
Abstract
Introduction
Past research has indicated that Australians with a mental disorder or those experiencing high levels of psychological distress are less likely to have private health insurance (PHI) than those with no mental health problem. In 2004/05 the Private Health Insurance Snapshot Report found that 61% of all people aged 45–64 had PHI, whereas only 49% of people in this age group with long-term mental health problems had PHI. The report also found that 35% of adults (18+) categorised as having high levels of psychological distress (measured using the Kessler Psychological Distress Scale K10; high scores correlate strongly with the presence of a mental disorder (Furukawa et al., 2008)) had PHI compared to 53% of adults with moderate/low levels of distress (Australian Bureau of Statistics, 2006). Similarly, Banks et al. (2009) in a study of older persons in NSW found rates of PHI of 47% for those with very high psychological distress compared to 70% for those with low levels of psychological distress. This discrepancy in PHI status is a concern as it indicates socioeconomic inequality between individuals with and without a mental health problem. It is even more concerning if PHI plays an important role in access to mental health services, however we have little research examining whether this is the case.
The Australian system of mental health service provision is complex. It includes services delivered through primary care, specialist and allied mental health services. Overlaying these different types of services are different service providers (e.g. state/territory versus private provision) and different sources of funding (e.g. Commonwealth funding of Medicare subsidised services versus state mental health service provision versus private provision). Further, even for services subsidised through Medicare or PHI, there are usually out-of-pocket costs (representing the gap between the Commonwealth rebate in the Medicare Benefits Schedule (MBS) and those charged by the service provider) that are met directly by patients (Jorm, 2011). Overall, governments, state and Commonwealth have the dominant responsibility for the costs of mental health services. For example, in considering those individuals who received clinical mental health services in 2007/08, the Australian Institute of Health and Welfare report that 74% of people received MBS-subsidised services, 24% received public (state/territory) services and only 2% received services funded through private sources (Australian Institute of Health and Welfare, 2010).
As of September 2010, 45% of the Australian population had PHI coverage for hospital services and 52% had general treatment/extras coverage (Private Health Insurance Administration Council, 2007). PHI does not subsidise non-inpatient services that are already subsidised by Medicare. There are incentives and penalties in place to encourage individuals to take up PHI, including the 30% PHI rebate introduced in 1999 and the Lifetime Health Cover policy introduced in 2000. In 2007/08 total expenditure on mental health services in Australia was $5325 million (Department of Health and Ageing, 2010). After accounting for Commonwealth contributions to private psychiatric services (through Department of Veteran Affairs and the government contribution to the 30% rebate), the Department of Health and Aging estimates PHI contributed $185 million, or only 3.5% of total expenditure (Australian Institute of Health and Welfare, 2010; Department of Health and Ageing, 2010).
Adding to the complexity is a number of important recent reforms of the Australian healthcare system that have impacted on access to mental health services. The Better Outcomes in Mental Health Care Program was introduced in 2001 to facilitate mental health service provision (including access to allied health services) through primary care (Fletcher et al., 2007). In addition, the Better Access to Psychiatrists, Psychologists and GPs through the Medicare Benefits Schedule Program was introduced in late 2006, and provides a Medicare rebate for short-term psychological services (Pirkis et al., 2011b). In supporting treatment from allied health professionals, these new government-subsidised services overlap with the main area of mental health service provision that was previously limited largely to PHI or personal/out-of-pocket costs. PHI does not subsidise these MBS-supported services.
Based on this overview it may be the case that, at a population level, PHI does not currently play a large role in supporting access to mental health care; however there is little published data assessing whether this is the case. The 2007 National Survey of Mental Health and Wellbeing estimated that the profile of mental health services received by those with a (12-month) mental disorder were hospital care (4.1%), services from GP (16.4%), psychologist (9.1%) and psychiatrist (5.8%). However, only 34.9% of those with a mental or substance use disorder were found to receive any type of health service for that disorder (Burgess et al., 2009; Slade et al., 2009). It is, therefore, important to understand the factors associated with (lack of) access to appropriate evidence-based treatment and to identify whether there are particular groups within society with differential access to mental health care. Despite the emphasis on public and subsidised mental health services, having PHI may provide greater choice, options and timely access to mental health treatment through private medical or psychological services or through private hospital services. Also, there is a strong income gradient in PHI, with much higher rates of PHI amongst those with higher incomes (Banks et al., 2009). In considering those receiving clinical mental health services, the Australian Institute of Health and Welfare report that in 2007/08 individuals in the least disadvantaged SEIFA (socioeconomic indexes for areas) quintile represented around 40% of those receiving services in the private sector compared to 15% of those receiving services in the public sector. In contrast, those in the most disadvantaged SEIFA quintile represented only 20% of those receiving services in the private sector and 25% of those receiving services in the public sector (Australian Institute of Health and Welfare, 2010). This demonstrates a different profile of mental health service use based on socioeconomic circumstances and, given that PHI is associated with socioeconomic status, provides some support for the notion that PHI may be associated with mental health service use.
