
Abstract
Early intervention into prodromal schizophrenia has shown promise, but controversy continues regarding the ethical acceptability of identifying a group of ‘ultra high risk’ individuals of whom only 30 to 50% will develop a psychotic disorder. With well developed early intervention services this group faces the possibility of being labelled as ‘pre-psychotic’, a condition for which the well known stigma associated with the diagnosis of schizophrenia or bipolar disorder is likely to be associated. In addition, the use of potent antipsychotic and other medications (albeit usually at lower doses than those used for those with manifest psychosis) mandates consideration of the risks associated with their use and neurological and metabolic side effects. The potential for iatrogenic morbidity in the ‘false positive’ group must be weighed against the need of the ‘true positives’ identified through screening and assessment. Current evidence for the concept of ‘at-risk mental state’ was reviewed within a neurodevelopmental framework, including emerging data on the effectiveness of early intervention for the purpose of providing recommendations for community mental health services. The review suggests that different treatment strategies may be appropriate depending on the clinical stage of the condition as long as the benefits of intervention outweigh its risk burden. It further suggests that the severity of psychoses and the evidence of its early onset in utero and its acceleration in adolescence positions ‘ultra high risk’ intervention as a core model for early intervention for young people by teasing apart the symptomatic components of the ‘prepsychotic state’ and ensuring the population is reaching targeted mental health services for screening. The model is not restricted to the delivery of intervention for ‘pre-psychotic’ young people but is applicable for targeted programmes for a number of clinical groups considered at ‘ultra high risk’. However, only further research in naturalistic populations embedded in clinical practice and ideally conducted in partnership of mental health services with academic research institutions will help clarify potential risks of early identification and intervention and assist in updating and making more explicit the clinical guidelines services will use in approaching those in the ‘ultra high risk’ group.
The challenge of prodromal schizophrenia
A substantial body of research with pioneering contributions from Australia over the past two decades has informed the feasibility, reliability and validity of identifying adolescents and young adults who are carrying a significant risk of developing a psychotic illness [1]. This scientific evidence of the ability to identify young people at risk for psychosis is now under consideration for inclusion into a revised DSM-5 [2].
More recent research has increasingly focused on longitudinal studies into early intervention when targeting ‘ultra high risk’ (UHR) populations with specific modes of intervention ranging from psychosocial approaches to medication treatment. While not providing evidence for prevention other than a delayed onset of clinical manifestation of a psychotic illness [3], together these studies demonstrate beneficial outcomes in terms of better treatment compliance, higher rates of participation in formal education and the workforce, and reduced hospital admissions once the psychotic illness has fully emerged [4].
This emerging evidence of beneficial effects of early intervention in the prodromal phase of illness is of profound importance when considering strategies of efficient and cost-effective health care delivery. While psychotic spectrum disorders only affect a relatively small proportion of the population when compared to high prevalence disorders such as major depressive, anxiety and substance abuse disorders that also emerge in the UHR age range of 12–25 years; affective and non-affective psychotic disorders account for a high proportion of psychiatric hospital admissions, the prison population, workforce drop-outs, and certainly constitute a huge burden for families who are facing the problem of largely unassisted primary care on a daily basis [5,6]. Hence any effective mode of early intervention in the prodromal phase of illness has the potential to reduce a significant proportion of public health care spending and decrease the impact on families and carers.
Unfortunately there is little evidence to suggest established mental health services are actively pursuing the necessary changes in work practices to take into account these new findings. Other than a few specialized and research-intensive centres in Australia and around the world, public mental health services show little inclination to change the current approach of predominantly delivering services around crisis care, emergency hospital admissions and community aftercare. An element of early intervention can usually be found in child and adolescent mental health services but often lacks the specificity and the conceptual framework to deal with the problem, and there is rarely an option for continued syndrome-specific care as clients become adults. UHR and the onset of high prevalence mental disorders fall into an age range that sits on the margins: too old and often too difficult to deal with in the child and adolescent setting versus not ill enough to make the triage in the adult setting. Not surprisingly, specialized youth mental health services such as Headspace in Australia are emerging outside the public sector in response to the lack of appropriate public services. However, these initiatives also have limitations by often lacking tertiary expertise and due to a reliance on the private sector.
The current paper will review the evidence around the concept of ‘at-risk mental state’ and the effectiveness of early intervention in UHR cohorts by reviewing the evidence for the neurodevelopmental model of schizophrenia and examining service models. The paper will conclude with recommendations for the treatment of UHR young people within community mental health services and particularly in rural services.
Neurodevelopmental model of schizophrenia
For many years there has been debate over whether schizophrenia is a neurodegenerative disorder as suggested by continuing decline in functioning for some people over the course of the illness. However, longitudinal studies have not shown progressive decline in neurocognition in schizophrenia [7]. Rather than cell atrophy or apoptosis occurring in schizophrenia, the evidence suggests normal brain development has been disrupted or over-activated. This is particularly noticeable during adolescence when fine tuning of neural connectivity occurs through processes such as synaptic pruning [8].
