Park et al., 2012), oppositional defiant disorder (Gould et al., 1998; Nock et al., 2013), substance (alcohol and drug) abuse (Buddeberg et al., 1996; Nock et al., 2013), eating disorders (Buddeberg et al., 1996; Nock et al., 2013) and impulsive aggression (Apter et al., 1993; Javdani et al., 2011; Kashani et al., 1989) are also major risk factors. In addition, family-related risk factors known to contribute to youth suicidal ideation include family discord, family history of suicidal behavior or mental disorders, family structure and low family support (Bridge et al., 2006; Evans et al., 2004; Prinstein et al., 2000). These factors may cause the risk of their suicidal ideation or indirectly influence risk through individuals’ psychological problems. In addition, the educational and social risk factors for suicidal ideation among youth include low school attendance rates, negative attitudes toward school and poor relationships with peers (Bearman and Moody, 2004; Evans et al., 2004; Prinstein et al., 2000).
Suicide cannot be explained by a single factor, and the clinical manifestations of suicidal ideation among adolescents are very diverse. As a result, several studies have investigated the heterogeneity of suicidal behaviors in adolescents. Jiang et al. (2010) found that suicide-related behaviors in adolescents can be classified into four groups according to their patterns (e.g. emotionally healthy, considered and planned suicide, attempted suicide, planned and attempted suicide) and reported that the effects of the predictors differed in each group. Similarly, Goldston et al. (2016) categorized the developmental trajectories of suicidal thoughts and attempts into four groups (e.g. increasing class, highest overall risk class, decreasing class, lowest risk class) in a longitudinal study. However, the interpretation of previous results such as these may be limited due to the specificity of the samples (e.g. clinical samples) and small sample sizes. Moreover, although most of the relevant influences included individual-level variables, factors at the social, psychological, community and other levels can interact and also result in suicidal ideation. For example, the structural characteristics of a community, including its poverty rate, proportion of government assistance recipients, and social cohesion (Aneshensel and Sucoff, 1996; Simons et al., 1996), can affect the mental health of individual members. Although several studies have examined the relationships between mental health in adolescents and community characteristics, such as mental health institutional resources or the perception of neighborhood (Aneshensel and Sucoff, 1996; Ross and Mirowsky, 2001), a comprehensive and multi-system strategy for suicide prevention is required to determine the effectiveness of these policies. Therefore, this study aimed to classify subgroups of Korean adolescents with suicidal ideation based on mental health problems and to examine their associations with relevant individual-, school- and community-level factors.
Method
Data
The Ministry of Education of the South Korea has been conducting compulsory school-based mental health screening tests under the School Health Act since 2012 to screen for and intervene in student mental health problems. The present survey was administered to all first- and fourth-grade students in entire elementary schools and to first-grade students in entire middle and high schools. At-risk adolescents can be identified using the total score on the Adolescents Mental Health and Problem Behavior Screening Questionnaire-II (AMPQ-II; Bhang et al., 2011). For this study, data from high school students were extracted from the school-based mental health screening test conducted in 2013 and analyzed with the permission of the Ministry of Education. These data did not include information that could personally identify a subject other than school and gender.
The study population included 618,271 high school students (97.5% of the total). Next, based on the proportion of high schools in each region according to the statistical yearbook of education published by the Department of Education, 26,440 students from 100 high schools were randomly selected for inclusion in this study. The response rates of the suicide ideation item were as follows: not at all, 84.7% (n = 22,407); slightly, 11.8% (n = 3120); quite, 2.7% (n = 708); very much, 0.8% (n = 205). Four schools were excluded because no students met the study criteria for the suicidal ideation group (i.e. endorsed ‘quite’ or ‘very much’ on the suicidal ideation question of the AMPQ-II). Thus, the final sample consisted of 913 students from 96 schools. Multilevel data were constructed by combining school characteristics and community variables from open public data sources with student clinical data from the mental health screening tests of the sample schools. This study was approved by the Institutional Review Board of Hallym University Sacred Heart Hospital.
Measures
AMPQ-II
The AMPQ-II was developed as a school-based mental health screening test to effectively screen for mental health problems in youth. This tool has acceptable internal consistency and test–retest reliability (α = 0.890 and r = 0.567), and there is a positive correlation between the AMPQ-II and the Symptom Checklist-90-Revision (r = 0.20–0.70, p < .01; Bhang et al., 2011). This questionnaire consists of 38 items that assess various mental health and socio-psychological problems, including problems specific to adolescents. Students respond by indicating whether they agree or disagree using a 4-point scale (0 = not at all, 1 = slightly, 2 = quite a bit, 3 = very much); a higher total score indicates more emotional or behavioral difficulties.
