
Abstract
Objective:
Parenthood is central to the personal and social identity of many people. For individuals with psychotic disorders, parenthood is often associated with formidable challenges. We aimed to identify predictors of adequate parenting among parents with psychotic disorders.
Methods:
Data pertaining to 234 parents with psychotic disorders living with dependent children were extracted from a population-based prevalence study, the 2010 second Australian national survey of psychosis, and analysed using confirmatory factor analysis. Parenting outcome was defined as quality of care of children, based on participant report and interviewer enquiry/exploration, and included level of participation, interest and competence in childcare during the last 12 months.
Results:
Five hypothesis-driven latent variables were constructed and labelled psychosocial support, illness severity, substance abuse/dependence, adaptive functioning and parenting role. Importantly, 75% of participants were not identified to have any dysfunction in the quality of care provided to their child(ren). Severity of illness and adaptive functioning were reliably associated with quality of childcare. Psychosocial support, substance abuse/dependence and parenting role had an indirect relationship to the outcome variable via their association with either severity of illness and/or adaptive functioning.
Conclusion:
The majority of parents in the current sample provided adequate parenting. However, greater symptom severity and poorer adaptive functioning ultimately leave parents with significant difficulties and in need of assistance to manage their parenting obligations. As symptoms and functioning can change episodically for people with psychotic illness, provision of targeted and flexible support that can deliver temporary assistance during times of need is necessary. This would maximise the quality of care provided to vulnerable children, with potential long-term benefits.
Parenthood is a common aspiration; however, this role is difficult to fully prepare for and involves a range of emotions and practical responsibilities. For most people, the steep learning curve accompanying parenthood is a joyous, albeit at times very challenging, part of life. Of people with psychotic disorders, more than half of women and around a quarter of men are parents (Campbell et al., 2012). As can be expected, parents with serious mental illnesses including psychotic disorders have the same aspirations to parent effectively and hold comparable dreams and fears for their children as parents without serious mental illness (Ackerson and Venkataraman, 2003; Fudge et al., 2004). However, people with serious mental illness might find the parental journey even more challenging. It is important then to identify factors that increase the likelihood of positive child and parent outcomes.
Parents who experience a psychotic disorder become parents on average at 20 years of age, with 65% of those yet to experience their first episode of psychosis (Nicholson and Miller, 2008; Morgan et al., 2005). For those 35% whose psychotic illness precedes parenthood, managing symptoms and meeting parental role obligations place immense pressure on them, and on their family and friends (Caton et al., 1999). Women who develop serious mental illness, including psychotic disorders, around the time of their child’s birth have worse parenting outcomes compared to those who had their children before mental illness onset (Mowbray et al., 2005). Yet, mothers with psychosis who have higher levels of marital and social support, and are of higher socio-economic status, tend to cope better with crises and have better parenting outcomes (Landeen et al., 2007; Morgan et al., 2012). Recent Australian clinical guidelines highlight the need for specialised care for mothers with psychosis (Galletly et al., 2016). However, in reality, many mothers with psychosis report wanting more support and often experience loneliness (Blegen et al., 2010; Hearle et al., 1999; Howard et al., 2001).
Individuals with serious mental illness report a great deal of pleasure from engagement in the parenting role (Bassett et al., 1999), although many also report considerable stress, making it challenging for them to parent well. This is unsurprising considering many non-parents and parents alike with psychotic disorders live in poverty, experience insecure living circumstances, and have difficulties completing education, maintaining employment and lack satisfying social relationships (Campbell et al., 2012; Harvey et al., 2012; Plant et al., 2002). Challenges associated with low levels of education, and subsequent problems with obtaining well-paid and flexible employment (Campbell et al., 2012), can also make it more difficult to parent, regardless of diagnosis. These stressors have been linked to poor parenting outcomes such as difficulties in forming attachments to their children and nurturing them appropriately (Oyserman et al., 2000). Indeed, mothers with psychosis appear particularly vulnerable to poor parenting outcomes compared to parents with, for example, mood disorders (Landeen et al., 2007).
For parents with psychosis, having access to support and respite in times of crisis or hospitalisation is critical (Morgan et al., 2012). However, for many people with psychosis, social isolation is a significant problem (Stain et al., 2012). Underlying the social isolation is often a pervasive sense of fear that their illness will lead to stigmatisation and custodial loss of their children to protective services or, if separated, to the other parent (Bassett et al., 1999; Zemencuk et al., 1995). Unfortunately, fear of custodial loss is not unfounded. Between 30% and 80% of mothers with psychotic disorders report having lost custody of their children (Nicholson et al., 2001). Poor insight, a feature common among individuals with psychotic disorders, can also exacerbate parenting difficulties (Landeen et al., 2007; Pini et al., 2001) and impair many parents’ ability to evaluate how well the family unit is functioning and seeking help when necessary (Plant et al., 2002).
Alcohol and other substance use is another factor known to negatively impact parenting. Among parents with psychotic disorders, substance use is common: around 70% of fathers and 45% of mothers with psychotic disorders have a lifetime substance use comorbidity (Campbell et al., 2012). Substance use increases the risk of treatment noncompliance, exacerbates pre-existing illness and impairs overall functioning and parenting capacity (Nicholson and Miller, 2008; Seeman, 2002). Additionally, substance use disorders are strongly associated with social disadvantage, violence, disruptive behaviour, and child abuse and neglect (Henshaw et al., 2011).