Neuroimaging studies have demonstrated both structural and functional brain changes during adolescence for young people who later develop schizophrenia. Several cross-sectional studies have shown reduced grey matter volume in the prodromal stage of schizophrenia [9,10]. A follow up study of UHR individuals has shown these deviations from normal brain development that are evident as reduced grey matter volume during the at-risk or prodromal period continue throughout the early years of the illness itself [11]. Other early signs of neuropathology and associated functional impairment in the emerging illness, however, may only be transient and phenotypically different from those found in established illness [12].
While adolescence is the period closely preceding the onset of psychosis for many people, the neurodevelopmental theory proposes that the aetiology of the disorder begins in utero through altered gene transcription and expression. The changes in utero then set the pattern for the altered course of brain development in adolescence. Minor physical anomalies and dermatoglyphic deviations in adults with schizophrenia are consistent with insults in the first or second trimester [13,14]. The neurological impact of in utero changes on the later course in adolescence results in impaired connectivity both at a structural and functional level [8,15,16]. As well as an influence on synaptic pruning, in utero changes impact on the cell migration for axonal development and connectivity. For example, there is evidence of changes in the cortical sub-plate, a transient structure present during second and third trimester that guides the formation of cortical connections [17]. Animal studies of prenatal insults have identified changes in biological markers such as protein expression that are involved in early migration of neurons, cell proliferation and synaptogenesis [18]. These ‘risk’ genes interact with environmental events in the pre- and perinatal periods such as maternal viral infections during pregnancy or obstetric complications (notably foetal hypoxia) – both known risk factors for schizophrenia [19–22]. Some of the schizophrenia candidate genes such as brain-derived neurotrophic factor (BDNF) are regulated by hypoxia [21,23]. Pre-natal nutritional deficiencies such as folate and vitamin D have also been implicated in adult risk for schizophrenia [24,25]. It is important to note that current evidence indicates schizophrenia has a complex mode of heritability and varied expression with an aetiology emanating from interactions of multiple genes and environmental insults [26].
While some researchers have debated between the neurodevelopmental and the dopamine theories of schizophrenia, Murray et al. [27] posited the dopamine hypothesis within the neurodevelopmental model. Murray strongly argued that dopaminergic activity was implicated in all the developmental risk factors for schizophrenia and that it provided a clue to the full development of psychotic symptoms as compared to the ultra high risk state [27]. However, this argument did not fully address the genetic factors, in particular the changes in utero. Others have proposed that schizophrenia is associated with heightened dopamine activity commencing in late adolescence [28], or with increased dopamine turnover [29]. Howes and Kapur propose increased pre-synaptic striatal dopaminergic function as the common final pathway that accounts for synergistic and cumulative effects of pregnancy and obstetric complications, stress and trauma, drug use, and susceptibility genes in the pathogenesis of schizophrenia [30]. For instance, dysbindin (a schizophrenia susceptibility gene) has been shown in dysbindin mutant mice to be associated with an increase in dopamine turnover in the cortex and hippocampus [31] while cumulative exposure of psychosocial stress has been linked to dysregulation of the hypothalamus-pituitary-adrenal axis, thus contributing to a hypothesized final common pathway of dopamine sensitization in mesolimbic areas and increased stress-induced striatal dopamine release. Altered dysbindin expression has been shown to impact on neural development due to changes in actin skeleton [32] while disturbed post-natal brain maturation has been linked to neuregulin-1 (NRG1) and disrupted-in-schizophrenia-1 (DISC1) genes [33].
In summary, there is strong evidence for adolescence as a critical period of brain change but that this is dependent on changes that have already occurred in utero or even at conception when taking increased risk with paternal age of 55 and over into account [34]. Importantly, these factors are not causative since they only suggest increased vulnerability which may or may not develop into a severe mental illness such as schizophrenia. However, there is evidence to guide early identification and intervention for young people at risk of developing psychosis.
Measurable predictors
There have been numerous studies showing neurocognitive changes in behaviour and functioning in infancy and childhood that are associated with increased risk of schizophrenia in adulthood. These include impaired and delayed gross motor skills, delayed language and impaired social development [35]. Population level studies such as the East Anglia (AESOP) study show psychotic-like experiences are relatively common in childhood (59% of a sample of 9–12 year old children reported experiencing one psychotic-like experience) [36] and the Dunedin study showed that strong evidence of these psychotic-like experiences in childhood were associated with a 16-fold increase of risk for schizophreniform disorders at age 26 years [37]. Social adversity such as unemployment, poor education, an urban upbringing, social isolation as experienced through migration or lack of friends have been shown to have both an individual and a cumulative effect upon risk for schizophrenia [38–40]. Cannabis use is another factor that increases the risk for schizophrenia and has been shown to have a dose-dependent effect [41]. The Dunedin longitudinal study showed that cannabis use prior to 15 years of age was associated with a 4.5-fold increase in risk for schizophreniform disorder at age 26 years [42]. Again there is evidence of a gene environment interaction with functional polymorphisms in COMT mediating risk for psychosis in cannabis users [43,44].