Suicidal ideation
The suicidal ideation item on the AMPQ-II was used to identify students at risk (‘I have thought about killing myself consistently or made a concrete plan for suicide’.). Responses scored as at least 2 points (quite) were classified as reflective of suicidal ideation.
Indicators
This study used the items measured by the AMPQ-II as indicators for the classification of adolescent subjects into suicidal ideation subgroups. The AMPQ-II is divided into 13 domains related to mental health problems and 4 domains related to the experience of adverse life events (Bhang et al., 2011) and this study followed this framework. Based on previous studies (Bridge et al., 2006; Gould et al., 2003), the items assessing adverse life events were classified as individual-level predictors that influenced subgroup classifications. One domain related to seizures consists of an item with a very low incidence (mean = 0.6) and was excluded from this study; thus, 12 indicators were used to identify latent profile membership as described below.
Inattention and impulsivity consisted of three items (e.g. ‘Had trouble concentrating during lessons, study, or reading books, etc.’; α = 0.680); obsessions and compulsions included two items assessing compulsive behavior and thinking (α = 0.429); depressive symptoms were measured with two items (e.g. ‘Felt depressed or irritated for no apparent reason’; α = 0.693); behavior problems included four items (e.g. ‘Harassed or struck other people or animals’; α = 0.659) that evaluated serious violations of rules, stealing goods and/or destroying the belongings of others; Internet and substance overuse were assessed with two items (e.g. ‘Used substances prohibited to students, such as cigarettes, alcohol, ecstasy, etc.’; α = 0.272); psychotic symptoms included four items that measure auditory hallucinations and persecution (α = 0.709); sexual problems included two items that assessed sexual impulses (e.g. ‘Thought too much about sex’; α = 0.779); eating problems included two items that evaluated problem eating (e.g. ‘Sporadically engaged in binge eating and vomiting’; α = 0.459); anxiety was measured with two items (e.g. ‘Been afraid to speak in front of people’; α = 0.452); mood included two items that assessed difficulties with emotional regulation (e.g. ‘Experienced losing my temper’; α = 0.494); somatization was measured with one item (e.g. ‘Often been sick for no apparent reason (e.g. headache, stomachache, dizziness, etc.)’); and sleep disturbances was measured with one item (e.g. ‘Experienced difficulty falling asleep or intermittent awakening during the night, which caused problems’). A confirmatory factor analysis (CFA), which was performed to evaluate construct validity, revealed an appropriate model fit to the data (chi-square [χ2] = 734.531, degrees of freedom [df] = 194, comparative fit index [CFI] = 0.913, root mean square error of approximation [RMSEA] = 0.056 and standardized root mean square residual [SRMR] = 0.045).
Individual-level predictors
Individual-level predictors included gender (male = 1, female = 2), family conflict, peer conflict, academic problems and violent victimization and were measured based on the experience of adverse events measured by the AMPQ-II. Peer conflict assessed the experience of bullying and difficulties with peer relationships using three items: family conflict was measured based on the degree of discord among family members; academic problems were assessed based on the degree of difficulty understanding school lessons; and violence was determined based on the experience of physical and/or verbal violence and sexual humiliation. All items except gender were measured on a 4-point scale (0 = not at all, 1 = slightly, 2 = quite a bit and 3 = very much).
School/community-level predictors
School characteristics were collected using the official school information system provided by the Korea Educational and Research Information Service. ‘School Info’ provides information about the educational environment, student status and budget information of each school. The school dropout rate was calculated by dividing the total number of students by the number of students who had been expelled from or dropped out of school. The student-to-teacher ratio was calculated by dividing the enrollment of a school by the number of teachers employed by that school. Counseling rate was the average number of counseling sessions per student and included both internal and out-of-school counseling.
Community characteristics were obtained from the Korean Statistical Information Service (KOSIS) and administrative census data. The data included place of residence (metropolitan, urban or rural), proportion of population aged 15–19 years, suicide rate among youth (aged 15–19 years), number of social welfare facilities, proportions of the total budget accounted for by funding for education and welfare, and proportion of public assistance recipients in the local population. The availability of health care was calculated according to the density of the mental health clinics distributed within a distance of 10 km from each school location; a higher value indicated more mental health services were available.
Statistical analysis
A multilevel latent profile analysis (MLPA) was conducted to determine the subgroups of adolescents that were more likely to be considering suicide and to examine the associations between these groups and predictors at the individual and school/community levels. In the hierarchical structure, individuals were not considered completely independent in that one individual might share certain properties, such as culture and attitudes, with another. Thus, respondents in the same group were likely to be more similar to one another than to respondents in a different group. Thus, because the assumptions of independence and identical distribution across the groups were violated, standard errors may have been underestimated and the likelihood of Type I errors increased (Kenny and Judd, 1986). The present data represent a hierarchical structure in which many students belong to the school; therefore, a multilevel model was applied due to the dependency among students in the same school.