This study aimed to identify predictors of positive parenting outcomes for adults with psychotic disorders, using data from the second Australian national survey of psychosis (Morgan et al., 2012). The key question was which characteristics predict good versus poor parenting outcomes? The unique study design permitted the examination of quality of care provided by both mothers and fathers to their child(ren) over the last 12 months (outcome variable) and the investigation of the relationships between parenting outcomes as well as parental clinical, demographic and current psychosocial characteristics. We hypothesised that better adaptive functioning (defined as how well a person handles common demands in life; Table 3 lists the variables included in this construct), less symptomatology, low levels of substance abuse, parenting role (e.g. contact and responsibility) and strong psychosocial support would be predictive of better parenting outcomes.
Method
Design and recruitment
Data analysis was based on information collected as part of the second Australian national survey of psychosis – the Survey of High Impact Psychosis (SHIP). Briefly, a two-phase design was utilised to design a representative, population-based study covering a catchment population of ~1.5 million people aged 18–64 years (~10% of Australia’s population in this age group). The survey was carried out at seven mental health service sites across five Australian states, covering a total area of roughly 62,000 km2. Individuals who presented to mental health services and non-government organisations, and who screened positive for psychosis in the previous month using a specially developed psychosis screener, were included (Jablensky et al., 1999, 2000; Morgan et al., 2012). Screen items involved having hallucinations or delusions, being on antipsychotic medication or having been given a diagnosis by a doctor. The screen-positive cut-off was a positive rating on two or more of these items. The inclusion criteria identified 7955 individuals. Potential participants were randomised and stratified by age group. The final sample consisted of 1825 people who undertook interviews and assessments between April and December 2010. The study was granted ethics approval from the relevant institutional human research ethics committee at each site, and all participants provided written, informed consent. See Morgan et al. (2012) for detailed information pertaining to the study design and participants.
Participants
We report data from a subsample of the participants in the second Australian national survey of psychosis, namely, 234 (60 = men, 174 = women) parents with psychotic illness aged between 20 and 62 years (mean age = 37 years, standard deviation [SD] = 8.0 years) resident within the catchment areas. Inclusion criteria comprised living with at least one dependent child and having a role in the upbringing of their children. Exclusion criteria included the following: (1) insufficient English language abilities to complete an interview, (2) impaired cognition hindering capacity for informed consent or (3) residence in a nursing home or prison. As per the design, all participants met screening criteria for psychosis. At the time of full assessment, parents were diagnosed as per International Classification of Diseases, 10th Revision (ICD-10; World Health Organization, 2008) with non-affective (e.g. schizophrenia, non-organic psychosis [n = 138]) or affective psychosis (e.g. bipolar disorder, schizoaffective disorder, depressive psychosis [n=94]). Additional participant family composition, and demographic and diagnostic information are provided in Tables 1 and 2.
Family composition.
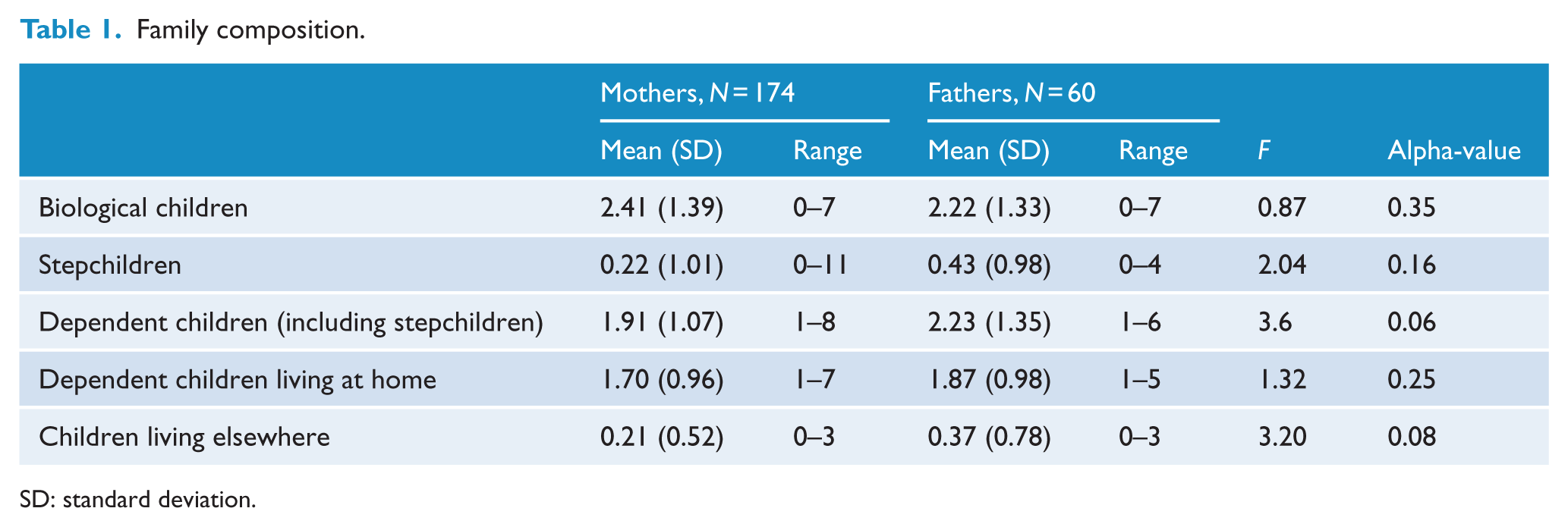
SD: standard deviation.
Demographic and diagnostic characteristics of parents living with dependent children by gender.
