
Abstract
Objectives:
The study aim was to estimate the current level of ambulatory mental health service delivery to young people aged 0–24 years in Australia and associated government expenditure. Recognising the importance of the early years for the development of mental illness and socioeconomic outcomes, we were particularly interested in service access by infants and young children.
Methods:
We extracted information from government administrative datasets on the number of people who received mental health services, number of services and expenditure through the health sector for 2014–2015. Results are primarily reported by age groups 0–4, 5–11, 12–17 and 18–24 years.
Results:
Less than 1% of 0- to 4-year-olds received a mental health service in any one service setting, whereas nearly 11% of 18- to 24-year-olds received a mental health service through the Medicare Benefits Schedule Better Access programme alone. Many more services were delivered to 12- to 24-year-olds (>4 million) than to 0- to 11-year-olds (552,000). Medicare Benefits Schedule Better Access delivers services to more children and youth than do state/territory community mental health services, although the latter provide more services per client. In 2013–2014, Australian Government expenditure on ambulatory mental health services for 0- to 24-year-olds was AUD428 million, similar to the AUD491 million spent by state/territory governments.
Conclusion:
The study provides a benchmark for data-driven service planning to ensure that the mental health needs of infants, children and young people are met. Our results indicate that the youngest age group are underserviced relative to need, even noting infants and children may receive services for behavioural/mental health issues from providers not captured in our study (such as paediatricians). The developmental origins of mental illness underlies the urgency of adequate provision by governments of perinatal, infant and child mental health services to avoid loss of life potential and reduce the pressures on the justice, child protection and welfare systems.
Introduction
Over the past 4 years, our research group has been investigating how to better design South Australia’s mental health system so as to intervene earlier in the development of mental illness. To do this, we have employed a need-based workforce and service planning framework (Segal and Leach, 2011) that emphasises a thorough understanding of the target population (descriptively and numerically) for planning an appropriate service response and assessing the adequacy of current service delivery.
Two key areas of knowledge are critical in understanding the need for mental health services. First, the evidence that trauma and adversity in utero, in infancy and in childhood can have lasting impacts on social, emotional and cognitive development (Hertzman and Boyce, 2010; National Scientific Council on the Developing Child, 2007; Shonkoff, 2011). Research across a range of disciplines including developmental psychology and neurobiology highlight the period from in utero to approximately 5 years of age as a time during which the developing brain is particularly sensitive to environmental influences (Hertzman and Boyce, 2010; Rash et al., 2016; Shonkoff, 2011). Nurturing interactions with caregivers alongside enriching environments are essential building blocks of healthy social, emotional and cognitive child development (Felitti et al., 1998).
The Adverse Childhood Experiences Study was instrumental in demonstrating the damaging effects of childhood trauma and maltreatment on adult social, emotional and physical health (Chapman et al., 2004; Clarkson Freeman, 2014; Dube et al., 2001, 2003; Williamson et al., 2002). Cohort studies examining the relationship between mental illness and (early) childhood adversity consistently confirm the role of early adversity in emergence of mental illness (see, e.g., the narrative review by Fryers and Brugha, 2013). These studies highlight the critical role that early family dynamics play in child development and mental health. A core policy lesson from this research is that timely access, from the antenatal stage to services that can address emerging mental health issues, is needed to address current distress, as well as reduce the risk of developing mental illness in adolescence and adulthood.
Second, and related to the above, mental illness or psychological distress in young people does not typically emerge in isolation. For example, we have found in both a general and Indigenous Australian cohort, high levels of psychological distress in young people co-occurs with multiple biopsychosocial adversities such as neurological vulnerability, poor school performance, financial and other major life stressors, child maltreatment and distressed parent child relationships, parental mental illness and substance abuse. Furthermore, this relationship increases with age, so by age 8–10 years, over 75% of children with high or very high levels of psychological distress will have four or more additional current adversities. Clinically, it means young people (including infants and young children) presenting with mental health problems will commonly bring with them current and historical adversities, often intergenerational in nature. It is important therefore that the mental health services that young people access have the capacity to respond to such complexity. As a step towards assessing the capacity of mental health services to meet the needs of young people, this study aims to quantify the level of mental health service delivery to young people in Australia.
Young people with mental health problems may receive services from a number of sources. These can include private mental health services (medical, allied health, complementary therapies), prescription and over-the-counter medicines, other Australian Government-funded programmes (e.g. headspace, perinatal depression initiative), maternal and infant health services, community-based child and adolescent mental health services (CAMHS), non-government organisations (NGOs) (e.g. Centacare, Anglicare), wellbeing initiatives offered through school-based counsellors, and online programmes (e.g. Reachout).
Services differ widely in terms of source and security of their funding, target population (age, demographic background and clinical severity), treatment approach (psychotherapeutic, case management, family support and pharmacological), flexibility of delivery models and workforce (discipline and skill-base). These differences influence the capacity of the service to manage complexity. This is important. The provision of specialist mental health services to highly vulnerable and complex young people and families requires high-level specialised competencies. For example, in young children (0–4 years), relational competencies such as understanding how to strengthen and repair dysfunctional parent–infant attachment relationships, or in older adolescents, competencies in multi-systemic work to stabilise chaotic functioning across multiple settings and a capacity to hold risk may be needed. Within the service system, there are few places with the high-level competencies and the structures in place to deliver what is needed – such as intensive long-term therapy, extensive outreach, multidisciplinary care, access to social supports and a responsive delivery model.
