
Abstract
Objective:
Being a parent is an important part of one’s identity and role. Previous research outlines many challenges associated with parenting by people with severe mental illness. However, there is a limited research describing parenting experiences of mothers and fathers who have psychosis.
Method:
The second Australian national survey of psychosis recruited 1825 people living with symptoms of, or a diagnosis of, psychosis. The survey was conducted through face-to-face interviews and included key clinical and demographic information, as well as parenting specific information.
Results:
Over half of all women and a quarter of men were parents. Almost a quarter of women but only 5.5% of the men had dependent children (own and/or stepchildren) living at home with them. Of parents with dependent children, the most common diagnosis was schizophrenia (48.2% fathers, 28.9% mothers), and there were high rates of comorbidity with substance abuse/dependence (alcohol: fathers 69.2%, mothers 44.3%; cannabis: fathers 69.22%, mothers 47.8%). A substantial proportion of parents with dependent children experienced challenges including low educational attainment, unemployment, poverty, and social isolation. Although many parents living with dependent children functioned in the average range, a significant proportion was moderately to severely disabled on global independent functioning ratings (fathers 49.1%, mothers 35.7%) and some were identified as having obvious/severe impairments in their ability to care for their child(ren) (fathers 28.3%, mothers 21.3%).
Conclusions:
Most parents living with psychosis function well. However, a significant proportion has impairments in parenting and general functioning that could have adverse consequences for both the parent and children. This study brings into focus the need for interventions to optimise successful parenting outcomes.
Background
It is well known that parents with psychosis are likely to experience greater adversity compared to other parents. Aside from the challenges of the illness itself, these parents manage discriminatory behaviours and attitudes that they are not fit to be parents and experience social and self-stigma and a lack of targeted support services to assist them in proficient parenting (Ackerson, 2003b; Corrigan and Watson, 2002; Rüsch et al., 2005). Compared to the general population, parents with a mental illness have a higher likelihood of separation, divorce, and loss of custody of their children (Miller, 1997; Park et al., 2006). Since parental success has been linked with a sense of self-worth and competence and can increase motivation for seeking help to manage mental health problems (Evenson et al., 2008; Nicholson et al., 1998b; Oyserman et al., 2000), it is timely for service providers to examine the needs of parents with psychosis and the potential for programmes to improve and support their parenting skills (Howard, 2000).
To date, much of the focus of research and service development has been on the welfare of the children of people with severe mental illness (Miller, 1997). This child welfare perspective has led to the parents’ mental illness, rather than their individual experience as parents, being the primary concern of research and service provision. Further, instead of recognising the separation and loss suffered by both parent and child due to removal of children viewed as ‘at-risk’, research and service perspectives highlight the detrimental effects of keeping children with their biological parent with psychosis (Fudge et al., 2004). Consequently, parents in this position may lose access to their children as the courts may be more disposed to view them as incompetent parents (Nicholson et al., 1999; Reupert and Mayberry, 2009).
Despite indications that parent skills training as part of psychosocial treatment would be beneficial (Craig and Bromet, 2004), evidence-based parenting programmes are lacking (Nicholson, 2009). Further, both mothers and fathers with severe mental illness are reluctant to enlist agency help for fear of involuntary removal of children from their custody. Their reluctance to engage agency help may be further reinforced by awareness or personal experience of the risk of removal during the course of hospitalisation (Evenson et al., 2008; Hearle et al., 1999; Styron et al., 2002). Unfortunately, children have to be at significant risk of negligence or abuse before government or social services are able to intervene to help these parents raise their children (Ackerson, 2003b; Nicholson et al., 1999; Reupert and Mayberry, 2009). In addition, children’s services staff report feeling inadequately trained to deal with parents with severe mental illness, highlighting the need for better coordination between these services and mental health providers (Ackerson, 2003b; Azar et al., 1998).
Developing better services for parents with psychosis requires identifying the socio-demographic characteristics and needs of these people. Parents with psychosis have their first children around the age of 20 years and approximately 35% have had their first psychotic episode before parenthood (Craig and Bromet, 2004; Nicholson and Miller, 2008). A later age of onset and higher levels of education have been associated with better outcomes for parents with a severe mental illness (Craig and Bromet, 2004; Plant et al., 2002), and those with psychosis have better premorbid functioning compared to non-parents with psychosis (Nicholson and Miller, 2008).
The first Australian survey of psychosis highlighted stable accommodation and case management as being paramount in the amelioration of symptoms and the improvement of outcomes for people with psychosis (Morgan et al., 2006). Homelessness, insecurity of tenure, and a lack of sense of safety are risk factors for the exacerbation of symptoms leading to hospitalisation and custodial disruption, thus contributing to stigma, isolation, anxiety, and grief (Evenson et al., 2008; Folsom et al., 2005; Styron et al., 2002). Lack of safe housing can lead to child safety concerns for parents, and those with severe mental illness are more socially isolated and more likely to live below the poverty line than non- parent counterparts (Nicholson and Miller, 2008).
Social support including both material and emotional support are important for all parents regardless of mental health status. Severe mental illness can limit social networking and socialising skills. Although many parents with psychosis recognise that social supports would be helpful, they find it difficult to identify or maintain such support (Hearle et al., 1999). Fewer parents with severe mental illness live with a partner compared to those without mental health problems, and those who live with a partner experience greater difficulties in intimate relationships (Ackerson, 2003a; Nicholson et al., 2002; Reupert and Mayberry, 2009), making these parents less equipped to enjoy the benefits of enduring and supporting social networks. Instead, many parents with severe mental illness rely on their own parents to provide support to them in raising their children, a situation that can be both supportive but also a source of stress and conflict (Nicholson et al., 1998a).
