
Abstract
Objective:
To examine trends in prescribing psychotropic medications to children and adolescents in Australian primary care from 2011 to 2018.
Method:
A retrospective cohort study examined prescriptions written by general practitioners using MedicineInsight, a large Australian primary care database, covering approximately 9% of all general practitioner practices. Numbers of patients receiving prescriptions for five main classes of psychotropics (antipsychotics, antidepressants, attention deficit hyperactivity disorder medications, anxiolytics, and hypnotics/sedatives [including benzodiazepines and Z-drugs, but excluding melatonin]) were examined annually by age-group (0–4, 5–9, 10–14, 15–18 years). Melatonin was analysed separately.
Results:
The number of patients prescribed any psychotropic increased from 25.6 to 36.2 per 1000 individuals from 2011 to 2018 (average annual increase +4.5%, 95% confidence interval [4.1%, 4.9%]; overall +41.4%). Among the five main classes, the largest annual increase was for attention deficit hyperactivity disorder medications (+9.6%, 95% confidence interval [8.8%, 10.5%]; overall +95.8%), followed by antipsychotics (+6.2%, 95% confidence interval [5.0%, 7.3%]; overall +62.8%) and antidepressants (+4.5%, 95% confidence interval [4.0%, 5.0%]; overall +42.8%). Hypnotic/sedative prescribing decreased on average 6.5% per year (95% confidence interval [–8.0%, –5.0%]; overall −40.2%). Anxiolytic prescribing remained steady. Melatonin prescriptions showed the highest increase of all (+24.7%, 95% confidence interval [23.7%, 25.8%]; overall +606.7%). The largest annual increase in antipsychotic, antidepressant or attention deficit hyperactivity disorder medication prescribing occurred in 10- to 14-year-olds (+7.5%, +6.5% and +10.4%, respectively). The largest point prevalence occurred in 2018 among 15- to 18-year-olds, with 98.5 per 1000 prescribed antidepressants. Antidepressants were more frequently prescribed to females; antipsychotics, attention deficit hyperactivity disorder medications and melatonin more often to males. The most prescribed antipsychotics were risperidone (<15 years) and quetiapine (15- to 18-year-olds). Fluoxetine was the most prescribed antidepressant in those aged 5+ years and amitriptyline in 0- to 4-year-olds.
Conclusion:
General practitioner prescribing of melatonin, antipsychotics, antidepressants and attention deficit hyperactivity disorder medications to under-19-year-olds increased markedly from 2011 to 2018. Although benzodiazepine and Z-drug prescriptions declined, this was offset by a substantial increase in melatonin prescribing.
Introduction
Globally, prescriptions of most classes of psychotropic medications to children and adolescents have been on the rise in recent decades (Bachmann et al., 2016, 2017; Barczyk et al., 2020; Hálfdánarson et al., 2017; Hartz et al., 2016; John et al., 2016; Lagerberg et al., 2019; Pringsheim et al., 2019; Raman et al., 2018; Sarginson et al., 2017). This is despite ongoing debate about the efficacy and safety of psychotropics in young people (Hetrick et al., 2012, 2021; Vitiello et al., 2009), concerns about antidepressant-induced suicidality (Whitely et al., 2020) and evidence of increased risk of adverse events in children compared with adults (Correll et al., 2015).
A recent study found an increase in antipsychotic prescriptions from 2005 to 2014 in 0- to 19-year-olds in 10 of 16 countries, with Australia having the third highest increase (+159%) (Hálfdánarson et al., 2017). Several international studies have also found increases in antidepressant prescribing, ranging from +26% in the United States from 2005 to 2012 (Bachmann et al., 2016), to +78% in New Zealand (NZ) from 2008 to 2016 (Barczyk et al., 2020). In the United Kingdom, general practice antidepressant prescribing to 3- to 17-year-olds from 2006 to 2015 almost doubled, with the most rapid increase evident in 15- to 17-year-olds (Sarginson et al., 2017).
For attention deficit hyperactivity disorder (ADHD) medications, findings are similar. A multi-country analysis of ADHD medication prescriptions from 2005 to 2012 identified increases ranging from 10.7% (United States) to 302.7% (Denmark) (Bachmann et al., 2017). A more recent NZ study found a rise of 41.3% from 2011 to 2016 (Barczyk et al., 2020). In all countries, ADHD prescription rates were highest in 10- to 14-year-olds.
Few studies, however, have examined prescribing of anxiolytics and hypnotics/sedatives, with varying results. Anxiolytic prescribing was stable in Norway (2004–2014) (Hartz et al., 2016), increased 50% in NZ (2008–2016) (Barczyk et al., 2020) and showed an increase only in 15- to 18-year-olds in Wales (2003 to 2011) (John et al., 2015). Hypnotic/sedative prescribing was reported in the same studies. Rates of hypnotic/sedative prescribing were stable in the Welsh study, but increased by 37.5% in the NZ study. The Norwegian study reported substantial increases in prescribing in adolescents only (girls, +238%; boys, +157%), which the authors attributed to increasing use of melatonin (Hartz et al., 2016).
In Australia, the Pharmaceutical Benefits Scheme (PBS) provides government subsidies for approved medications for all Australian citizens and eligible residents. Studies using dispensing data from the PBS have also shown psychotropic medications have been increasingly prescribed to children and adolescents (Drug Utilisation Sub-Committee [DUSC], 2018; Karanges et al., 2014; Morrison et al., 2014). Examining dispensing of antidepressants, antipsychotics and ADHD medications from 2009 to 2012, Karanges et al. (2014) found increases for all ages (>2 years), but the most rapid increase was observed in 10- to 14-year-olds for antidepressants (+35.5%) and antipsychotics (+49.1%). DUSC reports have analysed subsidised antipsychotics for children and adolescents from 2010 to 2012 (Morrison et al., 2014), and stimulant use for all age-groups from 2013 to 2017 (DUSC, 2018). However, PBS datasets only provide information on prescriptions dispensed. They do not provide data on private prescriptions or approved medications not listed on the PBS schedule. PBS data also do not allow an estimation of the number of patients receiving medications.
To our knowledge, no study has explored recent trends for all classes of psychotropics for Australian children and adolescents nor analysed data from general practice, which is the main source of psychotropic prescribing. In 2018–2019, 86.3% of all psychotropics (90.6% of antidepressants, 73.9% of antipsychotics, 91.2% of anxiolytics, 93.0% of hypnotics/sedatives and 18.6% of psychostimulants) were prescribed by general practitioners (GPs) in Australia, with percentages remaining consistent from 2012 to the present (Australian Institute of Health and Welfare [AIHW], 2020: Table PBS.5). An examination of GP prescribing trends is, therefore, essential for a deeper understanding of psychotropic drug use in Australia. Importantly, no recent studies have examined psychotropics prescribing in Australia in 0- to 4-year-olds specifically.
This study examines (1) prescribing trends from 2011 to 2018 for all classes of psychotropic medications for Australian children and adolescents under 19 using a national primary care database of electronic health records, which includes private and PBS-subsidised prescriptions written by GPs; and (2) sociodemographic factors associated with these prescriptions. This study also includes an analysis of prescribing trends for melatonin.