The Australian Government funds primary mental health services (e.g. general practitioner [GP]) and secondary or specialist services/mental health services (private psychiatry and eligible allied health through the Medical Benefits Scheme [MBS] Better Access programme and the Access to Allied Psychological Services [ATAPS] programme). The Australian Government also subsidises private paediatricians, who increasingly see behavioural and developmental issues in infants and children as part of their caseload (Hiscock et al., 2017).
Under the MBS Better Access initiative introduced in 2006, consumers with mental health concerns on attending their GP can receive a mental health treatment plan, under which the GP may deliver limited therapy sessions, refer them to a psychiatrist or paediatrician or for ‘focused psychological strategies’ provided by a psychologist, social worker or occupational therapist, for which the patient can be reimbursed for up to 10 individual and 10 group sessions in a year.
State and territory governments provide specialised, tertiary-level community mental health services through CAMHS and other community settings such as Emergency Department (ED) and hospital outpatients.
In this study, we set out to determine the level of government-funded ambulatory mental health services provided through the health sector to infants, children, adolescents and youth. We estimated the number of young people receiving services, number of services delivered and their cost to government. We report on service delivery within the age range of 0–24 years, although we were particularly interested in the level of service delivery to infants and young children aged 0–4 years and 5–11 years, given the growing understanding of the critical importance of early childhood.
Methods
Scope
In scope for this research were government-funded mental health services delivered through the health sector and involving psychotherapeutic treatment:
Australian Government-funded mental health services:
Provided by medical and allied health workers through the MBS Better Access programme Provided by allied health workers through the ATAPS programme Mental health-related medications administered through the Pharmaceutical Benefits Scheme (PBS) Headspace services
State and territory government-funded ambulatory mental health services:
Ambulatory mental health services provided in community including hospital outpatient settings ED Presentations
Figure 1 shows a diagrammatic representation of mental health services funded by the Australian and state and territory governments and delivered through their mental health service systems. It excludes for example services funded through Transport Accident or Work-cover insurance organisations, services paid in full by the consumers or paediatric consults (which are not identified as a mental health service).
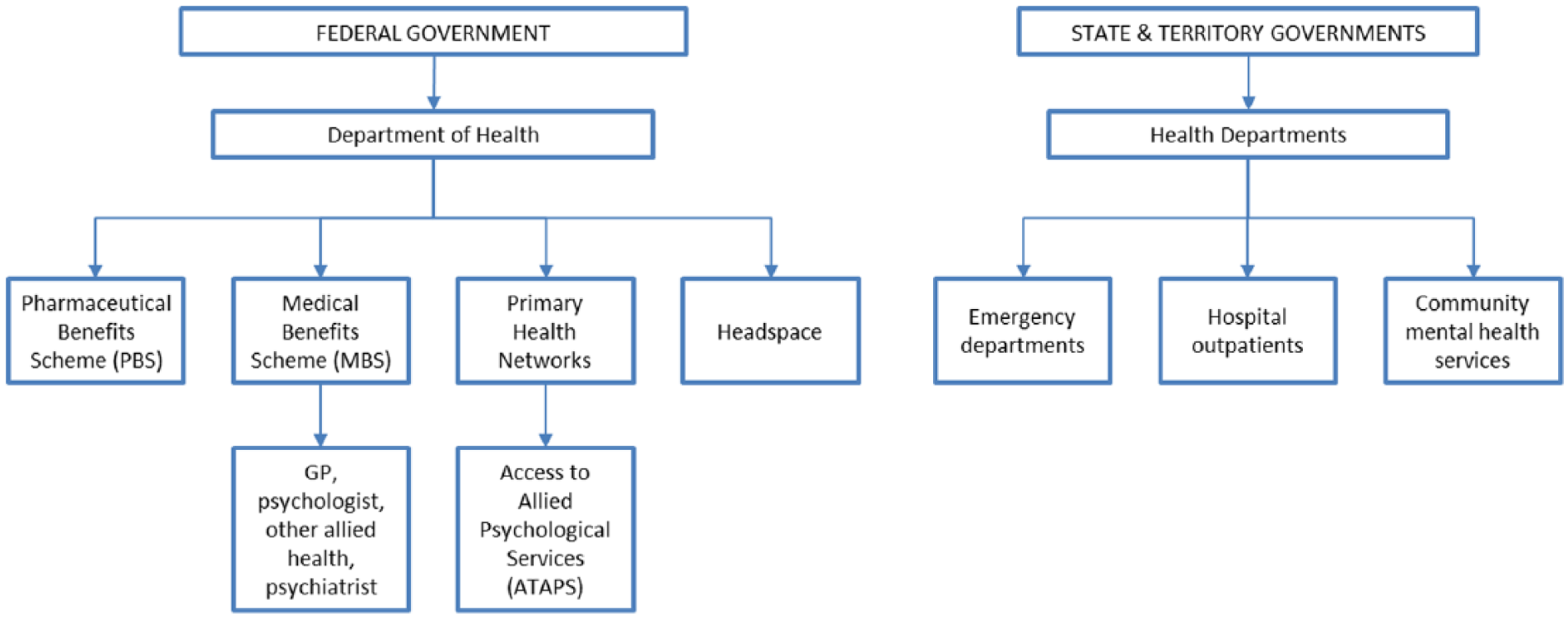
Map of government-funded ambulatory mental health services in Australia.