There is limited research looking at gender differences in parenting experiences among people with severe mental illness. Fathers with psychosis have an earlier age of onset, more often have comorbid substance abuse compared to mothers with psychosis (Craig and Bromet, 2004), and have a very high risk of losing custody of their children (Reupert and Mayberry, 2009). Qualitative research indicates fathers experience a lack of support in their role from service providers and the community (Evenson et al., 2008; Reupert and Mayberry, 2009), even though fathers with serious mental illness are more likely to engage professional support, compared to mothers in this group who tend to seek help from non-professionals (Reupert and Mayberry, 2009). Clinicians are less confident in the information they provide to fathers compared to mothers and rate children as being more important to mothers than fathers (Nicholson et al., 1999).
The second Australian national survey of psychosis provides a unique opportunity to describe the experiences of parents with psychosis and the care arrangements for their dependent children in a population-based sample of parents with psychotic disorders. The aims of the current study were to report on clinical and social-demographic information for mothers and fathers living with psychosis and to describe family composition, caring arrangements and quality of care for own and stepchildren under the age of 18 years.
Method
Design
Comprehensive information about the study design and participants has been provided in earlier publications (Morgan et al., 2011, 2012).
The catchment for the second Australian survey of psychosis covered a population of 1.5 million people aged 18−64 years, approximately 10% of the Australian population in this age group. A two-phase design was used. In phase 1, screening for psychosis took place in public mental health services and in non-government organisations supporting people with a mental illness. In phase 2, people who were screen positive for psychosis in phase 1 were randomly selected and stratified by age group (18−34 and 35−64 years) for interview and assessment. This process identified 7955 people who were screen positive for psychosis and eligible for interview. Potential participants were randomly selected and approached to participate in the study; 1825 interviews were undertaken in phase 2 of the study. Diagnostic assessment was based on a semi-structured clinical research interview, the Diagnostic Interview for Psychosis (Castle et al., 2006). Diagnoses were made using the ICD-10 classification system (World Health Organization, 1992).
Interviewers
Data were collected and rated by interviewers who had professional mental health backgrounds and who based their judgments on participant responses throughout the course of the interview and the specific probes for specific items. To ensure interrater reliability, interviewers and site coordinators attended national training workshops, onsite training, weekly teleconferences, and interrater reliability testing at start and end of data collection as well as a number of time-points throughout the duration of the study.
Participants
A total of 7955 people were screened positive for psychosis and randomised for interview in phase 2. From the randomised list of people, the second national survey of psychosis interviewed 1825 people from April to December 2010. The exclusion criteria were people with insufficient English, people with communication or cognitive impairment that would hinder their capacity to give consent or participate in the interview, and people residing in prison and nursing homes at the time of interview (n=501). For more information about sample composition, please refer to Morgan et al. (2011, 2012). The current study describes the subset of participants, aged between 18−64 years old, who identified themselves as parents. Human research ethics approval was obtained at institutional local, state, and national levels as required at each site. All participants provided written informed consent.
Participants were interviewed by mental health clinicians using a survey consisting of 33 modules of questions, some close-ended, others open-ended. The survey included questions about accommodation, income, substance use, stigma, and social and occupational function. In addition, the participants were asked a series of questions about their children (if any) and their situation regarding parenting; while diagnosis, age of onset, and course of illness were determined using the Diagnostic Interview for Psychosis (Castle et al., 2006). Diagnoses were made using the ICD-10 classification system (World Health Organization, 1992). Global independent functioning was measured using the Multidimensional Scale of Independent Functioning. This rating is corrected for level of support and performance relative to community norms and reflects an overall level of disability taking into account performance at work (paid and unpaid work/childcare/caring), in study, and in activities of daily living (Jaeger et al., 2003).
Analysis
Descriptive statistics were extracted using IBM SPSS statistical software (version 19.0; SPSS, Chicago, IL, USA). Chi-squared tests were used to assess univariate associations between nominal variables. To interpret the chi-squared tests, adjusted residuals were inspected to provide information on how far the observed count was from the expected count; a cut-off value of 2 was utilised. To measure the strength of association among the levels of the row and column variables, Cramer’s V is reported (>0.5, high association; 0.3−0.5, moderate association; 0.1−0.3, low association; 0−0.1, little if any association).
The dependent variables included were: (1) clinical variables; (2) social-demographic variables; (3) functioning and quality of life; and (4) childcare including caring arrangements, presence/absence of children requiring intense levels of care (including, for example, regular insulin, dialysis, or Activities of Daily Living (ADLs) associated with disability), care taking responsibilities, contact with the state’s relevant department of community services, and an interviewer rating of quality of caring for children in the past 12 months.
Results
Parents with psychosis
Diagnostic characteristics and demographics
Of the 1825 participants in the survey, a significant minority (38.1%) had children of any age (n=696; 281 men, 415 women; Table 1). More than half of the female participants (56.2%) had children of their own of any age, whilst 5.3% had stepchildren. The respective percentages for male participants were 25.9 and 4.8%. Mothers were more likely to have dependent children living with them than fathers (23.6 versus 5.5%, respectively).