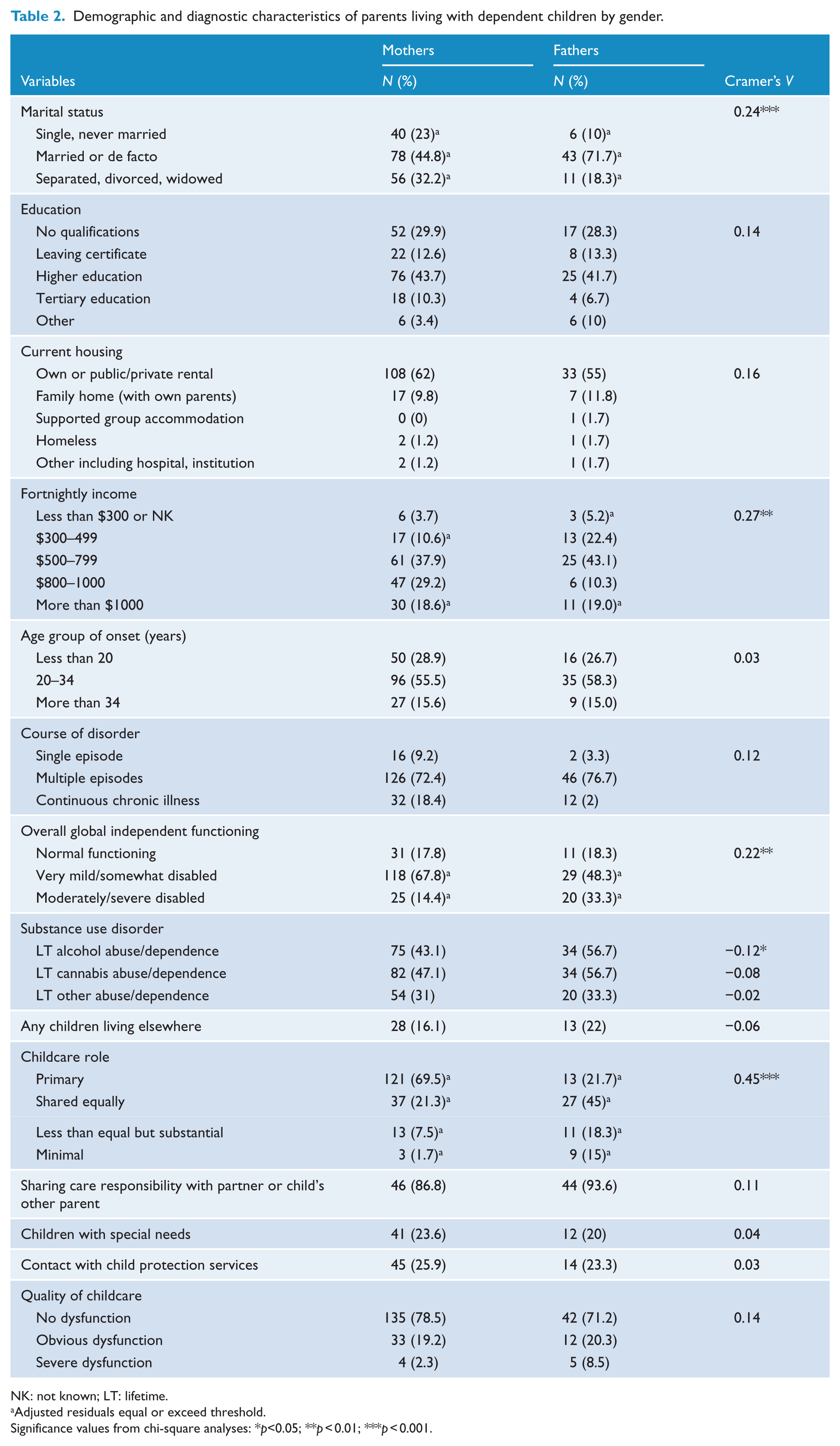
NK: not known; LT: lifetime.
Adjusted residuals equal or exceed threshold.
Significance values from chi-square analyses: *p<0.05; **p < 0.01; ***p < 0.001.
Materials
Assessment included the Diagnostic Interview for Psychosis to determine ICD-10 diagnosis (Castle et al., 2006; World Health Organization, 2008). The remaining survey consisted of 33 modules including questions about education, accommodation, income, substance use, stigma, social and occupational function, service utilisation, past and present symptoms, and intellectual ability. The Multidimensional Scale of Independent Functioning (MSIF) which has good criterion, discriminative, inter-rater and construct validity, assessed global independent functioning and reflected the participant’s overall level of adaptive functioning while controlling for the level of performance in each category (Jaeger et al., 2003). Participants were asked about the number of biological- and step-children they had, how many of these were less than 18 years of age, the living and shared-care arrangements, childcare needs and contact with child protection services. Quality of care of child(ren) in the last 12 months was rated based on participant report and interviewer enquiry/exploration using a number of probes and other relevant interview information. The ratings were made by trained clinicians with regular discussions within each local site team and across the national site team to ensure high reliability of ratings. There were three quality of care ratings: no dysfunction (defined as participating in childcare about as much as the average carer of same sex/age group would under similar circumstances), obvious dysfunction (defined as having little interest in childcare or reduced competence for up to half the time) and severe dysfunction (defined as a total lack of interest in childcare or reduced competence for more than half the time or evidence of neglect). These three quality of care ratings provided the operational definition of ‘parenting outcome’.