Aims and objectives
The current paper has two aims. First, to provide updated information regarding the association between PHI and mental health status across a wide age range and, second, to examine whether PHI is associated with self-reported mental health service use. Given only a global measure of mental health service use was available (see both Measures and Limitations sections), a series of additional stratified analyses were conducted to provide further insight into the nature of any association. Analyses were stratified by PHI type (e.g. hospital cover vs. extras cover) to evaluate whether PHI may facilitate access to different types of mental health services. Analyses were stratified by severity of mental health problem to evaluate whether PHI facilitated access to services for those with less/more severe conditions. Finally, analyses were stratified by household income to determine whether any effect of PHI was a reflection of broader socioeconomic differences.
Methods
The current investigation utilised data collected during 2009 from a large population-based survey: The Household Income Labour and Dynamics in Australia (HILDA) Survey. This manuscript reports secondary analysis of a non-identifiable dataset. Ethical approval for the collection and analysis of HILDA has been provided by the Human Ethics Advisory Committee at the University of Melbourne, Australia.
Sample
The HILDA Survey is a nationally representative household panel survey conducted annually since 2001. At baseline, there were 7682 responding households (response rate of 66%). Within households, 13,969 household members aged 15 years and over (92% of eligible population) completed a personal interview and 94% of these returned a self-completion questionnaire (SCQ). The original sample was obtained using a multi-stage approach, sampling households within dwellings in a selection of administrative areas. Additional respondents are added in each wave depending on changes within the household. Attrition rates across waves of the survey are similar to those found in other national household panel surveys (Melbourne Institute of Applied Economic and Social Research, 2011). Further details of the sample and survey methodology are published elsewhere (Wooden and Watson, 2002). The current analyses considered data from wave nine (release 9.0), with interviews conducted in 2009, as at this wave participants were asked about their PHI status. The final sample included 13,301 individuals aged 15–93 (9245 retained from original sample; 47.5% male).
Measures
Covariates. Respondents reported their gender, age and level of education. The areas included in the HILDA Survey comprise five locational categories: major city, inner regional, outer regional, remote, and very remote. For this study, a summary measure with three categories ‘1’ major city, ‘2’ regional location (inner and outer regional) and ‘3’ remote location (remote and very remote)’, was coded. The measure of financial hardship was based on four dichotomous items that assessed lack of basic goods and opportunities (‘Over the past year have the following happened because you were short of money: pawned or sold something, went without meals, unable to heat home, asked for help from welfare/community organisations’). A dichotomous summary measure representing any experience of hardship (one or more of the individual items versus none) was then calculated. A measure of income was also calculated to use in sensitivity analyses. This measure divided the 13 gross household income bands available in HILDA into four categories: Band 1: up to $29,999; Band 2: $30,000 to $59,999; Band 3: $60,000 to $124,999; Band 4: $125,000 or more. The coding of income bands was primarily chosen to provide an equal division of the sample size between all four bands, to maximise numbers in the stratified sensitivity analyses.
PHI was measured using two items. The first asked ‘Apart from Medicare, are you currently covered by private health insurance?’ Possible responses were ‘yes’ and ‘no’. Those who responded that they did have PHI were then asked ‘What type of health insurance do you have?’, and could answer ‘hospital cover only’, ‘extras cover only’, ‘both hospital and extras cover’. In multivariate models this measure was coded into two categories 0 ‘no PHI’ and 1 ‘any PHI’.
General mental health was measured using the Mental Health Index (MHI) of the Medical Outcomes Study Short Form (SF-36) (Ware et al., 1994). The measure was dichotomised to represent those with and without a mental health problem, using cut-offs recommended by Gill et al. (2007). Those with a score less than 50 were categorised as having a mental health problem, while those with scores equal or higher than 50 were categorised as having no mental health problem. In sensitivity analyses examining the impacts of severity, the sample was stratified into those with mild mental health problems (MHI score ≥ 40 and ≤ 50; n = 629), and those with moderate or major mental health problems (MHI < 40; n = 418).
Service use was measured using the question ‘During the past 12 months have you seen any of the healthcare providers listed below?’ The list of providers included: general practitioner, hospital doctor, specialist doctor, mental health professional (psychologist/psychiatrist), podiatrist, chiropractor or osteopath, physiotherapist, and optometrist.