Demographic and diagnostic characteristics of all parents (includes parents of adult and dependent children) by gender
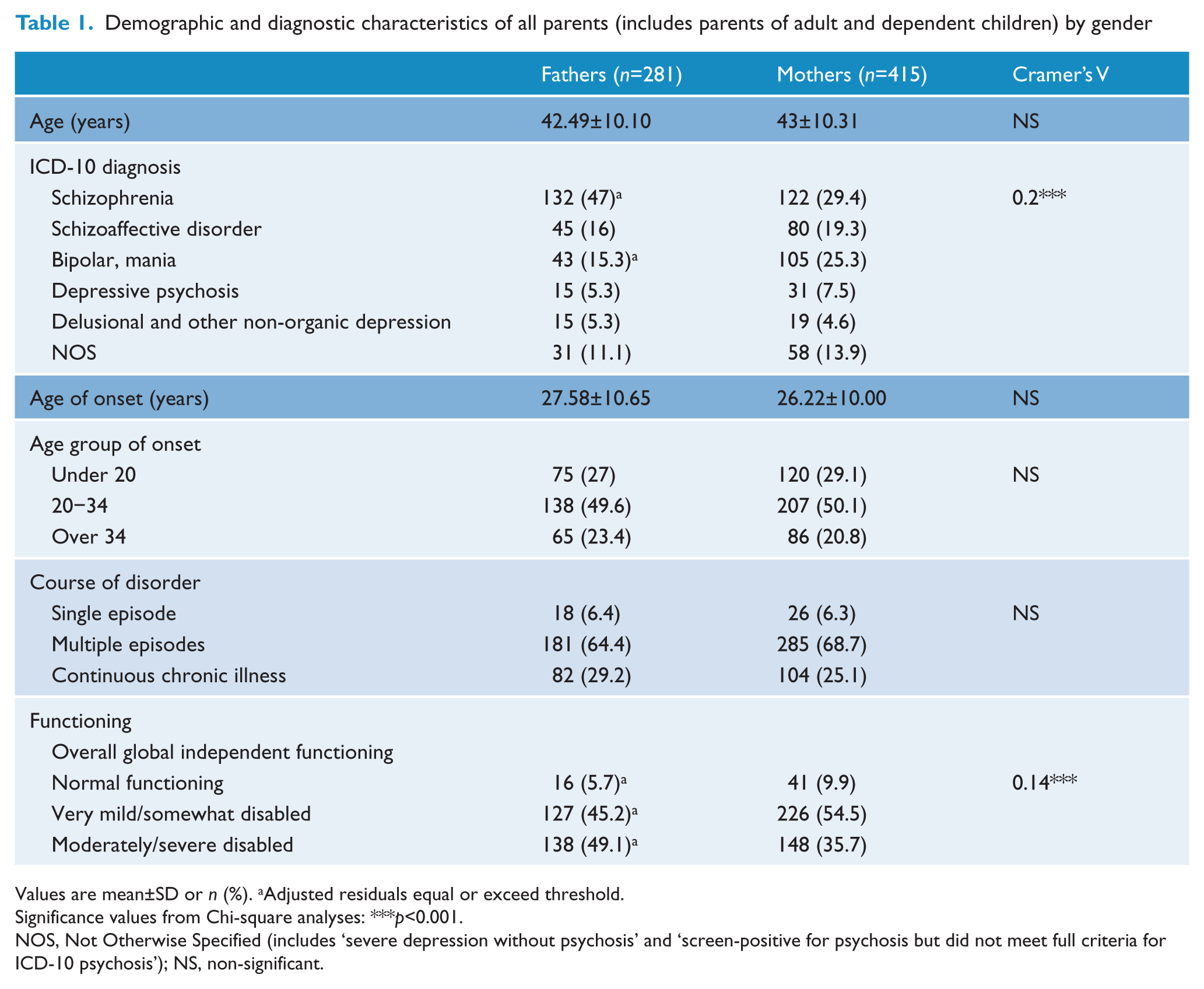
Values are mean±SD or n (%). aAdjusted residuals equal or exceed threshold.
Significance values from Chi-square analyses: ***p<0.001.
NOS, Not Otherwise Specified (includes ‘severe depression without psychosis’ and ‘screen-positive for psychosis but did not meet full criteria for ICD-10 psychosis’); NS, non-significant.
More than 60% of parents experienced multiple episodes of illness and 29.2% of male and 25.1% of female parents experienced continuous illness (Table 1). The most common diagnoses were schizophrenia, schizoaffective disorder, and bipolar mania. Mothers had significantly lower rates of schizophrenia and higher rates of bipolar/mania compared to fathers [χ2(6, n=696)=27.57, p<0.0005, Cramer’s V=0.2]. Almost half (49.1%) of male parents and 35.7% of female parents were moderately to severely disabled as per the global independent functioning scale (Table 1). Of the parents, 35.9% of the mothers and 26.7% of fathers had own children under 18 years of age, whilst the remainder had adult children only.
Parents with dependent children
Social demographics and clinical information
In this section, we outline the characteristics of parents with children under the age of 18 years (n=195 men and 253 women; no distinction is made between own children and stepchildren; Table 2). There was no significant age difference between the mothers and fathers (p>0.05). The majority had one or two children living with them (80.8%), although 15% had three or four children and 4.3% had five or more children living with them.