Analysis
Descriptive statistics were extracted using IBM SPSS statistical software (version 22.0; SPSS, Chicago, IL, USA). Initially, mothers and fathers were compared on a number of demographic variables (see Table 1) using one-way analyses of variance (ANOVAs) with gender as the between-group variable. Chi-square tests assessed univariate associations between nominal variables of interest (variables of interest included current housing, fortnightly income, age group of onset, course of disorder, overall global independent functioning, lifetime substance use disorder, childcare role, sharing arrangements, children with special needs, contact with community services [last 12 months] and quality of care of child(ren) [last 12 months]). Adjusted residuals (cut-off value of 2) were inspected to enable interpretation of the chi-square tests, and Cramer’s V provided an indication of the strength of association among the levels of the row and column variables (>0.5, high association; 0.3−0.5, moderate association; 0.1−0.3, low association; 0−0.1, little if any association).
A structural equation model (SEM) tested hypothesised associations between groups of indicator variables and parenting outcome, operationalised as quality of care of children (last 12 months). Associations were mediated by five hypothesis generated latent variables. These were labelled as follows: psychosocial support, illness severity, substance abuse/dependence, adaptive functioning and parenting role. (Further details on the full set of variables that were included and the different models that were fit can be found in the Supplementary Material.) The observed variables that operationalised these latent variables are listed in Table 3, e.g., the latent variable ‘illness severity’ was operationalised by variables such as the age of onset of symptoms and the lifetime presence/absence of symptoms (see Table 3).
Loadings of observed (indicator) variables on latent variables.
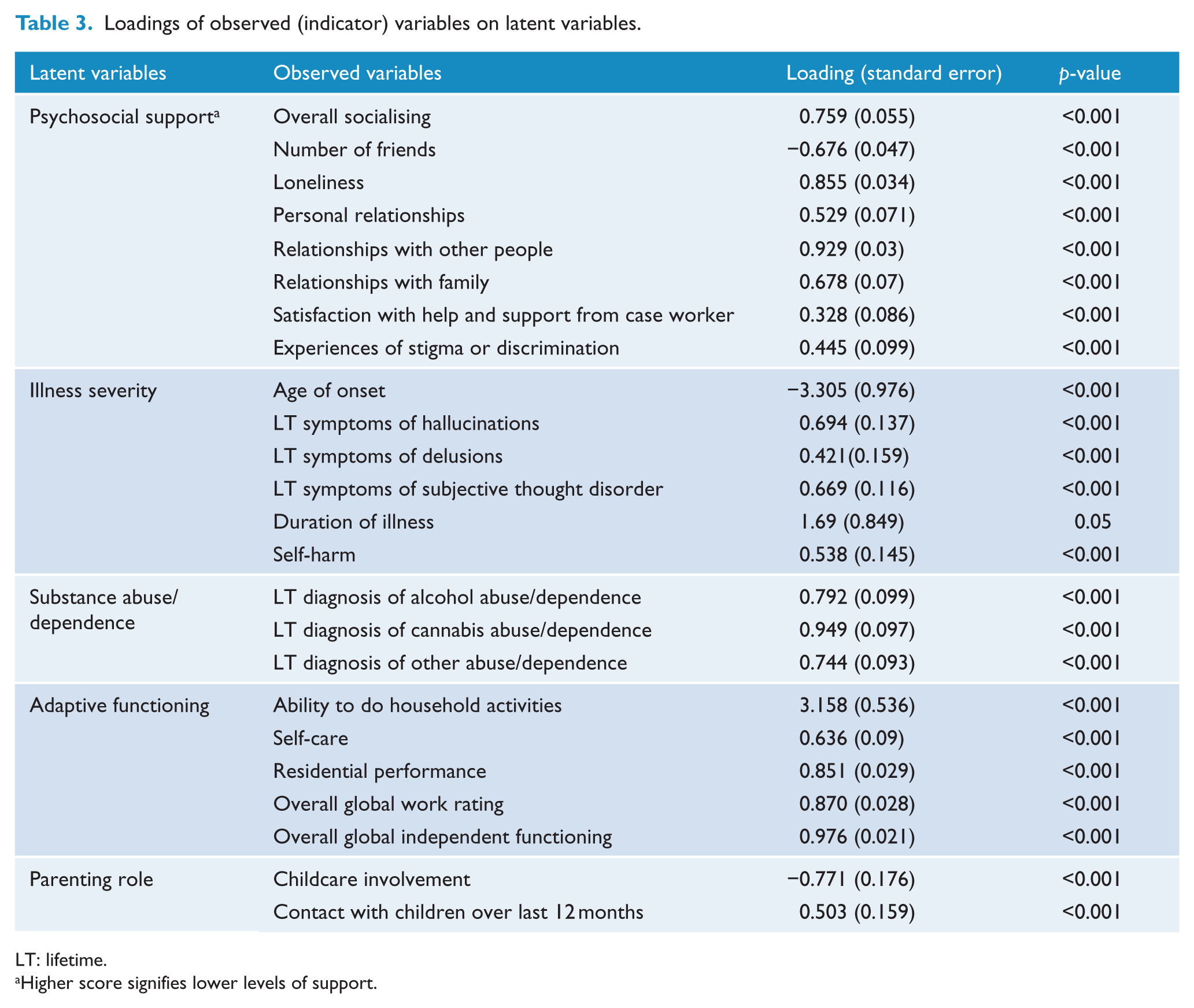
LT: lifetime.
Higher score signifies lower levels of support.