Data sources
We located government administrative data that provided information about the level of mental health service delivery to young people and levels of expenditure in Australia drawing on primary data sources. In all but one case, the data were publicly available and published online, the exception being community mental health for which we made a specific data request to the Australian Institute of Health and Welfare (AIHW) to obtain data for our study age groups. The data sources used in the study are summarised in Table 1.
Description of data sources used to estimate mental health service delivery and expenditure to infants, children and youth in Australia.
Data analysis
Using the above data sources, we report the number of 0- to 24-year-olds who received a mental health service, the number of service occasions delivered in a 12-month period, and annual expenditure by type of services. Where possible, data are reported in the age categories of 0–4 years, 5–11 years, 12–17 years and 18–24 years. Number of services delivered per person was calculated for each age group as well as the proportion of people in each age group who received a mental health service using population data from the Australian Bureau of Statistics (2015). The results are reported for the most recent financial year available (2014–2015 or 2013–2014).
To compare the level of service delivery to younger (0–11 years) and older (12–24 years) age groups, data were summarised in a stacked bar chart. Data on MBS Better Access, headspace, and state and territory services matched these age categories; however, data on ATAPS services and ED presentations did not. Data are either reported for combined age categories or estimated on a pro-rata basis as illustrated below. Data on ED presentations were reported in the age groups 0–14 and 15–24 years; to estimate the number of presentations by 0- to 11-year-olds, the number of presentations was assumed to be evenly spread within the 0–14 age range, such that 80% of services in the 0–14 age group would relate to persons aged 0– <12. The remainder is then allocated into the 12–24 age group. A similar process was applied to the ATAPS data.
To estimate expenditure on PBS services, the percent of all mental health scripts dispensed to young people aged 0–11 years and 12–24 years (estimated from reported data for age groups 0–14 and 15–25) was applied to total expenditure on mental health scripts from the Report on Government Services (Productivity Commission, 2016).
State and territory government expenditure on ambulatory mental health services by age group is not published. We calculated mean expenditure per service in 2014–2015 as total expenditure on community mental health care of AUD1947.8 million (AIHW, 2016b, Table Exp.1), divided by total number of occasions of service of 8.52 million (AIHW, 2016c, Table CMHC.1) = AUD228.50 and applied this to state-funded community mental health services in our study age groups.
The amount spent on ATAPS services for 0- to 24-year-olds was estimated by applying the percentage of ATAPS consumers who were 0- to 24-year-olds to total ATAPS expenditure.
Results
Number of young people receiving mental health services
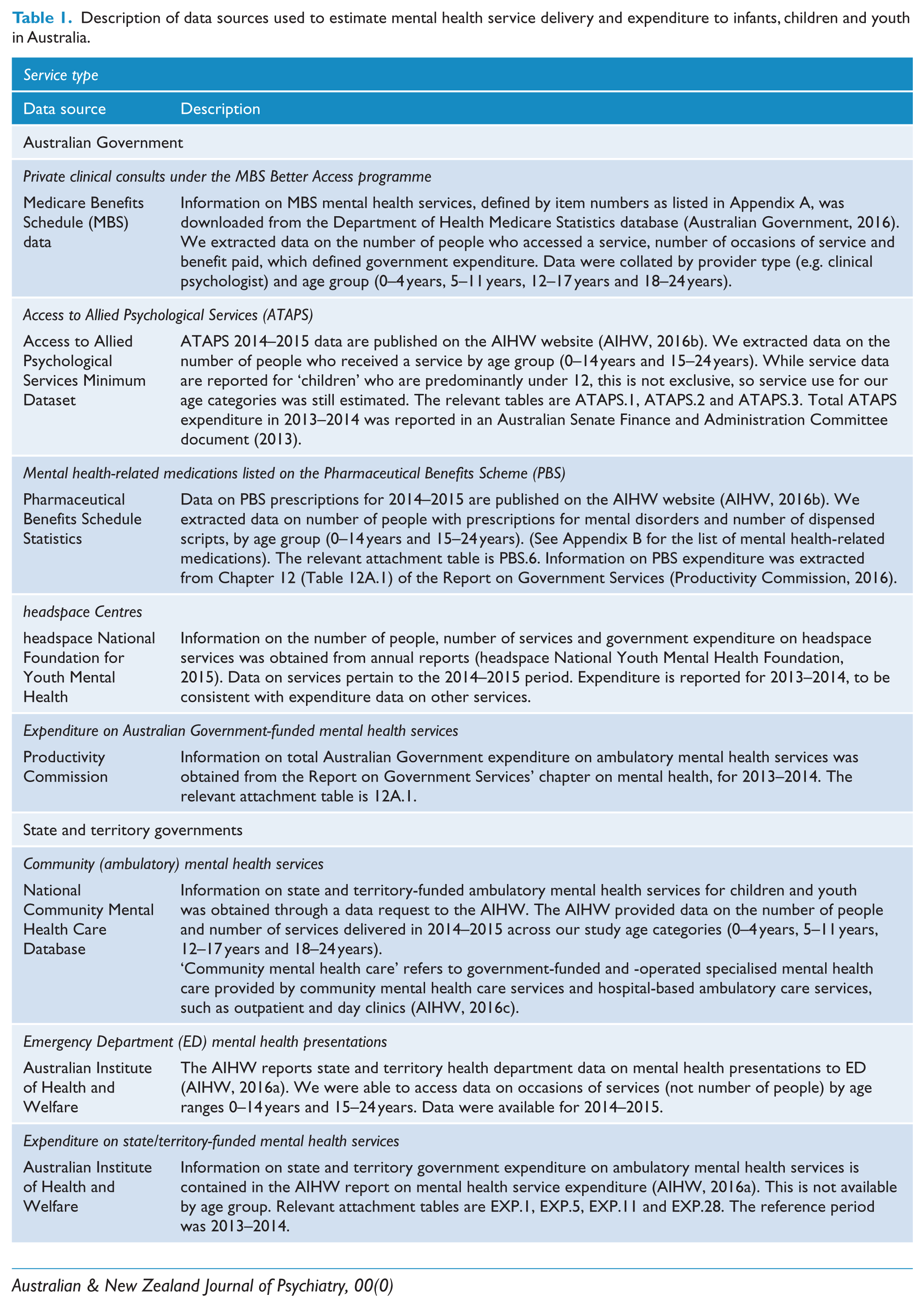