Walker has conducted extensive research on the role of the hypothalamic-pituitary-adrenal (HPA) axis in risk for schizophrenia [45]. The HPA axis is a primary neural system activated by stress exposure and there is a normative increase in HPA activity in adolescence. Walker argues for a number of associative links of the HPA axis with schizophrenia given such findings as (i) HPA activity is dysregulated in schizophrenia; (ii) cortisol can increase activity of dopamine pathways; and (iii) childhood trauma is associated with increased risk for schizophrenia [45]. Consistent with impaired HPA-axis impairment in young people at UHR, Thompson and colleagues [46] reported positive associations of plasma cortisol levels and experiencing depression and anxiety symptoms whereas global function levels, global psychopathology, psychotic symptoms or pituitary and hippocampal volumes were unrelated to plasma cortisol levels. A positive combined dexamethasone corticotrophin releasing hormone (DEX/CRH) test response was also associated with greater severity of depression and anxiety symptoms in UHR but did not predict the onset of acute psychosis [47]. Given the small sample sizes of the respective studies, further investigations are required into the potential association of HPA-axis impairment and the onset of psychosis.
The Emory Adolescent Prodrome Study (now part of North American Prodrome Longitudinal Study - NAPLS [48]) showed that UHR young people who later converted to psychosis had higher levels of cortisol at entry to the study and greater increases in cortisol at 12 month follow up compared to non-converters. Deficits in role functioning had a positive association (r = 0.35 to 0.55) with cortisol levels at these same time points. The results suggested a bidirectional relationship between stress and role functioning, namely stress-inducing effects and stress sensitivity [49]. Such findings provide reason and mode for intervention in the at-risk state for psychosis population.
Identification
The evidence clearly shows that risk for schizophrenia begins in utero and that these changes impact on factors at later stages of development, namely perinatal and adolescent periods. It is the changes occurring in adolescence that have close temporal links to the emergence of psychotic symptoms. While cognitive impairments similar to those evident in the illness itself can be detected in childhood [50] there is a significant decline in functioning for UHR individuals in the adolescent phase [51]. This functional decline is associated with subjective and objective cognitive changes as well as subclinical perceptual disturbances. The impairments are often first noticed in the classroom setting but even then may go undetected for a considerable period especially if accompanied by social withdrawal. Yet this is a critical period when the young person is completing basic education essential for future employment and negotiating the challenges of relationships with peers and increasing independence within the family. A disruption of the developmental trajectory at this phase will have a life-long impact on social inclusion, work experience and meaningful community participation.
The substantial body of UHR research has led to criteria for the identification of UHR individuals and two quite similar assessment schedules, the Structured Interview for Prodromal Symptoms (SIPS) [52] and the Comprehensive Assessment of At-Risk Mental States (CAARMS) [53]. The schedules identify three groups of UHR: the familial high risk, the attenuated positive symptoms, and the brief limited intermittent psychotic symptoms groups. A recent analysis of a large UHR data set (N = 377) showed the SIPS criteria could reliably distinguish between UHR attenuated positive symptoms or brief limited intermittent psychotic symptoms groups, UHR familial high risk individuals, help-seeking individuals and healthy controls in terms of later conversion to a psychotic disorder [48]. Interestingly, life-time substance abuse did not distinguish any of the groups. It is important to note that identification of UHR individuals can only be confirmed retrospectively following later conversion to a psychotic disorder. For this large sample drawn from multiple North American sites there was a 40% conversion for UHR individuals after 2.5 years and 36% conversion for individuals with schizotypal personality disorder (SPD). Close examination of the data suggested the SPD group were less symptomatic and converted at a slightly later rate than the UHR, although this may have been influenced by being younger at baseline. The evidence indicates that young people with SPD are at significant risk for later conversion to psychosis and that it may represent a more gradual pathway than those captured on the UHR criteria alone. However, it may also be an early phase or pre-prodrome. A critical finding of this large sample analysis was the ability to distinguish between UHR individuals and young people who were help-seeking/clinically referred to a UHR service. Some studies have shown that negative, anxiety and depressive symptoms may precede attenuated positive symptoms [54] and that subjective changes as defined by Huber's basic symptoms may also identify an early prodromal phase [55]. The reliability of such symptoms is yet to be established for UHR but is an important consideration for service delivery as is the finding of a similar rate of conversion for SPD compared to UHR youth.