Data analysis
Initially, sample statistics were calculated (Table 1). Rates of PHI status in association with mental health status were then calculated across four age groups (Table 2). Logistic regression was used to identify associations between PHI and mental health both univariately (Model 1) and then adjusting for relevant covariates (sex, age, education, financial hardship and location) (Model 2) (Table 3). Service utilisation rates based on PHI status were calculated for those with a mental health problem (Table 4). In the first instance rates were calculated representing univariate associations between service use and PHI status. This was followed by a series of multivariate logistic regressions that examined the association between PHI and service use after adjustment for relevant covariates. Finally, a series of sensitivity analyses were undertaken in relation to Table 4 to examine the association between PHI and access to a mental health professional in more detail.
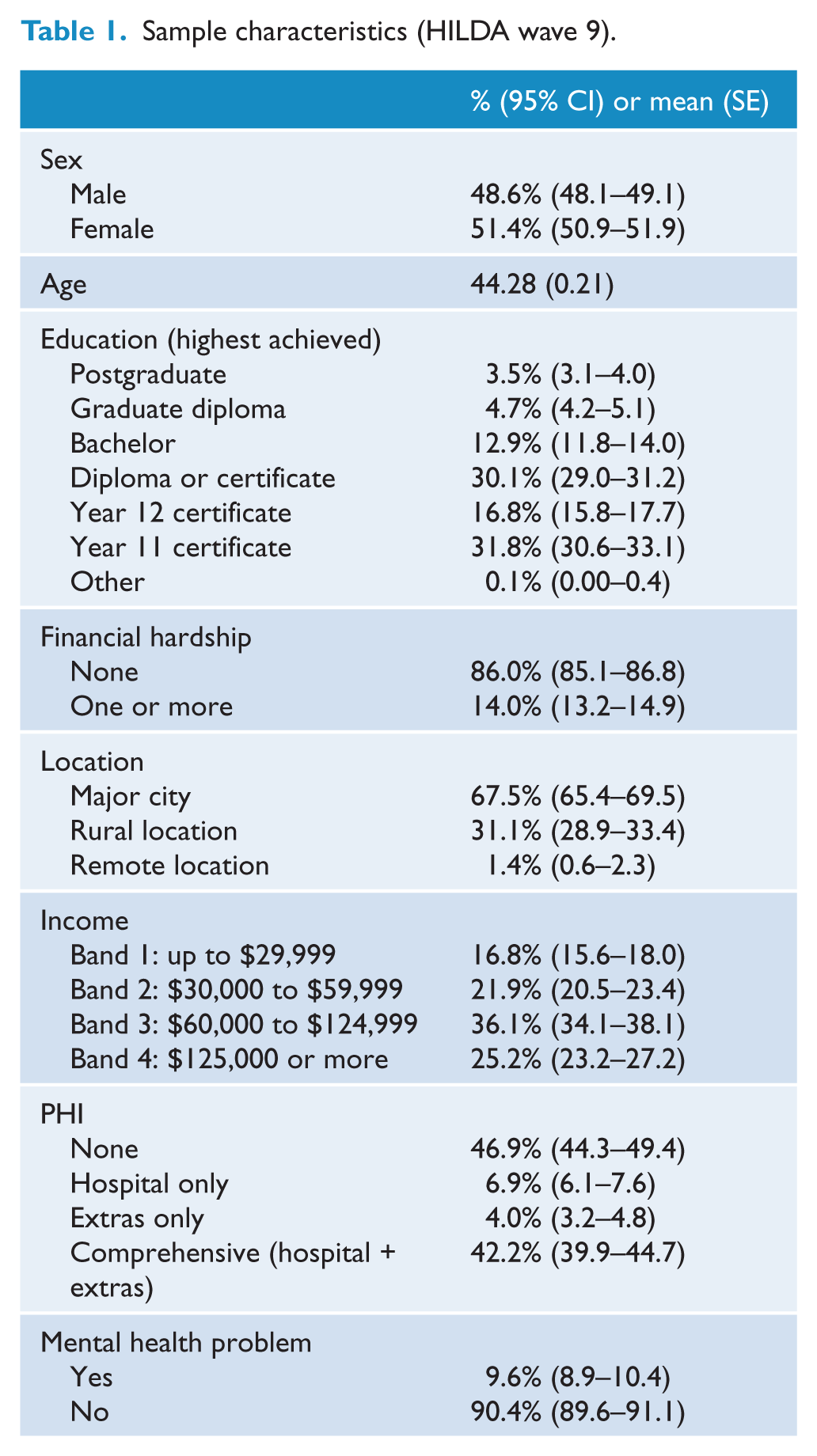
Sample characteristics (HILDA wave 9).