The numbers of young people who received an ambulatory mental health service in 2014–2015 across the different jurisdictions and service types are shown in Table 2. The data show that within any one service type, <1% of children aged 0–4 years received a mental health service. By comparison, over 10% of young people in the 18- to 24-year age group received an MBS Better Access service in 2014–2015.
Number of children, adolescents and youth who received ambulatory mental health services in 2014–2015 by service type and age group.
MBS: Medicare Benefits Schedule; GP: general practitioner; ATAPS: Access to Allied Psychological Services.
Any provider refers to GP, clinical psychologist, psychologist, social worker, occupational therapist, mental health worker and psychiatrist. Individual provider data do not sum to any provider totals because a person may see more than one provider in a financial year. Medicare item numbers are shown in Appendix A.
Service contacts cover all clinically significant services by a specialised community mental health provider for patient/clients and are not restricted to face-to-face communication but can include telephone, video link or other forms of direct communication and can be with the patient or a third party, such as a carer or family member, other mental health worker or other service provider.
Other allied health providers were psychologists (non-clinical), social workers, occupational therapists and mental health workers.
Data from Australian Capital Territory (ACT) were not available and were not included in totals.
Analysis of Medicare item number data showed that most GP mental health services provided to young people were for care planning. Care planning made up the majority of services delivered by GPs to 0- to 14-year-olds, although among 15- to 24-year-olds, the majority of GP services involved the provision of treatment. Of GP services involving treatment, the proportion that delivered focused psychological strategies (i.e. psychotherapy, as opposed to other forms of treatment, e.g., medication) varied by age group: 24% (461 of 1957 services) of GP services to 0- to 4-year-olds, 11% of services to 5- to 14-year-olds (3283 of 31,226 services) and 3% of services to 15- to 24-year-olds (5742 of 205,894 services), reflecting an increase in use of pharmacotherapies in the older age groups.
We estimate that 11,742 children aged 0–11 years received an ATAPS, equivalent to 0.3% of the population and 16,112 persons aged 12–24 years, a rate of 0.4% of that age group. Mean services per person was just under 5.
Many more people received a mental health service through MBS Better Access than those receiving a state/territory community mental health service in the three older age groups but not the youngest (0–4 years). State/territory-funded community mental health services provided a similar number of services, reflecting more services per client. Among 18- to 24-year-olds, the average number of service occasions delivered in a state/territory mental health service was 12.7 compared with 4.4 through MBS Better Access. Although, as described in the note to Table 2, State/Territory community mental health, occasions of service are not always delivered directly to the young person.