Recent consideration and debate has been given to the inclusion of UHR as a ‘prodromal risk syndrome’ in DSM-5 as researchers ask whether clinical practice should now act upon research evidence to implement early detection and intervention for UHR individuals [56,57]. Issues under debate include accuracy of classification (e.g. false positives) and the potential for stigma and over/inappropriate treatment [58]. While the criteria for UHR are primarily mild psychotic-like symptoms it is imperative that classification in clinical practice does not overlook the distress and dysfunction in the clinical presentation. A recent editorial addressed the issue of UHR being included in DSM-5 and suggested it was timely for clinical practice to test the utility of UHR research evidence for detection and intervention [59]. The draft DSM-5 criteria for a ‘risk syndrome for first psychosis’ note common comorbid disorders such as major depression, social anxiety or substance abuse disorders [58]. Interestingly the draft argues for three potential clinical outcomes for the UHR state: progression to psychosis, symptom stabilization or remission. While this is true, researchers would define the remission category as potential false positives or misidentification. However, once identified as UHR, around 20%–50% of individuals will progress to full psychosis in 1 to 2 years with diagnoses being schizophrenia spectrum (50%), affective psychosis (10%–25%) and the remainder psychosis NOS [58].
Intervention
Early detection and intervention services for psychotic disorders initially focused on people experiencing a first episode of psychosis with the view that this ‘early intervention’ would reduce long-term disability known to be associated with psychosis and particularly the delay from onset of positive symptoms to treatment access. The significant advances of UHR research has enabled early detection and intervention prior to the onset of manifest positive symptoms. Numerous UHR intervention services have been established across Europe, Australasia and America. Rather than a focus on a reduction in the expectant disability known to be a long-term outcome of psychosis, the UHR interventions propose to delay or even prevent the onset of psychosis [60]. Data from only three randomized controlled trials were available at the time of a recent Cochrane review of UHR interventions: the EDIE trial in the UK (cognitive therapy), PACE in Australia (low dose risperidone combined with cognitive behaviour therapy) and Prevention through Risk Identification, Management and Education (PRIME) [61] in North America (olanzapine) [62]. The review reported that the EDIE trial showed no significant differences between cognitive therapy and monitoring on development of psychosis in 12 months [63]; the PRIME trial showed no effect for olanzapine over placebo in rates of conversion at 12 months [64]; and the PACE trial showed low dose risperidone combined with CBT was effective for symptom reduction at 12 months but was not maintained at 24 months [65]. The review concluded that it was too early to make recommendations for clinical practice due to insufficient data (only three trials and all were underpowered) but that this could change in the near future with more treatment trials nearing completion. At 3 year follow up of the EDIE trial cognitive therapy was associated with a reduced likelihood (OR 0.13) of being prescribed antipsychotics compared to the monitoring only group [32]. A randomized double blind placebo controlled trial of a 12 week intervention period with long chain omega-3 fatty acids has since been published and showed reduced transition rates for UHR young people in the treatment group compared to placebo [66]. A narrow focus on symptom reduction in these research efforts leaves unexplored the likely contribution of a variety of factors including the environment, stress, and concomitant drug use to progression of identified UHR young people to psychosis.
There have been a number of UHR studies reported at recent international conferences. The ED:IT programme in the UK targets engagement and intervention for UHR young people and improved access to care for ‘at-risk’ populations and communities (e.g. minority ethnic communities, neighbourhoods with high incidence of psychosis and primary care). Such clinical research has resulted in the UK Department of Health funding a five year public health programme to reduce the rates of UHR transitions to psychosis and the duration of untreated psychosis [67]. The UK National Institute for Health Research has funded the establishment of a Mental Health Research Network to provide infrastructure to support large scale clinical research conducted within clinical services [68]. The UK National Institute for Health and Clinical Excellence (NICE) guidelines for schizophrenia identify cognitive behaviour therapy as a core intervention that should be offered to all people with schizophrenia including those in the acute phase [69,70]. Australian research has clearly shown the cost benefits of early intervention for psychosis [71].