The SEM model structure is illustrated in Figure 1. Each observed variable was used as an indicator for only one latent variable. All latent variables were allowed to correlate with one another and to directly associate with the outcome measure. The parameters of the model were estimated using the SEM routine in the package ‘lavaan’ for the statistical programming language R. We report parameters estimated on the scale defined by standardising at the level of latent variables. Both the R language and the lavaan package are freely available open-source software (R Development Core Team, 2004; Rosseel, 2012).
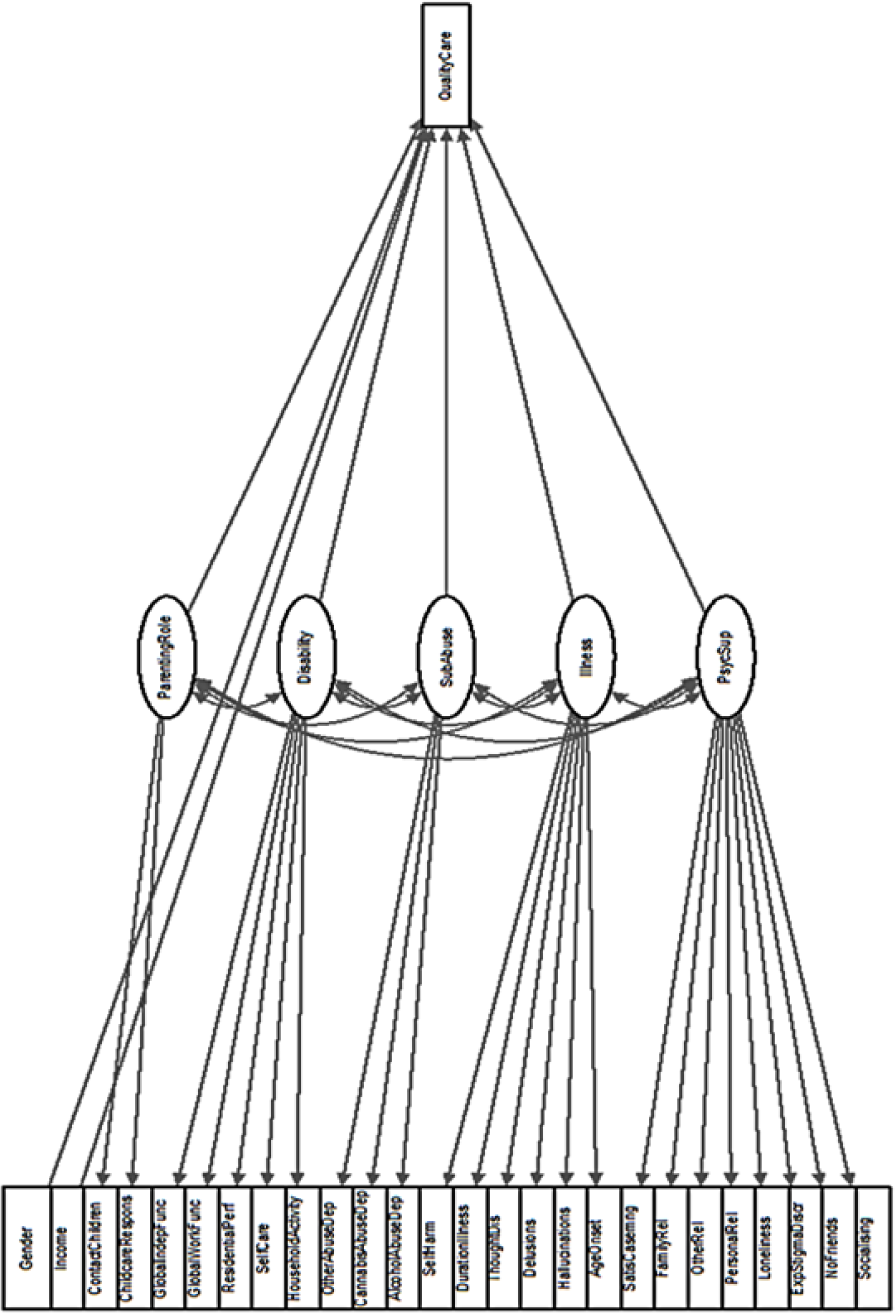
Confirmatory factor analysis tree chart.
Results
Participant characterisation
Characteristics of the participants in the study are shown in Tables 1 and 2. The majority of parents were married or in a de facto relationship. However, it was more common for fathers to still be married and for mothers to be divorced (χ2 (2, n = 234) = 13.03, p < 0.001, Cramer’s V = 0.24). Many parents had completed higher education (42% fathers; 44% mothers), but more than one-quarter of parents had no post-high school qualifications. The majority of parents lived in their own or public/private rental accommodation, and had a fortnightly income above $300. Most parents experienced illness onset between the ages of 20 and 34 years, and had experienced multiple episodes of illness. The majority of parents were in the ‘mild to somewhat disabled’ functioning range, but it was more common for mothers than fathers to fall in this range, with more fathers having moderate to severe disability (χ2 (2, n = 234) = 11.05, p < 0.004, Cramer’s V = 0.22). About half the sample had lifetime substance use disorder.