Clinical and social demographic information for parents with dependent children (including own and stepchildren)
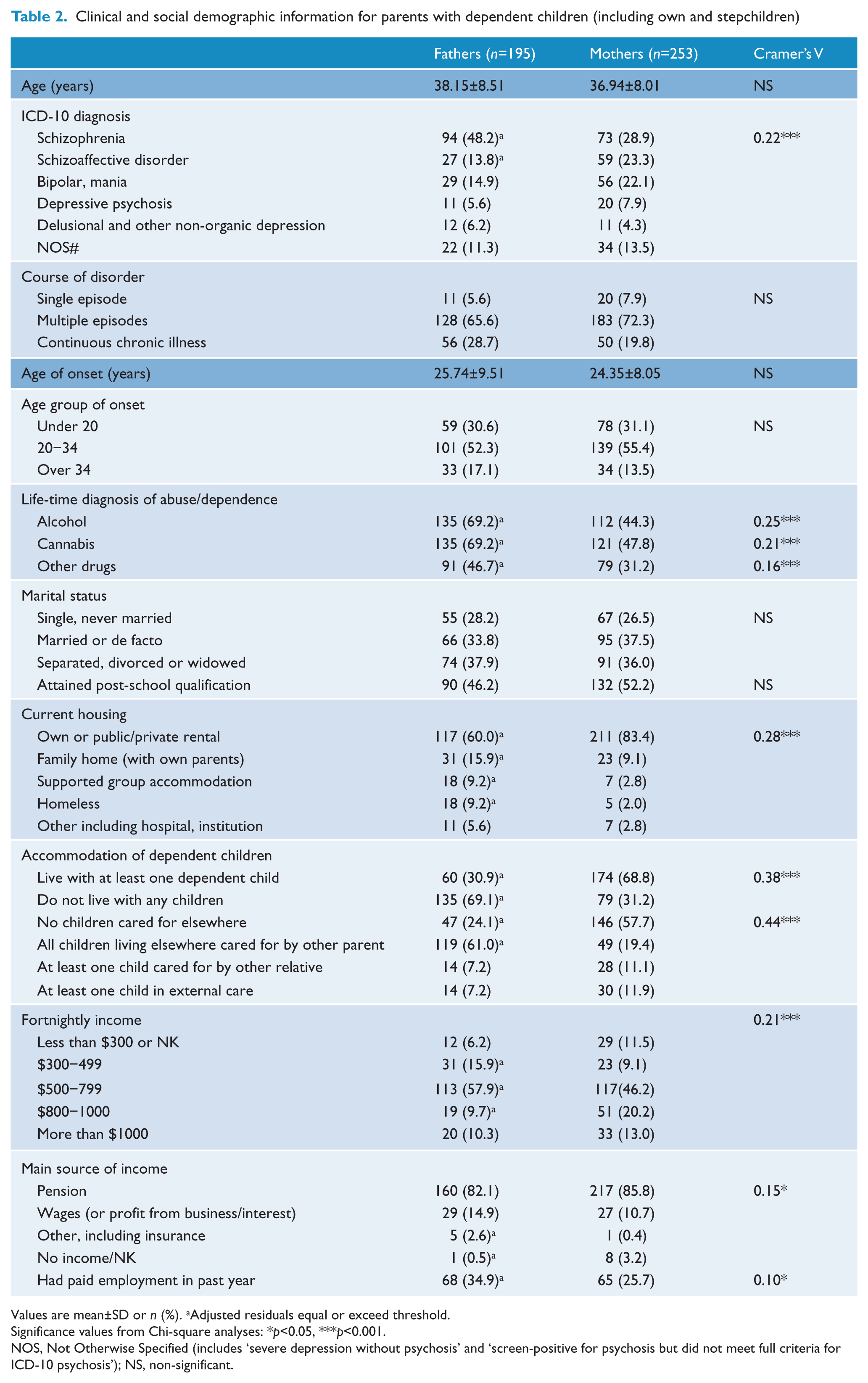
Values are mean±SD or n (%). aAdjusted residuals equal or exceed threshold.
Significance values from Chi-square analyses: *p<0.05, ***p<0.001.
NOS, Not Otherwise Specified (includes ‘severe depression without psychosis’ and ‘screen-positive for psychosis but did not meet full criteria for ICD-10 psychosis’); NS, non-significant.
Approximately one-third of parents with dependent children was married or in a de-facto relationship, one-third was separated or divorced parents, and one-third single (Table 2). Just under half the mothers compared to almost 70% of fathers had a life-time additional diagnosis of alcohol abuse/dependence [χ2(1, n=448)=27.74, p<0.0005, Cramer’s V=0.25] and/or cannabis abuse/dependence [χ2(1, n=448)=20.60, p<0.0005, Cramer’s V=0.21; Table 2].
The types of accommodation for parents differed between mothers and fathers [χ2 (4, n=448)=34.27, p<0.0005, Cramer’s V=0.28; Table 2]. Mothers (83.4%) were more likely to live in their own home or rented accommodation compared to fathers (60%). In addition, a larger than expected proportion of fathers, compared to mothers, lived with their own parents (15.9%), in supported group accommodation (9.2%), or were homeless (9.2%).
The majority of parents with dependent children had fortnightly income of between AU$500−799, with the main source of income being a pension. However, it was more common for mothers to have incomes in the higher brackets compared to fathers [χ2(4, n=448)=18.93, p<0.001, Cramer’s V=0.21; Table 2]. Only around one-quarter of mothers and one-third of fathers had paid employment in the past year.
When comparing the proportion of parents who lived with dependent children compared to those who did not live with dependent children, it was found that it was more common for people who lived with children to be in a stable relationship whilst those who did not live with their children more often were single or separated, divorced or widowed [χ2(2, n=448)=53.17, p<0.0005, Cramer’s V=0.34; Table 3]. There was no difference in attainment of post-school qualifications or employment in the past 12 months but it was more common for parents living with dependent children to have higher fortnightly incomes [χ2(4, n=448)=50.08, p<0.0005, Cramer’s V=0.33; Table 3].
