
Abstract
Objective:
For at least two decades, concerns have been raised about inappropriate psychotropic prescribing in Australian residential aged care facilities, due to their modest therapeutic benefit and increased risk of falls and mortality. To date, the majority of prevalence data has been collected in Sydney exclusively and it is not known if recent initiatives to promote appropriate psychotropic prescribing have impacted utilisation. Thus, we aimed to comprehensively analyse psychotropic use in a large national sample of residential aged care facility residents.
Method:
A cross-sectional, retrospective cohort study of residents from 150 residential aged care facilities distributed nationally during April 2014–October 2015. Antipsychotic, anxiolytic/hypnotic and antidepressant utilisation was assessed, along with anticonvulsant and anti-dementia drug use. Negative binomial regression analysis was used to examine variation in psychotropic use.
Results:
Full psychotropic prescribing data was available from 11,368 residents. Nearly two-thirds (61%) were taking psychotropic agents regularly, with over 41% prescribed antidepressants, 22% antipsychotics and 22% of residents taking benzodiazepines. Over 30% and 11% were charted for ‘prn’ (as required) benzodiazepines and antipsychotics, respectively. More than 16% of the residents were taking sedating antidepressants, predominantly mirtazapine. South Australian residents were more likely to be taking benzodiazepines (p < 0.05) and residents from New South Wales/Australian Capital Territory less likely to be taking them (p < 0.01), after adjustment for rurality and size of residential aged care facility. Residents located in New South Wales/Australian Capital Territory were also significantly less likely to take antidepressants (p < 0.01), as were residents from outer regional residential aged care facilities (p < 0.01). Antipsychotic use was not associated with State, rurality or residential aged care facility size.
Conclusion:
Regular antipsychotic use appears to have decreased in residential aged care facilities but benzodiazepine prevalence is higher, particularly in South Australian residential aged care facilities. Sedating antidepressant and ‘prn’ psychotropic prescribing is widespread. Effective interventions to reduce the continued reliance on psychotropic management, in conjunction with active promotion of non-pharmacological strategies, are urgently required.
Introduction
Residents of Australian residential aged care facilities (RACFs), similar to those in many countries, have high rates of sleep disturbance, anxiety, depression, and behavioural and psychological symptoms of dementia (BPSD) (Björk et al., 2016; Chen et al., 2016). Although professional guidelines advocate non-pharmacological management as the first-choice treatment option for these common mental health conditions, in most cases, psychotropic agents – antipsychotics, antidepressants and/or anxiolytic/hypnotics (predominantly benzodiazepines) – are prescribed (Pitkala et al., 2015; Royal Australian and New Zealand College of Psychiatrists (RANZCP), 2016; Royal Australian College of General Practitioners, 2015; Snowdon et al., 2011; Zuidema et al., 2015). Antipsychotics are often used in RACFs to manage BPSD despite modest evidence for effectiveness, alongside substantial adverse effects such as falls, stroke, cardiovascular events and death (Maher et al., 2011). Similarly, benzodiazepine prescribing to manage sleep disturbance, anxiety and agitation in older people is problematic given adverse outcomes of falls, and evidence of increased rates of pneumonia and dementia (Glass et al., 2005; Islam et al., 2016; Taipale et al., 2017). Furthermore, Boyce et al.’s (2012) review of the effectiveness of antidepressants in nursing home residents concluded that the limited evidence available suggested that they confer only a modest response; yet, use in older people is associated with increased risk of falls, stroke, hyponatraemia and seizures (Coupland et al., 2011).
Inappropriate and high rates of psychotropic medication use in Australian RACFs have been reported for over 20 years (Snowdon et al., 2011). The issue first came to national prominence in 1995 with Snowdon et al.’s (1995) prevalence study of 50 Sydney facilities, revealing that a third of residents were taking benzodiazepines daily, alongside high rates of ‘pro re nata’ (prn) or ‘as required’ prescribing; rates described as ‘among the highest reported from geriatric institutions around the world’. This finding resulted in extensive media attention and a dedicated State Ministerial Taskforce enquiry (NSW Health, 1997). Snowdon et al. (2011) repeated their prevalence study on three occasions from 1998 to 2009 in similar cohorts of RACFs in central Sydney, observing a dramatic reduction in benzodiazepine prescribing over the ensuing 15 years, but a rebound to previously high levels of antipsychotic use (28% of residents).
Since 2010, further research and continued media focus on psychotropic use in residential aged care has resulted in two Federal Ministerial Roundtables, a Senate Committee inquiry and a dedicated report on psychotropic medication in people with dementia, commissioned by Alzheimer’s Australia (Peisah and Skladzien, 2014; Senate Community Affairs Committees for Inquiry and Report, 2014; Snowdon et al., 2011; Westbury et al., 2010b). In addition, several guidelines to promote appropriate use of psychotropic medication in older people have been released (NSW Health, 2006; RANZCP, 2016; Royal Australian College of General Practitioners, 2015), along with tightened Pharmaceutical Benefits Scheme (PBS) restrictions for risperidone, the only antipsychotic subsidised for BPSD in Australia (Department of Health, 2017b). The utilisation of quetiapine 25 mg was also restricted when repeat authorisations were removed from PBS subsidised prescriptions in January 2014 (Department of Health, 2017c).
In response to the recent focus on risks associated with antipsychotic and benzodiazepine treatment, some international researchers suggest that these medications are now being substituted by alternative psychotropic agents, such as sedating antidepressants and anticonvulsants, observing increases in prevalence of their use (Bourgeois et al., 2012; Pitkala et al., 2015; Vasudev et al., 2015). However, not only do these substitutes have a limited evidence base for ‘off-label’ indications, such as agitation in dementia or insomnia, they are associated with their own significant adverse effects of falls, infections and gastrointestinal irritation (Bloom et al., 2009; Farina et al., 2017).
Little is known about current psychotropic utilisation in Australian RACFs and whether professional guidelines, and the considerable media and political attention devoted to this issue over the last 5 years, have impacted use. Furthermore, much of the research on psychotropic use in Australian RACFs has been conducted in central Sydney (Snowdon et al., 2011) exclusively. The patterns of use in a region in one large capital city may not be representative of other areas of the country. Consequently, the aim of this study was to provide a comprehensive analysis of current psychotropic use in a large national sample of RACFs. A secondary aim was to seek associations between psychotropic use and the characteristics of State, rurality and facility size.
Methods
Sample
The data for this retrospective, cross-sectional study were derived from the ‘Reducing Use of Sedatives’ (RedUSe) expansion project, a federally funded initiative intended to promote the appropriate use of antipsychotics and benzodiazepines in Australian RACFs (Westbury et al., 2014). ‘RedUSe’ was initially trialled as a controlled trial in 2008/2009 in Tasmania and was subsequently funded for national expansion and delivered between April 2014 and April 2016 to 150 RACFs distributed throughout all six States of Australia and the Australian Capital Territory (ACT) (Westbury et al., 2010a, 2014). RedUSe is a multi-strategic interdisciplinary intervention, comprising a structured 6-month programme involving a cycle of audits, education and sedative review (Westbury et al., 2010a). Psychotropic prescribing data for each resident audited for the baseline measure between April 2014 and October 2015 were analysed for this study.
