
Abstract
Objectives:
This study reports the rate of unmet needs for professional mental health care in a large multi-state sample of adolescents. We also sought to describe barriers to professional help, informal help seeking and future help-seeking intentions among adolescents with wholly unmet needs for counselling for mental illness.
Methods:
We collected measures of mental health, help-seeking and unmet needs in 1599 students (817 males and 781 females) in 16 schools (mean age = 17.7 years, standard deviation = 0.42 years). Adolescents meeting ‘case’ criteria for high psychological distress were classified as having no need, fully met needs, partially met needs or wholly unmet needs. Participants were asked about actual service use, perceived unmet needs, barriers to professional help, help seeking from other sources, use of self-management strategies and future help seeking intentions.
Results:
In all, 35.7% (n = 571) of the sample met criteria to be designated ‘cases’ with high psychological distress. Of these, 25.9% (n = 148) were classified as having ‘wholly unmet needs’ (cases of untreated prevalence with self-perceived unmet needs), translating into 9.3% of the original sample. Compared to cases with partially met needs, adolescents with wholly unmet needs engaged in significantly less self-help, used less informal help from family/friends and reported lower future help-seeking intentions. Common barriers to care included a preference for self-management and concerns regarding stigma.
Conclusions:
A concerning proportion of adolescents have untreated high psychological distress with wholly unmet mental health needs. This group is rendered particularly vulnerable by low rates of access to non-professional sources of help and low engagement in self-management strategies. Further research is needed to support this vulnerable group to access needed professional mental health help.
Introduction
Data from the second Australian Child and Adolescent Survey of Mental Health and Wellbeing (CASMHW) suggest that the rate of service use for mental disorders among adolescents appears to be increasing (Johnson et al., 2016). However, over a third of adolescents with mental health problems did not receive any professional mental health care (Lawrence et al., 2015) and little is known about the unmet mental health needs of this group.
It has been argued that epidemiological prevalence data alone are insufficient to estimate the unmet mental health needs of a population (Meadows et al., 2000c). It has been further suggested that methods for assessing unmet needs should consider service use and perceived need alongside disorder prevalence (Joska and Flisher, 2005). One method that combines all three factors and which has been commonly applied in adult populations is described by Meadows et al. (2000a). This method yields four categories: ‘no need’, ‘fully met needs’, ‘partially met needs’ and wholly ‘unmet needs’. For example, the partially met needs group includes individuals who received some mental health service but still indicated they had a need for mental health counselling.
Using this method, Meadows et al. found that while 11.0% of Australian adults were cases of untreated mental health disorder, more than half of these adults did not perceive a need for professional care. As such, Meadows et al. (2000a) noted this ‘no needs’ group may not be an efficient target for additional resources.
A corollary argument is that it might be a higher priority to target resources toward cases of untreated mental health disorder who do perceive unmet needs, that is, the wholly ‘unmet needs’ group. This is particularly the case for disordered adolescents with wholly unmet needs, since mental illness is highly prevalent in adolescence and early intervention for mental health problems confers long-term financial and social benefits to society (Fox et al., 2015). As such, a better understanding of the unmet mental health needs of adolescents might inform how to best distribute finite mental health resources to maximise long-term benefits.
Most of what is known about the unmet mental health needs of Australian adolescents comes from the Report on the Second Australian CASMHW (Lawrence et al., 2015, 2016). This large-scale study involved 2967 adolescents between the age of 11 and 17 who completed self-report questionnaires and adolescents aged 13–17 completed the self-report major depressive disorder module of the Diagnostic Interview for Children Version IV (DISC-IV). This revealed that almost 60% of depressed adolescents reported some level of unmet need for services for emotional or behavioural problems. Of these, almost one-third (32.2%) reported having wholly unmet needs. Of the types of need adolescents were asked about (information, medication, counselling, social skills training), counselling was the most commonly reported unmet need, with 42.0% of depressed adolescents reporting any unmet need for counselling and 20.4% reporting their needs were wholly unmet. This is consistent with findings in adult populations, where counselling has been recognised as the most common unmet need in Australian and other national samples (Dezetter et al., 2015; Meadows et al., 2000a). Indeed, Meadows et al. (2000a) used unmet needs for counselling specifically as the means for identifying cases of ‘untreated prevalence’ described above. Unmet need for counselling is of particular interest for several reasons. First, there are now empirically supported talk-based treatments for a range of mental health concerns. As such, counselling offers a way to reduce prevalence of mental disorder in the short term, while potentially offering skills and knowledge to manage difficulties later in life (Lambert, 2013). Second, adolescents often prefer counselling and talk-based therapies over other types of professional help, likely translating into higher treatment acceptability and retention (McHugh et al., 2013).
While the CASMHW offers some insight into adolescent unmet needs, it has several methodological limitations. In particular, although the common category labels of ‘unmet’, ‘partially met’, ‘fully met’ and ‘no needs’ were applied, the method for classifying unmet needs into these categories did not take actual service use into account as has been previously recommended (Joska and Flisher, 2005). Consequently, the unmet needs of untreated individuals could not be determined.