The mean number of children was 2.41 (SD, 1.39) for mothers and 2.22 (SD, 1.33) for fathers. Most parents had no children living elsewhere (78% of fathers; 84% of mothers). It was more common for mothers to rate themselves as primary caregivers compared to fathers, and fathers were more likely to have a less than equivalent level of caregiving responsibility (χ2 (3, n = 234) = 47.51, p < 0.0005, Cramer’s V = 0.45). When care responsibilities were shared, they were most frequently shared with a partner or the child’s other parent (94% of fathers; 87% of mothers). A smaller proportion relied on the child’s grandparents for help (6% of fathers; 13.2% of mothers). Of the parents who received childcare support, 82% reported that they would have some or a lot of difficulties if childcare support or help was no longer available. In total, 20% of fathers and 24% of mothers reported caring for children who had psychological or physical special needs. Importantly, around three quarters of the sample were rated as having no dysfunction in their quality of care for their child(ren) (last 12 months). No relationship between quality of care and ratings of insight was identified (p > 0.05). Three quarters of parents had not been in contact with child protection services in the past 12 months. In total, 70% of those who had been in contact with child protection services were in the group rated as providing adequate care. In all, 17 of 40 parents, who reported that they were in contact with non-governmental organisations for various types of support, had received specific advice or support with parenting in the last 12 months and 17% of all parents reported that they had received family support from other services.
SEM
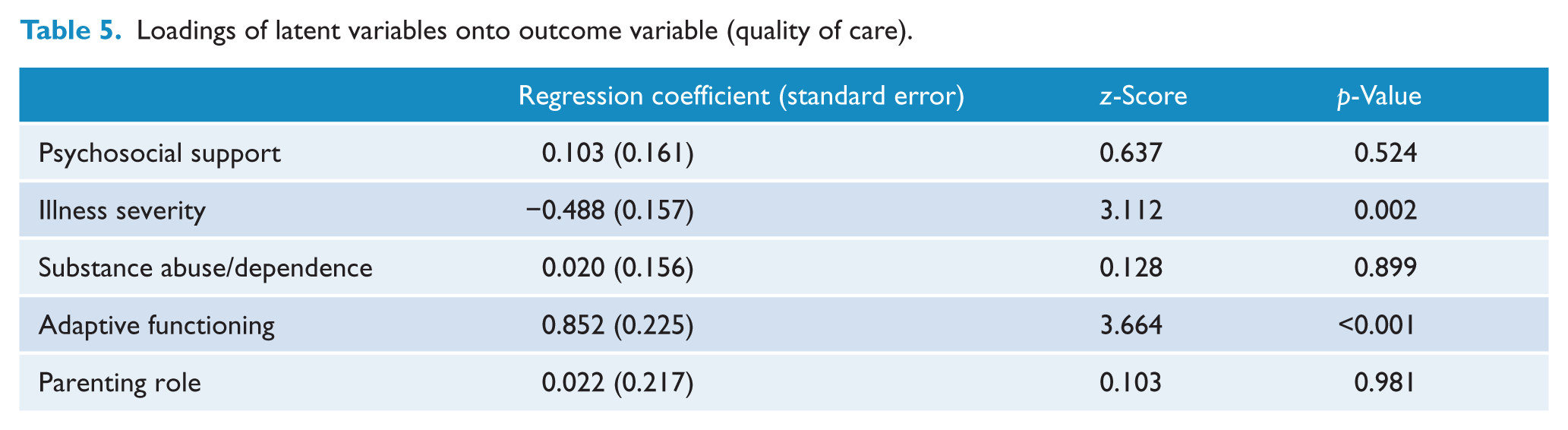
The SEM approach allows one to simplify the complex patterns of association naturally present in such a large, variable dataset. Four variables were hypothesised to influence parenting outcome. The two latent variables were reliably associated with this outcome measure, and strongly so: illness severity (est = −0.72, z = −3.1, p < 0.01) and adaptive functioning (est = 1.09, z = 5.4, p < 0.001). The two manifest variables were not reliably associated with parenting outcome (both ps > 0.44). The indicators that loaded onto the latent variable measuring illness severity were age of onset, duration of illness, self-harm and lifetime symptoms of hallucinations, delusions and subjective thought disorder, and the latent variable measuring substance abuse. Indicators that loaded onto the latent variable measuring substance abuse were alcohol abuse, cannabis abuse and other abuse. Meanwhile, the ability to perform household activities, self-care, overall residential performance, overall global work rating, global independent functioning, the latent variable measuring psychosocial support and the latent variable measuring parenting role loaded onto the latent variable measuring adaptive functioning. Indicators that loaded onto the latent variable measuring psychosocial support were overall socialising, number of friends, experienced stigma or discrimination due to mental illness, perceived loneliness, personal relationships, relationships with other people, relationships with family and satisfaction with case manager. Indicators that loaded onto the latent variable measuring parenting role were responsibility of childcare role and any form of contact with (step)children.