The analysis was conducted using the following steps. First, the most appropriate number of groups at the individual level was determined based on the results of an analysis performed without covariates, and the optimal number of profiles was determined by considering statistical criteria and profile interpretability. The statistical criteria included information criteria, likelihood-based tests and quality of classification; the information criteria contained the Akaike information criteria (AIC), Bayesian information criterion (BIC) and sample size-adjusted Bayesian information criterion (SABIC); the lowest value indicates the best fitting model. The bootstrap likelihood ratio test (BLRT) and the Lo–Mendell–Rubin likelihood ratio test (LMR LRT) were used to compare k – 1 and k class models and to provide estimates with p-values; when the value of p was significant, the k – 1 class model was rejected and the k class model was accepted. Entropy, which indicates the quality of the classification, has a value between 0 and 1, and values closer to 1 indicate that the group classification is clear. Finally, the effects of the covariates were assessed at both levels with a multinomial logistic regression based on the probability of belonging to each group. All data analyses were performed using Mplus 7.4 (Muthén and Muthén, 1998–2015) and missing data were treated using the full information maximum likelihood.
Results
Identification of subgroups
Three latent profile models were considered when selecting the best model (Table 1). The maximum decrease in the BIC was observed when the number of groups increased from two to three, and entropy was highest in the three-class model. The LRT was not significant in the four-class model, whereas the three-profile model was interpretable and theoretically meaningful. Group 1 had higher scores in all mental health problem domains, including the internalizing and externalizing domains, compared with the other two groups (6.5%; Figure 1). Group 2 had higher scores on the emotional domains (e.g. depression, anxiety and mood) but lower scores related to behavior problems, Internet and substance overuse, and sexual problems (40.2%). Finally, Group 3 had relatively lower scores on all mental health problem domains compared to Groups 1 and 2 (53.3%). However, the average score for suicidal ideation in Group 3 was 2.16 points, which was similar to those in the other two groups (Group 1 = 2.31 and Group 2 = 2.30). Since the response ‘quite’ is dominant in the three groups, the medians of the groups are the same but not discriminative. Therefore, it should be noted that the Likert scores are presented in the average form, not median or mode.
Model fit statistics for each model.
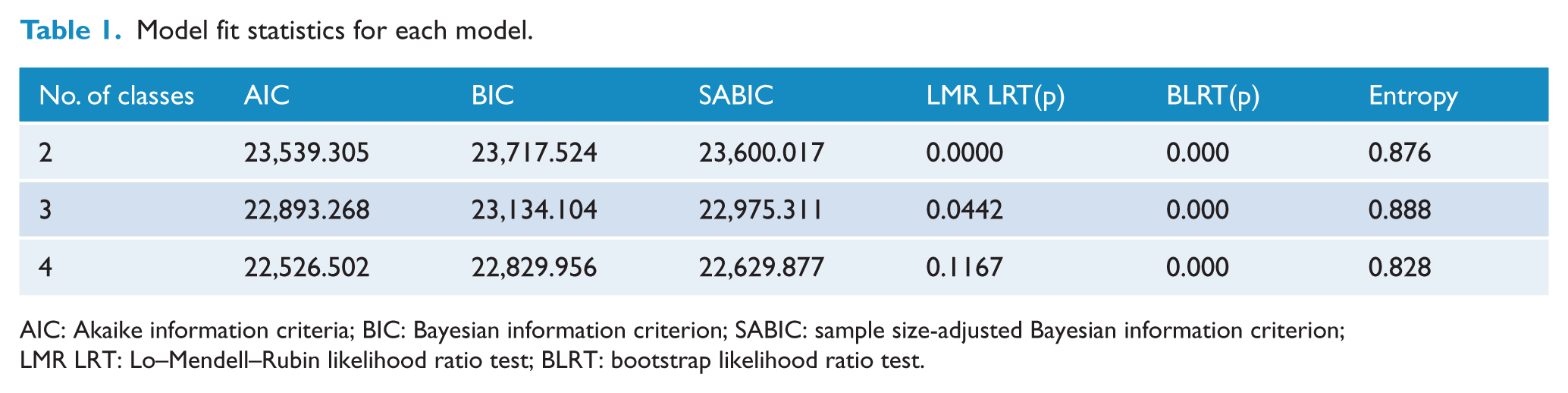
AIC: Akaike information criteria; BIC: Bayesian information criterion; SABIC: sample size-adjusted Bayesian information criterion; LMR LRT: Lo–Mendell–Rubin likelihood ratio test; BLRT: bootstrap likelihood ratio test.