In contrast, the adult study of Meadows et al. (2000a) differentiates disordered individuals with unmet needs into two categories: Those reporting ‘partially met needs’ following some service use, and those with wholly ‘unmet needs’ who have not accessed services at all. This service use distinction is important because the path from perceiving a need for professional help to actually accessing this help is a complex process. We know from the help-seeking literature that factors influencing this process include adolescents’ beliefs about help seeking from professionals, preference for self-management and help seeking from non-professional sources (Gulliver et al., 2010; Rickwood et al., 2005).
For instance, several studies have identified attitudinal and practical barriers to adolescents receiving services (Rickwood et al., 2005). In the CASMHW report, reasons given for not receiving needed care included barriers associated with mental health literacy (33.1%), fear of stigma/not wanting to talk to a stranger (27.9%), a preference to manage by one’s self or with friends/family (26.2%) and accessibility issues such as transport and affordability (12.8%) (Lawrence et al., 2015). It would be useful to know the preferences and beliefs that act as barriers to care among those adolescents with wholly unmet needs for care. Given that a preference for self-management is consistently identified by adolescents as a major barrier to accessing professional help (Rickwood et al., 2005), we predict that adolescents with wholly unmet mental health needs will have utilised more self-management strategies than those with partially met needs (H1).
Adolescents are more likely to seek help from informal sources than formal sources (Boldero and Fallon, 1995). Although the appropriateness and effectiveness of informal help alone has been questioned (Rickwood, 1995), it has been recognised that such informal support can provide an important link into professional service use (Logan and King, 2001; Rickwood et al., 2015). As such, those who have sought help from non-professional sources are more likely to be supported into accessing professional help. We thus predict that fewer adolescents in the wholly unmet needs group will have accessed informal help than those in the partially met needs group (H2).
Future help-seeking intent has been found to be positively associated with actual help seeking (Wilson et al., 2005). Knowing the help-seeking intentions of adolescents with wholly unmet needs would allow us to estimate the likelihood they will access professional help in the future. We anticipate that those who have not used services would have lower help-seeking intentions than those who have used services (H3).
Objectives
This study estimates the percentage of unmet needs of adolescents with high psychological distress and explores the behaviours and attitudes of those adolescents who have wholly unmet needs for professional mental health care. The study has the following research questions.
What proportion of adolescents with high psychological distress fall into each category of need for professional mental health care? In particular, what proportion of adolescents have wholly unmet needs for professional mental health care?
What barriers to professional mental health care do adolescents with wholly unmet needs experience?
To what extent do adolescents with wholly unmet needs engage in self-management strategies or access informal supports?
How likely are these adolescents with wholly unmet needs to seek needed help in the future?
We hypothesise that compared to adolescents with partially met needs, adolescents with wholly unmet needs will engage in more self-management strategies, be less likely to seek help from informal sources and have lower future help-seeking intentions.
Method
Participants and procedures
Participants were year 12 students recruited from 17 Catholic secondary schools from two Australian states (New South Wales and Queensland) who were participating in the Australian Character Study (ACS). Thus, data in this study were collected as part of the ACS during 2014. Catholic schools account for approximately one quarter of Australian secondary school students, and the demographic makeup (e.g. ethnicity, employment and religious beliefs) of these schools broadly reflects that of the general Australian population (Australian Bureau of Statistics, 2010). The average Index of Community Socio-Educational Advantage (ICSEA) for Australian schools in 2013 was 1000 (Australian Curriculum Assessment and Reporting Authority, 2014) and the average index for the schools in the ACS was 1026. Active consent was obtained from all participants in the study, and participation was voluntary and without financial incentive. Ethics approval was obtained from the University of Wollongong Human Research Ethics Committee (HE10158). Data for the analyses in this study can be accessed at https://figshare.com/s/aa663e27a13ab48ed1a6. Students completed the pencil-and-paper survey in class rooms, where teachers supervised and collected the surveys.
Measures
Mental health
Mental health was measured using the General Health Questionnaire –12 (GHQ-12) (Goldberg et al., 1997). The GHQ-12 is a self-report measure consisting of six positively worded items (e.g. Have you recently been feeling reasonably happy, all things considered?) and six negatively worded items (e.g. Have you recently felt you couldn’t overcome your difficulties?). Items were rated on a 4-point Likert scale ranging from 0 to 3, with varying item response stems and with higher scores indicating worse mental health. The GHQ-12 has been validated against the Structured Clinical Interview for Diagnostic and Statistical Manual of Mental Disorders-IV-Test Revision (SCID-IV, First et al., 2002) as a valid measure of general psychological distress and mental health in Australian adolescents (Baksheev et al., 2011). The GHQ-12 also had good reliability in the adolescent sample (Baksheev et al., 2011; α = 0.87), which was also demonstrated in the present study (α = 0.90).