Methods
Study design and data source
A retrospective cohort study was conducted using MedicineInsight (Busingye et al., 2019), a large longitudinal Australian primary care database of electronic health records. MedicineInsight was established in 2011, with core funding from the Australian Government, to improve the quality use of medicines and monitor medication safety. As of June 2020, the database consisted of data from 732 general practices (9.0% of all Australian general practices) and 5199 GPs (NPS MedicineWise, 2020). In participating practices, all data recorded into the clinical information system is automatically transferred to the MedicineInsight data warehouse monthly using a secure third-party extraction tool. To ensure data quality, only general practice sites established for at least 2 years with no interruptions of more than 6 weeks, and a consistent volume of data transactions, are included in analyses. MedicineInsight data are de-identified. Each patient is assigned a unique patient identifier, which allows linking of all the records held in the database, enabling longitudinal analyses.
The database includes both subsidised (PBS) and private prescriptions written by GPs, regardless of whether they are dispensed. It also includes detailed individual-level data on all patient encounters, including diagnoses, medical tests, prescribed drugs and patient sociodemographics. The dataset has been successfully used in recent years to estimate trends in the use of insomnia medications in Australia (Begum et al., 2021).
Study population
This study includes all children and adolescents under 19 who attended a MedicineInsight practice from 2011 to 2018. Only ‘regular patients’ (defined as patients with at least three visits within the current and previous year, and at least one visit in each of those 2 years) were included in the analysis. The final sample included 537,371 unique patients (ranging from 112,997 in 2011 to 336,432 in 2018) attending 539 Australian practices.
Outcomes and covariates
The main outcome was recorded prescriptions of psychotropic medications, analysed in total, separately in five main classes and in subclasses. Melatonin was analysed separately. Numbers of original prescriptions recorded per patient were extracted from the MedicineInsight prescriptions table, using information on medication name and/or active ingredient. The five classes were antipsychotics, antidepressants, ADHD medications, anxiolytics and hypnotics/sedatives, excluding melatonin (Supplementary eTable S1). Supplementary eTable S2 lists current Therapeutic Goods Administration (TGA) drug approvals for psychotropic use in children and adolescents in Australia.
With the exception of the hypnotics/sedatives and ADHD drug classes, the groupings of medications were classified according to the Anatomical Therapeutic Chemical (ATC) classification system (World Health Organization [WHO] Collaborating Centre for Drug Statistics Methodology, 2021). The ADHD medications class included stimulants and non-stimulants (atomoxetine, guanfacine, clonidine, modafinil, armodafinil) used to treat ADHD. The hypnotics/sedatives class excluded melatonin. Although classified as a hypnotic/sedative in the ATC system, melatonin is not a traditional psychotropic and has been classified in some studies as a non-psychotropic (Efron et al., 2017) or neurohormonal drug or chronobiotic (Boafo et al., 2019). International studies have recorded substantial increases in paediatric hypnotic/sedative prescribing when including melatonin in the hypnotics/sedatives class (Barczyk et al., 2020; Hartz et al., 2016). Because of this, and because there are no studies addressing paediatric hypnotic/sedative prescribing in Australian primary care, we chose to analyse it separately. Mood stabilisers were excluded, because they are used extensively for epilepsy and seizures, and it was not possible to distinguish which prescriptions were for psychiatric conditions.
The main drug classes were further divided into subclasses. Antipsychotics were divided into first- and second-generation (atypical); antidepressants were divided into selective serotonin reuptake inhibitors (SSRIs), selective noradrenaline reuptake inhibitors (SNRIs), monoamine oxidase inhibitors (MAOIs), tricyclic antidepressants (TCAs), noradrenaline and specific serotonergic antidepressants (NaSSAs), and other antidepressants. Hypnotics/sedatives included benzodiazepines and Z-drugs (zopiclone and zolpidem).
Patient sociodemographic data were also obtained. Gender was divided into male or female, and age stratified into four groups (0–4, 5–9, 10–14 or 15–18 years), roughly corresponding to infancy/toddler years, childhood, puberty and older adolescence. We used the 0- to 4-year age-group as a proxy for the pre-school period. In most states and territories, children start their preparatory year of school during the year they turn 5 and start formal schooling by age 6 (Australian Curriculum Assessment and Reporting Authority [ACARA], 2019). Socioeconomic position, derived from residential and practice postcodes, was analysed using the Index of Relative Socio-economic Advantage and Disadvantage (IRSAD) divided into quintiles. IRSAD is an indicator that summarises information obtained from census data about the economic and social conditions (i.e. income, education, employment, occupation and housing variables) of people and households within specified geographic areas, with higher scores indicating more advantaged areas (Australian Bureau of Statistics [ABS], 2018a, 2018b). State, rurality (major cities, inner regional, outer regional/remote/very remote) and practice IRSAD quintiles were also included as covariates for adjustment.
Statistical analysis
Prescriptions by age-group for each main drug class, melatonin and the five main psychotropic classes combined were calculated as adjusted annual rates of prescriptions per 1000 patients. Trends in psychotropic prescriptions between 2011 and 2018 were analysed using Poisson regression and reported as average annual changes (percentages) with 95% confidence intervals (CIs), using the practice as cluster, and robust standard errors (Tables 1 and 2).
Trends in prescribing of all psychotropic medications (excluding melatonin) to children and adolescents, according to patient sociodemographics, from 2011 to 2018. a
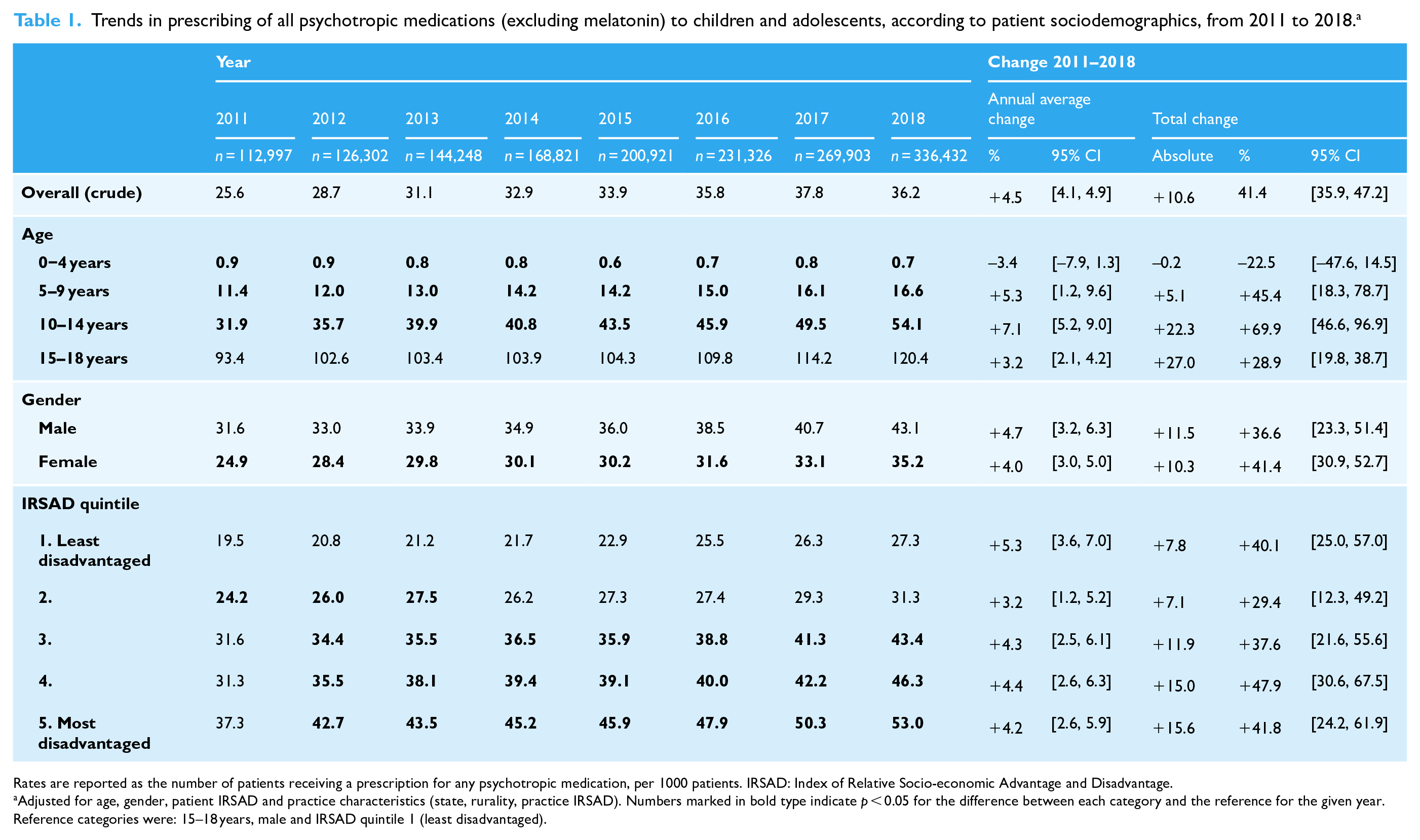
Rates are reported as the number of patients receiving a prescription for any psychotropic medication, per 1000 patients. IRSAD: Index of Relative Socio-economic Advantage and Disadvantage.
