
Abstract
Introduction
Mental disorders are highly prevalent in young people, with half of all lifetime case-level mental disorders starting by age 14 and three-quarters by age 24 (Kessler et al., 2005). However, many young people do not seek help (Reavley et al., 2010; Sawyer et al., 2007) or delay seeking help (Marshall et al., 2005), which may contribute to adverse consequences for their long-term mental health, and secondary effects on education, occupational achievement and social relationships (Harris et al., 2005). Furthermore, recent evidence has highlighted that mental disorders are the largest contributors to disability in young people (Mathews et al., 2011). Such evidence comprises the argument for youth-focused services which integrate mental health, substance use and vocational recovery services (McGorry, 2007). In 2006, the Australian government responded to this call by providing funding for headspace, a national youth mental health initiative. This funding has been used to set up youth-oriented services for the 12–25-year-old age group in 30 regions across Australia (McGorry et al., 2007). For this type of service initiative to be effective, it must become known to young people, especially those in need. Furthermore, given that young people are an important first port of call for peers with mental health difficulties (Yap et al., 2011), their awareness of such services is also important for facilitating help-seeking in their peers. For this reason, there have been national and local awareness-raising programs associated with the roll-out of headspace services.
A recent report on young people’s awareness of headspace in a 2008 national survey of Australian young people indicated that in the 2 years after its launch, with 12 centres in operation, headspace had established some awareness among young people, especially in areas where its services operate (Jorm, 2009). However, this study also found that young people who have the greatest need for these services, namely those with elevated psychological distress, were not more aware of these services. Since that report, headspace has increased its national coverage, with the total number of centres increasing to 30. In addition, the 2011–2012 federal budget has also included further funding to establish more headspace centres. In view of these developments, it is important to assess whether young people’s awareness of headspace has changed, not just generally about headspace being a mental health organization, but also as a service for themselves and their peers with mental health problems.
Based on a 2011 national survey of mental health literacy and stigma in young people aged 15 to 25, this paper presents data on young people’s spontaneous recall of headspace as an organization related to mental health problems and their specific recognition of it when prompted. Data are also presented on their spontaneous mention of headspace as a service they would go to for help, or suggest that a peer seek help from, for mental health problems. Finally, predictors of headspace awareness are examined to determine which subgroups of young people should be targeted in future awareness campaigns.
Methods
Participants
The survey involved computer-assisted telephone interviews with 3021 young people aged between 15 and 25. The survey was carried out by the survey company Social Research Centre. The sample was contacted by random-digit dialling of both landlines and mobile phones covering the whole of Australia from January to May 2011. Up to six calls were made to establish contact. The response rate was 47.9%, defined as completed interviews (3021) out of sample members who could be contacted and were confirmed as in scope (6306). Interviewers ascertained whether there were residents in the household within the age range and, if there were multiple, selected one for interview using the nearest-birthday method.
Survey interview
The interview was based on a case vignette of a young person (John or Jenny) with a mental disorder. On a random basis, respondents were read one of six vignettes – depression, depression with suicidal thoughts, psychosis (early schizophrenia), social phobia, depression with alcohol abuse, or PTSD – portraying a person aged 15 years (for participants aged 15–17 years) or 21 years (for participants aged 18–25 years) of the same sex as the respondent (for more details see Reavley and Jorm, 2011, in press).
All respondents were then asked a series of questions that assessed sociodemographic characteristics, mental health literacy, stigma, exposure to mental disorders, beliefs about interventions and prevention for the mental disorder in the vignette, psychological distress (using the K6 screening scale; Kessler et al., 2002), and exposure to mental health organizations and media campaigns.
Awareness of headspace
Awareness of headspace was assessed in three ways: (i) its recall and recognition as a mental health organization; (ii) its spontaneous mention as a service that respondents would seek help from for a mental health problem (i.e. help-seeking intention); and (iii) its spontaneous mention as a service they would suggest to a peer they are helping with a mental health problem (i.e. first aid intention). Responses were coded with a ‘yes’ = 1 if they included a specific mention of ‘headspace’ or ‘no’ = 0 if there was no mention of ‘headspace’. Responses were also searched to pick up any other name associated with specific headspace centres that might have been mentioned, using the search terms: clock, work, top, end, riverina, gate, way, oasis, jigsaw, shop, front, corner, second, story. This resulted in two responses being coded as 1, namely ‘Clock work’ and ‘Second story’, which refer to specific centres at Geelong, Victoria, and Elizabeth, South Australia, respectively.