Cohort selection
Recruiting involved a combination of approaches, as a heterogeneous sample comprising residents from RACFs of various sizes, locations, States and from different organisations, was sought. Initially, two large national nursing facility organisational groups nominated facilities to be involved. Two Aged Care advocacy bodies assisted in the recruitment of smaller organisations and independent RACFs by featuring ‘RedUSe’ in industry journals, resulting in over 300 expressions of interest from facilities. Five RACFs were also directly approached to participate by the researchers.
Facilities with less than 29 residents or from remote locations and those located in the Northern Territory were excluded for logistical reasons. Furthermore, RACFs that specialised in psychogeriatric management were excluded as they had a disproportionate use of psychotropic medication and visiting old age psychiatrists. After exclusions were applied, RACFs were formally invited to participate. Facilities were then purposely selected to ensure a stratified national representative sample was obtained. Recruiting continued until signed consent was gained from the recruitment target of 150 RACFs. Figure 1 outlines the RACF sample selection process for the RedUSe intervention. The overall final sample of residents was compared to Federal Government Australian Institute of Health and Welfare (AIHW) Aged Care 2014/2015 statistical data to assess representativeness (AIHW, 2016).
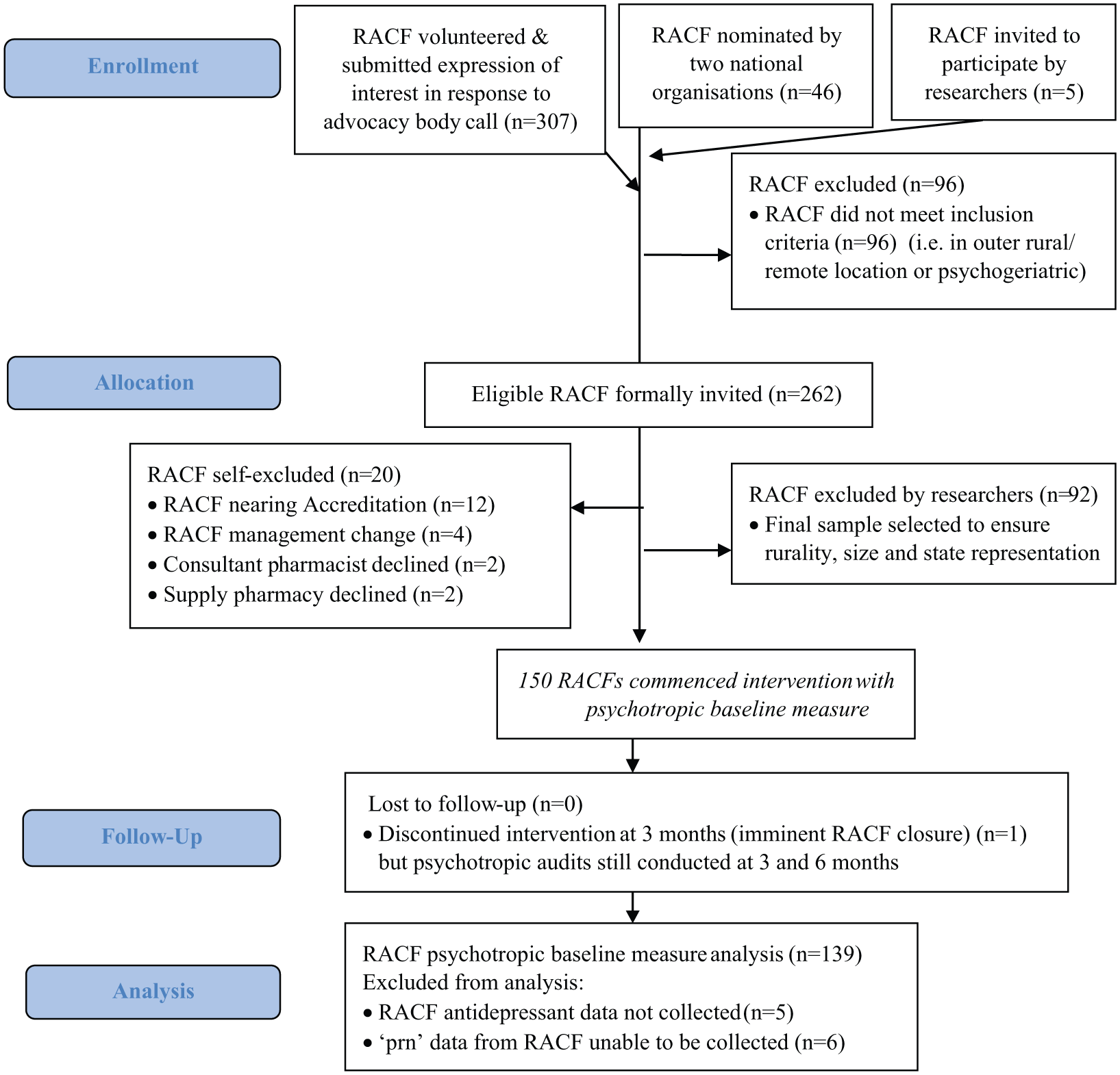
RACF selection flow chart.
Data collection process
Most Australian RACFs obtain their medications from community pharmacies that utilise commercial computerised medication packing systems (e.g. Webstercare©, MPS© and FRED©) to record and pack each resident’s medications into separate blister packs or sachets. Prescribing data from these systems was extracted via a custom-made website and client programme and then securely sent to a webserver (Ling et al., 2017). All community pharmacies supplying the 150 participant RACFs consented to have their medication packing data accessed. Each resident’s prescribing record on the ‘RedUSe’ website was then checked and validated by a trained ‘champion nurse’ at each home. Residents in respite care and those receiving end-stage palliative care were excluded from analysis. Those residents self-administering medication had their prescribing data manually added to the database. Once validated by the champion nurse, all prescribing data were then de-identified and re-checked by researchers for missing data or spurious results. Once this additional checking process was performed and any necessary corrections made, the prescribing data were aggregated to produce individual RACF psychotropic audit reports as a ‘point-prevalence’ snapshot.