Characteristics of parents with dependent children, living with or living apart from their children
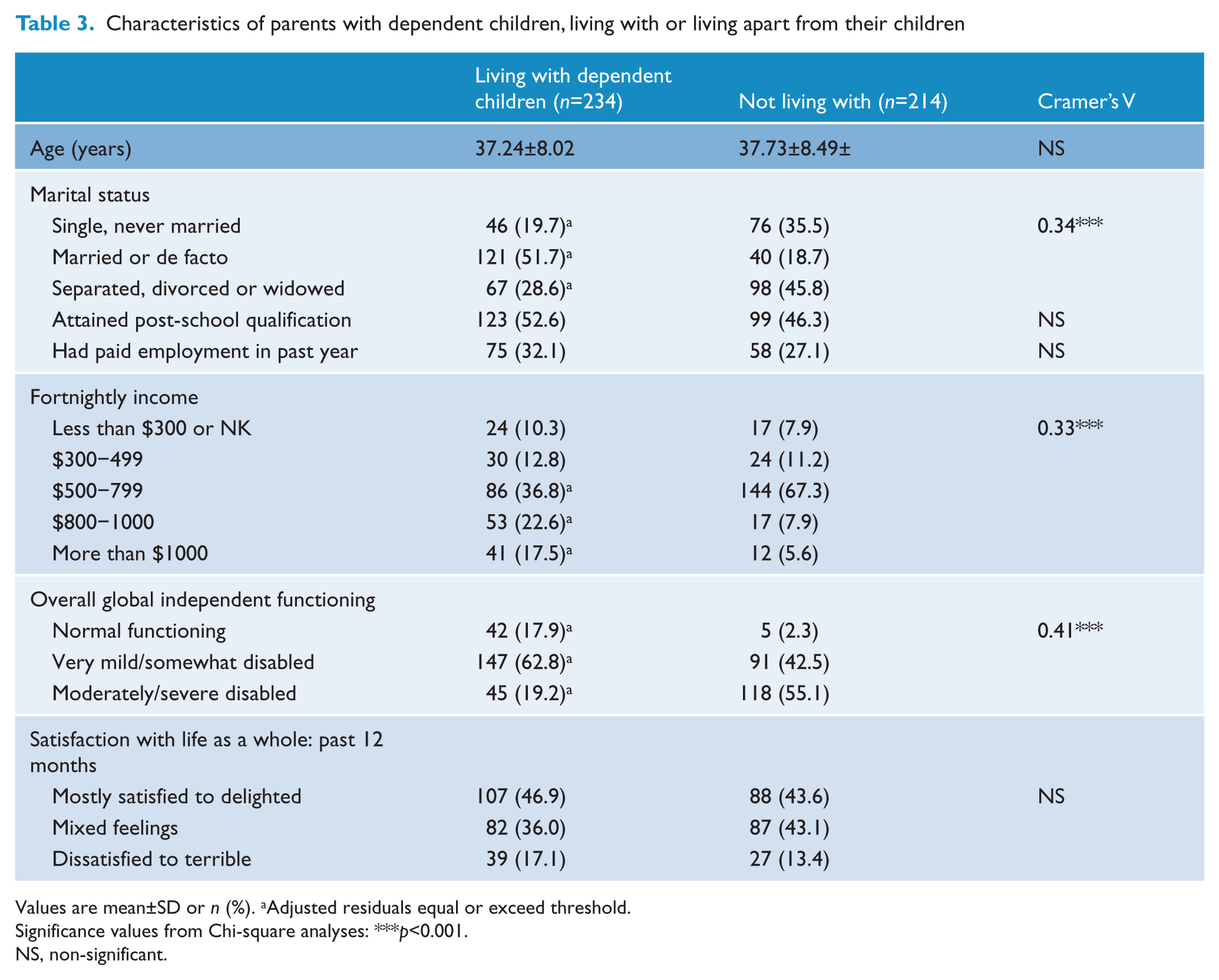
Values are mean±SD or n (%). aAdjusted residuals equal or exceed threshold.
Significance values from Chi-square analyses: ***p<0.001.
NS, non-significant.
Functioning and quality of life
Whilst most parents living with dependent children (45.7%) had no perceived difficulties with household responsibilities in the last 4 weeks, 30.9% reported that they had some difficulties, and 18.8% reported they had a lot of difficulties. The perceived reason for difficulties with household activities in the last week was reported as due to mental health issues (53.5%), both mental and physical health (22.8%) or physical health (15.8%). Global independent functioning of parents with dependent children indicated that whilst some individuals were functioning in the normal range (mothers 13%, fathers 7.2%), a large proportion was functioning in the mild to somewhat disabled range (mothers 60.1%, fathers 44.1%) or in the moderate to severely disabled range [mothers 26.9%, fathers 48.7%; χ2 (2, n=448)=23.34, p<0.0005, Cramer’s V=0.23; Table 4].
Functioning and quality of life for parents of dependent children (including own and stepchildren)
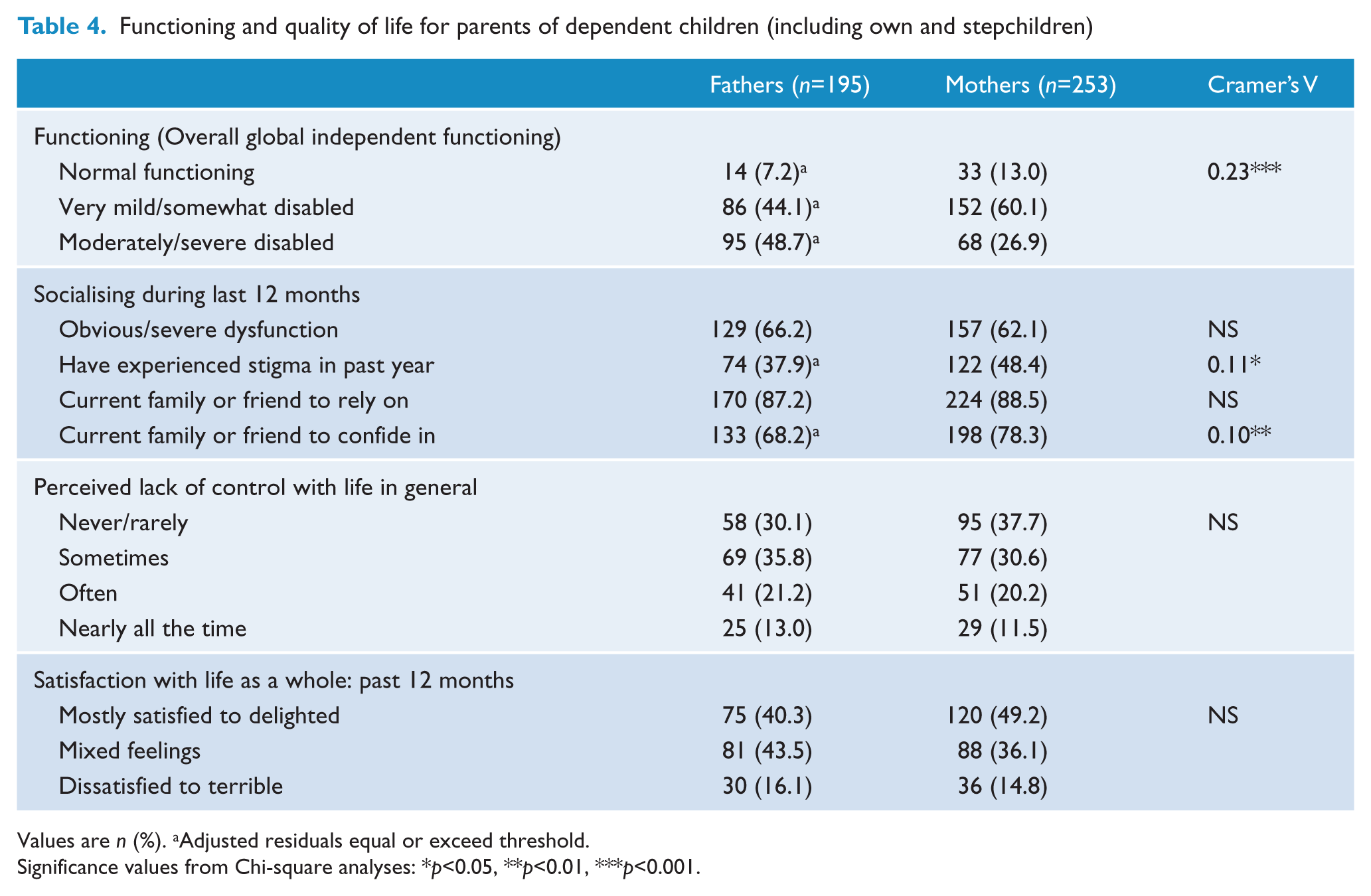
Values are n (%). aAdjusted residuals equal or exceed threshold.
Significance values from Chi-square analyses: *p<0.05, **p<0.01, ***p<0.001.