Total GHQ-12 scores were used to determine ‘caseness’. Individuals whose GHQ-12 total score fell above the cut-off (13 for males and 18 for females) were identified as ‘cases’. These cut-offs were identified by Tait et al. (2003) in an Australian adolescent sample and ‘At a threshold of 13/14 for males and 18/19 for females the overall sensitivity was 88.8% and the specificity was 87.3% with 13% of cases misclassified’ (p. 378). While Baksheev et al. (2011) identified lower cut-offs in an Australian adolescent sample, these yielded a large proportion of cases in our study (almost 70%). Severity of mental health problems has been associated with help seeking from professional sources and as such may influence need group status (e.g. Van Zoonen et al., 2015). The Tait et al. cut-offs were preferred for this study as they were more conservative and required higher scores (i.e. higher symptom severity) in order to be classified as cases. By using these high thresholds for determining caseness, we ensured that only those meeting stringent criteria for caseness were included in analysis. All unmet needs analyses were conducted on the case sample only.
Unmet need classification, help seeking–related behaviours and help seeking–related attitudes
The ACS survey combined items from established measures to assess help-seeking and unmet needs. Perceived unmet needs, barriers to professional care and use of self-management strategies were assessed using items from the Perceived Need for Care Questionnaire (Meadows et al., 2000b). Actual professional help-seeking and future professional help-seeking intentions were assessed using items derived from the General Help Seeking Questionnaire (Wilson et al., 2005).
Unmet need classification
Classification was modelled on the method of Meadows et al. (2000a), combining service use and perceived unmet needs. Perceived unmet mental health need was determined by the item ‘In the past 12 months did you ever feel you needed but did not receive counselling for mental illness?’ (‘yes’ or ‘no’ response). Actual service use was determined by the item ‘In the past 12 months have you had a consultation with any professional for mental health problems?’ (‘yes’ or ‘no’ response). See Figure 1 in Results for a flow diagram representing need classification and proportions of adolescents falling within each classification.
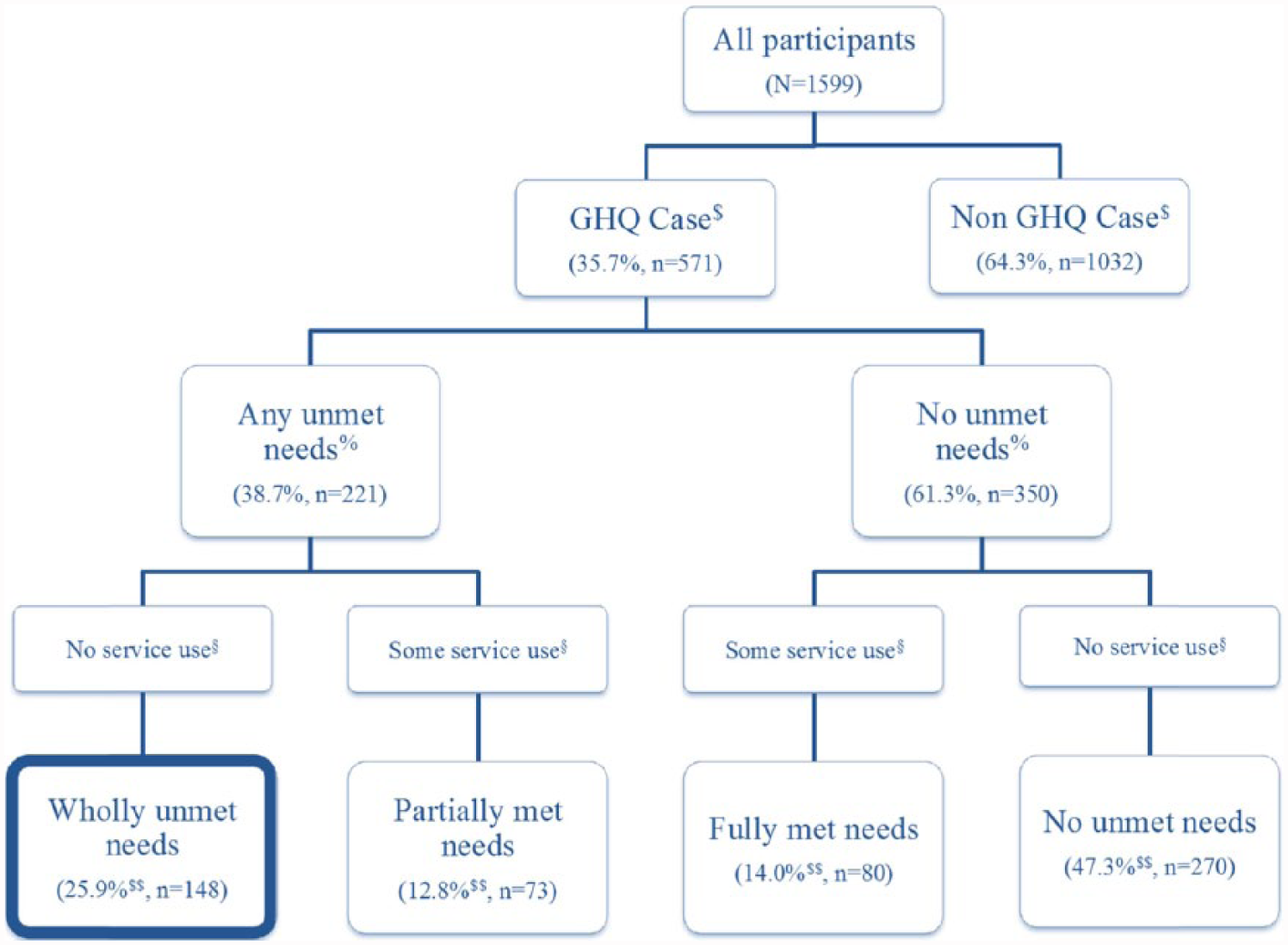
Unmet need classification flow chart.