Adjusted for age, gender, patient IRSAD and practice characteristics (state, rurality, practice IRSAD). Numbers marked in bold type indicate p < 0.05 for the difference between each category and the reference for the given year. Reference categories were: 15–18 years, male and IRSAD quintile 1 (least disadvantaged).
Trends in prescribing of psychotropic medications to children and adolescents by drug class, from 2011 to 2018.
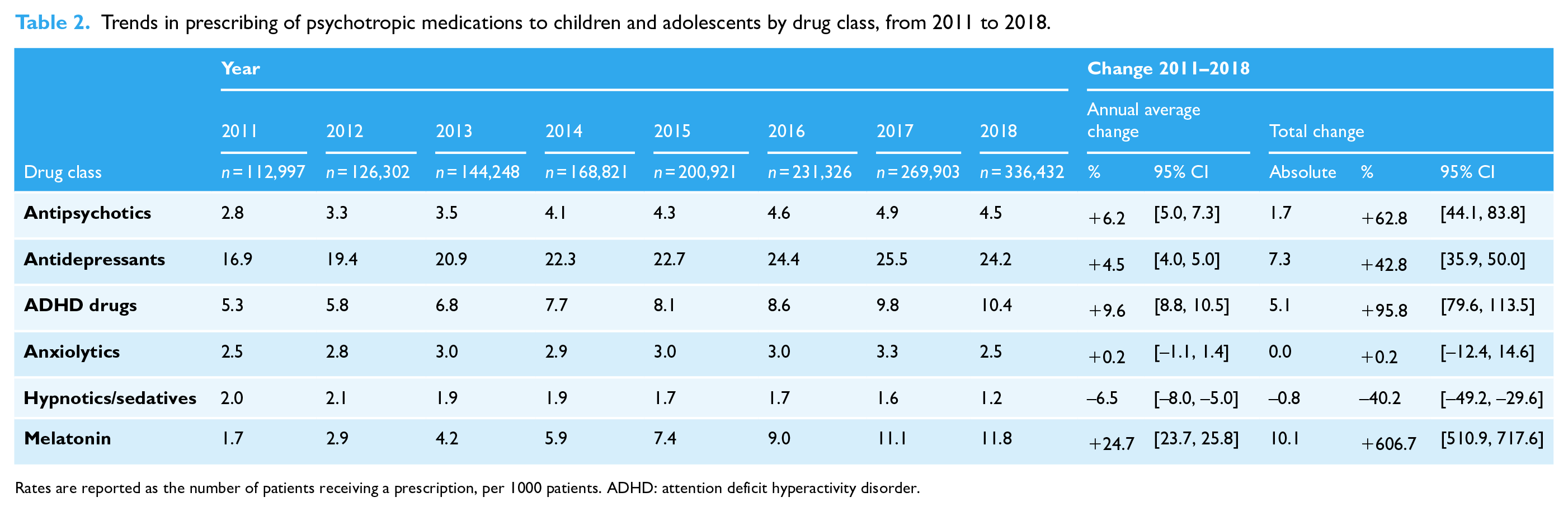
Rates are reported as the number of patients receiving a prescription, per 1000 patients. ADHD: attention deficit hyperactivity disorder.
To explore prescribing in greater detail, tables of prescriptions were created for the year 2018 only, including class and subclass of medications (Table 3) and the most frequently prescribed medications within each class (Table 4).
Number of regular patients prescribed medications by class and subclass in 2018, according to age-groups.