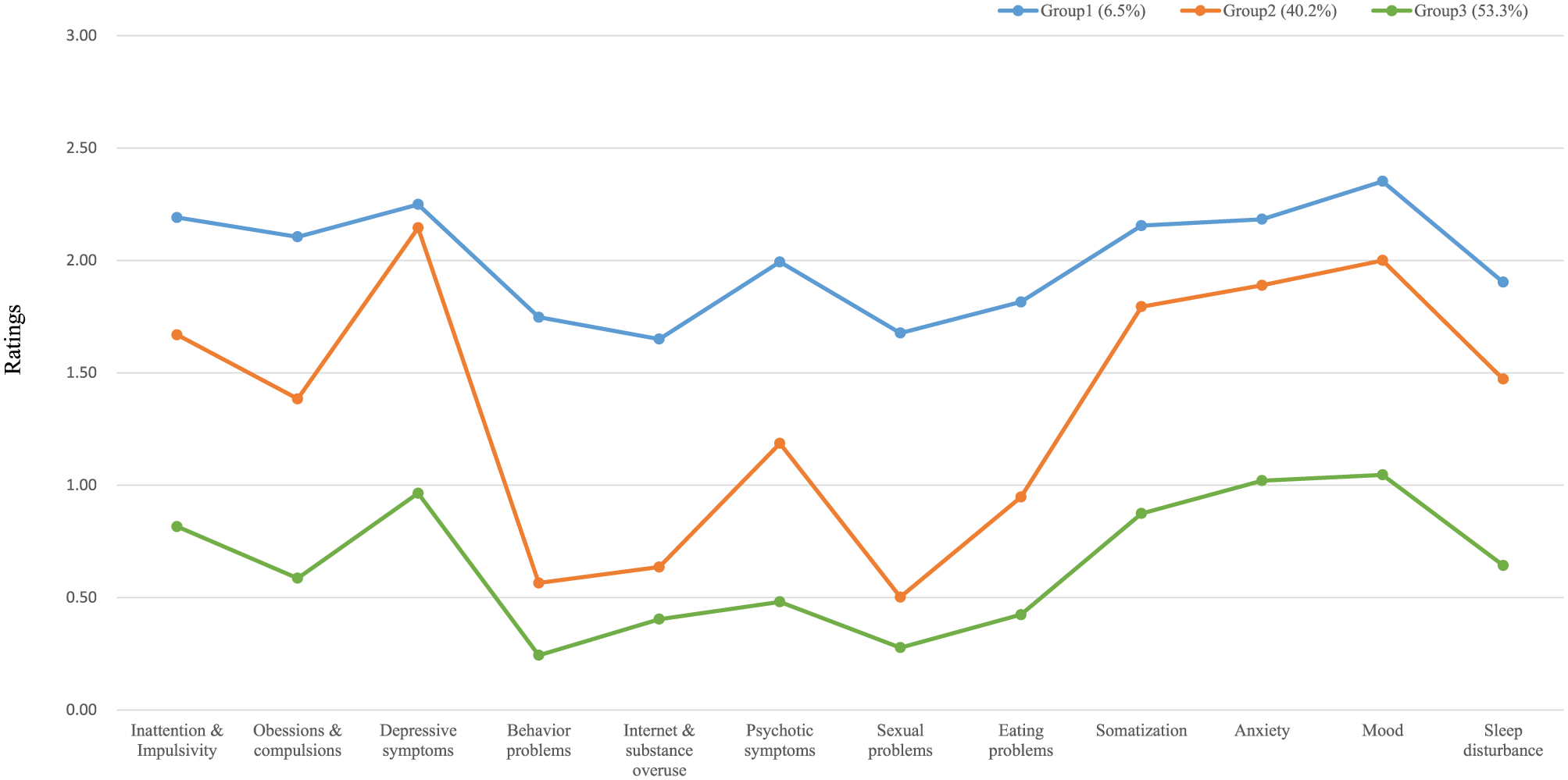
Mean scores for each mental health domain among the three profiles.