The majority of participants reported that they had a family member or friend upon whom they could rely if they had serious problems (fathers 87.2%, mothers 88.5%; Table 4). Further, most parents felt that they had someone to share their thoughts and feelings with, although this was less common for fathers (68.2%) compared to mothers (78.3%) [χ2(1, n=448)=5.78, p<0.01, Cramer’s V=0.11; Table 4].
When comparing the proportion of parents who lived with dependent children compared to those who did not live with dependent children, it was found that more parents who did not live with their children (55.1%) had a moderate to severe disability with regards to overall global independent functioning compared to those who did live with their children [19.2%; χ2(2, n=448)=74.25, p<0.0005, Cramer’s V=0.41; Table 3]. Mothers were more likely to have daily contact with fathers [χ2(2, n=448)=0.139, p<0.01, Cramer’s V=0.13; Table 5].
Contact experience for fathers and mothers with dependent children (including own and step children)
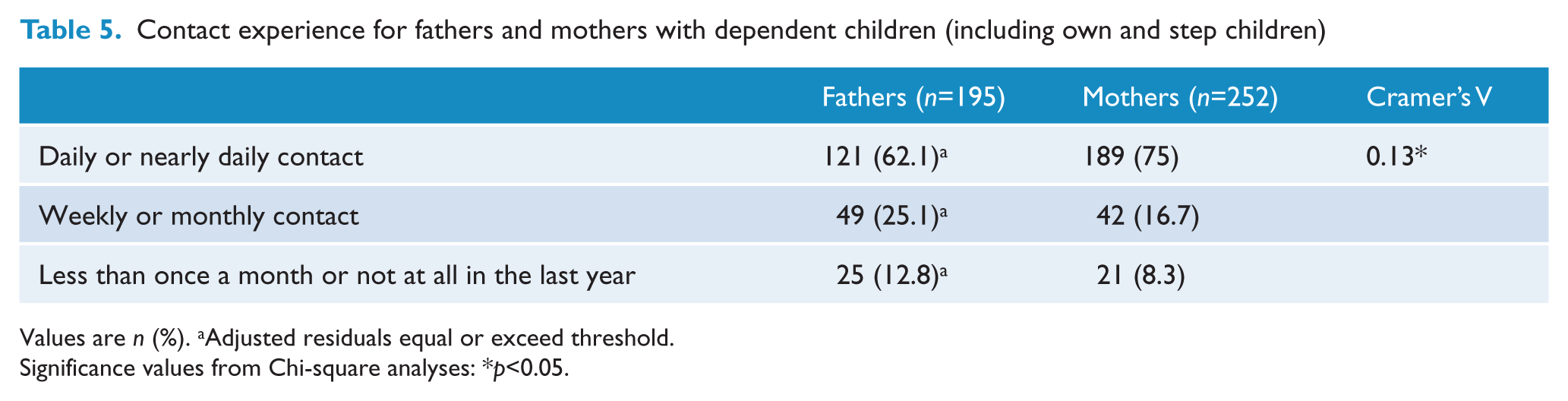
Values are n (%). aAdjusted residuals equal or exceed threshold.
Significance values from Chi-square analyses: *p<0.05.
Childcare and quality of care
Of the mothers living with a child, 69.5% considered themselves as the primary caregiver, with an additional 21.3% sharing caring responsibilities equally. Meanwhile, 21.7% of men considered themselves as the primary caregiver, with 45% sharing equal responsibilities for care giving (Table 6).