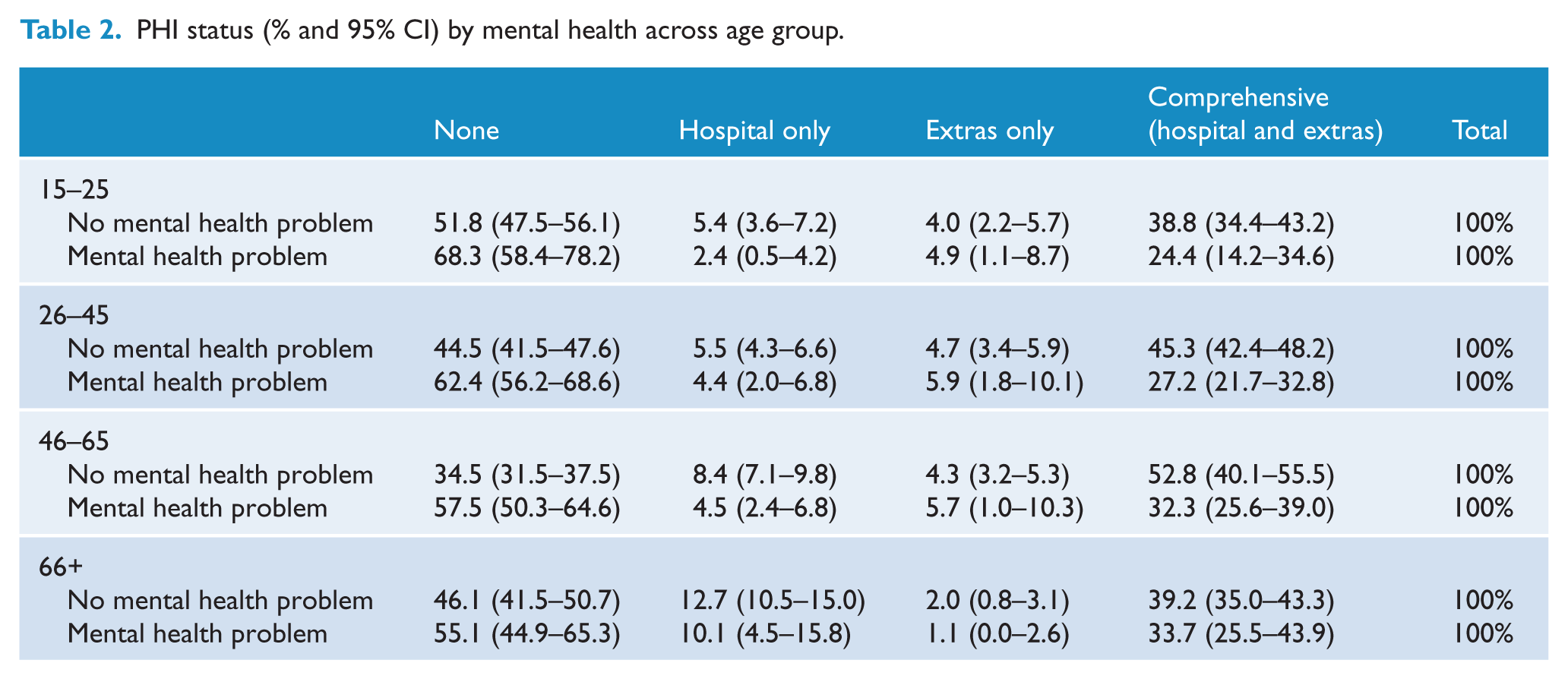
PHI status (% and 95% CI) by mental health across age group.
Association between mental health and PHI status.