UHR early intervention service
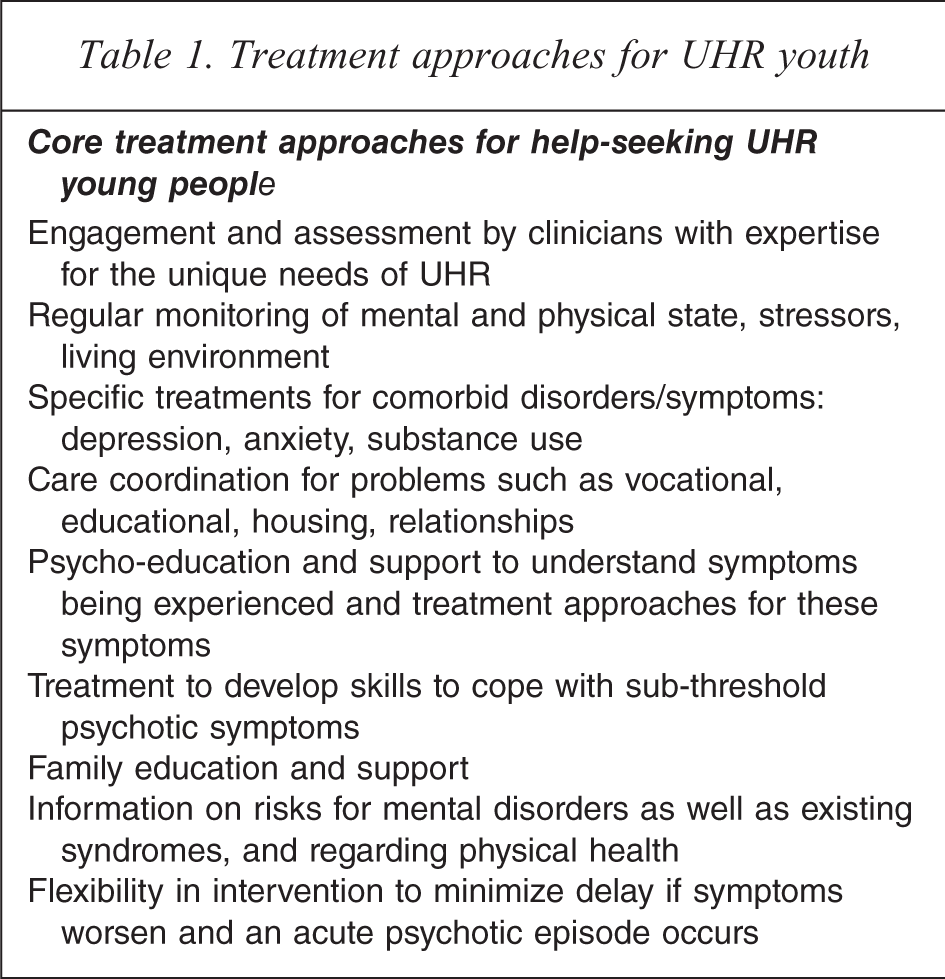
Across the world, help-seeking UHR young people are more likely to receive targeted and evidence-informed treatment at a clinical research centre rather than a specialist health service. These research or UHR centres are likely to have strong links with health services to facilitate referrals between the services and the UHR service, and usually have an active outreach approach to recruitment by the provision of clinical education to youth and health services [72]. Most UHR centres have a triage system to review possible referrals and offer extensive sequential assessments for intake. The PRIME clinic in New Haven highlighted the importance and benefit of informing the UHR young people and their families of the meaning of risk for psychosis [73]. While some argue that identifying UHR status may be stigmatizing, the PRIME clinic experience has shown that identifying the status and engaging in treatment has resulted in regular monitoring and management of distress and psychotic symptoms [73]. In fact none of those in the PRIME clinical trial who converted to psychosis required hospitalization; all but one maintained school or work; 93% were compliant with medication; and relationships with family and friends were maintained [73]. There is a wide range of interventions provided at UHR centres including engagement strategies, supportive therapy, case management, cognitive behaviour therapy, psycho-education, family-based treatment (e.g. multi-family groups) and pharmacotherapy. While there is a need for more research to provide clear evidence of the efficacy of treatment approaches for UHR, Table 1 delineates the core treatment approaches common to current UHR intervention services [74]. It is paramount that further UHR research focuses on multicentre RCTs to examine the effectiveness of early intervention for UHR young people. Despite the paucity of RCT studies for UHR, the trials to date provide clear evidence of (i) reduction in sub-clinical psychotic symptoms, (ii) prevention of decline in social functioning, and (iii) prevention or delay in transition to psychosis [75].
Treatment approaches for UHR youth
Early intervention service for UHR and help seeking youth
Limitation in funding of public mental health services in Australia has meant that targeted services for early intervention for UHR have been scarce. The few services that have been established are based in high population urban settings where client throughput will be greatest and skilled clinicians are more likely to be seeking employment. The location of UHR services internationally would suggest the same. The concentration of UHR services in high density population areas results in limited availability of such services in rural areas, replicating the pattern of reduced access to general mental health services for rural residents. Numerous European studies have demonstrated that urbanicity is associated with a higher prevalence of some psychiatric disorders such as psychoses [76]. However, Australian and international studies show poorer physical health outcomes, poor access to services and socio-economic disadvantage in rural areas [77]. Suicide rates continue to rise for Australian males in rural areas despite a reduction in urban areas [78]. Australian rural young people (18–24 years) have fewer social supports, are more likely to have hazardous levels of alcohol use and have higher rates of death by injury than urban young people [79].