Outcome measures
For each resident, the RedUSe website captured all prescribing data, including agent, dose and frequency (Ling et al., 2017). The website also distinguished between medications administered on a regular basis (i.e. a documented regular sequence of administration) and ‘prn’. Medications were classified according to the World Health Organization (WHO) Anatomical Therapeutic Chemical (ATC) code (WHO, 2016). The psychotropics evaluated were antipsychotics (ATC code: N05A, excluding lithium (N05AN) and prochlorperazine (N05AB04)), anxiolytics (N05B), hypnotics (N05C), antidepressants (N06A), phenytoin (N03AB), carbamazepine (N03AF01), clonazepam (N03AE01) and sodium valproate (N03AG01). The utilisation of cholinesterase inhibitors (N06DA) and memantine (N06DX) was also assessed. To obtain an indication of the average dosages of psychotropic medications taken, the mean daily dosage (mDD) for frequently prescribed agents was calculated and compared to the WHO defined daily dose (DDD), which is the assumed average maintenance dose per day for a drug used for its main indication in adults (WHO, 2016). The RACF variables collected were (1) facility size, based on the number of residents (Small: ⩽60 residents, Medium: 61–90 residents, Large: 91–120 residents and Very large: ⩾121 residents), (2) State and (3) rurality according to the Australian Statistical Geographical Standard (Department of Health, 2017a).
Statistical analyses
Pearson’s chi-square test of independence were used to compare the distribution of baseline characteristics of the RedUSe resident sample to the expected distribution based on AIHW aged care data on resident characteristics during 2014/2015. The prevalence of use of each psychotropic class was expressed using the percentage of residents, with confidence intervals. Negative binomial regression analysis was used to study variation in the proportion of residents taking regular antipsychotics, benzodiazepines and antidepressants as a function of State, rurality and home size. Results are presented as incidence rate ratios and adjusted prevalence rates. Queensland was chosen as the reference State because it had the highest number of residents. The goodness of fit of the final model was assessed by graphical examination of goodness-of-fit residuals and standardised residuals. All statistical analyses were completed using R (R-3.3.2 for Windows) (The R Foundation, 2017).
Ethical approval
Ethical approval was obtained from the Human Research Ethics Committee (Tasmania) Network (reference, H0013545). Individual consent was not required from each resident as their data were fully de-identified, with only prescribing information collected. Routine psychotropic audits are endorsed in RACFs as part of the federally funded Quality Use of Medicines (QUM) programme (Pharmaceutical Society of Australia, 2011). Consent to participate in this study was obtained from each of the 150 RACFs, community pharmacies supplying medication to the RACF and consultant pharmacists.
Results
A full data set of psychotropic prescribing information was available for 139 (93%) of the 150 RACFs, resulting in a total sample of 11,368 residents. Data on antidepressant use were not available from five RACFs; likewise, ‘prn’ data were unavailable in six of the RACFs due to data extraction difficulties. The 11 RACFs not included were from South Australia (SA; 5), Victoria (VIC; 3), New South Wales (NSW; 2) and Queensland (QLD; 1). The number of RACFs and residents in each State is shown in Figure 2. Facility size ranged from 29 to 171 residents (mean, 81.8 residents; SD, 31.6). In all, 98 (71%) of the RACFs were situated in a ‘major city’ (RA1), 35 (25%) were classified as ‘inner regional’ (RA2) and 6 (4%) were located in ‘outer regional’ (RA3) areas (Department of Health, 2017c). The majority of the RACFs (82%) were part of an organisational group and 18% of the facilities operated independently.
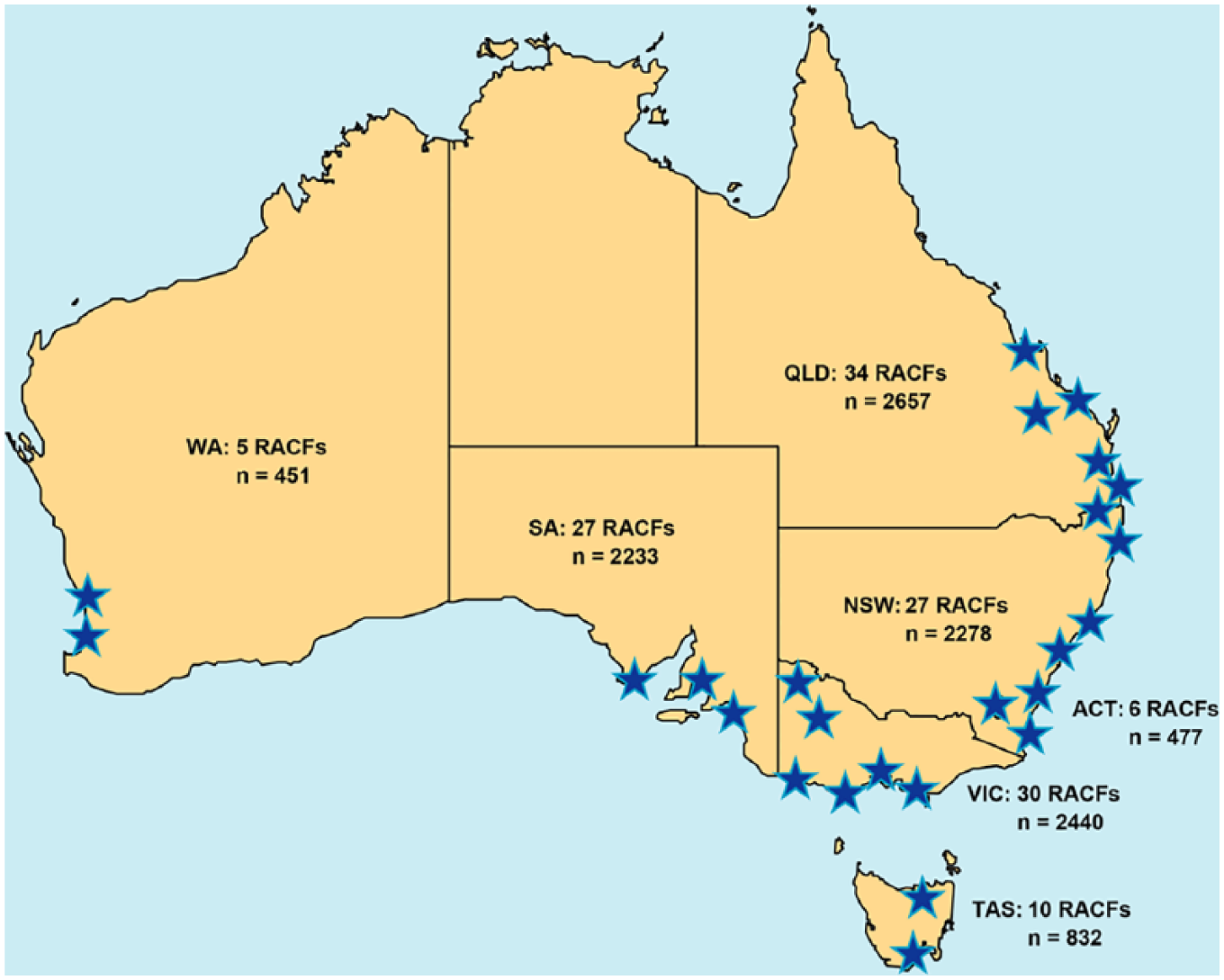
RACF and resident state distribution.