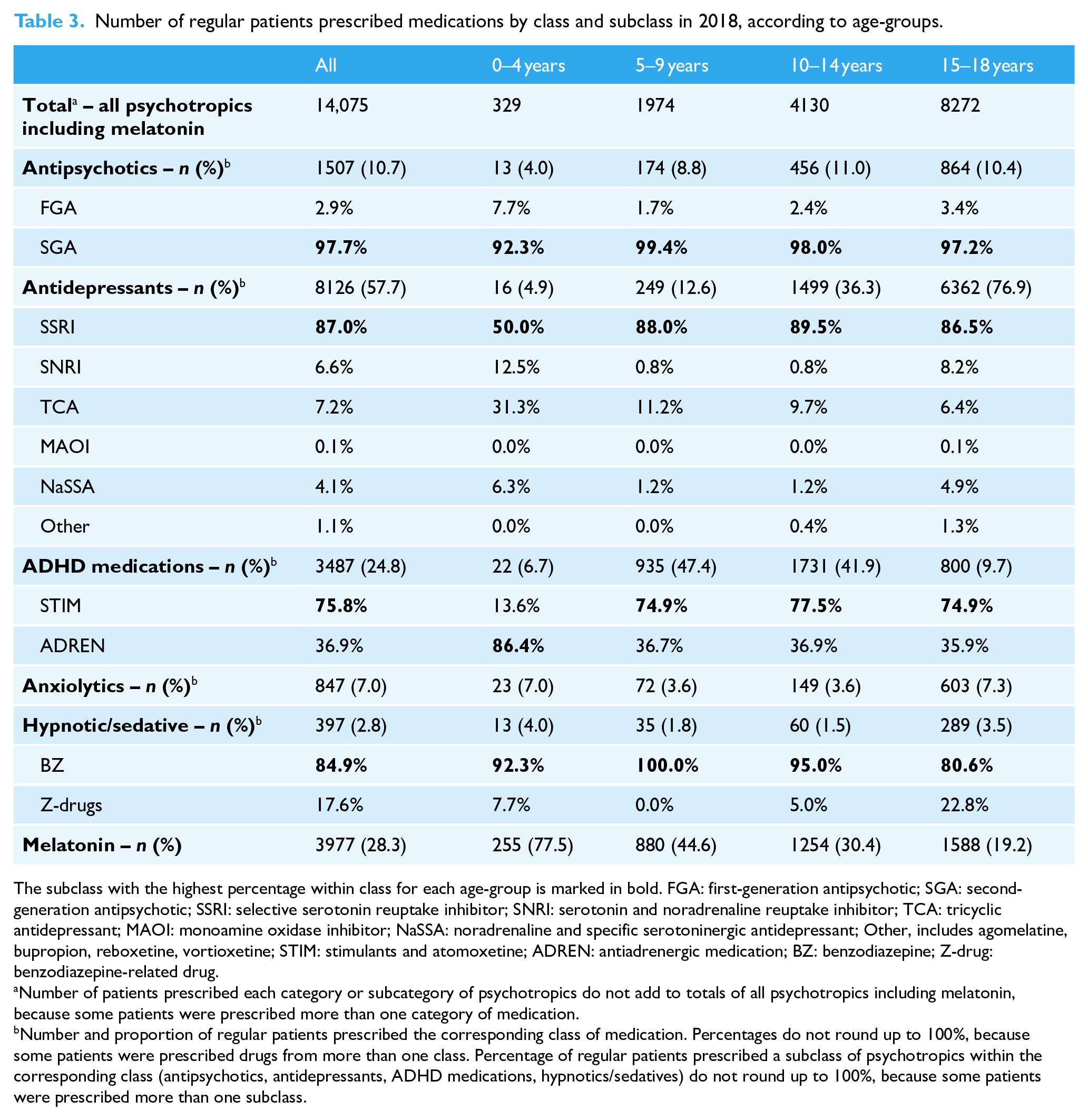
The subclass with the highest percentage within class for each age-group is marked in bold. FGA: first-generation antipsychotic; SGA: second-generation antipsychotic; SSRI: selective serotonin reuptake inhibitor; SNRI: serotonin and noradrenaline reuptake inhibitor; TCA: tricyclic antidepressant; MAOI: monoamine oxidase inhibitor; NaSSA: noradrenaline and specific serotoninergic antidepressant; Other, includes agomelatine, bupropion, reboxetine, vortioxetine; STIM: stimulants and atomoxetine; ADREN: antiadrenergic medication; BZ: benzodiazepine; Z-drug: benzodiazepine-related drug.
Number of patients prescribed each category or subcategory of psychotropics do not add to totals of all psychotropics including melatonin, because some patients were prescribed more than one category of medication.
Number and proportion of regular patients prescribed the corresponding class of medication. Percentages do not round up to 100%, because some patients were prescribed drugs from more than one class. Percentage of regular patients prescribed a subclass of psychotropics within the corresponding class (antipsychotics, antidepressants, ADHD medications, hypnotics/sedatives) do not round up to 100%, because some patients were prescribed more than one subclass.
Most frequently prescribed drugs in 2018 by age-group, a reported as percentage of total patients on each class of drug in each age-group.
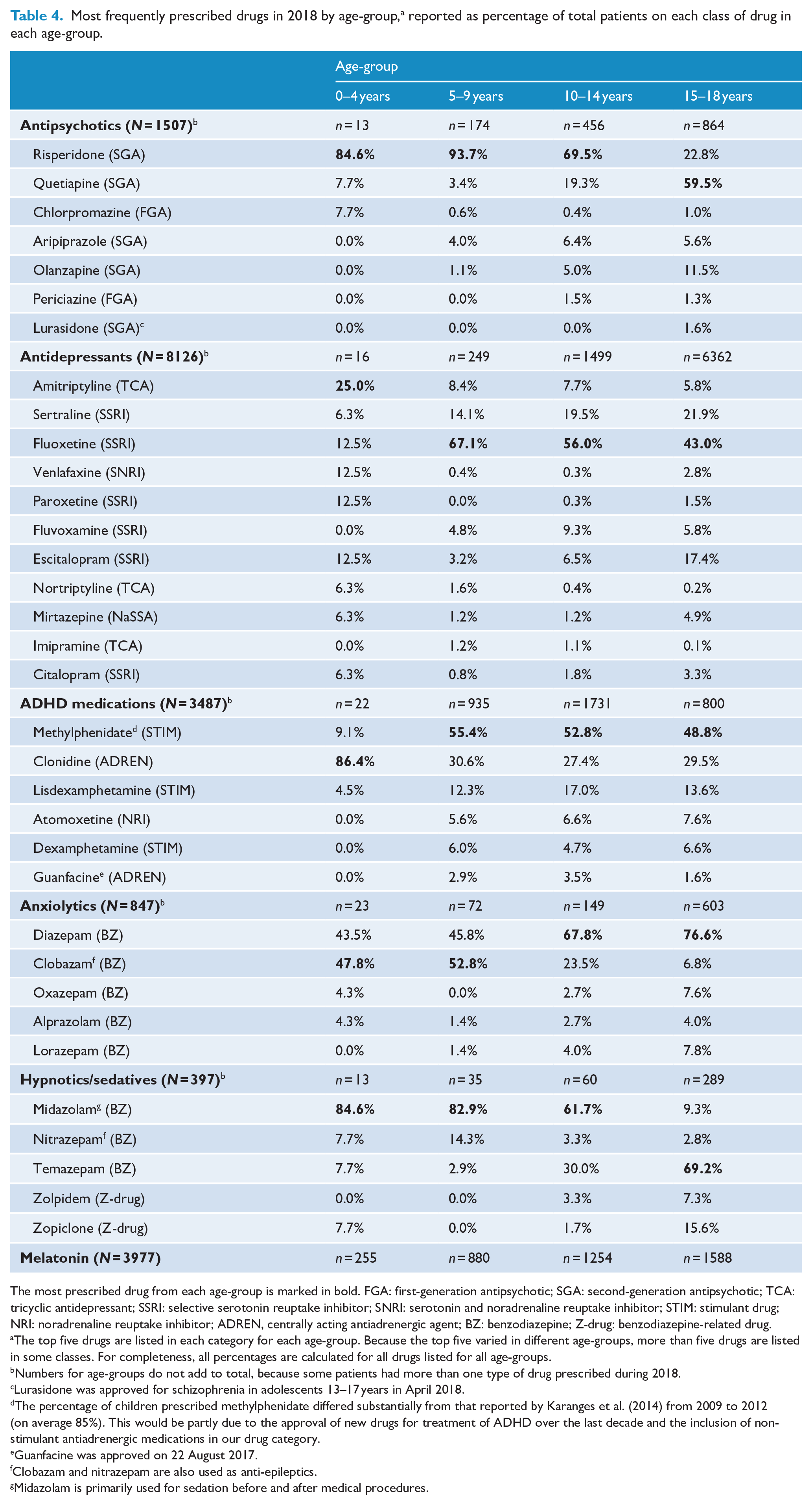
The most prescribed drug from each age-group is marked in bold. FGA: first-generation antipsychotic; SGA: second-generation antipsychotic; TCA: tricyclic antidepressant; SSRI: selective serotonin reuptake inhibitor; SNRI: serotonin and noradrenaline reuptake inhibitor; STIM: stimulant drug; NRI: noradrenaline reuptake inhibitor; ADREN, centrally acting antiadrenergic agent; BZ: benzodiazepine; Z-drug: benzodiazepine-related drug.