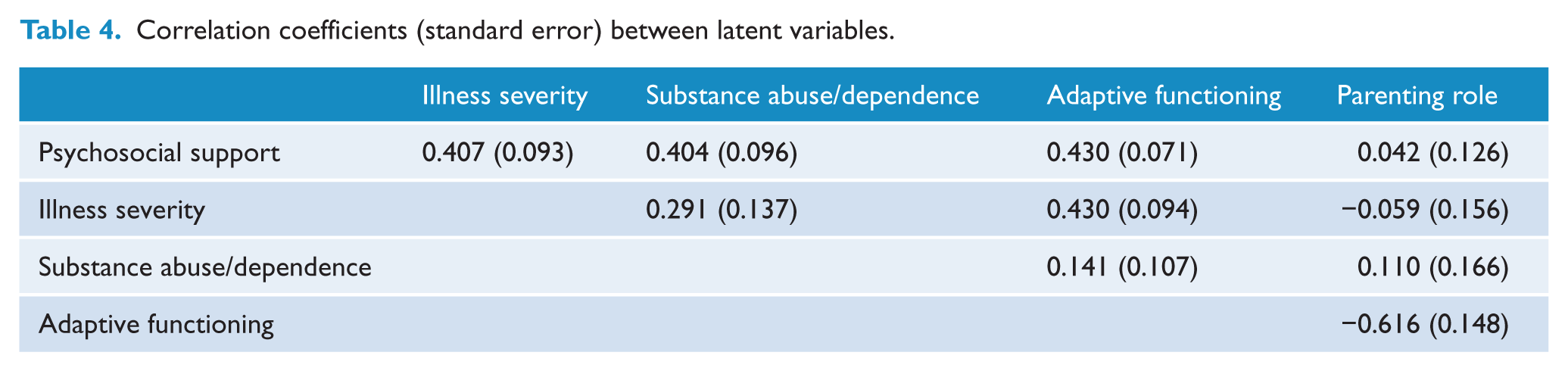
The influence of the remaining three latent variables on parenting outcomes was mediated by the illness severity and adaptive functioning variables. These associations were detailed in the SEM’s estimated correlations between the latent variables (see Table 4). The two predictive latent variables (illness severity and adaptive functioning) covaried significantly (est = 0.65, z = 6.6, p < 0.001). The latent variable measuring strength of psychosocial support loaded significantly on adaptive functioning (est = 0.51, z = 4.9 p < 0.001). The latent variable measuring parenting role loaded significantly on adaptive functioning (est = 0.59, z = 2.7 p < 0.01). Finally, the latent variable measuring substance abuse loaded significantly on illness severity (est = 0.49, z = 2.9, p < 0.01) (Table 5).
Correlation coefficients (standard error) between latent variables.
Loadings of latent variables onto outcome variable (quality of care).
Discussion
Parents with psychotic illness experience a high cumulative rate of adversities that makes parenting very challenging. Due to the long-term consequences of poor parenting, not only for the child but also the parent, it is important to identify parents at risk of providing inadequate quality of care to their children. The most pertinent finding in this study was that the majority of parents were functioning adequately, with 75% having no reported dysfunction in the quality of care of their child(ren) over the past 12 months. Wide dissemination of these findings could reduce the effect of stigma from members of the community, healthcare professionals and parents with psychotic illness. The knowledge that others in the same situation find strategies to cope and even flourish could bestow a sense of hope on parents with psychotic illness. This research provides some information about what predicted adequate parenting in the current sample.
We hypothesised that better adaptive functioning, less mental health symptomatology, low levels of substance abuse/dependence and strong psychosocial support would significantly be associated with, and predict, better quality of care of child(ren) in the last 12 months. Our hypotheses were partially supported with the two latent variables ‘illness severity’ and ‘adaptive functioning’ being significantly associated with quality of care of child(ren) in the last 12 months. These findings are important since they allow us to propose that attention in the clinical setting should continue to focus on ameliorating symptom severity and the concomitant experience of stigma, but should be fortified by a further concentration on adaptive strategies to improve everyday functioning. Each of these will be discussed in turn below.
Illness severity is a significant risk factor for poor parenting and has been identified in many studies (e.g. Mowbray et al., 2002). Consistent with the literature, the latent variable of illness severity in this study included the age at which the illness emerged (with younger illness onset associated with lower quality of care), while a longer duration of illness and lifetime presence of symptoms such as hallucinations, delusions, subjective thought disorder and self-harm were also associated with lower quality of care of children. Psychosis symptoms (and medication side effects), particularly negative symptoms, include a range of cognitive and emotional problems including lethargy, irritability, poor concentration, blunted affect, withdrawal and amotivation motivation (Evenson et al., 2008; Nicholson et al., 1998). The presence of such symptoms can make it difficult for parents to interact well with their children and to form appropriate relationships. Positive symptoms can include misinterpretation of information, and erratic and bizarre behaviours which may also adversely impact parenting (Ostler and Ackerson, 2009). It is not only important to recognise the impact that symptoms of mental illness have on child-rearing but also imperative to be cognisant of their frequently episodic and fluctuating nature. A well-designed longitudinal study showed that when mental illness symptoms decreased, parenting stress decreased and was associated with an increase of parental adaptive behaviours including nurturance (Kahng et al., 2008).
Meanwhile, the ability to perform household activities and carry out other residential obligations, to look after oneself appropriately, to function at work and overall global independent functioning loaded onto the latent variable adaptive functioning. Parents with poor functioning are likely to have difficulties caring for a child when not provided with appropriate support. Indeed, neglect is a risk factor for removal of children from the home (Ostler and Ackerson, 2009). Negative symptoms and cognitive impairments in particular make it difficult not only to plan but also to be motivated to accomplish daily parental tasks, such as providing meals and ensuring the children have clean clothes (Nicholson and Miller, 2008). As expected, the level of adaptive functioning was moderately associated with severity of illness, suggesting that parents with psychotic illness experience more problems in performing everyday activities when in a more active or severe phase of the illness. This then has a cumulative negative effect on the responsibilities associated with child-rearing.