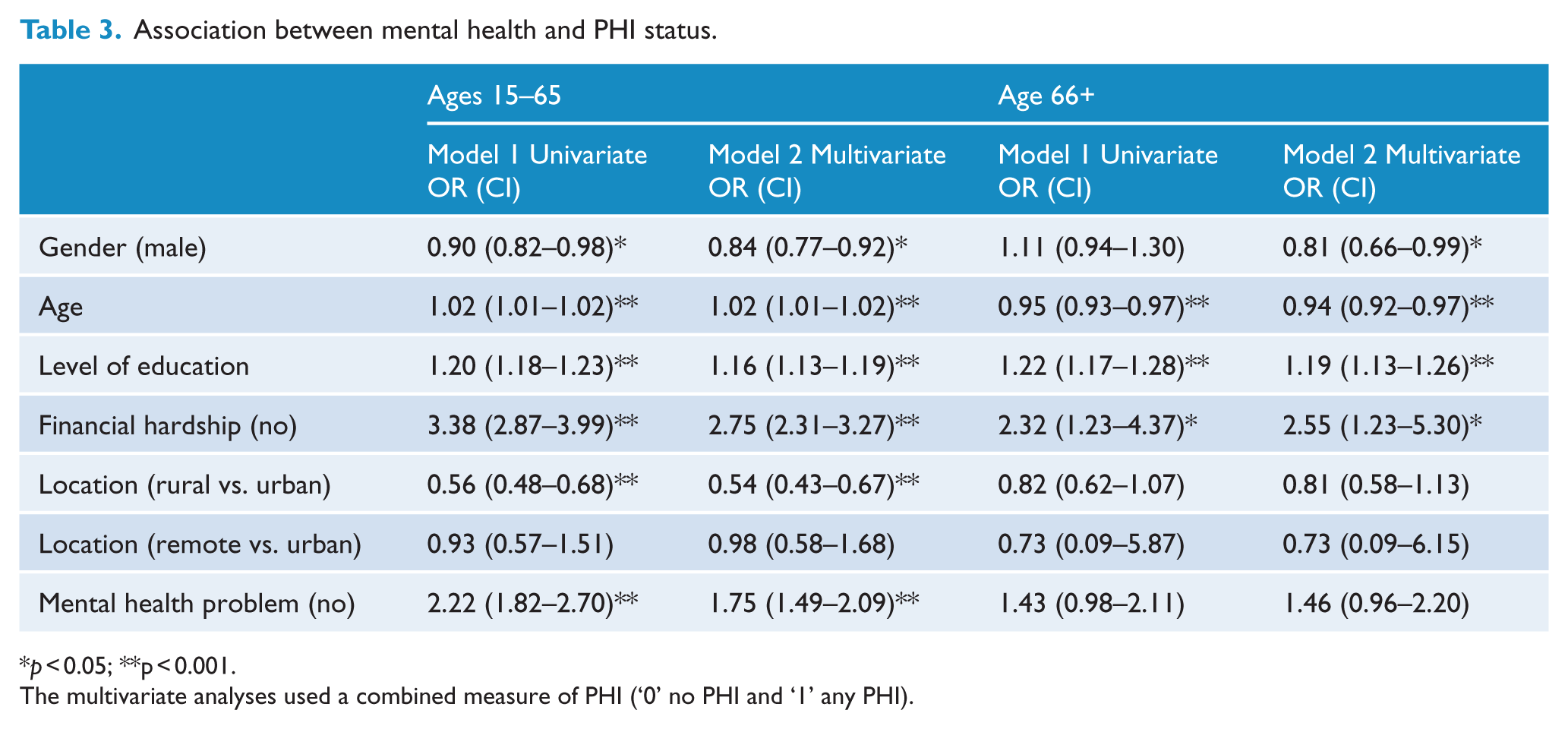
p < 0.05; **p < 0.001.
The multivariate analyses used a combined measure of PHI (‘0’ no PHI and ‘1’ any PHI).
Service access (% yes and 95% CI) in the past 12 months by PHI status.
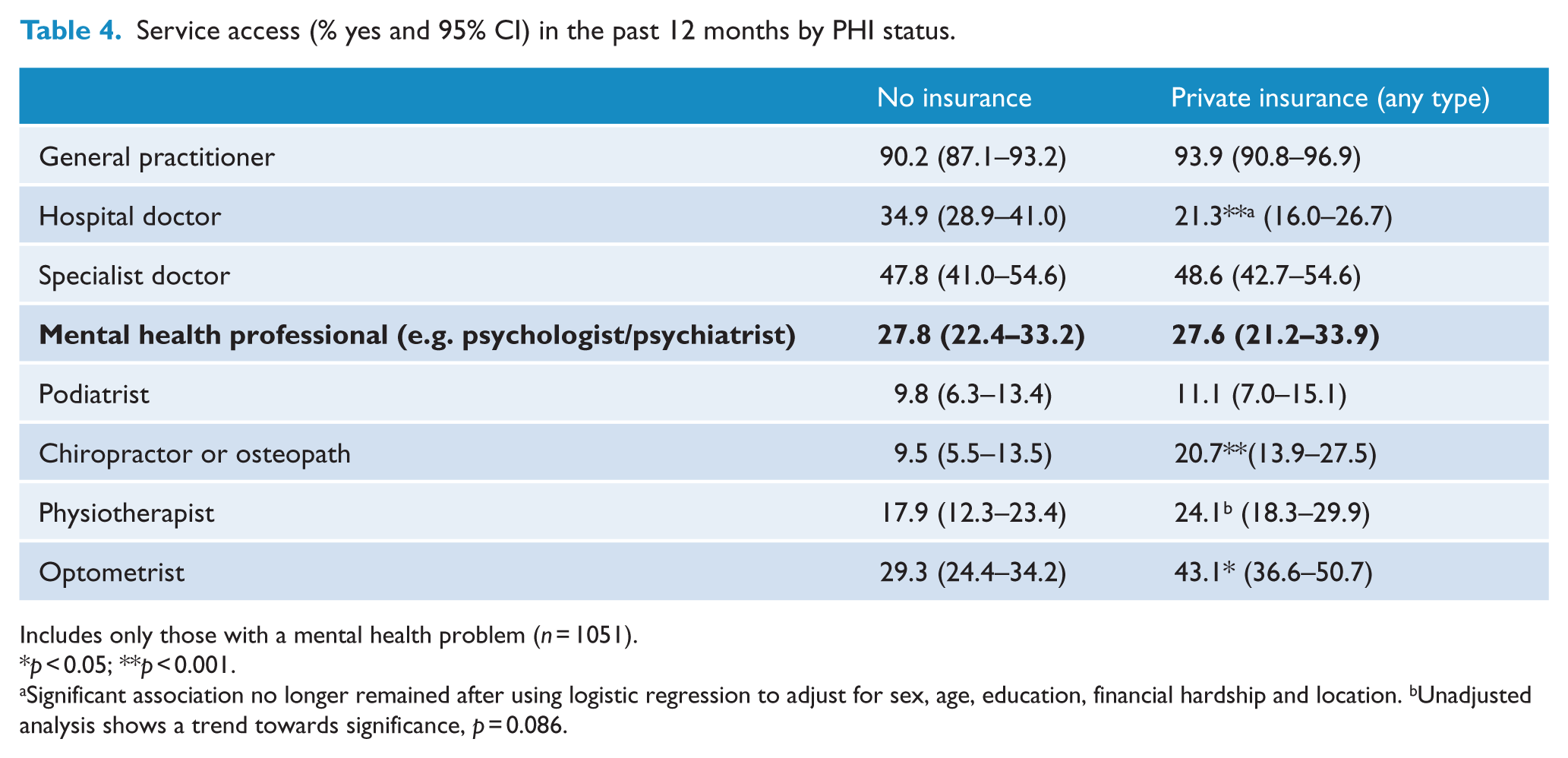
Includes only those with a mental health problem (n = 1051).
p < 0.05; **p < 0.001.
Significant association no longer remained after using logistic regression to adjust for sex, age, education, financial hardship and location. bUnadjusted analysis shows a trend towards significance, p = 0.086.
All analyses were weighted to reflect population characteristics using the person-level sample weights supplied with wave 9 of the HILDA dataset. The jack-knife method (using the 45 replicate weights available within the dataset) was used to calculate standard errors adjusting for the complex survey design. This allowed for the presentation of confidence intervals (CIs) around rate estimates in Tables 1, 2 and 4 and in the sensitivity analyses. To account for the complex survey design, we report the p-values associated with Wald’s chi-square test when testing rate differences in Tables 1, 2 and 4 and in the sensitivity analyses, as this test takes account of the stratification and clustering of the data when calculating estimates. In addition, the relationships between independent variables used in the logistic regressions (Tables 2 and 4) were screened for collinearity. All measures of tolerance (> 0.3) and variance inflation factor (< 3) were found to be within the acceptable range.
Cases with missing data were minimal (ranging from 0 to 1.4% of responses to individual items for HILDA data) and so were excluded on an analysis-by-analysis basis. Analyses were conducted using Stata 10.0.
Results
Table 1 presents the relevant characteristics of the sample (weighted). The data show that 9.6% of people were categorised as having a mental health problem. Overall, almost half (46.9%) the sample had no PHI, 6.9% had hospital cover only, 4.0% had extras cover only and 42.2% had comprehensive cover (hospital plus extras).