Associations with individual-level predictors
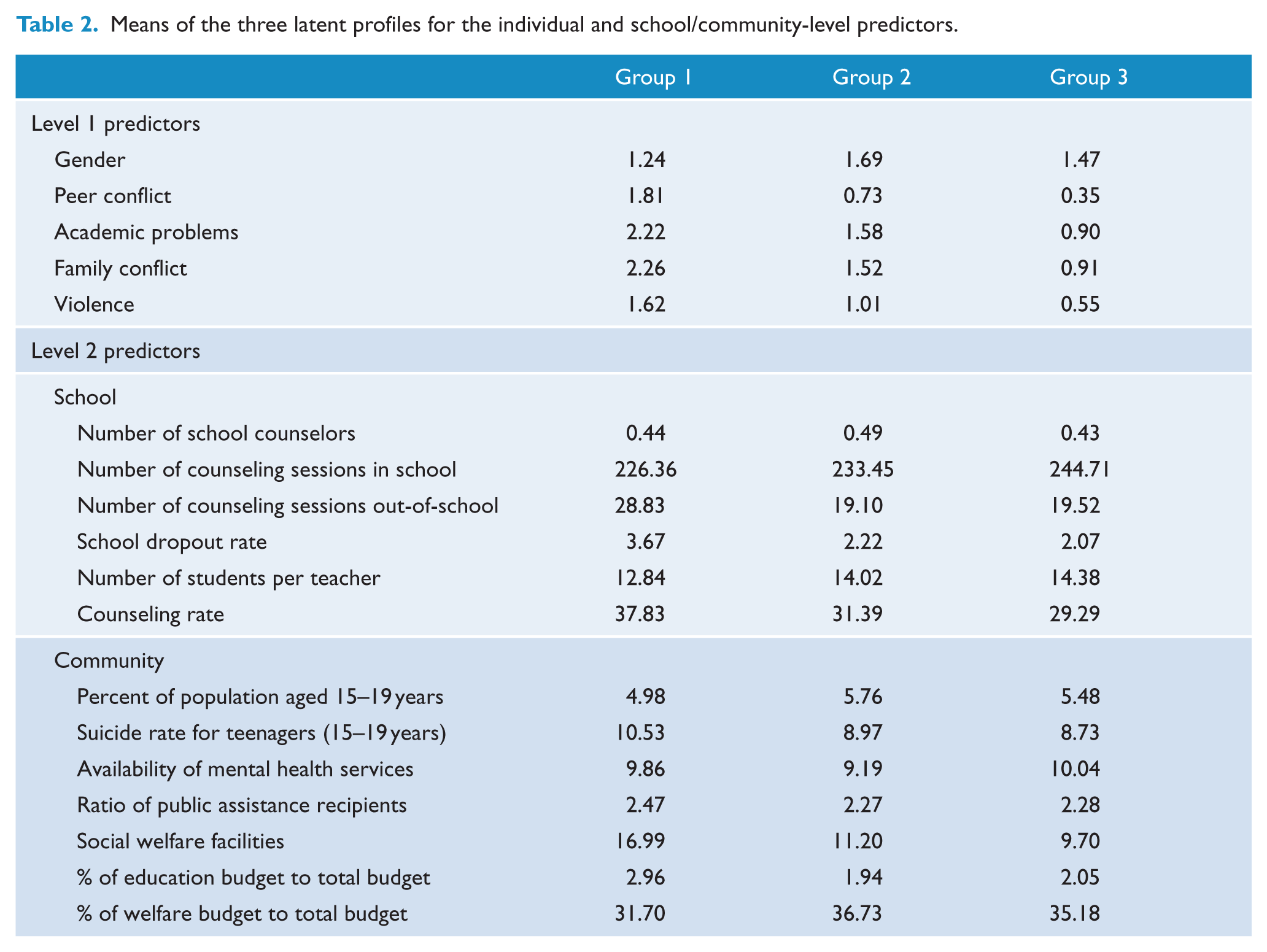
Table 2 summarizes the means of the three latent profiles for the individual- and school/community-level predictors. The statistical results of the conditional MLPA are given in Table 3. Latent profile membership was regressed on the individual predictors in a multinomial logistic regression with Group 3 set as the reference group in the analysis. All individual variables, except the violence covariates, were statistically significant (Table 3). Group 1 was associated with higher levels of peer conflict, family conflict and academic problems than Group 3, and male students were more likely to belong to Group 1 than Group 3. Group 2 was also associated with higher levels of peer conflict, family conflict and academic problems than Group 3, and female students were more likely to belong to Group 2 than Group 3.
Means of the three latent profiles for the individual and school/community-level predictors.
Statistical results of the conditional multilevel latent profile analysis.