When our sample of residents was compared to AIHW 2014/2015 National Aged Care Data, significant differences were observed, although these were relatively small in magnitude. The RACF size was larger than the national average, fewer outer regional RACFs were represented and the State distribution of RACFs differed (Table 1). A lower proportion of residents resided in NSW and WA in our sample, with a higher proportion of residents from SA, Tasmania and the ACT (AIHW, 2016).
Baseline characteristic comparison between AIHW data and the study sample.
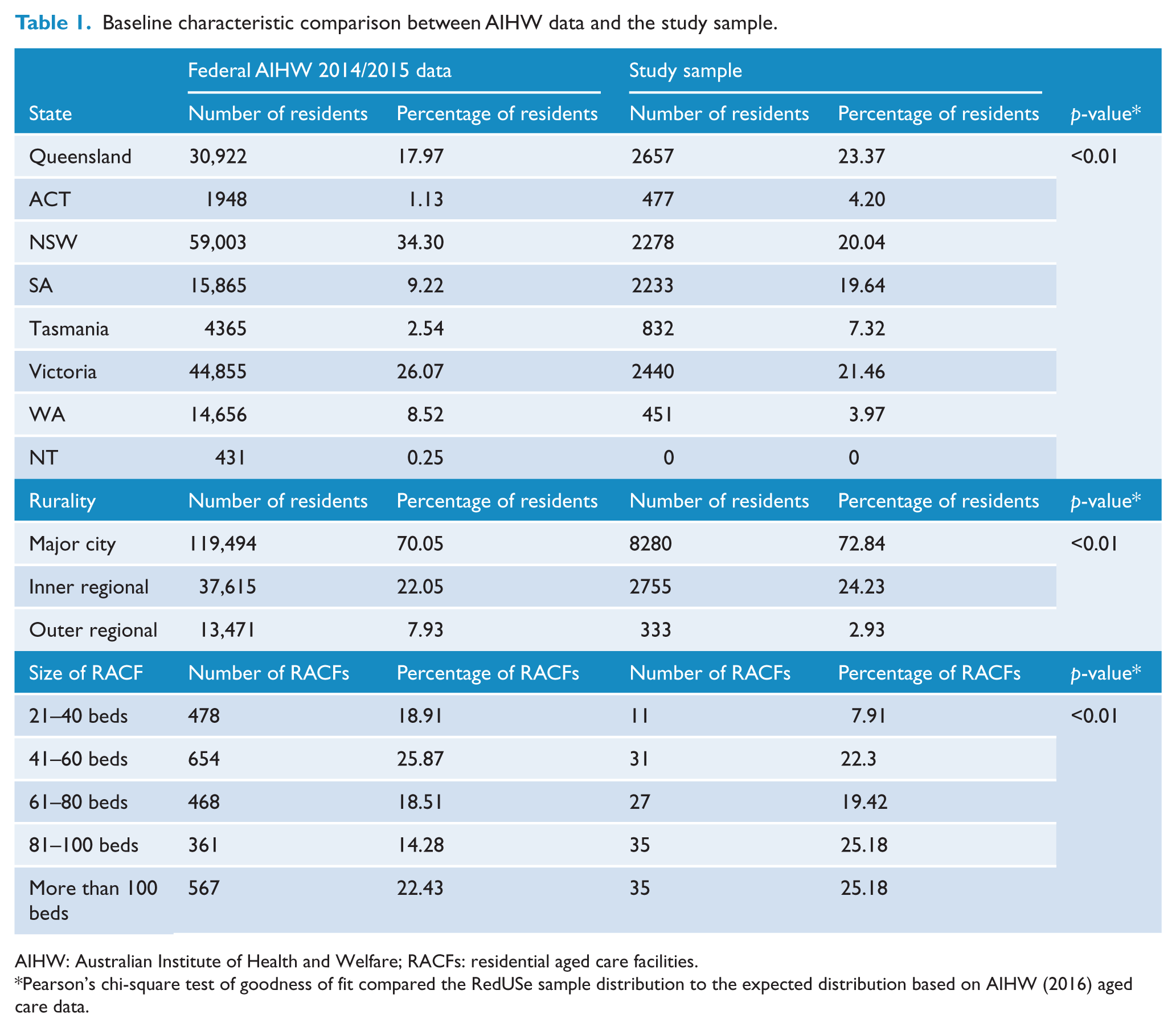
AIHW: Australian Institute of Health and Welfare; RACFs: residential aged care facilities.
Pearson’s chi-square test of goodness of fit compared the RedUSe sample distribution to the expected distribution based on AIHW (2016) aged care data.
In terms of regular psychotropic use, nearly two-thirds (61.2%) of all residents were taking an antipsychotic, anxiolytic/hypnotic or antidepressant medication, or combinations of these agents. Over one-third (37%) of the sample were taking an antipsychotic and/or a benzodiazepine every day. The use of two or more psychotropics was common, with a quarter of all residents (23%) taking two or more agents concurrently. Notably, almost a third of those residents taking a regular antipsychotic (30%) were also taking benzodiazepines daily.
Specifically, 21.8% of residents (95% confidence interval [CI] = [21.1, 22.6]) were administered antipsychotics, 41.4% (95% CI = [40.5, 42.3]) antidepressants and 21.6% (95% CI = [20.8, 22.4]) benzodiazepines on a regularly charted basis. Atypical agents constituted the majority of antipsychotic use (93%), with risperidone accounting for half of all antipsychotic prescribing (n = 1291, 11.4% of residents). In all, 12% (95% CI = [11.4, 12.6]) of residents were taking anxiolytics daily, whereas 11.6% (95% CI = [11.0, 12.2]) were administered hypnotics nightly, with only 26 residents in total taking Z-drugs (i.e. zolpidem and zopiclone). The mDD for all antipsychotic and benzodiazepine agents (aside from nitrazepam) were well below WHO DDDs. A comprehensive breakdown of psychotropic prevalence, alongside mDDs, is shown in Table 2.
Psychotropic medication utilisation in Australian RACFs (n = 11,368 residents).