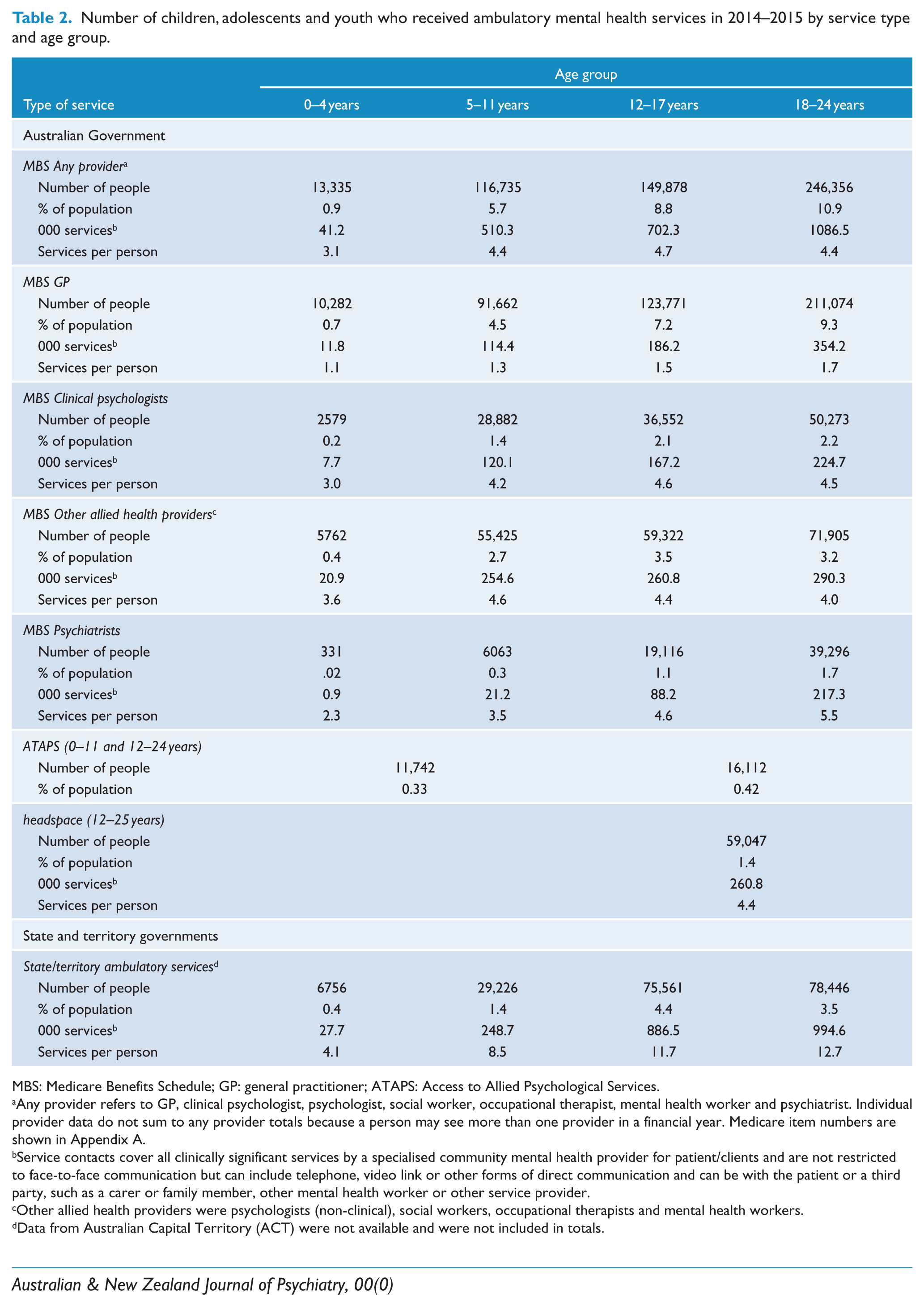
Data on mental health presentations in EDs showed that in 2014–2015, there were 9494 occasions of service among 0- to 14-year-olds and that 15- to 24-year-olds received 55,428 occasions of service in the same period (AIHW, 2016a), suggesting approximately 7595 services were delivered to 0- to 11-year-olds and 57,323 to 12- to 24-year-olds (as shown in Figure 2).
Total number of mental health services delivered in 2014–2015 by age group and service type.
Table 3 shows the number of young people who were prescribed psychiatric medication in 2014–2015 as well as the total number of scripts written. A list of the medications included in the analysis is provided in Appendix B. The data indicate that one in 10 young people aged 15–24 years was dispensed a psychiatric medication in 2014–2015. The vast majority of mental health prescriptions are written by GPs, 87% of all mental health scripts (all ages) (AIHW, 2016b).
Number of youth prescribed a psychiatric medication in 2014–2015.

Source: Australian Institute of Health and Welfare (AIHW, 2016b).
Figure 2 shows the number of services provided to young people in two age groups by type of mental health service. The figure illustrates the markedly fewer mental health services delivered to 0- to 11-year-olds than 12- to 24-year-olds. Three times as many MBS services and close to seven times as many state/territory mental health services were delivered to the older age group compared to the younger age group, compared with a 20% difference in number of persons in each age group (3.5 million 0- to 11-year-olds and 4.3 million 12- to 25-year-olds in Australia in 2014).
Government expenditure on mental health services to young people
Government expenditure on mental health services for young people has been estimated from a number of sources. Total expenditure on ambulatory mental health services (all ages) in Australia in 2013–2014 was just under AUD3.8 billion (Table 4). Mental health services provided through MBS Better Access accounted for 26% of all Government funding, prescriptions for psychiatric medication accounted for 19% and state and territory government spending on ambulatory mental health services at almost AUD1.9 billion accounted for 50%.
Australian and state and territory government expenditure in 2013–2014 on ambulatory mental health services – 0- to 24-year-olds and all ages.