The top five drugs are listed in each category for each age-group. Because the top five varied in different age-groups, more than five drugs are listed in some classes. For completeness, all percentages are calculated for all drugs listed for all age-groups.
Numbers for age-groups do not add to total, because some patients had more than one type of drug prescribed during 2018.
Lurasidone was approved for schizophrenia in adolescents 13–17 years in April 2018.
The percentage of children prescribed methylphenidate differed substantially from that reported by Karanges et al. (2014) from 2009 to 2012 (on average 85%). This would be partly due to the approval of new drugs for treatment of ADHD over the last decade and the inclusion of non-stimulant antiadrenergic medications in our drug category.
Guanfacine was approved on 22 August 2017.
Clobazam and nitrazepam are also used as anti-epileptics.
Midazolam is primarily used for sedation before and after medical procedures.
All results were adjusted by age, gender, patient IRSAD quintiles and practice characteristics (state, rurality, practice IRSAD). All analyses were carried out using Stata version 16 (StataCorp, Texas, USA).
Ethics approval
The independent MedicineInsight Data Governance Committee approved the present study (protocol 2019-029), and the Human Research Ethics Committee of the University of Adelaide exempted it from a full ethical review due to the use of non-identifiable data.
Results
The sample included 537,371 patients under 19 years (51.1% females), ranging between 112,997 in 2011 and 336,432 in 2018. These individuals mainly attended practices located in major cities (66.4%), 22.4% in inner regional and 11.3% in outer regional/remote/very remote areas. Participants in higher IRSAD areas were over-represented (30.1% very high [least disadvantaged], 19.0% high, 22.4% middle, 13.4% low and 15.2% very low [most disadvantaged] IRSAD quintiles).
Change over time
The prescription of all psychotropics, excluding melatonin, increased from 25.6 per 1000 patients in 2011 to 36.2 per 1000 in 2018 (average annual increase +4.5%, 95% CI [4.1, 4.9]; overall +41.4%) (Table 1). The prescription rate remained steady at less than 1 per 1000 patients in 0- to 4-year-olds. The highest rate was for those 15–18 years. Except for the 0- to 4-year-olds, prescriptions increased over time, especially among 10- to 14-year-olds (+7.1%, 95% CI [5.2, 9.0]; overall +69.9%). Prescription rates were higher in males, but a similar annual increase was found in both genders. The highest rate in any year was among those in more disadvantaged areas, but the annual increase was similar in all IRSAD quintiles.
The annual trends for each class of drug are reported in Table 2. The highest prescription rate in any year was for antidepressants (ranging from 16.9 per 1000 patients in 2011 to 25.5 per 1000 in 2017). There was an increase in prescriptions for all classes, except anxiolytics, which showed no change, and hypnotics/sedatives, which had a 40.2% decrease between 2011 and 2018. The rate of melatonin prescriptions increased just over 600% between 2011 and 2018 (annual change +24.7%, 95% CI [23.7, 25.8]; overall +606.7%).
Figure 1 and Supplementary eTables S3–S8 illustrate the adjusted trends by sociodemographic characteristics. Antipsychotic and antidepressant prescription rates (Figure 1(a) and (b)) increased only among those 10 years or over; for younger children, these prescriptions remained low. ADHD medication prescriptions (Figure 1(c)) showed a similar annual increase in the three older age-groups, ranging from 8.7% to 10.4% per year, but no change was found in 0- to 4-year-olds. Annual average anxiolytic prescribing declined in 10- to 14-year-olds (−3.7%, 95% CI [−6.8, −0.4]), while overall change was non-significant (−16.0%, 95% CI [−37.7, 13.1]); prescribing remained steady in all other age-groups (Figure 1(d)). Hypnotics/sedatives (Figure 1(e)) were the only medications showing a decrease from 2011 to 2018 (annual change −6.5%, 95% CI [−8.0, −5.0]; overall −40.2%), but the reduction was only evident among those 0–4 years and especially 15–18 years. The decrease in hypnotics/sedatives was driven largely by an annual reduction in prescriptions for nitrazepam (−13.1%, 95% CI [−20.0, −5.5]), temazepam (−8.7%, 95% CI [−10.5, −6.8]) and zolpidem (−14.6%, 95% CI [−19.7, −9.2]; Supplementary eTable S9). Melatonin (Figure 1(f)) was the only medication with an increase in prescription rates across all age-groups (Supplementary eTable S8).
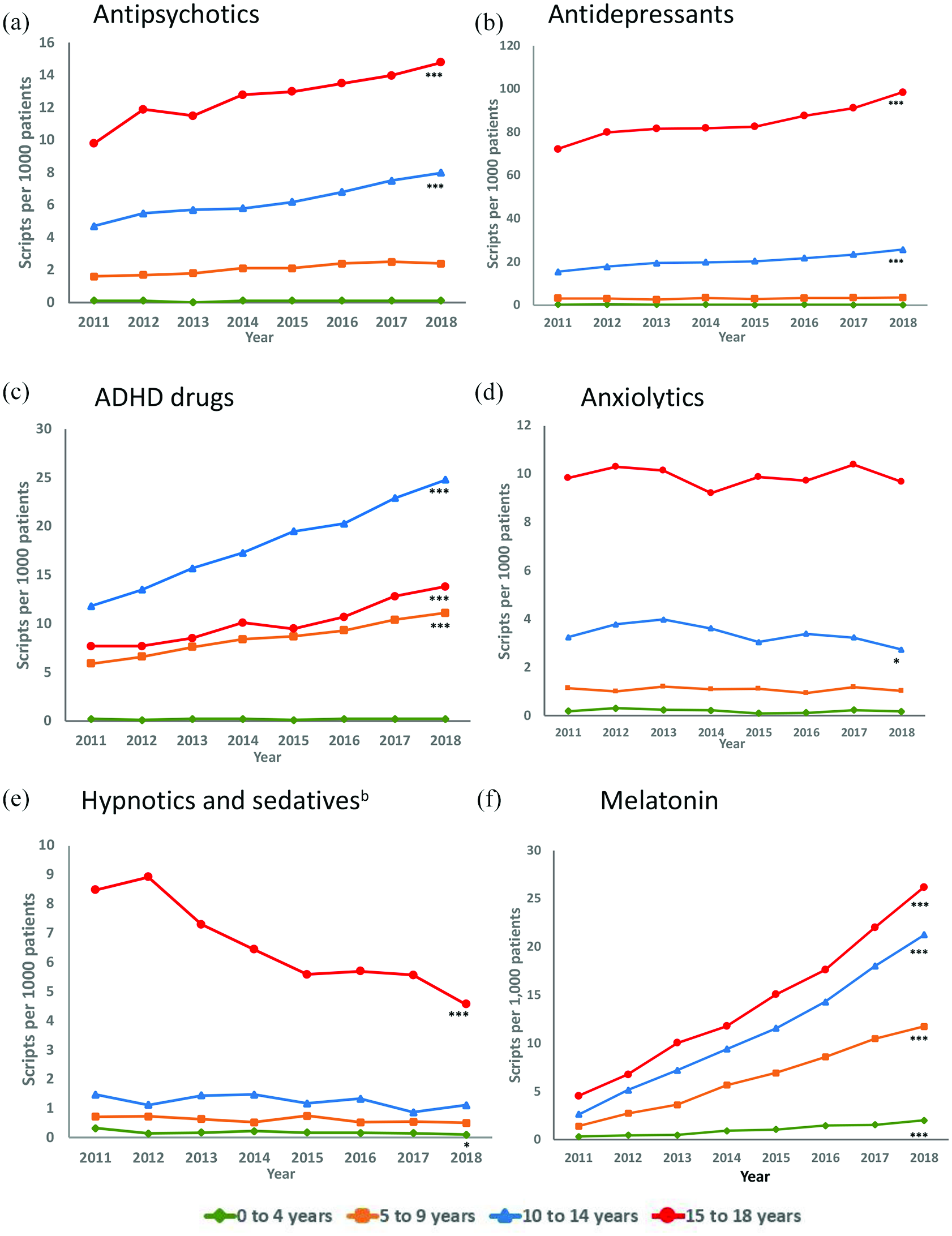
Trends in prescribing by age-group for the five major classes of psychotropic medications and melatonin from 2011 to 2018, reported as prescriptions per 1000 patients.a (A) Antipsychotics, (B) Antidepressants, (C) ADHD drugs, (D) Anxiolytics, (E) Hypnotics and sedativesb and (F) Melatonin.