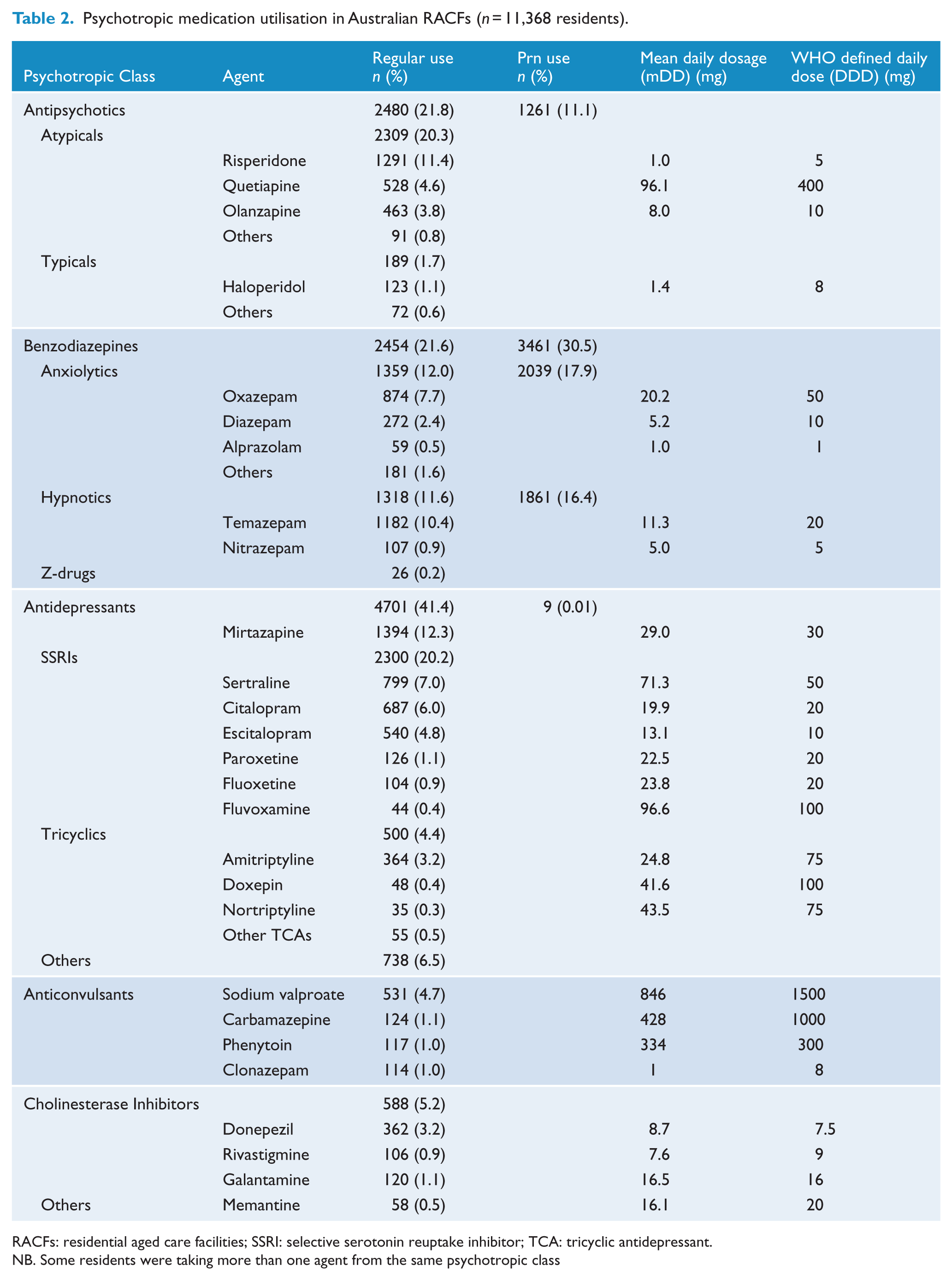
RACFs: residential aged care facilities; SSRI: selective serotonin reuptake inhibitor; TCA: tricyclic antidepressant.
NB. Some residents were taking more than one agent from the same psychotropic class
The most commonly prescribed antidepressant was mirtazapine (n = 1394, 12.3%), followed by citalopram/escitalopram (10.8%), sertraline (6.9%) and tricyclic antidepressants (4.4%). Other psychotropic agents prescribed at significant rates included sodium valproate (n = 531, 4.7%) and the cholinesterase inhibitors (n = 587, 5.2%), while only 58 (0.5%) residents were taking memantine. The majority of selective serotonin reuptake inhibitor (SSRI) antidepressant mDDs exceeded recommended WHO DDDs. Conversely, anticonvulsant and tricyclic antidepressant mDDs were considerably lower than WHO DDDs (Table 2).
A high prevalence of ‘prn’ prescribing was observed. A total of 1261 residents (11.1%) were prescribed ‘prn’ antipsychotics and almost a third of all residents (30.5%) were charted for ‘prn’ benzodiazepines, with anxiolytic ‘prn’ prescribing at 17.9% being slightly higher than hypnotic ‘prn’ prescribing (16.4%). Approximately half of residents prescribed regular doses of benzodiazepines were also prescribed these agents on a ‘prn’ basis (n = 1150 or 47% of regular benzodiazepine users). Similarly, 29% (n = 724) of regular antipsychotic users were also charted for additional ‘prn’ doses. With both regular and ‘prn’ prevalence taken into account, more than half of the residents (n = 6155 or 54.1%) were prescribed antipsychotic and/or benzodiazepine agents.
The distribution of regular psychotropic administration according to State, rurality and RACF size is shown in Table 3. Multivariate analysis indicated that State, but not rurality or RACF size, was an independent predictor of both benzodiazepine and antidepressant use as shown in Table 4. Benzodiazepine prevalence was 61% less (95% CI = [46, 72]) and 30% less (95% CI = [18, 40]) in the ACT and NSW, respectively, but 16% more (95% CI = [1, 34]) in SA as compared to QLD RACFs, after adjustment for rurality and size of RACF (Figure 3(A)). Similarly, antidepressant prevalence was 24% less (95% CI = [8, 37]) and 15% less (95% CI = [6, 24]) in the ACT and NSW, respectively, as compared to residents in QLD RACFs, after adjustment for rurality and size of RACF. Rurality was also an independent predictor of antidepressant use, with 27% (95% CI = [8, 42]) lower use in outer regional RACFs as compared to facilities in major cities, after adjustment for size and State location of facility (Table 4). State, rurality or RACF size were not significantly associated with antipsychotic prevalence (Figure 3(B)).
Summary data of psychotropic use by State, Rurality and RACF size.