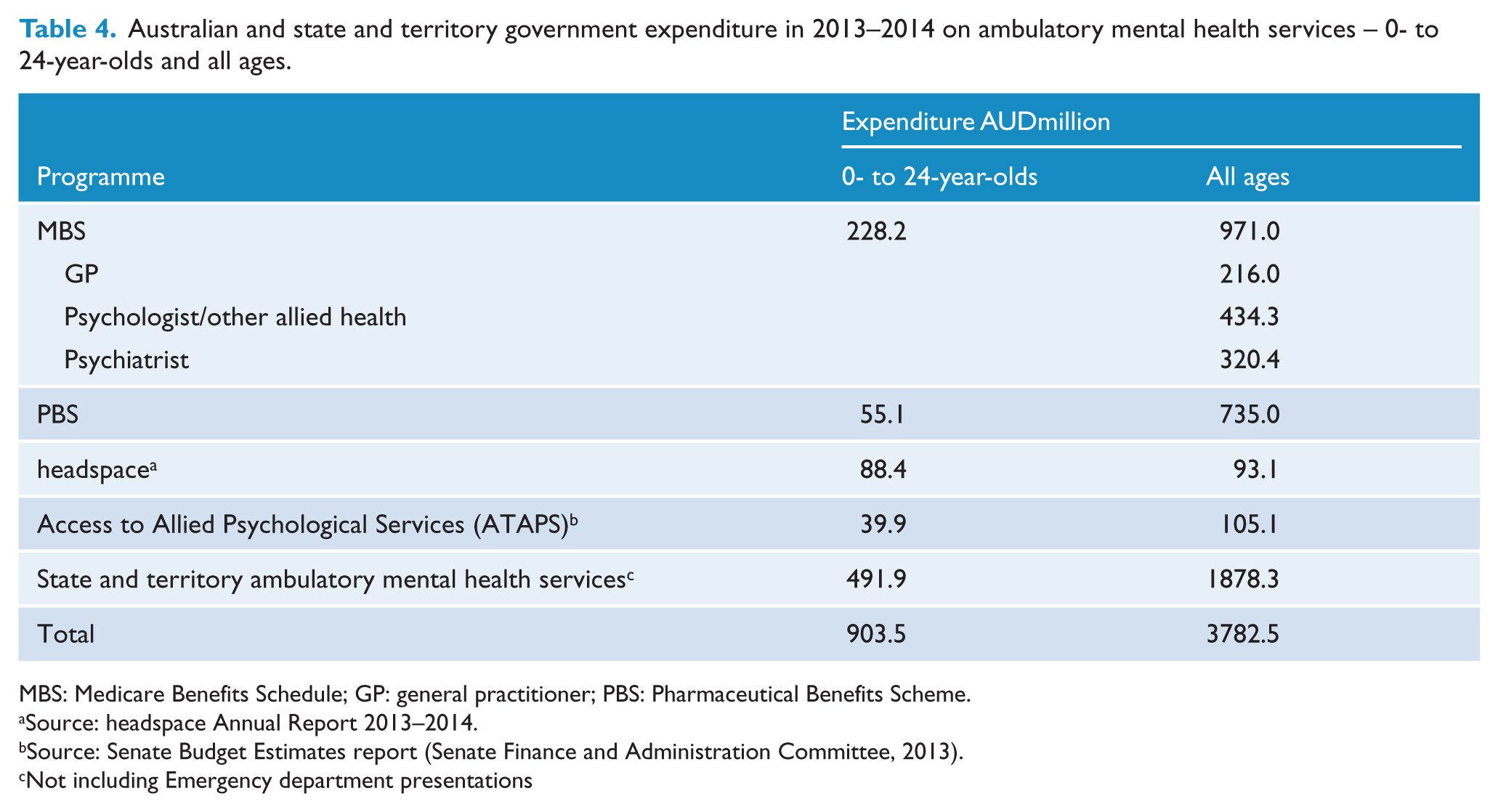
MBS: Medicare Benefits Schedule; GP: general practitioner; PBS: Pharmaceutical Benefits Scheme.
Source: headspace Annual Report 2013–2014.
Source: Senate Budget Estimates report (Senate Finance and Administration Committee, 2013).
Not including Emergency department presentations
We estimated government expenditure on mental health services for young people aged 0–24 years across all jurisdictions at just over AUD900 million in 2013–2014 (Table 2 and Figure 3). This is 24% of the amount spent across all ages on these services. Australian Government expenditure through MBS, PBS, ATAPS and headspace comprised 45% of the total government expenditure on ambulatory mental health services for 0- to 24-year-olds. Approximately AUD14.7million was spent on mental health prescriptions for 0- to 14-year-olds and AUD40.4million for 15- to 24-year-olds.