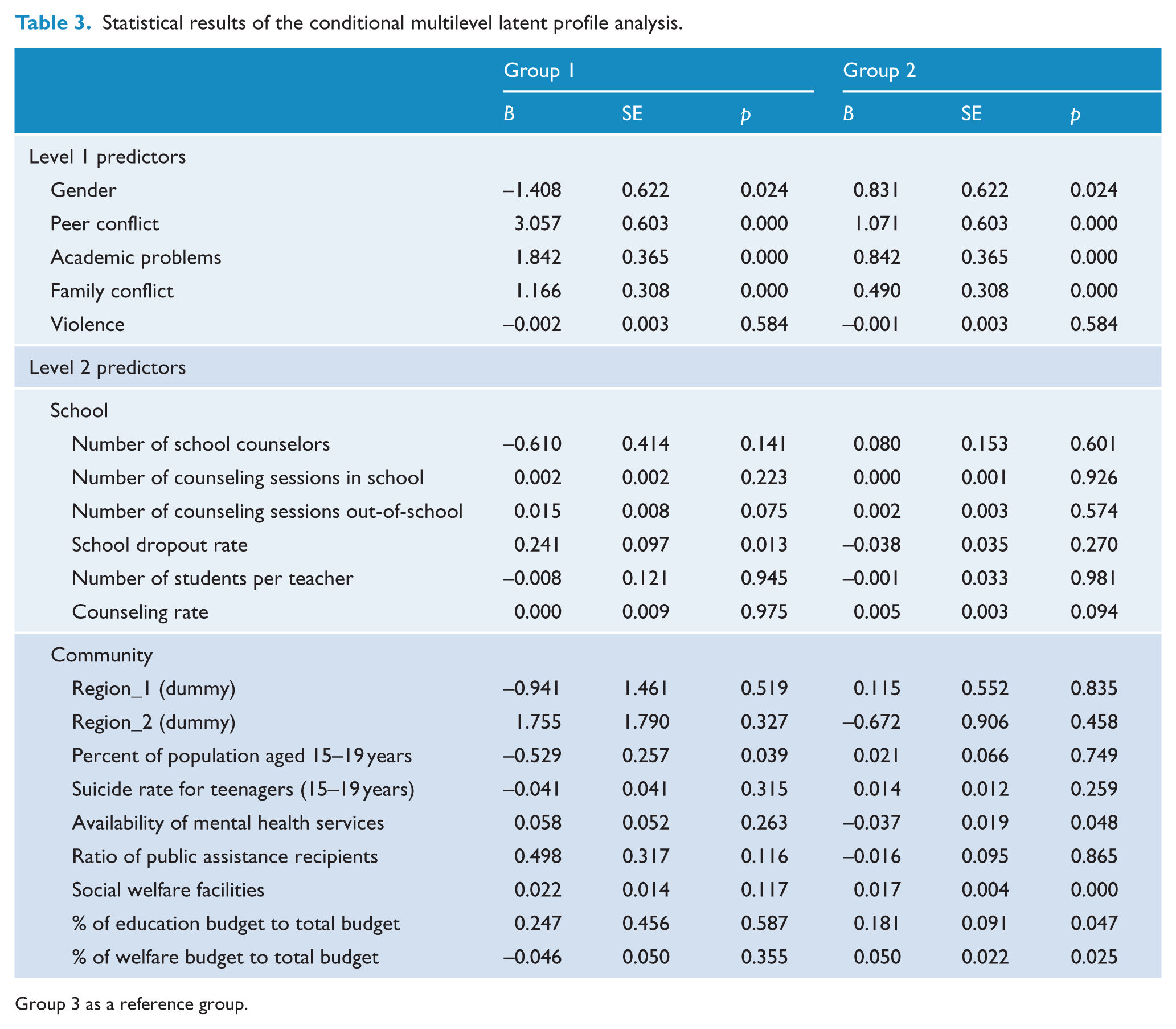
Group 3 as a reference group.
Associations with school/community-level predictors
Group 1 was associated with a higher school dropout rate and a lower percentage of individuals aged 15–19 years than Group 3. There were no differences between Groups 1 and 3 with respect to the other predictors. On the other hand, Group 2 was associated with a higher welfare/education budget ratio and a lower availability of mental health resources than Group 3, and Group 2 had more social welfare facilities than Group 3. These groups did not differ regarding the other school/community-level variables.