Females were more likely than males to be prescribed antidepressants in any year; but antipsychotics, ADHD medications and melatonin prescriptions were more frequent among males (Supplementary eTables S3–S8). Both genders showed similar increases in annual antipsychotic and antidepressant prescription rates, and similar decreases in hypnotic/sedative prescriptions. ADHD drug prescriptions increased more rapidly in females than males. This reduced the differential in prescribing rates in males versus females from 4.7 times in 2011 to 3.4 in 2018. Anxiolytic prescriptions remained steady over time among males and females.
Rates of antipsychotic and ADHD prescriptions in the lowest IRSAD quintile (most disadvantaged) were around three times those recorded in the highest quintile (least disadvantaged) (Supplementary eTables S3, S5). For antidepressant prescriptions, the rate in the lowest quintile was around 1.7 times the rate in the highest quintile (eTable S4). However, there were no substantial differences in the annual increases across quintiles for antipsychotics, antidepressants and ADHD drugs.
For hypnotics/sedatives (Supplementary eTable S7) and melatonin (Supplementary eTable S8) prescribing, there were no substantial differences in trends across time for IRSAD quintiles; hypnotic/sedative prescribing decreased around 8% and melatonin increased around 26%. There appeared to be no consistent change in rates from high to low IRSAD quintiles for anxiolytics, hypnotics/sedatives or melatonin.
Prescribing patterns in 2018
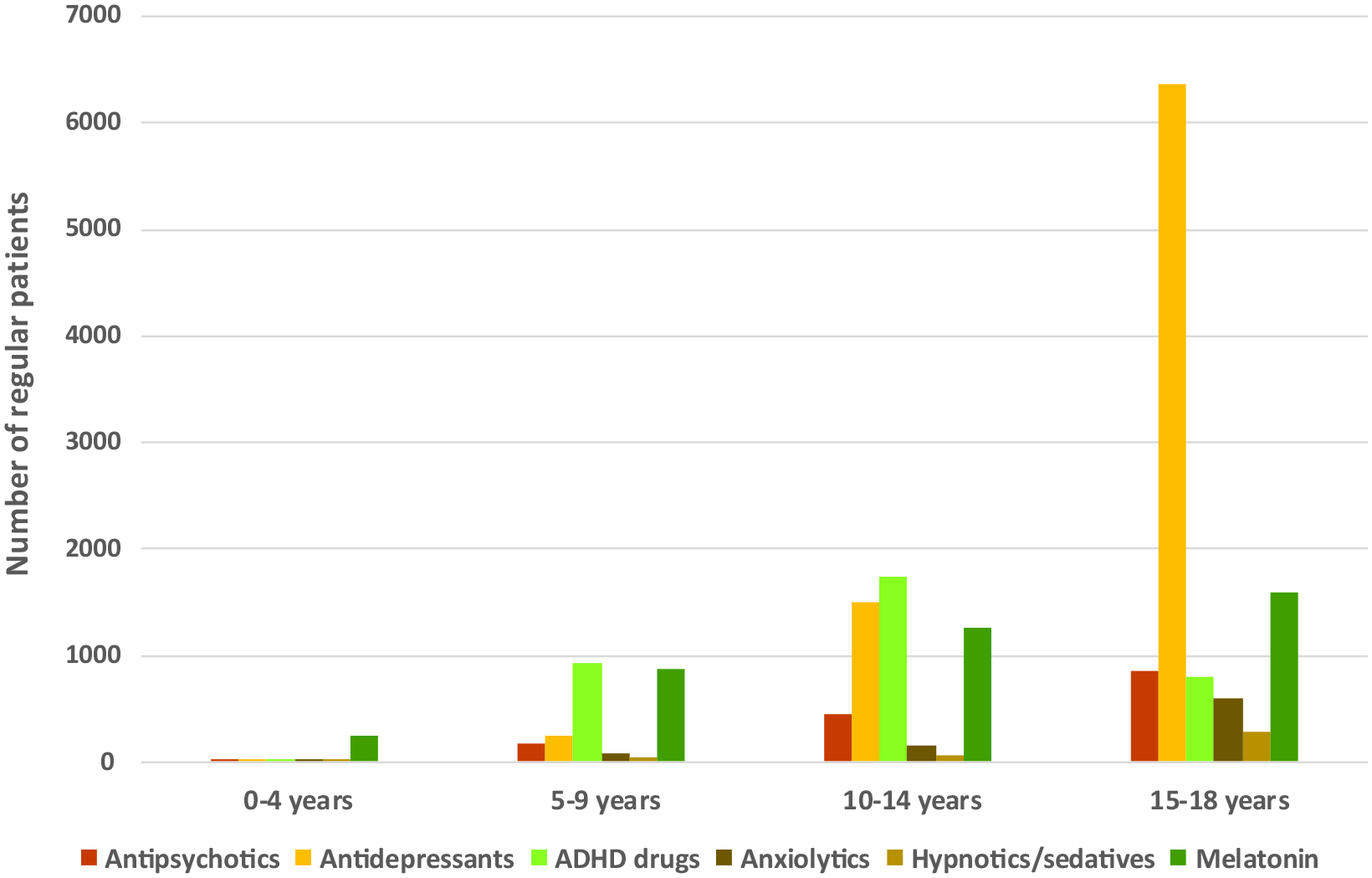
Of all 14,075 children and adolescents who were prescribed one of the main psychotropic classes or melatonin in 2018, 57.7% were prescribed antidepressants (n = 8126), 24.8% ADHD medications (n = 3487), 10.7% antipsychotics (n = 1507), 7.0% anxiolytics (n = 847), 2.8% hypnotics/sedatives (n = 397) and 28.3% melatonin (n = 3977; some individuals were prescribed more than one group of drugs). Figure 2 shows that the most frequently prescribed class of psychotropics and melatonin varied with age. Among 0- to 4-year-olds (n = 329) melatonin was prescribed more than any other psychotropic. For those 5–9 (n = 1974) or 10–14 years (n = 4130), ADHD medications were the most common psychotropics prescribed. Among 15- to 18-year-olds (n = 8272), antidepressants were the most frequent psychotropics prescribed (76.9%), with a point prevalence of 98.5/1000 patients. This was more than twice the prevalence in 10- to 14-year-olds (36.3%) and at least six times the prevalence among those under 10 years (Table 3).