Cases who endorsed ‘yes’ to needing but not receiving counselling were classified as having ‘any unmet need’. Cases with any unmet need who reported accessing professional help in the past 12 months were classified as having ‘partially met needs’. Cases with any unmet need who had not accessed professional help were classified as having ‘wholly unmet needs’.
Practical and attitudinal barriers to receiving needed services
Cases with any unmet needs were asked ‘What was the main reason for not getting any counselling from health professionals about mental illness?’ Options provided were, a preference for self-management, thinking nothing could help, not knowing where to get help, being afraid to ask for help, being unable to afford the money, asked but did not receive help, that they got help from another source and ‘other’.
Actual help seeking from other sources
Participants were asked three separate yes/no questions about help seeking from other sources, which all began and closed with the same stem: ‘In the past 12 months, did you ever … [seek help from friends or family]/[use the internet to get help or information]/[use telephone counselling] … for mental health problems?’.
Self-management strategies
Participants were asked, ‘In the past 12 months did you use self-management strategies to cope with mental health problems?’ Options provided were increased level of exercise, did more enjoyable activities, sought support from family or friends, cut out alcohol or other drugs, used alcohol or other drugs, ‘other’ and ‘none of the above’. The proportion of the population who used each strategy was reported.
The number of ‘healthy self-management strategies’ used was also calculated for each participant. This variable was a simple count of the number self-management strategies used, excluding use of drugs, ‘other’ and ‘none’.
Future help-seeking intentions
Participants were asked, ‘If you were to experience a distressing mental health problem in the future, how likely is it that you would seek help from a mental health professional?’ Participants rated their intent on a 7-point Likert Scale from 1 (extremely unlikely) through to 7 (extremely likely).
Statistical analysis
For ‘reasons for unmet needs’, we ran a series of 2 × 2 chi square analyses to identify significant differences between the wholly unmet needs group and the partially met needs group. For help from other sources and use of self-management strategies, we ran 4 × 2 chi square analyses to identify significant differences between all groups. Where we found significant differences, we ran a single step-down 2 × 2 chi square analysis comparing the wholly unmet and partially met needs groups. Only significant results are reported. Chi square analyses were not run for cell sizes with less than 10 participants. Between groups t-tests were conducted to examine differences in help-seeking intentions and number of self-management strategies used by the partially and wholly unmet needs groups. Bonferroni adjusted p-values were used for each block of analysis due to multiple comparisons.
Results
Participant characteristics
Surveys were excluded from analysis if the data required to determine caseness (mental health and gender) or unmet need status (perceived unmet need and actual service use) were missing (n = 42). The final sample consisted of 1599 adolescents (818 males, 781 females) who were an average age of 17.7 years old (standard deviation [SD] = 0.42). Adolescents in the sample identified mainly as Christian (60.4%), while 15.9% identified with other religions (Jewish, Muslim or ‘other’) and 23.7% indicated having no religious affiliation. The majority of the sample identified as Caucasian/Western European (63.6%), with a number of other ethnicities reported in small proportions, including Indigenous Australian (1.1%) and Asian (2.8%).
Case identification
Participants who completed less than 10 items on the GHQ-12 were excluded from analysis (n = 3). If at least 10 items were completed, missing values were replaced with prorated scores (mean of available items multiplied by 12). Only 12 cases were prorated.
Using the Tait et al. (2003) cut-offs, 35.7% (n = 571) of participants were identified as cases with high psychological distress (males = 341, females = 230). Table 1 presents GHQ-12 descriptives for the overall sample and case sample, reported by gender due to the differing cut-offs for males and females. As was expected given the different GHQ-12 cut-offs for males and females the mean GHQ-12 score for male cases (M = 18.49, SD = 5.44) was lower than for females (M = 23.25, SD = 4.80).
Mean and standard deviation total scores on the GHQ-12.

GHQ 12: General Health Questionnaire.
Unmet needs classification
Figure 1 presents the proportions of psychologically distressed adolescents falling within each need status classification. Almost 40% of the case sample reported having any unmet need for counselling for mental illness in the past 12 months. Notably, 25.9% (n = 148) of the case sample reported having ‘wholly unmet needs’. This represents a rate of ‘untreated prevalence’ with unmet needs of 9.3% (n = 148) of the original sample
Secondary analyses were undertaken to examine whether gender or severity of psychological distress might impact need group status (wholly unmet and partially met). The results of a univariate analysis of variance (ANOVA) indicated a significant gender by need status interaction, F(1, 217) = 8.45, p < 0.005, such that females showed no significant difference in severity between needs status groups (wholly unmet M = 23.61, SD = 4.89; partially met M = 24.31, SD = 5.36), but males within the wholly unmet needs group had significantly lower GHQ-12 scores (M = 18.92, SD = 5.80) than those in the partially met needs group (M = 24.25,SD = 6.00), t(103) = −4.13, p < 0.000.