Associations between mental health and PHI
Table 2 reports the percentage of people with each type of PHI, for individuals with and without a mental health problem, across four age ranges. In the first three age groups, the findings indicate people with a mental health problem were significantly less likely to have comprehensive cover (hospital plus extras cover) and more likely to have no PHI, than people without a mental health problem (12–25: Wald χ2(3) = 21.62, p = 0.001; 26–45: Wald χ2(3) = 41.73, p < 0.001; 46–65: Wald χ2(3) = 43.16, p < 0.001). Although the trend was similar for the oldest age group, 66+, differences in PHI status for those with and without a mental health problem were not statistically significant (Wald χ2(3) = 4.26, p = 0.270).
Table 3 reports the univariate and multivariate associations between the covariates mental health and PHI (combined measure). These analyses are split for those younger than 65 and those older, given the discrepancy shown by age group in the previous analyses. For the younger age groups, model 1 shows that being female, older, having higher levels of education, reporting no financial problems, being in an urban (versus rural) area and, critically, reporting no mental health problem, were all independently associated with having PHI. These factors remained significant within the multivariate model. The analyses were repeated excluding those with extras cover only (as this group may be younger and/or with less financial means) and the results remained essentially the same. For the older age group, model 1 shows that being younger (within the age range 66–96), having higher levels of education and reporting no financial problems (but not mental health status) were independently associated with having PHI. The factors remained significant in the multivariate model.