Rural health service providers are well aware of inequity in funding coupled with difficulties in recruitment and retention of clinicians compared to urban services. Given the lack of resourcing to pilot rural models of early intervention there remains the expectation at the policy level that an urban model of early intervention can simply be ‘rolled out’ to rural areas. Not only does this view overlook the vast disparity between urban and rural settings but it fails to encapsulate the heterogeneity of rural areas especially in terms of population and geographic characteristics (e.g. age distribution, distance and ease for transport). A one-stop shop for youth services is not necessarily the ideal in a rural area where anonymity is unlikely to be maintained and there is a lack of youth services generally. While the value of a community awareness campaign to reduce stigma and encourage help-seeking is just as critical for rural areas, the focus and delivery is likely to require modification. A recent study of mental health literacy found rural Australian adults were more likely than urban residents to perceive alcohol and painkillers as helpful for the treatment of depression and counselling as unhelpful [80]. This is consistent with evidence of high rates of harmful alcohol use for rural Australian youth [79].
Given the known poorer health outcomes, relative paucity of youth-orientated mental health services and increased risk behaviour of young people in rural areas it is critical that early intervention programmes be established and evaluated. The severity of psychoses such as schizophrenia and evidence of its onset in utero plus acceleration in adolescence positions UHR intervention as a core model for early intervention for young people. The provision of such a service in relatively resource poor rural areas can be achieved by embedding UHR clinical research practice and findings within clinical services. Table 2 provides an illustration of the key factors essential for service delivery. Many of these ‘rural’ factors would be applicable to resource poor urban settings.
Mapping a rural UHR service
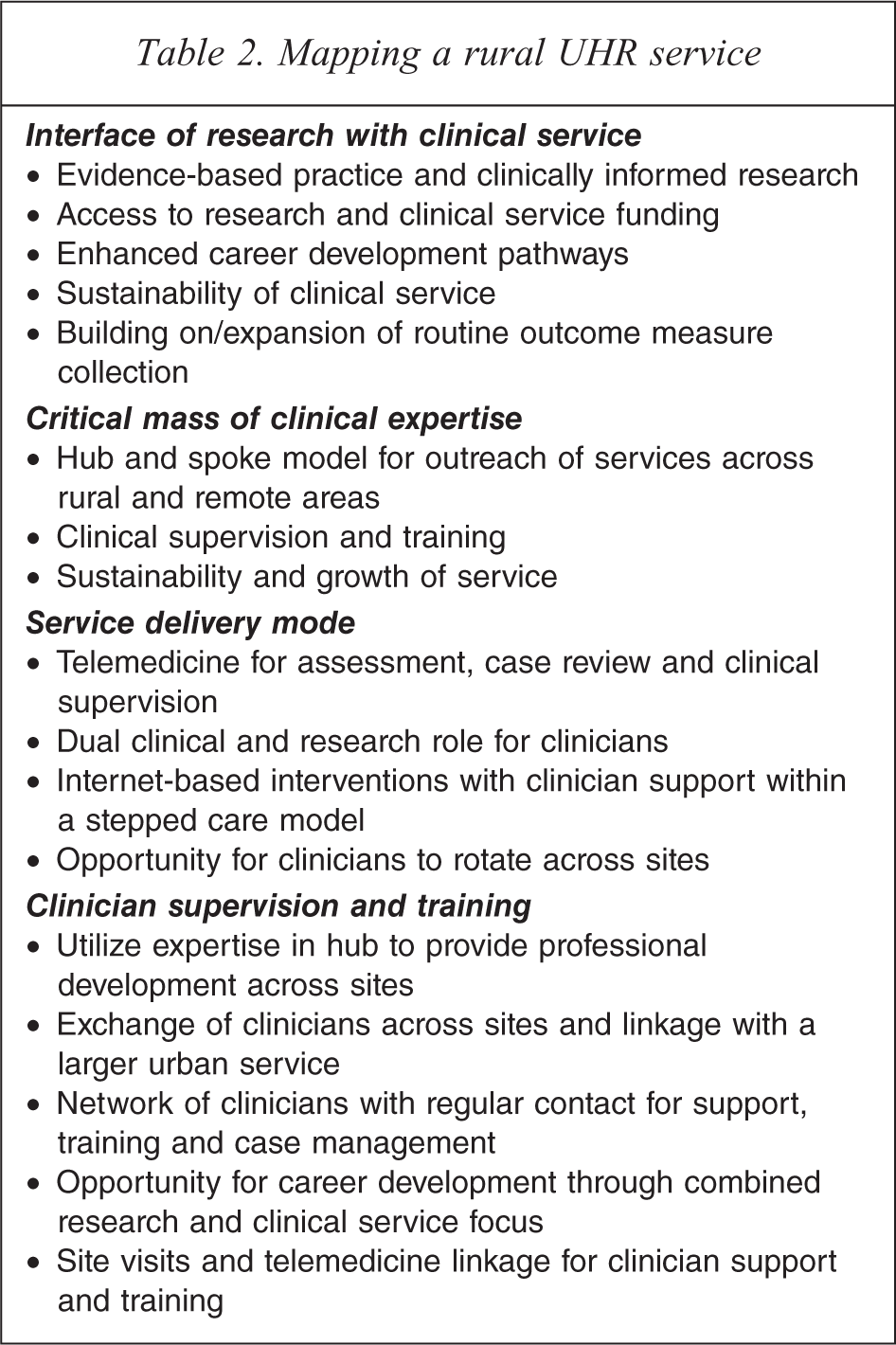
There are clear advantages to linking research and clinical services, such as increased capacity through shared funds and staff as well as enhanced retention and recruitment of staff, a critical issue for service provision in rural areas. The model is not restricted to the delivery of intervention for UHR young people but is applicable for targeted programmes for a number of clinical groups. Hence the model could be for a programme of early intervention for young people grounded in the evidence-based practice for UHR young people. This would be efficient use of the limited resources for rural services while targeting a high need group such as schizophrenia.