Practical and attitudinal barriers to receiving needed professional care
Table 2 presents the rates of endorsement of reasons for not receiving needed counselling for mental illness. The most commonly endorsed reason for both wholly unmet and partially met needs groups was a preference for self-management, followed by a fear of asking for help. Compared to the partially met needs group, a lower proportion of the wholly unmet needs group (27.4%) endorsed ‘not thinking anything could help’, χ2(1, N = 221) = 8.88, p = 0.003. This was the only significant between-group difference.
Main reasons for not receiving needed counselling for mental illness among adolescents with mental health problem and unmet needs.
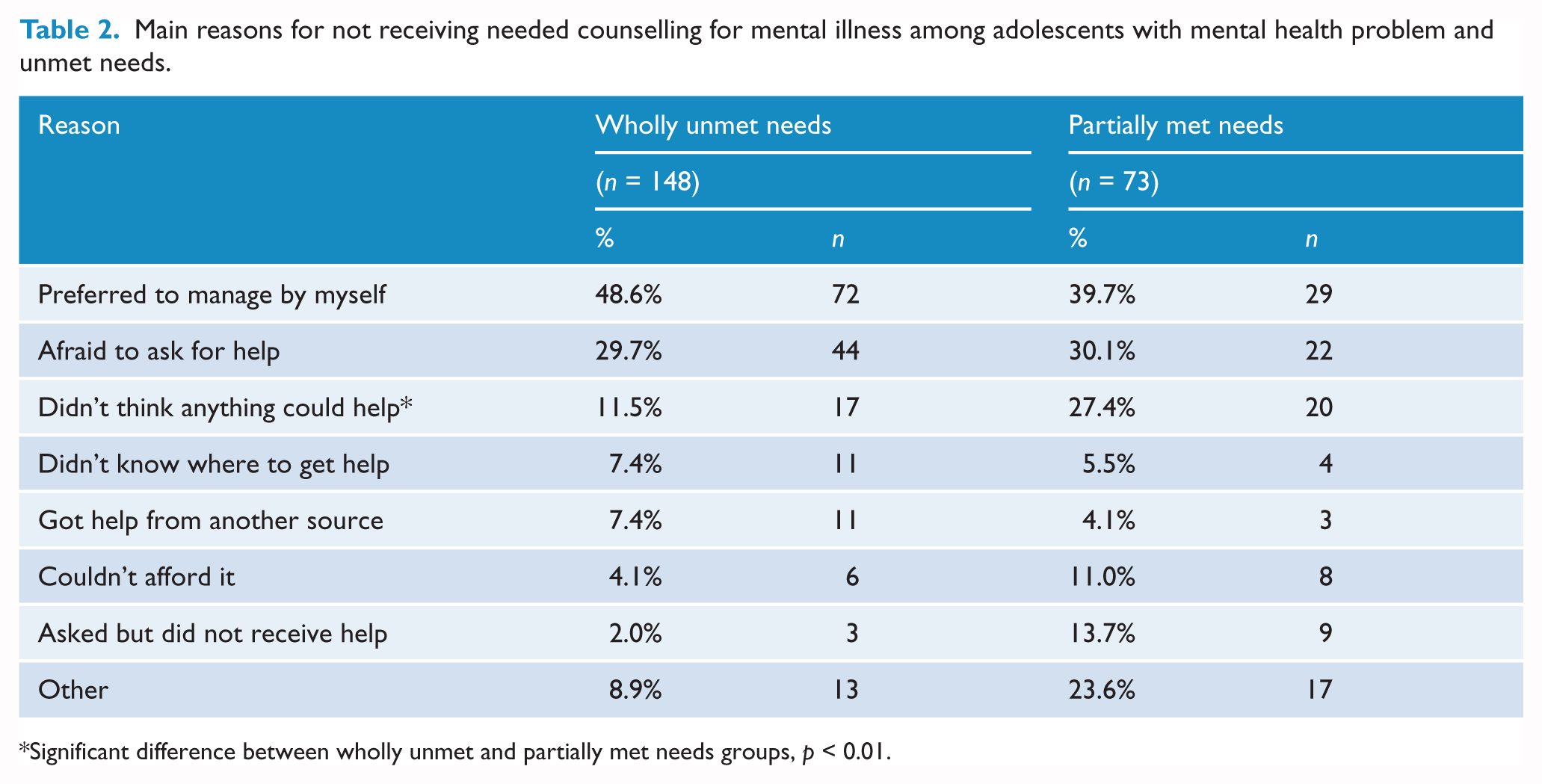
Significant difference between wholly unmet and partially met needs groups, p < 0.01.