Number of regular patients receiving prescriptions for psychotropics by drug class and age-group in 2018.
The most frequently prescribed subclasses of medications in 2018 were also examined (Table 3). In all age-groups, second-generation antipsychotics (SGAs) were far more often prescribed than first-generation antipsychotics, with well over 90% of prescriptions being for SGAs. SSRIs were the most frequently prescribed class of antidepressants in all age-groups (50.0% among 0- to 4-year-olds and more than 85% in other age-groups). With ADHD medications, the non-stimulant antiadrenergic medications predominated in 0- to 4-year-olds, but the stimulant class was prescribed more often in other age-groups.
Table 4 lists the most frequently prescribed medications from each psychotropic class by age-group for the year 2018. Risperidone was the most prescribed antipsychotic for children under 15, but quetiapine was the most prescribed in 15- to 18-year-olds. Amitriptyline was the most prescribed antidepressant in 0- to 4-year-olds, but fluoxetine was the most prescribed in the other three age-groups. Clonidine was the most prescribed ADHD medication in 0- to 4-year-olds, with methylphenidate predominating in older children.
Among patients prescribed a psychotropic in 2018, 17.5% (n = 2134) were prescribed more than one type of medication concurrently, with almost 10% of these patients (n = 206) prescribed three or more (data not shown). Psychotropic polypharmacy in children and adolescents will be examined in a future study using the same database.
Discussion
To our knowledge, this is the first study to explore psychotropic prescribing to children and adolescents using a large Australian general practice database. Four main findings can be highlighted. First, the prescribing rate for psychotropics, excluding melatonin, has increased at an annual average of 4.5%, with 3.6 out of 100 children and adolescents being prescribed at least one psychotropic in 2018. The most rapid increase was among 10- to 14-year-olds. Second, trends differed according to the class of psychotropic medication. The highest increase was for ADHD medications, followed by antipsychotics and antidepressants. Third, patients in more disadvantaged areas were more likely to be prescribed antipsychotics, antidepressants and ADHD medications than those in the least disadvantaged areas. Finally, melatonin showed the most pronounced rise, increasing just over 600% between 2011 and 2018.
Our trends are consistent with those reported in studies using Australian PBS data (DUSC, 2018; Hálfdánarson et al., 2017; Karanges et al., 2014; Raman et al., 2018) and data from other countries (Barczyk et al., 2020; Hartz et al., 2016). However, although these studies showed similar increases for antidepressants, antipsychotics and ADHD medications, rates differed from our findings, partly due to differing timespans and data sources. Individual drug classes are examined in more detail below.
Antipsychotics
From 2011 to 2018, there was a 62.8% increase in the prescribing of antipsychotics to under-19-year-olds. It was higher than the increase observed in most European countries and the United States from 2005 to 2014, but lower than the 159% increase observed from 2006 to 2014, using Australian PBS data (Hálfdánarson et al., 2017). This difference may be related to the fact that our dataset does not include prescriptions issued by specialists or drugs dispensed through hospital pharmacies. Our study also found the highest increase in 10- to 14-year-olds (+72.2%), continuing the trend observed by Karanges et al.’s (2014) study using PBS data (+49.1%, 2009–2012).
The most frequently prescribed antipsychotics by age-group were also similar to those reported by Karanges et al. (2014), who found risperidone the most prescribed antipsychotic in 3- to 9-year-olds and 10- to 14-year-olds, and quetiapine in 15- to 19-year-olds. Although impossible to determine from the current analysis, these results appear to be mostly consistent with current TGA drug approvals for psychotropic use in children and adolescents. Antipsychotics are approved for children with severe behavioural problems associated with autism and conduct disorders. Therefore, the increasing trend for antipsychotic prescribing is likely due partly to the increased prevalence of diagnosed/reported autistic disorders in 0- to 19-year-olds from 2009 to 2015 (AIHW, 2017). Other conditions for which antipsychotics are approved have had decreased diagnosis rates (e.g. conduct disorders; Sawyer et al., 2018), or are conditions rarely diagnosed in children and adolescents (e.g. schizophrenia; Galletly et al., 2016).
However, antipsychotics are increasingly being used as ‘broad spectrum psychotropic drugs’ for a diverse range of non-psychotic disorders in paediatric populations, including anxiety, ADHD, depression and insomnia (Carton et al., 2015; Penfold et al., 2013). There is some evidence suggesting that anxiety diagnoses have increased over the last decade (ABS, 2009/2018; Spence et al., 2018), and a 2014 PBS report has suggested antipsychotics are being used in children and adolescents with anxiety and stress in Australia (Morrison et al., 2014). Therefore, the increasing antipsychotic prescription rates may also reflect increasing off-label use.
Antidepressants
The overall increase in antidepressant prescriptions to children and adolescents (+42.8%) was consistent with international findings using both dispensing (Barczyk et al., 2020; Lagerberg et al., 2019) and general practice datasets (Bachmann et al., 2016; John et al., 2016; Pringsheim et al., 2019). Similar to antipsychotics, and again demonstrating a continuation of the trend previously observed in Australia (Karanges et al., 2014), our study recorded the highest increase in 10- to 14-year-olds. Although 15- to 18-year-olds were prescribed more antidepressants than any other age-group, the increase has been more rapid in 10- to 14-year-olds.
In Australia, no antidepressants are approved for managing depression in children and adolescents (Supplementary eTable S2). Despite this, and consistent with previous studies in Australia (Karanges et al., 2014) and NZ (Barczyk et al., 2020), most prescriptions in 5- to 18-year-olds were for fluoxetine. This is likely due to the inclusion of fluoxetine as a treatment option for depression in Australian (McDermott et al., 2011) and international guidelines (Cheung et al., 2018; National Institute for Health and Care Excellence [NICE], 2019). However, given that two meta-analyses have concluded that no SSRIs are beneficial in treating childhood or adolescent depression (Hetrick et al., 2012, 2021) and fluoxetine is not approved for any childhood conditions in Australia, the high rates of prescriptions for fluoxetine need to be investigated.
Consistent with international studies, TCAs were prescribed less often than SSRIs, most likely for nocturnal enuresis (Nankivell and Caldwell, 2014). In our study, although numbers were low, limiting the reliability of the finding, 31.3% of 0- to 4-year-olds who had been prescribed an antidepressant were prescribed a TCA – a higher percentage than any other age-group. However, no other study has explored TCA prescribing in this age-group to allow a comparison. Given that only non-pharmacological treatments for enuresis are recommended for children under 7 (BMJ Best Practice, 2020), the prescribing of TCAs in this age-group warrants further investigation.
ADHD medications
Corroborating findings of two large multi-country studies (Bachmann et al., 2017; Raman et al., 2018) and Australasian studies (Barczyk et al., 2020; Karanges et al., 2014), prescribing of ADHD medications increased in our study. Indeed, the overall and average annual increase was the highest of any psychotropic class and increased the most in 10- to 14-year-olds (+111.2%). This is in contrast to the findings of Karanges et al. (2014), and all countries examined in Bachmann et al. (2017), where 15- to 19-year-olds showed the highest increase in ADHD drug prescriptions.