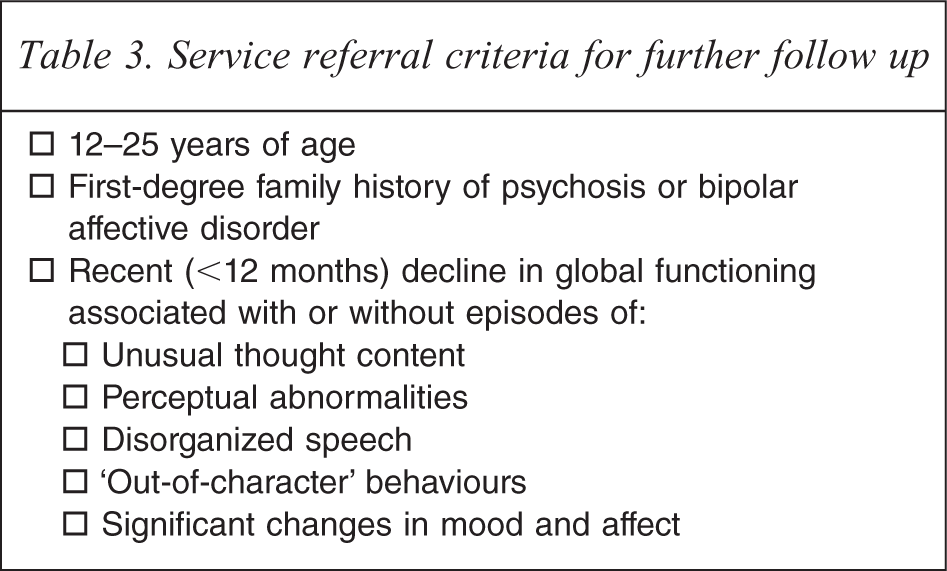
Such a programme should be an integral part of any community-based mental health service and aim for the early detection of ‘at-risk mental state’ and emerging first-episode psychosis (non-affective and affective) in young people aged from 12 to 25 years. The nature of such a programme requires multi-disciplinary cooperation of psychiatrists, psychologists, nurses, and social workers. All referrals meeting the target age range should be screened against key criteria indicative of a potential ‘at-risk mental state’ (Table 3). Referrals meeting these criteria should be targeted for comprehensive assessment by specifically trained staff that would contact the referrer or client (as appropriate) for further information (Table 4).
Service referral criteria for further follow up
At-risk mental state referral checklist
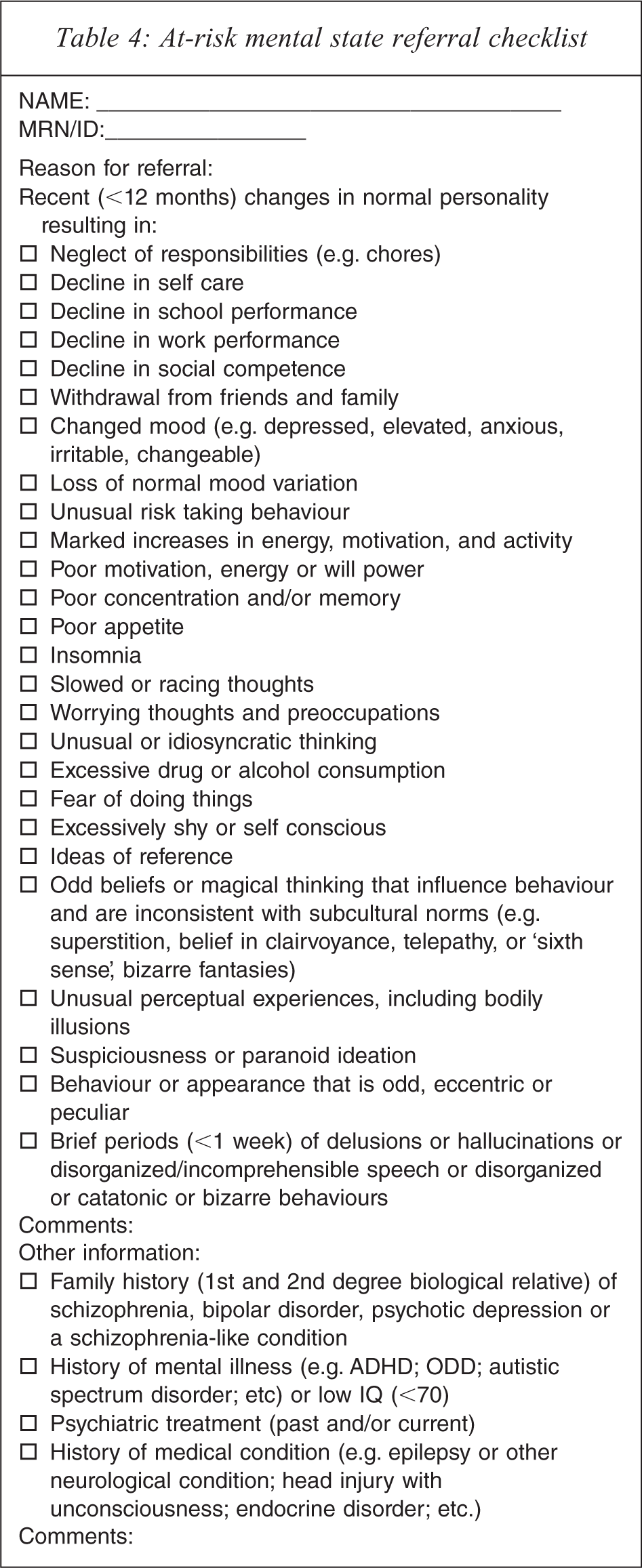
This initial triage can be conducted by telephone while the subsequent assessment of ‘at-risk mental state’ should be conducted face to face or via telemedicine (i.e. for referrals from more isolated areas) as a structured clinical interview (e.g. CAARMS). For those meeting ‘at-risk mental state’ criteria, further clinical assessments and examinations including review by a psychiatrist would follow for diagnostic clarification and treatment planning. It is important to communicate that ‘at-risk mental state’ does not constitute a diagnosis but rather an increased vulnerability of developing a mental illness. Neuropsychological assessments may be used to examine the level of cognitive and functional impairment. The identification of ongoing risk factors such as substance abuse or psychological trauma is guiding further intervention strategies which should include psycho-education, counselling, psychological treatment (e.g. CBT-based psychotherapy, cognitive remediation, etc.), and pharmacotherapy as indicated. Importantly, regular follow ups (e.g. every 3 months) over at least 2 years should be offered to detect a potential deterioration of mental state and the transition to psychosis. Similar models of early intervention for psychosis have been successful in Norway [4] and Germany [81].