Discussion
Previous studies of suicidal ideation and risk factors in adolescents have either examined the subjects reporting suicidal ideation as a single group or grouped them by gender or age. However, several heterogeneous subgroups stratified according to various characteristics may exist within such a population. For example, several studies have classified individuals into subgroups based on the trajectories of suicidal thoughts and suicide attempts, patterns of suicide-related behaviors, and patterns of self-harm and suicidal behavior (Goldston et al., 2016; Hamza and Willoughby, 2013; Jiang et al., 2010). Goldston et al. (2016) emphasized how suicidal ideation and attempts can be developed into different consequences from adolescence to adulthood and classified the developmental trajectories of suicidal thoughts and behaviors into four classes: an ‘increasing risk class’, a ‘highest overall risk class’, a decreasing risk class and a low risk class. Jiang et al. (2010) rather focused on the suicidal planning and execution and suggested four latent classes of suicide risk: emotionally healthy group, considered and planned suicide group, attempted suicide group, and both planned and attempted suicide group. Additionally, psychiatric disorders are well-known major risk factors for suicide as nearly 90% of adolescents who experience suicidal ideation meet the lifetime criteria for at least one Diagnostic and Statistical Manual of Mental Disorders (DSM; Nock et al., 2013). However, no studies have used a person-centered approach to determine whether a group of adolescents with suicidal ideation exhibits different patterns of behavior based on individual mental health problems and then used these characteristics to distinguish subgroups. Thus, this study conducted an MLPA to identify subgroups of adolescents with suicidal ideation and examined how these profiles were related to individual-, school- and community-level variables. The present findings demonstrated that adolescents with suicidal ideation could be classified into three distinct groups according to various patterns of mental health problems. Additionally, the groups significantly differed in terms of the effects of each level of variables.
Group 1 was characterized by suicidal ideation in conjunction with internalizing problems (e.g. depression and anxiety) and externalizing problems (e.g. behavior problems and impulsivity). This group also had higher levels of family conflict, peer conflict and academic problems than the other two groups (Table 2). Male students were more likely to belong to Group 1, and students at a school with a high dropout rate and those who attended a school in an area with a lower percentage of adolescents (15–19 years) in the population were more likely to belong to Group 1 than Group 3. Group 2 was characterized by suicidal ideation in conjunction with internalizing problems, such as depressive symptoms and anxiety. This group also had relatively high levels of family conflict, peer conflict and academic problems compared to Group 3. Female students were more likely to belong to Group 2, and students in areas with lower levels of community mental health services, a higher number of social welfare facilities and a higher proportion of the total budget devoted to welfare/education were more likely to belong to Group 2 than Group 3.
This study showed that adolescents who experienced family or peer conflicts were more likely to belong to Group 1 or 2 than Group 3. Furthermore, the frequency of negative events was relatively low in Group 3, in which externalizing and internalizing problems did not accompany suicidal ideation. These results indicate that negative life experiences may affect suicidal thoughts as well as mental health problems. A meta-analysis concluded that family discord and poor peer relationships are significantly associated with suicidal ideation (Evans et al., 2004) and several studies have shown that family conflict is related to externalizing as well as internalizing problems (Formoso et al., 2000; Jenkins and Smith, 1991). In particular, externalizing problems in children and adolescents are highly influenced by their family experiences (Patterson, 1982).
Groups 1 and 2 had higher levels of academic problems relative to Group 3. Previous empirical studies revealed a significant association between academic failure and depression (Ang and Huan, 2006; McCarty et al., 2008) and other studies have reported that academic difficulties increase negative feedback on academic performance, which leads to the development of depressed mood (Moilanen et al., 2010; Owens et al., 2012). These findings suggest that academic difficulties are directly related to depression and have the potential to influence various mental health problems through negative emotions. Therefore, peer conflicts, family conflicts and academic problems may operate in conjunction with mental health problems, acting as important predictors of suicidal ideation in subgroups of adolescents. These characteristics should be considered when assessing and intervening with students with numerous negative life experiences.
Of the school-level variables, the dropout rate of the school that the student attended was associated with Group 1, which indicates that school climate may be associated with adolescent mental health problems and suicidal ideation. Christle et al. (2007) found significant positive correlations between dropout rate and five school characteristics, including retention rate, socioeconomic status (SES), law violation rate, suspension rate and board violation rate. In other words, an elevated school dropout rate suggests that the abovementioned characteristics are common and that the school climate is not positive. School climate has been described as the characteristics and quality of school life such that a positive school climate promotes social, mental and emotional development in students and enhances behavioral and learning outcomes (Lester and Cross, 2015; Loukas and Robinson, 2004). Kuperminc et al. (2001) demonstrated that perceptions of school climate have a moderating effect on psychological vulnerability to both internalizing and externalizing problems. In other words, the perception of a positive school climate is a protective factor that reduces personal vulnerability to the development of internalizing and externalizing problems. Therefore, although it is important to intervene in adolescents with psychiatric disorders to prevent suicide and improve mental health, it is also important to develop effective school policies to establish a positive school climate. This study showed that students in a school located in a region with a high ratio of adolescent youth were more likely to belong to Group 3 than Group 1. These areas likely have good educational environments, and many of the parents are supportive of education. These local characteristics and the characteristics of parents are thought to be protective factors against the development of mental health problems in adolescents.