PHI and service use
The following analyses included only those with a mental health problem to explore whether having (or not having) PHI affected access to a range of health services. Results indicated having PHI had no effect on whether people saw a mental health professional (psychologist/psychiatrist) during the past 12 months (Wald χ2(1) = 0.00, p = 0.959). Of those without PHI, 27.8% saw a mental health professional, and of those with PHI 27.6% saw a mental health professional. However, there were differences in service access for a number of other medical services based on PHI status. Table 4 shows that those with PHI were significantly more likely to see a chiropractor or osteopath (Wald χ2(1) = 12.00, p = 0.001), and optometrist (Wald χ2(1) = 7.47, p = 0.009), with a trend towards being more likely to see a physiotherapist (Wald χ2(1) = 2.58, p = 0.115). Those with PHI were also significantly less likely to see a hospital doctor than those without PHI. Additional analyses were conducted (logistic regression) adjusting for covariates (gender, age, education, financial hardship, rural/remote location) which explained this association. The other associations remained unchanged after adjusting for covariates.
Sensitivity analyses
The sample was stratified into a number of groups to gauge whether the lack of association between PHI and access to a mental health professional is a consistent finding, or whether the introduction of other factors, such as PHI type, symptom severity and income level, identifies instances where the association is less robust.
PHI type: The sample was stratified into those with hospital cover only, those with extras only, and those with hospital and extras cover. The analyses showed PHI type had no effect on whether a mental health professional was accessed: 21.0% (n = 7) of those with hospital cover only gained access, 27.3% (n = 12) of those with extras cover only gained access, and 28.6% (n = 82) of those with both hospital and extras cover gained access (Wald χ2(2) = 2.73, p = 0.274).
Mental health severity: The sample was stratified into those with mild mental health problems (MHI score ≤ 50 and ≥ 40; n = 629), and those with moderate or major mental health problems (MHI < 40; n = 418). The analyses showed there was no association between PHI and access to a mental health professional, regardless of severity. For those with mild mental health problems, 20.2% (n = 50) of those without PHI and 21.2% (n = 48) of those with PHI accessed a professional (Wald χ2(1) = 0.039, p = 0.844). For those with moderate/severe mental health problems, 36.9% (n = 80) of those without PHI and 38.4% (53) of those with PHI accessed a professional (Wald χ2(1) = 0.055, p = 0.815).
Household income band: The sample was stratified into four household income types as described in the methods. The analyses showed income type had no effect on the association between PHI and access to a mental health professional. In all income bands, PHI had no association with whether a professional was accessed. For income band 1: 21.1% (n = 15) of those with PHI and 31.1% (n = 60) without PHI accessed a professional (Wald χ2(1) = 1.72, p = 0.197); for income band 2: 31.6% (n = 17) of those with PHI and 26.8% (n = 30) without PHI accessed a professional (Wald χ2(1) = 0.297, p = 0.588); for income band 3: 26.4% (n = 28) of those with PHI and 23.3% (n = 37) of those without PHI accessed a professional (Wald χ2(1) = 0.184, p = 0.670): and for income band 4: 30.2% (n = 9) of those with PHI and 29.5% (n = 28) of those without PHI accessed a professional (Wald χ2(1) = 0.007, p = 0.933).
Discussion
PHI rates shown in this study are broadly consistent with industry figures. Individuals with a mental health problem were less likely to have comprehensive PHI, but we found no evidence that this influenced rates of mental health service use (access to a mental health professional (psychologist/psychiatrist)). This finding was consistent across severity and type of cover. There were also no significant differences within income categories, indicating the effects are not driven by concern about out-of-pocket expenses. There was some indication that those without PHI were more likely to see a hospital doctor and this association was explained after adjusting for covariates.
The current results confirm there is still a gap regarding the uptake of PHI between individuals with and without a mental health problem. Previous figures from 2004/05 indicated about 35% of adults with a psychological problem had PHI compared to 53% without a psychological problem (Australian Bureau of Statistics, 2006). Current findings from the HILDA Survey suggest these figures have changed little. Although we used a different measure of psychological distress, we found that 38.8% of people with a mental health problem and 57.1% without a problem indicated they had some level of PHI in 2009. Multivariate analyses point towards some explanations for this difference – common socioeconomic predictors of mental illness such as lower education and greater financial hardship (Lorant et al., 2003) were associated with not having PHI. However, poor mental health remained associated with PHI after adjustment for these factors. This association was found to be consistent across all age groups except for the eldest (66+), where the discrepancy was not statistically significant. These results indicate that, even after controlling for a range of socioeconomic measures, people with a mental health problem are less likely to take out PHI than those without a mental health problem. While not necessarily a causal relationship (other underlying unmeasured factors may be responsible), the results do suggest that those with mental health problems may not see a need for PHI to facilitate access to appropriate services, even within more economically advantaged segments of the community.