Parents living with dependent children (including own and stepchildren)
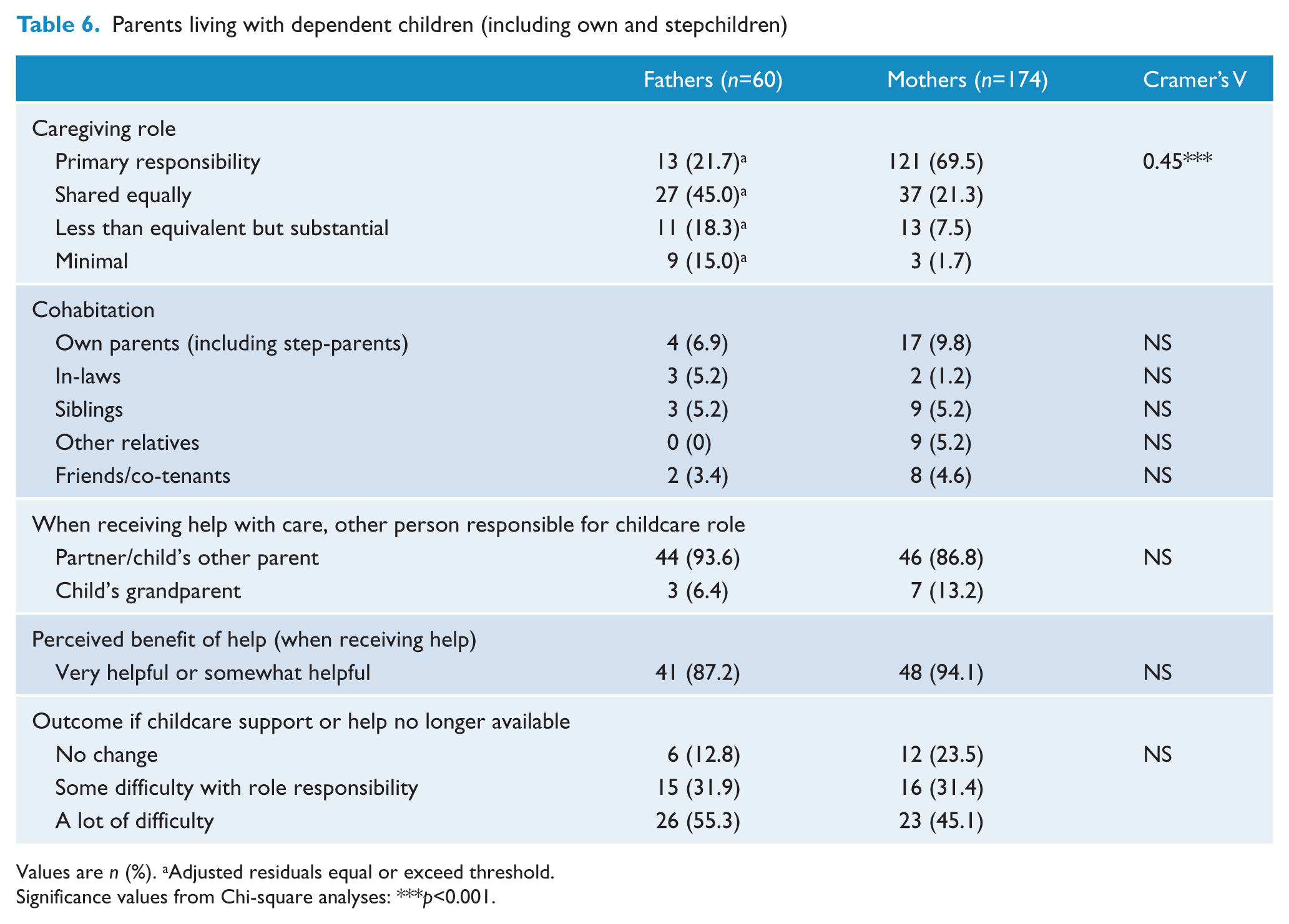
Values are n (%). aAdjusted residuals equal or exceed threshold.
Significance values from Chi-square analyses: ***p<0.001.
Interviewers rated the majority of parents (76.6%) as providing a good quality of care for their dependent children in the past year. However, it was found that 21.3% of the mothers and 28.3% of the fathers had obvious or severe impairments in their ability to care for their child or children. A quarter of the parents (25.2%) had been in contact with their state department of family/community services in the last 12 months. Behavioural (e.g., conduct disorders) and medical problems in children that required intense levels of care (e.g., dialysis) affected 17% of fathers and 24.7% of mothers. Of the parents with dependent children, who reported receiving help or support from non-government health agencies (n=99), 40% reported that they had been provided advice or support with parenting. In addition, 12% (55 of 442) of parents reported that they had had contact with services providing specific support for their family.
Discussion
The current survey indicates that the number of parents with psychosis has increased since the first Australian national survey of psychosis and improves on that survey by identifying more parenting-specific information. This study has additionally enabled a more thorough examination of caring arrangements for parents, with specific attention paid to those with dependent children. Importantly, we also focused on the possible differences between mothers and fathers with psychosis. However, it was not the focus or scope of this paper to compare parents with psychosis to those without.
In this second national survey, more than half of the women and one-quarter of men with psychotic disorders were parents. Compared to the first national survey, the overall proportion of parenthood had increased for both women and men (women from 50.5 to 56.2%, men from 21.3 to 25.9%). In contrast with the decline in parenthood in the general population in Australia (Gray et al., 2008), our data indicate that the number of families in which at least one parent suffers from psychosis is growing and this finding is in agreement with the general literature suggesting that, since deinstitutionalisation, the rate of parenthood among people with severe mental illness is increasing (Monds-Watson, 2010). Similarly, the number of Australians with psychosis living with dependent children (own and/or stepchildren), particularly women, has increased since the first survey of psychosis (women from 14.5 to 23.6%, men from 3.6 to 5.5%). Hence, services and government can now further develop sexual health counselling and specialist perinatal psychiatry services and provide opportunities for greater collaboration with obstetric, midwifery, and community outreach services for those with a mental illness intending to be parents. These services should consider the differences in help-seeking between fathers and mothers and their perceived benefit from that help-seeking, as well as the difficulties faced by children’s support services staff in addressing the needs of parents of either sex. While there are fewer fathers than mothers with psychosis, there is certainly an increase for both since the first survey, indicating increased needs for parenting support. It was found that a large number of parents with dependent children were either separated or single compared to in the general population (one-fifth of families with children under 15 being lone parent families (Linacre, 2007), indicating an increased risk for social disadvantage and a need of additional social support.