This study also showed that when the availability of mental health care services in a community was high, students were more likely to belong to Group 3. In this context, a high level of availability means that many mental health care facilities were accessible within a 10 km radius of a school. The availability of medical resources is closely related to the ease of physical access as well as psychological familiarity with the use of medical services. In other words, it is possible to provide timely and appropriate mental health services to adolescents. Accordingly, compared to the other groups, adolescents in Group 3 in this study had a relatively low level of mental health problems associated with suicidal ideation. Intervention is one of the most important factors that can reduce the severity of adolescent mental health problems and minimize long-term side effects (Hurlburt et al., 2004). Therefore, it is necessary to consider not only expanding the accessibility of mental health services in the community but also reducing the psychological distance associated with using these facilities.
This study also found that students were more likely to belong to Group 2 than Group 3 when there were many social welfare facilities in the community and a large proportion of the budget was allocated to education or welfare. An analysis of types of welfare services according to regional characteristics revealed a relatively high level of welfare provision in regions with a low ratio of financial independence or a high ratio of poverty (Park, 2006). In such areas, the ratio of public assistance recipients, the percentage of child-headed families and the proportion of elderly people are high. Community characteristics, such as residential instability and concentration of poverty, are also risk factors for mental health (Bernburg et al., 2009; Silver et al., 2002). In particular, Wickrama and Bryant (2003) found that community poverty affects depressive symptoms in adolescents even after controlling for family and individual characteristics. Cutrona et al. (2006) proposed that vulnerable neighborhood conditions influence depression in three different ways: by increasing levels of daily stress, enhancing vulnerability to negative events and disrupting social ties. Thus, there should be concern for adolescents with suicidal ideation accompanied by internalizing problems if they live in areas with vulnerable community characteristics. Taken together, these findings underscore the importance of considering community conditions when establishing suicide-related and other mental health policies.
Group 3, which comprised 53.3% of the sample, included adolescents who scored <1 on all domains of mental health problem and, thus, had a lower risk of mental health problems relative to the other two groups. The rates of peer conflict, family conflict and academic problems in Group 3 were the lowest among the three groups. Thus, Group 3 was characterized by a high risk of suicidal ideation that was not accompanied by obvious psychopathology, which may make it more difficult to prevent and intervene in this group compared to Groups 1 and 2. In practice, many current interventions focus on groups that possess many risk factors (Carli et al., 2014; Stanford et al., 2017). Therefore, the need to continuously monitor students with these characteristics and comprehensively evaluate changes in their suicide risk should be emphasized. In addition, further studies should be conducted to identify the characteristics of individuals in Group 3.
The present findings should be interpreted in the context of several limitations. First, the data used in this study were collected from 10th-grade students attending school. Therefore, the characteristics of out-of-school youths, such as those who dropped out of school or received alternative educations due to various academic and interpersonal difficulties, may not be reflected in our results. Based on national statistical data, approximately 30,000 high school students, approximately 1.6% of the total enrollment, stopped studying in 2014. Second, the data were collected using self-report questionnaires. In these types of questionnaires, respondents tend to under- or over-report their actual status since they want to be perceived themselves in a more positive way. Third, demographic information (other than gender) was not collected, and the influences of these variables could not be controlled for.
Despite these limitations, this study has several strengths. Most importantly, this study was conducted using data collected from all high school first-graders in Korea, whereas previous studies of adolescent suicidal ideation included only a small number of participants. Second, the present results confirmed that students with a high risk of suicide should be classified into heterogeneous subgroups and that the factors affecting each of these groups differed. Given this heterogeneity, it will be important to develop and examine the effectiveness of targeted interventions. This may be particularly true for Group 3, in which the level of suicidal ideation was high but the degrees of externalizing and internalizing problems were not serious. This indicates that suicidal ideation may not be accompanied by mental health problems in all cases; thus, it can be expected that many potential risk groups may be overlooked if suicide prevention counseling is centered solely on students with mental health problems. Third, the factors influencing group classification were divided into individual-, school- and community-level variables and verified by multidimensionality.
This study showed that adolescents with suicidal ideation could be classified into heterogeneous subgroups and that the individual-, school- and community-level factors influencing each group differed. Therefore, to increase the effectiveness of suicide prevention policies, it may be necessary to develop programs that are customized based on factors specific to each group.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
This work was supported by the Ministry of Education of the Republic of Korea and the National Research Foundation of Korea (NRF-2015S1A5B8A02061201).