While the discrepancy in PHI status is a marker of inequity between those with and without a mental health problem, the current study found no difference in access to a mental health professional based on PHI status. Thus, those with and without PHI were equally likely to have received services from a mental health professional. However, as only a very broad measure of service use was available, without clarification regarding inpatient and outpatient services, we undertook a series of sensitivity analyses. Previous research shows the greatest expense for mental health services met by PHI is for hospital care. Therefore, in our stratified analyses we may have expected to see a difference in access to mental health services for those with hospital cover only, but this was not the case. It may be that because inpatient care is only a small segment of mental health services, differences were not evident. Alternatively, PHI may facilitate access to allied mental health services through extras cover, but again, no differences were evident in analyses that considered only those with extras cover.
It seems unlikely that the lack of association between PHI and access to mental health services is simply a sensitivity issue, as the data showed that PHI was associated with greater use of other allied health services. Those with PHI were more likely than those without to have seen a chiropractor, osteopath, physiotherapist (p = 0.086) and optometrist in the previous 12 months. Differences in service use based on PHI status in these categories, where PHI is required to gain some form of remuneration, suggest PHI does facilitate access to assistance.
We anticipated that PHI might also facilitate greater access to psychological services, as such services are commonly included in extras cover by most PHI agencies. One hypothesis for why this was not the case is that recent reforms in the mental health system, in particular the introduction of the Better Outcomes/Access schemes, have been effective in increasing access to allied mental health care for all Australians regardless of economic inequities (such as those associated with PHI status) (Jorm, 2011; Pirkis et al., 2011a). In fact, unpublished data does show that since the introduction of the Better Access program, PHI-subsidised psychological services have reversed a trend of annual increases and declined (data supplied by Commonwealth Department of Health and Ageing). Thus it may be that any benefit PHI bestowed in the past in terms of access to non-inpatient services is no longer present post the introduction of Medicare rebates for psychological services. In addition, previous research has demonstrated the critical role of the GP in accessing mental health services (Henderson et al., 2000). This finding is supported by the high percentages of GP access in the current study – a service which is not supported by PHI. One interpretation of the findings, therefore, is that access to mental health services is currently based on need rather than personal resources. While this interpretation is encouraging and implies equal access to mental health services, it is important to recognise that overall, the number of Australians with mental or substance use disorders accessing formal health services remained at one-third between 1997 and 2007 (Andrews et al., 2001), indicating that significant barriers to service access remain (Burgess et al., 2009; Slade et al., 2009).
Limitations
There are some limitations which must be noted. First, the current study was unable to report the level of PHI for different types of mental illnesses (e.g. affective disorders, psychotic disorders), as the dataset utilised did not contain diagnostic measures. Second, the service access item in HILDA asked broadly about accessing a ‘mental health professional (psychologist/psychiatrist)’, without further detail. While we found no effect of PHI status with this broad category of service use, it may be that if more specific information about the type of service is analysed (private psychiatrist/psychologist, community services, mental health crises assessment, etc.) differences emerge. For example, it was not possible to ascertain whether PHI provided other benefits such as greater choice or more timely access to mental health services. In addition, the analyses contained no information about the effectiveness or adequacy of services received. Third, it would have been preferable to have longitudinal data or multiple occasions of cross-sectional data on the use of mental health and other services, particularly covering the period before and after the introduction of the Better Access Program in 2006. This would have allowed us to more effectively evaluate the influence of the Medicare rebate for psychological services. However, the HILDA Survey did not ask about service use in sufficient detail in previous waves of data collection. Finally, the reduced numbers available in the sensitivity analyses limit the generalisability of these findings; however they also provide some support that the lack of association between PHI and access to a mental health professional is robust.
Conclusions
The current study found that in Australia in 2009, individuals with a mental health problem were less likely to have comprehensive PHI than those without a mental health problem. However, PHI status was not associated with differential access to a mental health professional during the past 12 months. Further research is needed to thoroughly investigate the role of PHI and how/if PHI status interacts with Better Access to facilitate access to mental health services.
Footnotes
Funding and Acknowledgements
PB is supported by NHMRC Population Health Career Development Award Fellowship No. 525410. This paper uses unit record data from the Household, Income and Labour Dynamics in Australia (HILDA) Survey. The HILDA Project was initiated and is funded by the Australian Government Department of Families, Housing, Community Services and Indigenous Affairs (FaHCSIA) and is managed by the Melbourne Institute of Applied Economic and Social Research (MIAESR). The findings and views reported in this paper, however, are those of the author and should not be attributed to either FaHCSIA or the MIAESR.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.