To assess recall of mental health organizations, respondents were asked: “Which organizations related to mental health problems, if any, can you think of?” If headspace was not spontaneously recalled, respondents were tested for recognition by asking: “Have you heard of headspace – Australia’s national youth mental health foundation?” Because these recognition questions could elicit false-positive responses, a question was also asked about a fictitious organization: “Have you heard of the Mellow Yellow Institute?” Responses to this question were used to gauge false-positive rates.
To assess their help-seeking intentions, respondents were asked: “If you had a problem right now like (John/Jenny), would you go for help? Where would you go?”
To assess respondents’ spontaneously reported first aid intentions, they were asked: “Imagine John/Jenny is someone you have known for a long time and care about. You want to help him/her. What would you do?”
Potential predictors of first aid intentions and beliefs
Information about respondent sex and age was collected as part of the interview. Respondent age was coded into two categories: adolescents (aged 15–17) or young adults (aged 18–25). To measure psychological distress, participants were given the K6 scale, with questions asked in relation to “the one month in the past 12 months when you were most depressed, anxious, or emotionally stressed” (Kessler et al., 2002).
Because headspace services are offered only in some areas, respondents were classified as living in or outside a headspace area based on their postcode. If a respondent’s postcode was in the same Statistical Local Area (Australian Bureau of Statistics, 2007) as the postcode of a headspace service, they were coded as living in a headspace area.
Statistical analyses
The data was first analysed using per cent frequencies for the spontaneous mention of headspace as a mental health organization and as a service respondents would go to or refer a peer to in the context of a mental health problem. These data were compared with other organizations or services that were mentioned by at least 1% of the total sample. This data was analysed for the whole sample and for subgroups based on whether the respondent lived in a headspace area. We also examined respondents’ recall or recognition of headspace and the fictitious Mellow Yellow Institute using per cent frequencies and 95% confidence intervals (CIs) for the same subgroups. Finally, predictors of awareness of headspace were examined using a multiple logistic regression, including age, sex, psychological distress, and residence in a headspace area as predictors. Sex (male as reference category) and residence in a headspace area (not in headspace area as reference category) were dichotomous predictors, whereas age in years and psychological distress were continuous variables. Analyses used sample weights that took account of number of in-scope persons in the household, phone type (mobile or landline), age group, sex and geographic location.
Ethics
Oral consent was obtained from all respondents before commencing the interview. Respondents aged below 18 could only commence their interviews after their parents provided oral consent. This study has been approved by the University of Melbourne Human Research Ethics Committee.
Results
Of the 3021 respondents, 14.5% (n = 438) lived in a headspace area. When asked about their awareness of mental health organizations, only 507 nominated at least one organization. In contrast, 1943 nominated at least one person or service they would go to for help if they had a mental health problem, and 3005 mentioned at least one action they would take to help a peer.
Figure 1 shows the organizations and services spontaneously mentioned by at least 1% of the total sample, as well as headspace which was mentioned by less than 1%. A local or community health service (including GP) and helplines were most frequently mentioned as mental health organizations, whereas headspace was only mentioned by three respondents – all females, two aged 18–25 years, and two not living in a headspace area. GPs/doctors or counsellors were the most commonly mentioned professionals whom respondents would go to, or refer a peer to, for a mental health problem. Only 18 respondents mentioned that they would go to headspace, nine of whom lived in a headspace area (2.35%; five males and one female aged 15–17; one male and two females aged 18–25) and nine outside (0.27%; one male and one female aged 15–17; four males and three females aged 18–25). Only five respondents (all aged 18–25) mentioned that they would refer a peer to headspace, two of whom lived in a headspace area (0.56%; both females) and three outside (0.07%; two males and one female).