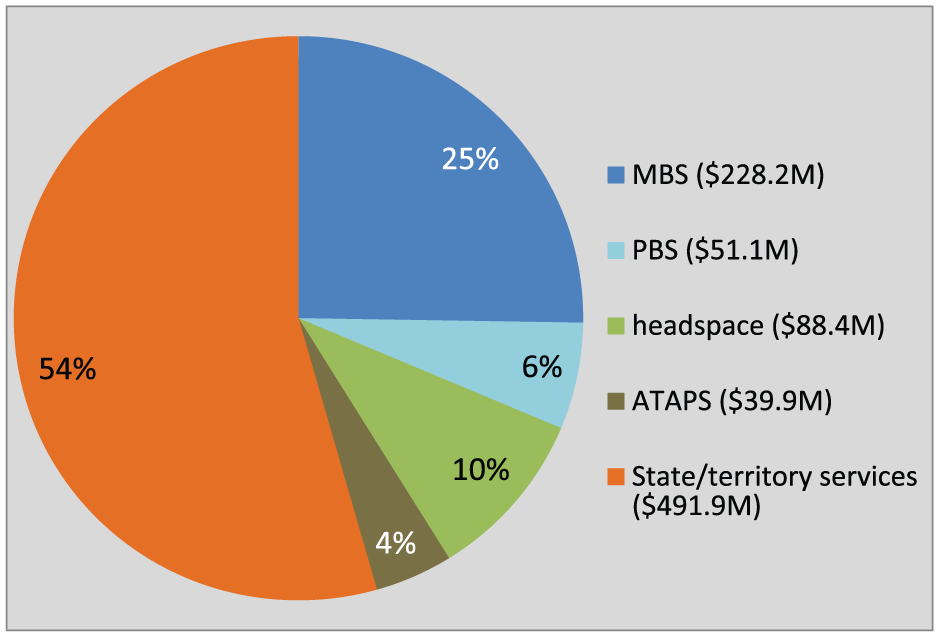
Expenditure on mental health services delivered in 2013–2014 to youth in Australia aged 0–24 years.
The Australian government expenditure on MBS mental health services by age group is shown in Figure 4, showing almost half of the expenditure in the 0–24 age group was spent on young people aged 18–24 years. Only 2% of MBS Better Access expenditure was on services delivered to 0- to 4-year-olds.
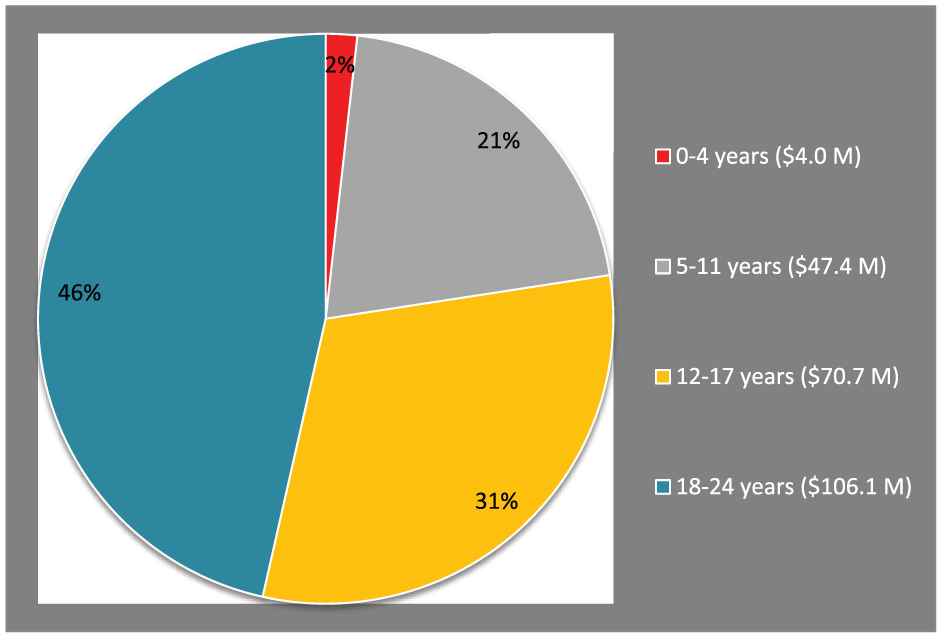
Australian Government expenditure on benefits paid for MBS Better Access services in 2013–2014, by age group.
Discussion
This study drew primarily on government administrative data to quantify the level of mental health service provision and expenditure on young people aged 0–24 years in Australia, limited to those delivered through the health sector. Our analyses showed that many more young people are receiving mental health services through the federally funded MBS Better Access programme than state/territory-funded community mental health services, but the latter offered more occasions of service per client. Children aged 0–4 years were especially underrepresented in the mental health system, with less than 1% receiving services within any of the different service types. This compares to 18- to 24-year-olds, where approximately 10% received an MBS service and 3.5% accessed a state/territory ambulatory service. This does not include services through ED. Data on mental health-related medication prescribing showed that 10% of 15- to 24-year-olds in Australia were dispensed a mental health-related medication in 2014–2015. Similarly, MBS Better Access spending by age showed that only 2% (AUD4 million) went to services delivered to 0- to 4-year-olds.
Our analysis of expenditure suggests that approximately AUD900 million was spent by the Australian and state/territory governments on mental health services to 0- to 24-year-olds in 2013–2014. The results indicate that slightly more is spent through state/territory ambulatory mental health services. It is important to remember that the expenditure data include only costs to government. It does not include patient payments or spending by other insurers (such as transport accident or work-cover agencies).