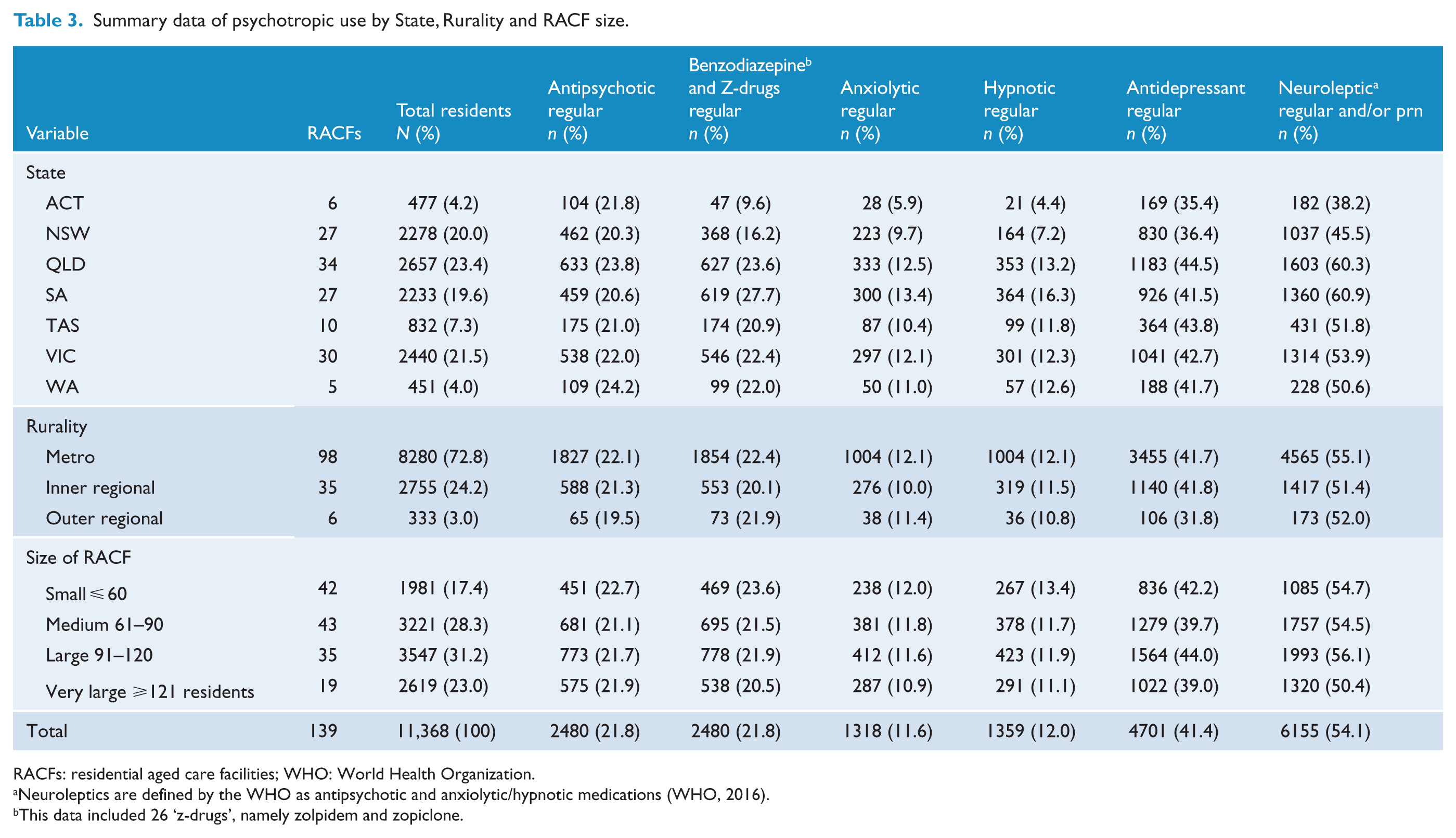
RACFs: residential aged care facilities; WHO: World Health Organization.
Neuroleptics are defined by the WHO as antipsychotic and anxiolytic/hypnotic medications (WHO, 2016).
This data included 26 ‘z-drugs’, namely zolpidem and zopiclone.
Predictors of psychotropic class prevalence (multivariate analysis). a
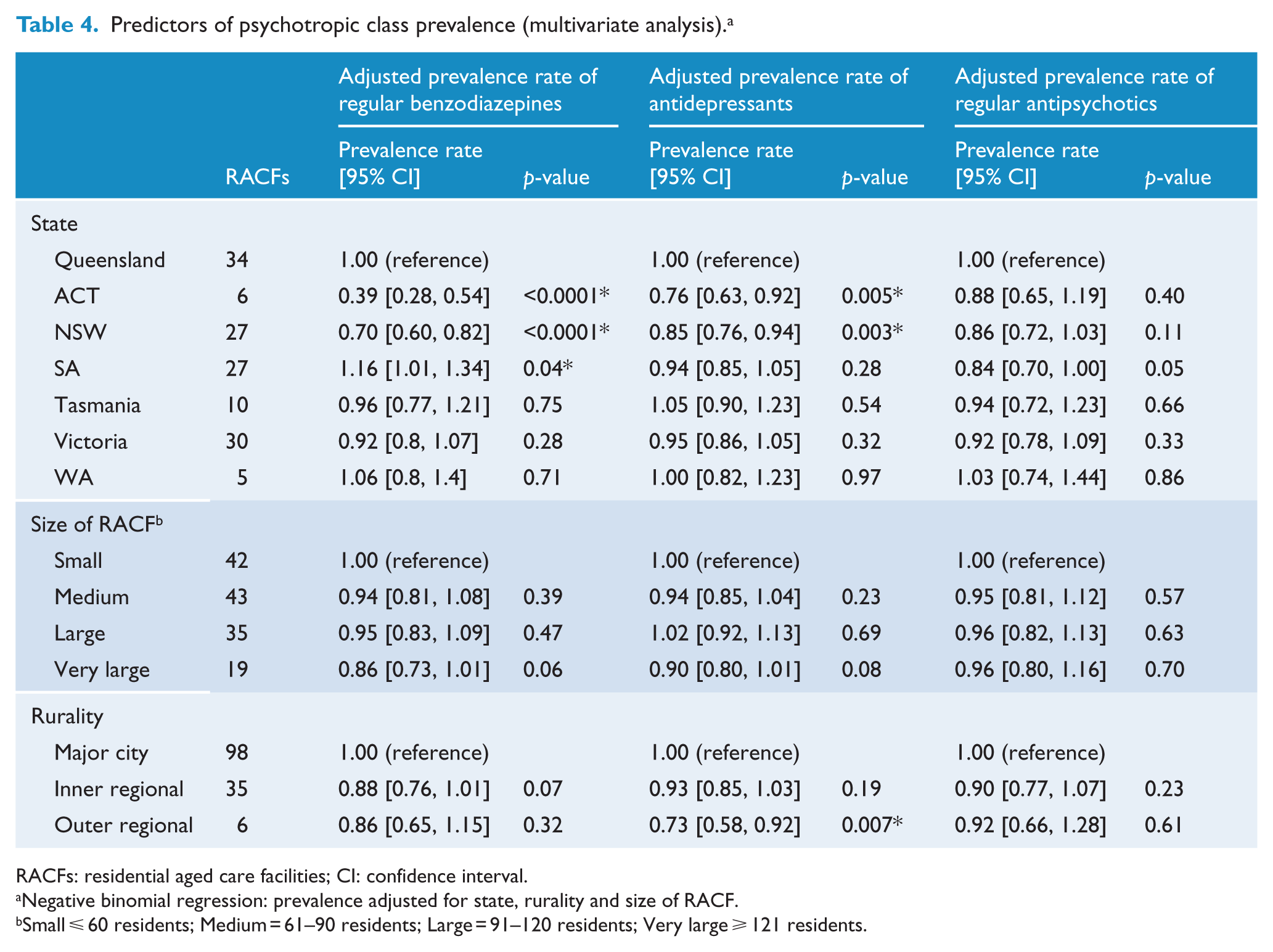
RACFs: residential aged care facilities; CI: confidence interval.