However, comparing prescribing trends for ADHD medications across studies is difficult. Most studies have used dispensing datasets, and countries differ in their prescribing regulations for ADHD medications. In Australia, stimulants have strict prescribing guidelines, and the primary responsibility for treatment resides with specialists, although GPs can be nominated as co-prescribers in some circumstances (Australian ADHD Professionals Association, 2021). Consequently, the rate of prescribing of ADHD medications by GPs is low and has remained stable at around 19% of prescriptions dispensed from 2012–2013 to 2018–2019 (AIHW, 2020: Table PBS.7). Nonetheless, some evidence suggests that the prevalence of diagnosed ADHD in 6- to 17-year-olds may have decreased over the study period (9.9% to 7.8% from 1998 to 2013–2014) (Sawyer et al., 2018). If this trend has continued until 2018, the increasing rate of stimulant prescriptions in our study may indicate a growing tendency to treat ADHD with medications in preference to non-pharmacological approaches.
A notable finding is the high percentage of 0- to 4-year-olds prescribed clonidine, which is not approved for children and adolescents in Australia (and is primarily prescribed for hypertension in adults). When combined with methylphenidate in children with ADHD, it has been associated with serious adverse events (Boehringer Ingelheim Pty Ltd, 2019).
Anxiolytics, hypnotics/sedatives and melatonin
Prescribing of anxiolytics in general practice showed no changes overall, declining only slightly in 10- to 14-year-olds. Hypnotic/sedative (benzodiazepines and Z-drugs) prescribing declined in the youngest and oldest age-groups. Australasian and international studies are scarce, and comparison was difficult due to differing drug groupings.
For anxiolytics, a Welsh study found a significant overall increase (+62%) only in the 15- to 18-year-olds (2003–2011) (John et al., 2015). A NZ investigation found a 50% increase in under-18 year-olds across 9 years (2008–2016) (Barczyk et al., 2020). However, in consonance with our findings, a Norwegian study from 2004 to 2014 found no meaningful change in prescribing (Hartz et al., 2016).
No other studies reported a decline in hypnotic/sedative prescribing. Studies from NZ (Barczyk et al., 2020) and Norway reported increases (Hartz et al., 2016), but these studies included melatonin in the hypnotic/sedative class. We found a substantial increase in prescriptions for melatonin in all age-groups, and our results would likely be more consistent with international studies if we had also analysed melatonin within the hypnotic/sedative class.
Given ongoing concerns about paediatric benzodiazepine use (O’Sullivan et al., 2015), prescribing melatonin may well be perceived as a safer and effective alternative. Indeed, studies reporting beneficial effects of melatonin for children with insomnia, with minimal reported adverse effects after years of daily use (Janjua and Goldman, 2016), may encourage off-label use of melatonin. However, until 2020, melatonin was not approved for any childhood conditions, and there are concerns with prescribing neurohormonal medications to pre-pubertal children (Boafo et al., 2019).
Demographics
Gender differences in our study were largely consistent with international studies. Females were prescribed antidepressants more often than males, although the female–male ratio was lower than that observed in several other countries (Bachmann et al., 2016; Barczyk et al., 2020; John et al., 2016). An inverse trend was found with antipsychotics, with males being prescribed the medications twice as often as females, similar to several European countries and the United States (Hálfdánarson et al., 2017), but differing from findings in NZ, where antipsychotic prescriptions were similar among boys and girls (Barczyk et al., 2020). ADHD medication prescription rates in males were on average 3.8 times those in females (Supplementary eTable S5), corroborating the NZ study findings (Barczyk et al., 2020). Although ADHD drugs were more frequently prescribed in males, our results showed that the increase was more rapid in females, similar to findings in Norway (Hartz et al., 2016).
Patterns of prescribing with age were similar to those in the NZ study (Barczyk et al., 2020). In both studies, there was an increase in prescriptions with increasing age observed for antidepressants, antipsychotics, anxiolytics and hypnotics/sedatives. The exception was ADHD medication prescribing, which was higher in 10- to 14-year-olds.
Regarding socioeconomic position, for antipsychotics, antidepressants and ADHD drugs, there was a tendency for those in the most disadvantaged areas to have higher prescription rates than those in the least disadvantaged areas. We only found one study that included socioeconomic factors – a Welsh primary care study analysing antidepressant prescribing (John et al., 2016). Findings were similar to our study. In Australia, there are higher rates of mental disorders in lower socioeconomic areas (Enticott et al., 2016; Lawrence et al., 2015), which could explain the higher rates of drug use in our study. However, it is also possible that children and adolescents in more disadvantaged areas are more likely to receive drug treatments rather than non-pharmaceutical options (Nunn et al., 2020). This may be due to different prescribing practices in lower socioeconomic areas, differing availability of alternative treatments and/or differing treatment preferences of those living in poorer areas. Analysis of social determinants of mental health is a limited but growing area of research, and future studies are needed to investigate sociodemographic correlates of mental disorders and psychotropic prescribing practices.
Strengths and limitations
MedicineInsight is a large, longitudinal database, covering 9% of GPs and over three million patients attending Australian general practices. Although some states, regions and participants in higher IRSAD areas were over-represented compared to census data, the patients in the database are considered representative of those attending Australian general practice (NPS MedicineWise, 2020). MedicineInsight records all prescriptions written by GPs, but does not indicate if they were dispensed, which could overestimate psychotropic use. Nonetheless, our findings were consistent with other national and international studies using dispensing data. Although most psychotropic prescribing occurs in general practice, there may be situations where trends differ (e.g. specialist prescribing), so the results cannot be generalised beyond general practice. As with all real-world health care databases, MedicineInsight is reliant on staff consistently and accurately completing data fields, resulting in potential problems with missing or misclassified data.
Conclusion
This study shows increasing trends in psychotropic prescribing to children and adolescents in Australia, consistent with observed increases in other Australian and international data sources. From 2011 to 2018, prescriptions for antipsychotics, antidepressants and ADHD medications rose substantially, with the greatest increase in 10- to 14-year-olds. Although benzodiazepine and Z-drug prescriptions have decreased, this has been more than offset by a marked rise in melatonin prescribing. Future research is needed to explore and understand the reasons why psychotropic prescribing is increasing, and its impact on child and adolescent health and well-being.
Supplemental Material
sj-pdf-1-anp-10.1177_00048674211067720 – Supplemental material for Trends in prescription of psychotropic medications to children and adolescents in Australian primary care from 2011 to 2018
Supplemental material, sj-pdf-1-anp-10.1177_00048674211067720 for Trends in prescription of psychotropic medications to children and adolescents in Australian primary care from 2011 to 2018 by Julie Klau, Carla De Oliveira Bernardo, David Alejandro Gonzalez-Chica, Melissa Raven and Jon Jureidini in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
The authors are grateful to the general practices that participated in MedicineInsight and the patients who allowed the use of de-identified information in health research. They also acknowledge the assistance of staff at the Department of General Practice at the University of Adelaide.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was supported by a research grant from the Channel 7 Children’s Research Foundation. Project Reference: 20/13437316.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.