Help seeking–related behaviours and attitudes
Use of self-management strategies
The wholly unmet needs group used an average of 1.28 healthy self-management strategies (SD = .93), which was significantly fewer than the partially met needs group (M = 1.67, SD = 1.16), t(120) = −2.54, p < 0.05.
Table 3 reports the proportion of each needs group who reported using each self-management strategy. Almost one-third of the wholly unmet needs group reported using drugs or alcohol as a self-management strategy and more than 10% reported using no self-management strategies at all. The only strategy that was significantly different between the partially met and wholly unmet needs groups was seeking support from family/friends, χ2(1, N = 221) = 4.81, p = 0.02, with a smaller proportion of the wholly unmet needs group having used this strategy.
Self-management strategies used by adolescents with high psychological distress.
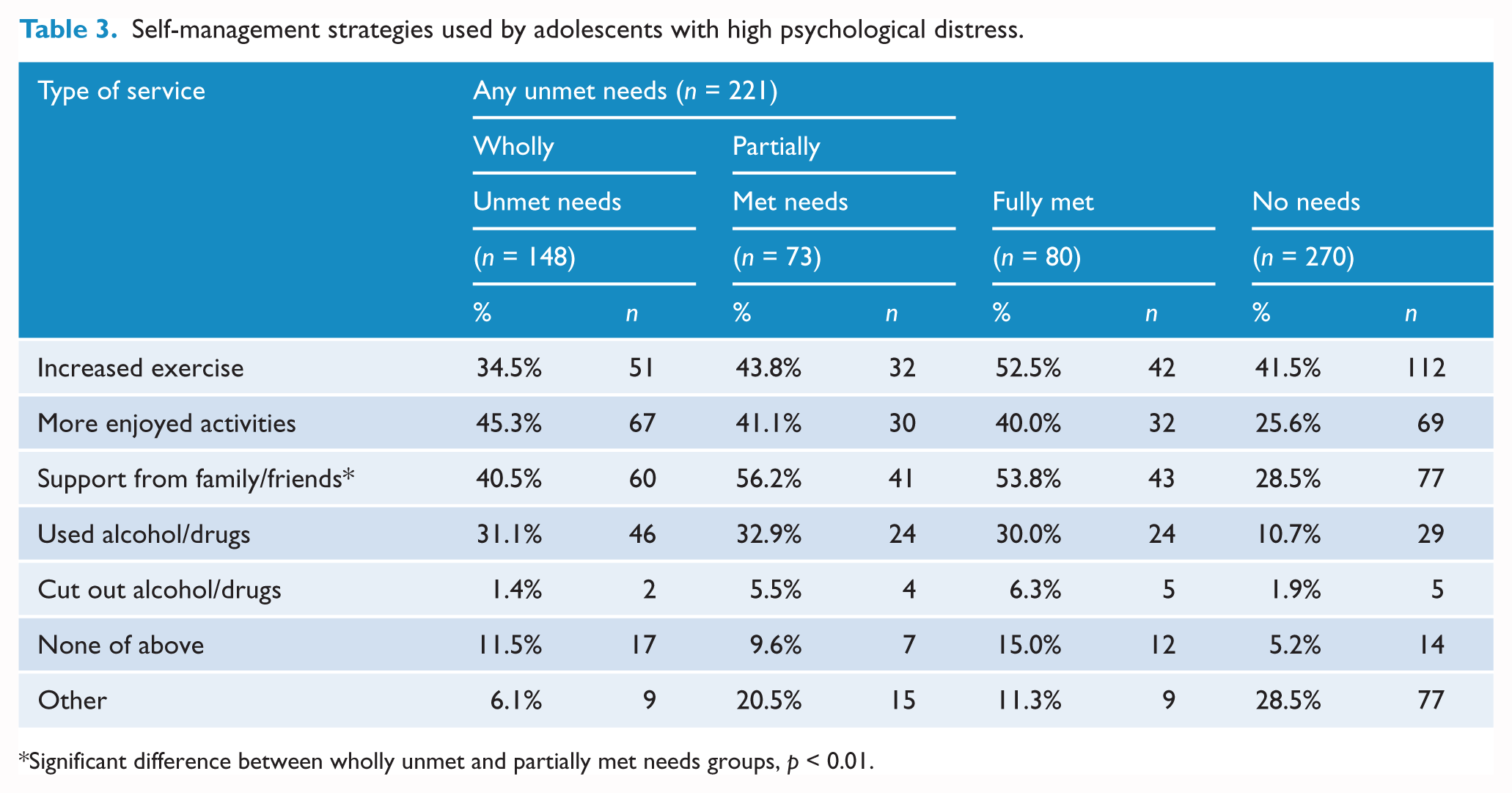
Significant difference between wholly unmet and partially met needs groups, p < 0.01.