Negative binomial regression: prevalence adjusted for state, rurality and size of RACF.
Small ⩽ 60 residents; Medium = 61–90 residents; Large = 91–120 residents; Very large ⩾ 121 residents.
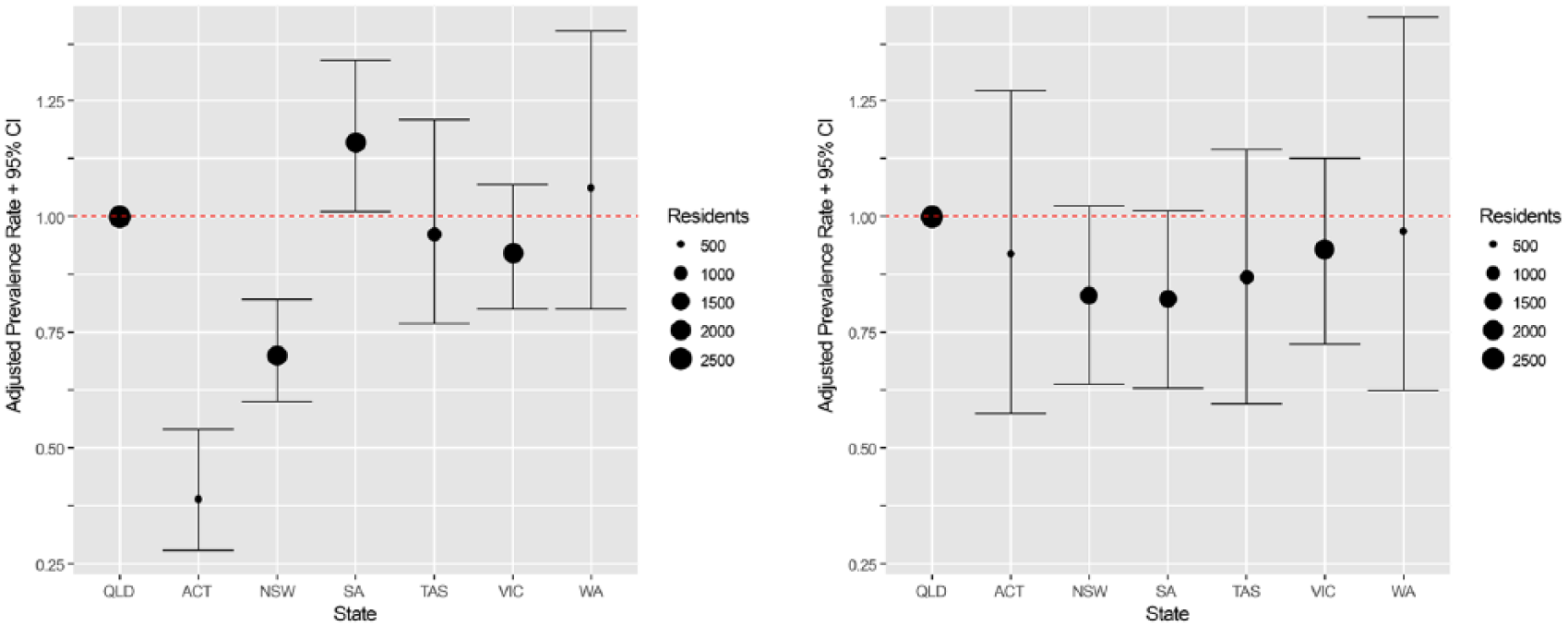
(A) Adjusted prevalence rate of benzodiazepine use by State and (B) adjusted prevalence rate of antipsychotic use by State.
Discussion
The pattern of psychotropic prescribing in RACFs observed in this study differs from that previously reported in Australia post-2010 (Snowdon et al., 2011; Westbury and Peterson, 2013). Notably, the prevalence of regular antipsychotic use is lower, a trend also observed internationally, and attributed to the release of guidelines, safety warnings and tightened prescribing restrictions (Pitkala et al., 2015; Vasudev et al., 2015). The regular antipsychotic prevalence (21.8%) in Australia is remarkably similar to rates recorded using large databases from the United States (22.7%) (Department of Health and Human Services, 2016) and England (21.0%) (Szczepura et al., 2016) in the same time frame. Yet, although the regular use of antipsychotics appears to have fallen in Australian residential aged care, the frequency of ‘prn’ antipsychotic prescribing has risen markedly and is the highest reported to date in Australia (Snowdon et al., 2011; Westbury et al., 2010b). Furthermore, the prevalence of both regular and prn benzodiazepine use is also much higher than that reported in a series of prevalence studies conducted in Sydney RACFs since 2009 (Snowdon et al., 2011), with use in South Australian RACFs significantly higher than in all other Australian states. The finding that over half of all residents were prescribed antipsychotics and/or benzodiazepines either on a regular or ‘prn’ basis, often concurrently, is concerning and demonstrates a continued reliance on pharmacological treatment to manage common behavioural and psychological symptoms encountered in this setting.
The observed high rates of benzodiazepine, sedating antidepressant and anticonvulsant prescribing, at 22%, 17% and 5% of residents, respectively, in conjunction with the decline in antipsychotic use, is consistent with an international trend of regularly administered antipsychotics being substituted by other agents with sedating properties (Pitkala et al., 2015; Vasudev et al., 2015). The use of low doses of benzodiazepines, anticonvulsants and antidepressants for behavioural symptoms in RACF residents has been reported elsewhere despite limited evidence to justify this practice (Pitkala et al., 2015; Tampi and Tampi, 2014; Vasudev et al., 2015). Tampi and Tampi’s (2014) systematic review evaluating benzodiazepine use to manage BPSD could only identify five small randomised controlled trials, concluding that available data did not support the routine use of these agents for this indication. In terms of antidepressant use, a recent review concluded ‘there is little evidence of the therapeutic value of using antidepressants in dementia, whatever the indication’ and also highlighted the high level of adverse events experienced in this cohort (Farina et al., 2017). Similarly, anticonvulsants, notably sodium valproate, have been judged ineffective for the treatment of agitation in dementia (Lonergan and Luxenberg, 2009).