The literature suggests that it is important to introduce a focus on the parent–child relationship as part of adaptive functioning. Forman et al. (2007) reported that while psycho-therapeutic interventions for mothers with postnatal depression could reduce mental health symptomatology and reduce parenting stress, no improvement in the parent–child relationship was found (Forman et al., 2007). In fact, early parental negative attitudes towards the child predicted more negative child outcomes at 18 months later. This combined with findings of an increased risk of poor developmental outcomes of children of parents with psychosis strongly suggests that intervention strategies focussed on adaptive functioning need to be family-centred (Liu et al., 2015). Family-centred approaches to improve adaptive functioning can include, for example, pre- and postnatal care, parenting skills such as building parent–child relationships and effective discipline and also social cognitive skills to facilitate greater parental sensitivity and responsiveness (Liu et al., 2015). In addition, a family-centred approach can also include support to other family members with the aim of helping parents cope more effectively not only with their illness but also in their role as parents. This is important because despite strong evidence for a link between psychosocial support and parenting outcomes in the literature (Chernomas and Clarke, 2003; Evenson and Simon, 2005), our results did not show a direct association between psychosocial support and quality of care for children. Instead, psychosocial support was associated with severity of illness and adaptive functioning, suggesting psychosocial support indirectly influences quality of parenting in the context of severity and adaptive functioning. Specifically and alarmingly, the results show that parents with the highest needs reported the lowest levels of psychosocial support. Indeed, parents with better psychosocial networks, including marital and social relationships, are more likely to have good parenting outcomes (Abel et al., 2005) and have been found to function better in times of crisis compared to socially isolated parents and to be less likely to lose custody of their children (Ackerson, 2003). Conversely, parenting stress is reportedly higher for mothers when they experience less psychosocial support and more social contextual risk factors such as frequent daily hassles (Kahng et al., 2008). Research on the general population suggests parents who have good psychosocial support have more adaptive interactions with their children and stronger parenting skills. Taken together with our findings, the growing recognition of the importance of psychosocial support for parents suggests greater need for longitudinal studies that model inter-relationships between psychosocial support and other factors relevant to parenting. An interesting, potentially related finding was that the majority of parents who had been in touch with child protection services over the past year were rated as providing adequate care for their children. Unfortunately, the nature of the available data did not allow for a closer examination of this finding, but there are several different explanations that might be possible. First, it is possible that the self-ratings are biased and that parents failed to recognise their own inadequacies, although careful interviewing of the parents using the established protocol should have minimised this bias. Second, it might also be so that contact with the child protection services either directly or indirectly (through partner organisations) provides the parent with help and assistance necessary to provide better care for their child, that is, the child protection services act as a psychosocial support structure.
The study also included other variables shown to be of interest to parenting outcomes in the general population. For example, substance misuse is generally recognised as a strong risk factor for poor parenting outcomes in the general population (Ostler and Ackerson, 2009) and occurred at a high rate in the current sample; however, abuse/dependence was only indirectly linked to parenting outcome through weak association with illness severity. Substance misuse potentially influences parenting outcomes for people with substance use disorders through other pathways. Indeed, the relationship between substance abuse/dependence and psychosocial support was moderate, indicating a risk of poor psychosocial networks for people with substance use disorders may be a significant factor to consider. Finally, the participants’ parenting role, that is, the amount of contact with children over the past 12 months and their childcare involvement, was also not associated directly with quality of care. However, it was significantly associated with adaptive functioning such that parents with lower levels of functioning did not interact as much with their children as parents with a higher level of functioning. This underscores the importance of parental functioning, indicating that treatment efforts aimed at improving parents’ functioning are also likely to benefit their children.
One of the strengths of this study of parenting is that it involved a large representative sample of people, receiving services or known to service providers, with psychotic disorders. However, due to the cross-sectional nature and diverse range of enquiry within the second Australian national survey of psychosis, the items mapping specifically onto the parenting section lacked sufficient detail to comprehensively explore the parenting experiences of the participants. For instance, it would have been preferable to have more detailed information regarding the parent and child and more than a single outcome to measure quality of parenting. Although the ratings were based on participant self-report and interviewer enquiry/exploration using probes and other relevant interview information, a more objective measure of parenting such as observational home-visits or dyadic interactions would have added value to this study.
Our findings underscore a growing body of literature stating that parents with psychotic illness are in high need of specifically targeted interventions addressing issues such as practical and social support and stress reduction related to parenting challenges, which commonly trigger illness relapse for many parents (Nicholson et al., 1998). Some clinical services may not consider the parenting status of clients and care is often designed to a ‘one-size-fits-all’ model (Fudge et al., 2004). Greater understanding of predictive factors for parenting difficulties and poor parenting outcomes would assist to improve targeting of appropriate and effective supports for parents and their children. Interventions should aim to include parenting techniques and also work on improving the parent–child relationship directly (Forman et al., 2007). However, while the emphasis on interventions and, by extension, research is most often centred of looking at the experiences of parents who are not doing well, our findings of a large cohort of parents who are doing well suggest that we also need to further explore their experiences.
To conclude, regardless of formidable challenges, parents with psychotic illness value their role as parents and being a parent is a critical part of their identity and daily lives. Our results indicate that there are many parents with psychotic illnesses who are doing well; however, the quality of their parenting is directly affected by their illness severity and daily functioning. Psychosocial support and substance abuse/dependence may indirectly influence the parenting ability of an adult with serious mental illness. In addition, financial hardship is present for many of these parents making it even more challenging to parent well. It is important to acknowledge that the support needs of parents with psychotic illness are likely to change episodically, and therefore, treatment plans should be flexible and targeted to times of greater needs. Consensus guidelines on care for people with psychosis including specific antenatal care recommendations can assist clinicians (Galletly et al., 2016; McCauley-Elsom and Kulkarni, 2007). However, it is important to not only consider mothers but also fathers. Indeed, parenthood, regardless of gender, needs to be viewed as more central to recovery from mental illness, along with connectedness, empowerment, future-centred hope and optimism as part of finding meaning and purpose in life (Tew et al., 2011). This will entail providing more effective and better-targeted treatment and support to parents with psychotic illness.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.