Help from other sources
Table 4 reports the proportion of adolescents in each needs group who used informal sources of help for mental health problems in the past year. The percentage of participants who sought help from family/friends and the Internet differed according to need status, family/friends: χ2(3, N = 561) = 89.91 p < 0.001 and Internet: χ2(3, N = 561) = 110.29, p < 0.001. Results of step-down chi square analyses indicated that a smaller proportion of the wholly unmet needs group sought help from friends/family, χ2(1, N = 219) = 16.18, p = 0.000, compared to the partially met needs group.
Use of help from other sources by adolescents with high psychological distress.
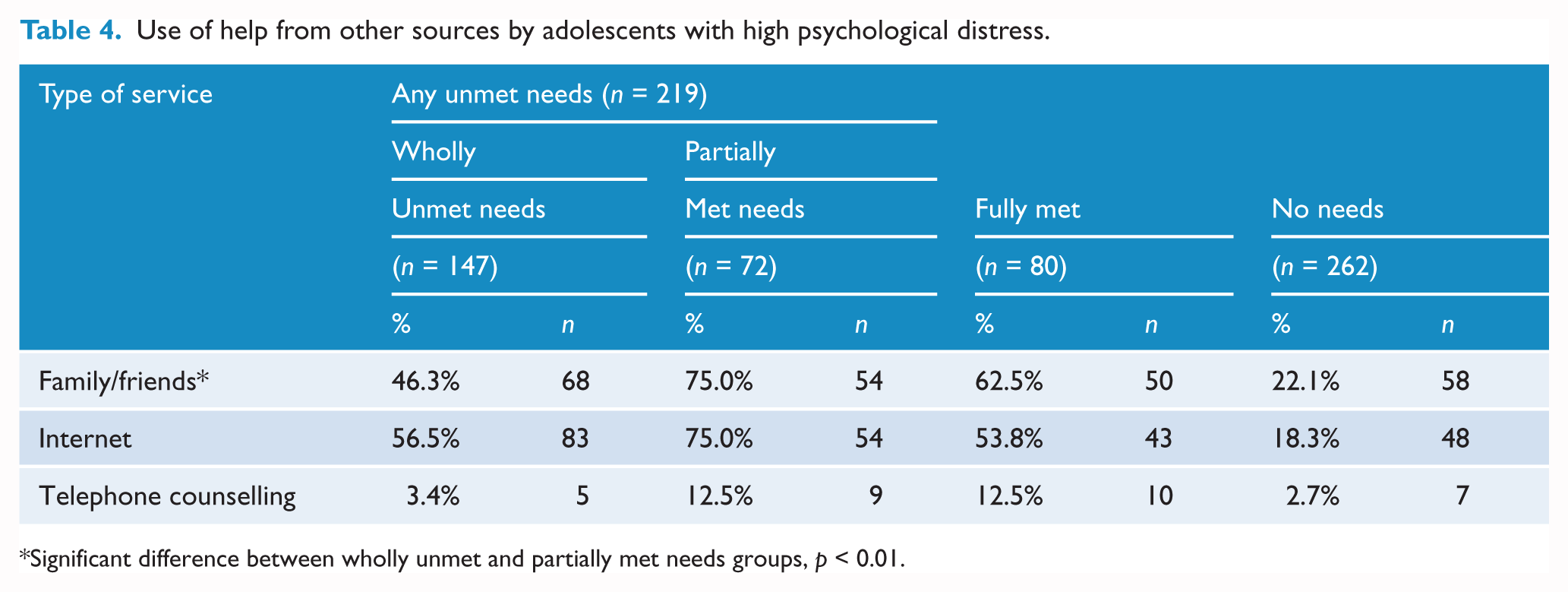
Significant difference between wholly unmet and partially met needs groups, p < 0.01.
Help-seeking intentions
The wholly unmet needs group had a mean help-seeking intention score of 3.42 out of 7 (SD = 1.78). This was significantly lower than the intentions score for the partially met needs group (M = 4.39, SD = 1.68), t(217) = −3.85, p < 0.001.
Discussion
Over one-third (35.7%) of adolescents in the current study met criteria to be considered cases based on high psychological distress. Using adolescent self-report measures, the CASMHW (Lawrence et al., 2015) reported that 19.9% of all adolescents had very high or high levels of psychological distress. It further estimated that 14% of adolescents aged 16–17 years met criteria for depressive disorders alone. Although these rates are lower than the proportion of cases identified in the current study, this is likely due to the wider inclusion criteria based on the GHQ-12 scores. Thus, it is possible that some of those considered ‘cases’ using the GHQ would be considered sub-threshold in terms of formal diagnostic criteria.
This study sought to report the rate of unmet mental health needs and particularly wholly unmet needs in an adolescent population. More than one quarter (25.9%) of adolescents with high psychological distress in the current study had wholly unmet needs for care. This equates to 9.3% of our total sample (cases and non-cases combined) identified as cases of untreated prevalence with wholly unmet needs. This is a substantial proportion of the population, and is much higher than the 3.6% estimated for the Australian adult population (Meadows et al., 2000a). This suggests the rate of cases of wholly unmet needs is higher for adolescents than adults.