Sedating antidepressants and other psychotropic agents are also prescribed off-licence for their hypnotic effects. Bourgeois et al. (2012) reported that over a quarter of prescribed antidepressants in a substantial sample of Belgian nursing home residents were not actually used to treat depression, with the majority of off-licence use being for insomnia. Over 16% of our resident sample were prescribed sedating antidepressants, mostly at doses significantly lower than those recommended for depression at night, which suggests these agents are also being utilised in Australian RACFs for their night-time sedating effects. Evidence-based recommendations stress there is no systematic evidence for the effectiveness of antidepressants or anticonvulsants when used off-label for the treatment of insomnia and consistently warn that the risks of use outweigh the benefits (Bloom et al., 2009; McMillan et al., 2013; Tiller, 2003). It should be acknowledged that residents taking amitriptyline (3% of residents) and carbamazepine (1%) may have been prescribed these agents for other conditions, such as neuropathic pain or, in the case of amitriptyline, urinary incontinence.
Substitute psychotropic agents are also associated with their own risks. Mirtazapine, for example, the most popularly prescribed antidepressant agent in our resident cohort, can cause daytime drowsiness, dizziness and weight gain and, in a large cohort study examining antidepressant use in older people, its use was associated with falls and stroke (Coupland et al., 2011). An alternative pharmacological option recommended for BPSD is cholinesterase inhibitor treatment (NSW Health, 2006; RANZCP, 2016); however, the use of these agents in this study (5%) was minimal in comparison to usage rates reported internationally (e.g. 28% in Norway; Pitkala et al., 2015), possibly due to historical PBS prescribing restrictions.
Aside from the use of substitute agents, the increased rate of ‘prn’ prescribing of antipsychotics and benzodiazepines observed in this study is concerning for several reasons. First, a recent study evaluating the risk of falls in RACF residents found that occasional ‘prn’ prescribing of psychotropic agents was still associated with a significantly higher risk of falling in older people. More concerningly, the study concluded that the ‘prn’ use of benzodiazepines conferred a greater risk of falling than the risk observed with the regular use of these agents, a finding the authors theorised was due to regular benzodiazepine use resulting in habituation (Cox et al., 2016). This means, in effect, that the practice of prescribing benzodiazepines ‘prn’, with the intention of reducing adverse effects, may inadvertently increase the risk of harm. In addition, injudicious ‘prn’ charting can lead to polypharmacy, drug interactions and total drug doses exceeding recommended maximum daily doses (Stokes et al., 2004). The risk of unintentional ‘overdosing’ is high as many residents were prescribed both regular and top-up ‘prn’ doses of antipsychotics and benzodiazepines. Furthermore, unclear instructions on the frequency of dosing and indication(s) for use increase the likelihood of inappropriate drug use as RACF nursing staff, often with limited medication knowledge, ultimately decide whether to administer prn charted medication or not (Dorks et al., 2016).
This study is the first to compare RACF psychotropic use in different regions of Australia. The rates of regular antipsychotic use in each State and the ACT were remarkably consistent. However, benzodiazepine and antidepressant prevalence were both significantly lower in NSW and the ACT; findings that mirror those of the Australian Commission on Safety and Quality in Healthcare (ACSQHC) (ACSQHC and National Health Performance Authority, 2015). The lower use of these agents may be attributable to NSW Health guidelines on psychotropic use and leadership in this area (NSW Health, 2006). In contrast, the prevalence of regular benzodiazepine use was significantly higher in RACFs in SA (at 28%), again aligning with ACSQHC data (ACSQHC, 2015) but also with the rate of use (25%) reported in a recent SA-based study (National Health Performance Authority, 2015; Chen et al., 2016). Reasons behind this higher benzodiazepine utilisation in SA are unknown although it is interesting to note that the RACF use of antipsychotics in this state was the lowest out of all states, which may indicate possible substitution of antipsychotics with benzodiazepines. Another finding that requires further research is why antidepressants were significantly less likely to be prescribed in outer regional RACFs than in urban and inner regional areas.
Strengths
This research has a number of strengths. First, the large national sample of residents enables a comprehensive analysis of Australian RACF psychotropic utilisation. To our knowledge, this is the first study to examine and compare RACF psychotropic use in residents across Australia rather than in a single locality or state. Furthermore, the study allows for a complete examination of each RACF’s psychotropic use due to the rigorous data-collection methodology, the fact that individual resident consent was not required and because exclusion criterion was purposely limited to enable full prescribing data from residents at each RACF to be captured.
Limitations
One limitation to this study is that the sample of RACFs was not random, thus selection bias cannot be excluded. To address this, we strove to ensure that a wide range of RACFs of various sizes, States and localities were recruited. In spite of our efforts, our final sample was statistically different from national AIHW data on resident characteristics during 2014/2015. The state distribution of RACFs was different from the national distribution mainly due to an over-representation of RACFs in South Australia, ACT and Tasmania, and an under-representation of RACFs in NSW and Western Australia. Recruiting NSW RACFs was impacted by concurrent research projects and a large group of Western Australian RACFs withdrew before consent was gained to participate. In addition, the size of our RACFs, at an average of 82 residents, was higher than the national average of 60 residents. Finally, although the proportion of urban and inner regional RACFs was broadly similar to the national distribution, we recruited fewer outer regional RACFs.
Another limitation was that information on how often ‘prn’ medications were actually administered was not collected. Many psychotropic agents may be prescribed on a ‘prn’ basis but then not administered to residents or taken infrequently. This non-administration was demonstrated by Snowdon et al. (2011) in their 2009 study of Sydney RACF residents, which found that 55% of psychotropic agents prescribed on a ‘prn’ basis were never taken. Furthermore, data on the use of non-pharmacological strategies were not collected. Research is required to investigate the extent to which these alternative management options are utilised in RACFs to manage common behavioural and psychological symptoms encountered in this setting. Finally, primarily due to ethical considerations, detailed clinical diagnostic and demographic information on the residents was not obtained. It should be acknowledged that some of the psychotropic use in residents may reflect treatment of a long-standing mental health condition, such as schizophrenia or bipolar disorder.
In summary, the finding that more than half of all RACF residents were charted for an antipsychotic and/or a benzodiazepine is of major concern. Although antipsychotic use in Australian facilities appears to have decreased over the past 5 years, there has been an increase in sedating antidepressant and overall ‘prn’ psychotropic prescribing, suggesting that substitution to other psychotropic agents and practices is occurring. In 2011, a call for action on psychiatric drug prescribing in older Australians was made (Hollingworth et al., 2011); however, it is evident that the issues of high rates and inappropriate use of psychotropic medications in the setting where our most vulnerable older citizens reside remain unresolved. Effective interventions are required to reduce RACF reliance on psychotropic agents, which should include a focus on their review and reduction, and the enhanced promotion of, and access to, non-pharmacological strategies.
Footnotes
Acknowledgements
The authors wish to acknowledge the support of the medication packing software companies; Webstercare, FredHealth, Minfos and MPS Australia. We would also like to sincerely thank the administration, clinical and champion nurses at all participating 150 RACFs and their community pharmacies for their participation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The RedUSe (Reducing Use of Sedatives) project from which this research was derived was funded by the Australian Government Department of Heath as part of the Dementia and Aged Care Service Fund (formerly known as the Aged Care Service Improvement and Healthy Ageing Fund).