Recognizing that prodromal phase of illness and first-episode psychosis represent a continuum with varying degrees of functional impairment rather than clearly defined diagnostic categories, such a programme should complement existing early psychosis services. The challenges are existing preconceptions based on traditional triage strategies which often hold to a high threshold for further engagement or follow up. Also the division into child and adolescent and general mental health services is particularly unhelpful when targeting youth mental health [82]. Moreover, increasing the awareness of early signs and symptoms of emerging psychosis amongst many health professionals needs to be addressed by training and education [83].
It is also paramount that the needs of rural young people are not forgotten in the strategic planning and funding of early intervention programmes, and in particular, intervention for UHR for psychoses. It is unfortunate that to date this has been the case despite evidence of high need for rural young people such as high rates of harmful alcohol use, death by injury and social isolation [78].
Finally, the partnership of mental health services with academic research institutions has to be fostered to provide the appropriate infrastructure for large-scale clinical research. In Australia, such an integration has only been achieved in some locations, for instance, in Melbourne (Orygen), in Newcastle (Psychological Assistance Service, PAS) and more recently in Sydney at the Brain and Mind Institute. In partnership with the Universities of Newcastle and New South Wales and Macquarie University, the Minds in Transition programmme (MinT) of the Hunter New England, South East Sydney Illawarra and Greater Western Area Health Services was established in 2009 to provide an urban, rural and remote research and service infrastructure for New South Wales. While these are promising initiatives, they fall short of international benchmarks such as the UK Mental Health Research Network, which could provide the largely lacking infrastructure for translational mental health research in Australia. In this context, prodromal schizophrenia is but one critical example of how mental health services have failed to meet community needs by not translating research evidence into routine best practice. It can be done.
Footnotes
Acknowledgements
We wish to acknowledge the MinT study Chief Investigators: Ulrich A. Schall, Patricia T. Michie, Helen J. Stain, Philip B. Ward, Robyn Langdon, Juanita Todd, Paul Rasser, Vaughan Carr, Thomas Weickert; and Associate Investigators: Rebbekah Atkinson, Sean Halpin, Renate Thienel, Jackie Curtis, Kristy Payne, Scott Clark, Maryanne O'Donnell and Carmel Loughland. We also wish to acknowledge the support of the Area Health Services wherein the study is being conducted: Hunter New England, Greater Western and South East Sydney Illawarra Area Health Services.