While the use of different definitions (CASMHW did not account for actual service use) prevents comparison of the wholly unmet needs group with the CASMHW findings for adolescents, the ‘any unmet needs’ group reflects perceived unmet need regardless of service use and so can be compared. In the CASMHW, 28.9% of depressed adolescents reported any unmet need for counselling, relatively lower than the 38.7% of adolescents with any mental health concerns in the current study. Given our more inclusive sample, this suggests that adolescents experiencing high psychological distress other than depression may be more likely to perceive unmet needs for professional care.
This study also sought to explore barriers to receiving professional mental health care. The most frequently endorsed barriers in the current sample were related to stigma and preference for self-management. Similar proportions of the wholly unmet needs group and partially met needs group endorsed each of the main barriers to care. Interestingly, the only significant difference between two unmet needs groups was that more cases with partially met needs reported ‘thinking nothing could help’. This raises the question about whether some previous service was viewed as ineffective, leaving adolescents feeling more helpless in the face of ongoing high psychological distress. The help-seeking literature has recognised that negative help-seeking experiences are associated with negative beliefs and attitudes about future help seeking (Rickwood et al., 2005). The present findings highlight the importance of ensuring that adolescents view their initial professional service experience as ‘helpful’ in order to promote future help seeking when needed.
Consistent with previous help-seeking research (e.g., Wilson and Deane, 2012), the most frequently endorsed reason for not receiving needed counselling in the current sample was a preference for managing by one’s self. As such, we expected that those with wholly unmet needs would engage in more self-management strategies than those with partially met needs. This was not the case. Adolescents with wholly unmet needs used significantly fewer management strategies than those with partially met needs. We might speculate that adolescents who engage in more self-management activity have internal or external resources (e.g. problem-solving skills or high-quality social support) that make them more active help-seekers in general, seeking help from both professional and informal sources. Perhaps adolescents with wholly unmet needs have fewer resources or a lower capacity to activate these resources such that they can neither resolve their mental health problem independently nor successfully overcome barriers to access professional help.
We explored the possibility that severity of psychological distress might impact need group status, and found that severity of psychological distress was not different between the wholly unmet and partially met needs groups for females, but was different for males. For males, greater severity of psychological distress was experienced by those in the partially met needs group. It could be that their higher level of problem severity has driven them more toward help seeking compared to the wholly unmet needs group. Notably, this effect was present even when using a high distress threshold to determine clinical case status.
The help-seeking literature recognises that informal support (particularly parents) plays an important role in facilitating adolescent service use. Less than half (46.3%) of adolescent cases with wholly unmet needs had sought help from family/friends, significantly fewer than those with partially met needs (75.0%). This supports our hypothesis that those with wholly unmet needs access less informal help compared to those with partially met needs. Ryan et al. (2015) argue that a variety of parent-related factors affect adolescent help seeking. In the context of the present findings, this suggests that investigating parental factors that influence adolescent help seeking could provide further insight into the unmet needs of adolescents.
In regard to future help-seeking intentions, it was found that adolescents with wholly unmet needs reported being somewhat unlikely to seek professional help if they were to experience a distressing mental health problem in the future. Consistent with our hypothesis, they reported significantly lower help-seeking intentions compared to the partially met needs group. These findings raise further concern about the future trajectory of adolescents with mental health problems and wholly unmet needs. They not only fail to access professional services, but also fail to actively help themselves or access informal help and are somewhat unlikely to seek help in the future. This raises the concern that this vulnerable group of adolescents may continue to experience untreated high psychological distress into adulthood.
Limitations
The main limitation of this study is the focus on adolescents in the Catholic school system. Although this sample was similar to other adolescent school attendees with regards to many demographic variables, and covered 16 schools across two states, caution should be used when generalising these results. In addition, ‘caseness’ was determined by self-report on a standardised questionnaire (GHQ-12). The use of diagnostic interview in addition to questionnaire data would have further strengthened the designation of caseness, although the GHQ-12 has been previously (Baksheev et al., 2011) validated against the gold-standard of diagnostic clinical interview (SCID-IV, First et al., 2002).
The use of brief single-item measures limits interpretation of some variables, for example, the question assessing service use asks about ‘consultation with any professional for mental health problems’, but it is unclear who respondents consider ‘professionals’ (e.g. welfare teachers in schools or internet counsellors). This study combined ‘friends and family’ to examine help seeking from non-professional sources. As such, we could not differentiate between help from friends versus family. Given that parents and friends likely play different roles in the help-seeking process (Rickwood et al., 2015), investigating these supports as distinct types of informal help would have offered additional insight into factors associated with adolescent unmet needs. Future research should clarify and distinguish these help sources in more detail.
Conclusion
Overall, adolescents with high psychological distress and wholly unmet needs are particularly vulnerable. They received no professional help, accessed little informal help, engaged in few self-help strategies and are unlikely to seek professional help in the future. This group accounted for over 25% of the case sample and almost 9.3% of our overall adolescent sample. As such, it is important to investigate this vulnerable group further in order to understand how we might better support access to needed professional mental health care.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was partially funded by grants from the Australian Research Council (DP110100989, DP140103874, DE140100080).