Only half the parents with dependent children had attained post-school qualifications, and successful employment outcomes were low. Taken in light of recent advances in early intervention, this is disappointing; however, the current cohort comprised many more participants in the older age group (over 35 years) than younger. The study revealed that the main source of income across mothers and fathers alike was a disability pension. Sadly, one-fifth of parents living with dependent children were found to live on incomes below the Australian estimated poverty line (AU$577 per fortnight per single adult as per December 2010) (Melbourne Institute of Applied Economic and Social Research, 2011). In the general population, data from 2006 indicated that 11.1% of Australians, including 7% of couples with children and 16% of single parent families, lived in poverty (Saunders et al., 2008). It was also found that a larger proportion of fathers lived in supported group accommodation, institutions, or were homeless compared to mothers who were more likely to live in their own home or rented accommodation. These data suggest that services should pay additional attention to reviewing access to social services supports and give weight to assisting the 20% of parents who are living below the poverty line with financial planning. Services which address homelessness and insecurity of tenure should be encouraged, particularly for the sake of these fathers.
The extended support networks available to parents with a mental illness suggest that, although many parents struggle with financial, emotional, and accommodation hardship, their social support networks often provide valuable assistance. The survey also confirmed that although most of the mothers lived with their dependent children, a substantial proportion of mothers and the majority of fathers had at least one child living elsewhere (mothers 42.3%, fathers 75.8%). Whilst most children were cared for by the other parent, around 7% fathers and 11% of mothers had children in the care of another relative and a similar number had children in external care including foster-care or adoption. In part, carers and supporters of parents with mental illness are vital cogs in the maintenance of social connectedness and sense of wellbeing in this group.
This survey highlighted that many parents (17% fathers, 24.7% mothers) had dependent children with high-intensity care requirements, including both behavioural and medical conditions, which may add a significant load on parents already heavily burdened. Unfortunately, the current analysis was not able to characterise the particular problems that these children had but it was reported that most of these children (84.4%) attended school, daycare, or other activities during the day. Further research is needed to determine the nature and extent of these disabilities. This presents new information for child and youth mental health services and the Departments of Health and Education to further coordinate existing programmes and identify more accurately these children and their parents.
The majority of parents with psychosis who lived with dependent children were found to function well with regards to quality of care for their dependent children in the past year, despite many parents having at least a mild level of disability of functioning, and to participate in childcare as much as an average carer of same sex/ age group would under similar circumstances. However, around a quarter of parents were rated as having obvious or severe impairments in the ability to care for their child or children. This is further reflected in a large number of parents having difficulties coping with their household responsibilities and who rated as having a moderate or severe impairment in global independent functioning. In addition, many parents felt that they at times or often had a lack of control with their life in general.
Together, these findings indicate that whilst many parents with psychosis are coping well with parenthood, there are some parents who have great difficulty in fulfilling their caring roles and require substantial physical and emotional support. Over the last decade, there has been an increased focus on support for parents through national resources such as the government-funded initiative the Early Intervention Services for Parents, Children and Young People; the Australian Infant, Child, Adolescent and Family Mental Health Association; and, for the children, the Children of Parents with a Mental Illness (COPMI) programme. Initiatives such as COPMI highlight the importance of increased coordination of adult mental health services and children’s services.
Limitations
The second Australian survey of psychosis is one of very few studies to collect comprehensive data on parenting in people with psychosis. In addition, comparison with data from the first survey allows an assessment of change over time. Although the survey included a section on childcare, it did not include items on how the parents perceived the impact of their psychosis on their role as parents. The current survey was cross-sectional and therefore it is not possible to infer the directionality of the findings. In addition, the survey did not identify intermittent or atypical custody arrangements. One important caveat for the interpretation of variables such as quality of care for children was that the interviewer based their rating on participants’ self-reports rather than being able to utilise observational data. It is also important to note, that despite significant Chi-squared analyses, the size of the sample may have unduly influenced some of the findings, as indicated by Cramer’s V. Further, the current study excluded participants who did not speak English and those with low intellectual functioning.
While the current study did not examine differences between participants who had children of any age (n=696) and those who did not (the remainder of the 1825), this will be addressed in a future publication, as it was outside the scope of the current manuscript to do such an analysis.
Conclusion
The present survey suggests that many parents with psychosis function well, which bodes well for chances of recovery and continued good functioning. They show strength of character, resilience in the face of adversity and discrimination, and promise for others who may follow in their footsteps. However the survey also shows that some parents with psychosis face many challenges including low educational attainment, unemployment, poverty, social isolation and stigma, significant childcare demands, and a high risk of loss of custody of their children. There is a need for more numerous and effective services to further assist parents with psychosis to provide optimal parenting for their children.
Footnotes
Acknowledgements
This publication is based on data collected in the framework of the 2010 Australian National Survey of High Impact Psychosis. The members of the Survey of High Impact Psychosis Study Group are: V Morgan (National Project Director), A Jablensky (Chief Scientific Advisor), A Waterreus (National Project Coordinator), R Bush, V Carr, D Castle, M Cohen, C Galletly, C Harvey, B Hocking, A Mackinnon, P McGorry, J McGrath, A Neil, S Saw, H Stain. Ethics approvals for the study were obtained from relevant institutional human research ethics committees. The study was funded by the Australian Government Department of Health and Ageing. This report acknowledges all the effort and hard work by the local site coordinators. We would also like to thank, the hundreds of mental health professionals who participated in the preparation and conduct of the survey and the many Australians with psychotic disorders who gave their time and whose responses form the basis of this publication.
Funding
The study was funded by the Australian Government Department of Health and Ageing.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.