Limitations
As noted in the ‘Introduction’, the health sector is not the only area in which mental health services are provided to young people in Australia. Mental health services are also provided through the NGO sector (e.g. in intensive family support programmes), youth justice, child protection and education sectors. Although, programmes delivered through other sectors will tend focus on social and other supports and typically refer children with mental health problems to the GP (and then captured in MBS Better Access) or to ATAPS or to State Child and Adolescent Mental Health Services for on-going therapeutic care.
Even within the health sector, we were not able to obtain all relevant data on community health services for children with mental health, behavioural or developmental concerns. Paediatric services are recorded with a generic item number used by other consultant physicians and so it is not possible to isolate services delivered by paediatricians nor determine which of these were mental health-related. Of the limited published data that exist, it appears that a large proportion of paediatric consults are for behavioural and developmental concerns. Hiscock et al. (2017) found, based on a survey of paediatricians, that consultations involving developmental and behavioural problems represented 60% of all paediatric consults in 2013. Additionally, a recent study investigating health service use by mothers and infants in Victoria (Le et al., 2016) indicated that the most frequently used service for infant behaviour problems (e.g. crying) and maternal psychological distress was maternal child health nursing services. Had it been possible to include paediatric and maternal child health nurse services in our study, it would have shown an increased number of children in the youngest age group receiving mental health services, although not necessarily delivered by mental health trained clinicians.
Implications
This study is unique in creating a comprehensive picture of the level of mental health service delivery to infants, children, adolescents and youth in Australia, delivered through ambulatory mental health services.
The study findings will be used by the authors to inform the development of a mental health workforce and service planning framework which combines a comprehensive needs analysis of the infant, child and adolescent population with information on the current level of service delivery to generate workforce estimates in terms of fulltime equivalent workloads (Furber et al., 2015).
Of particular interest was the low level of service delivery to infants and children. We found that a very small proportion of children aged 0–4 years received mental health services through the mental health sector and also a small proportion of 5- to 11-year-olds. We identified in a previous study that 8% of infants (0–1 years) have ⩾5 risk factors for mental illness increasing to 20% of 10- to 11-year-olds, and that 8–10% of 4- to 13-year-olds had clinically defined psychological distress as measured by the Strengths and Difficulties Questionnaire (Goodman et al., 2000; Guy et al., 2016). Taking these findings with the results of the current study suggests that mental health service capacity needs to be several times larger to address need in children and adolescents. Combining the two studies suggests that a substantially greater number of children should be accessing mental health services, even if just for an assessment. It is concerning that so few 0- to 11-year-olds are accessing community mental health services where clinical expertise is concentrated. It may be that paediatric and maternal/child nurse services are an easier access point than mental health services for vulnerable families, suggesting a strong case for including specialist mental health competencies as part of the core training for paediatricians and maternal/child health nurses.
There was a substantial difference in the number of service occasions per person delivered in the MBS Better Access programme compared to the state/territory ambulatory services, which may reflect the likely greater complexity of clients accessing State-based services. A quick scan of the implementation protocols of some evidence-based programmes indicates that there is a range of recommended treatment durations, which vary according to factors such as severity of the distress and age of the child. For example, the Childhaven’s Childhood Trauma Treatment is based on a model of therapeutic childcare, which recommends children aged 0–5 years attend 5.5 hours of treatment, 5 days per week for a duration that is individually determined (depending on the circumstances of each child) (Armsden et al., 1998). This example and others (Amos et al., 2007) illustrate the need for ambulatory mental health services to be able to offer intensive and long-term therapy, through multidisciplinary teams and with a capacity to respond flexibly to the complex needs of highly vulnerable children and families, typical of those with mental health concerns.
It may be that state- and territory-based mental health services have greater capacity and are better placed to provide longer duration treatments. CAMHS typically use team-based, multidisciplinary models of care that are more able to provide the wraparound support that traumatised and/or disadvantaged families require. In our work investigating the level of mental health complexity in Australian children, we find that children (0–15 years) with high levels of distress and co-occurring adversities (e.g. parent mental illness and socioeconomic disadvantage) are the norm rather than the exception (Twizeyemariya et al., 2017). This finding, which is strongly supportive of the developmental origins of mental illness, underscores the importance of providing multidisciplinary services with the capacity to engage in longer term care. It also has implications for the balance of spending across primary (Better Access) and tertiary mental health services (state/territory services). Directing greater investment into specialist services for infants and children will have the greatest chance of interrupting mental illness trajectories.
Conclusion
Australia’s public health insurance system, Medicare, which the Australian and state/territory governments remain committed to, is often held up as a successful example of universal health care. Arguably, it upholds this reputation in relation to physical health. But as the health of populations changes over time and with the emergence of mental health as a leading global health concern, it is necessary for the universal access principle to be extended to mental health commensurate with need. The consequences of not investing in the mental health needs of children at the earliest stages of life means denying thousands of children the opportunity to reach their life potential as well as accumulating huge financial costs, as many of these children eventually become clients of the justice, child protection and disability sectors. This is not to suggest that the service response to adolescents and youth mental health is adequate given the high rates of distress in these age groups – but that the mental health needs of infants and young children must also be taken seriously.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
This study was part of a larger project on mental health workforce and service planning, which was funded by the National Health and Medical Research Council (NHMRC) in partnership with the Department of Health South Australia (Partnership Project APP1055351).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.