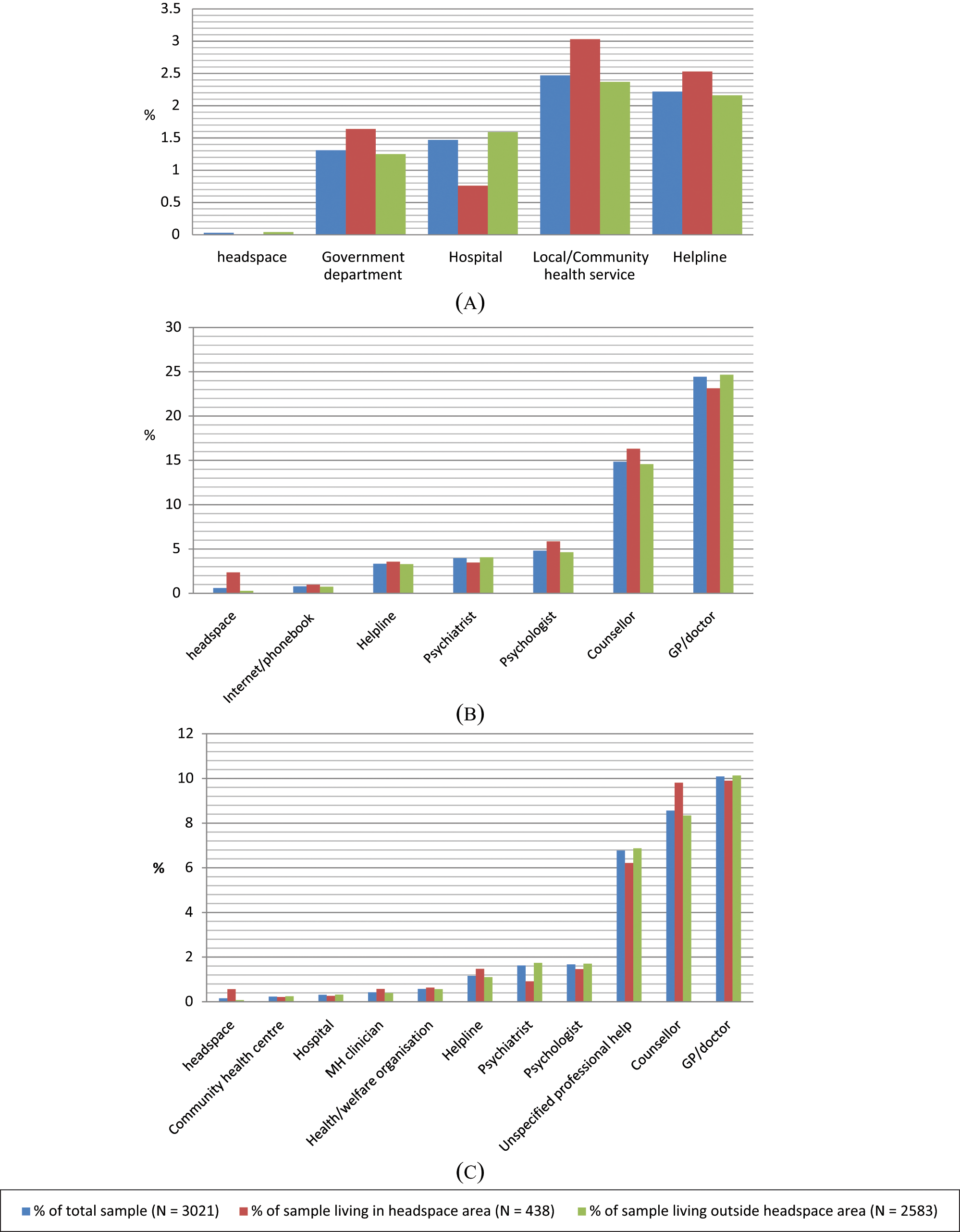
Young people’s spontaneous mentions of (a) mental health organizations they could think of, (b) services they would seek help from, and (c) services they would refer a peer to for a mental health problem: % frequencies.
Table 1 shows the per cent frequencies and 95% CI of respondents within each age, sex, and headspace residence subgroup who recognized or recalled headspace and the fictitious Mellow Yellow Institute as a mental health organization (given as an estimate of false-positive responses). Recognition of headspace exceeded the fictitious one for the whole sample and all subgroups.
Young people’s recognition or recall of headspace and the fictitious Mellow Yellow Institute: % frequencies and 95% confidence intervals (CI)
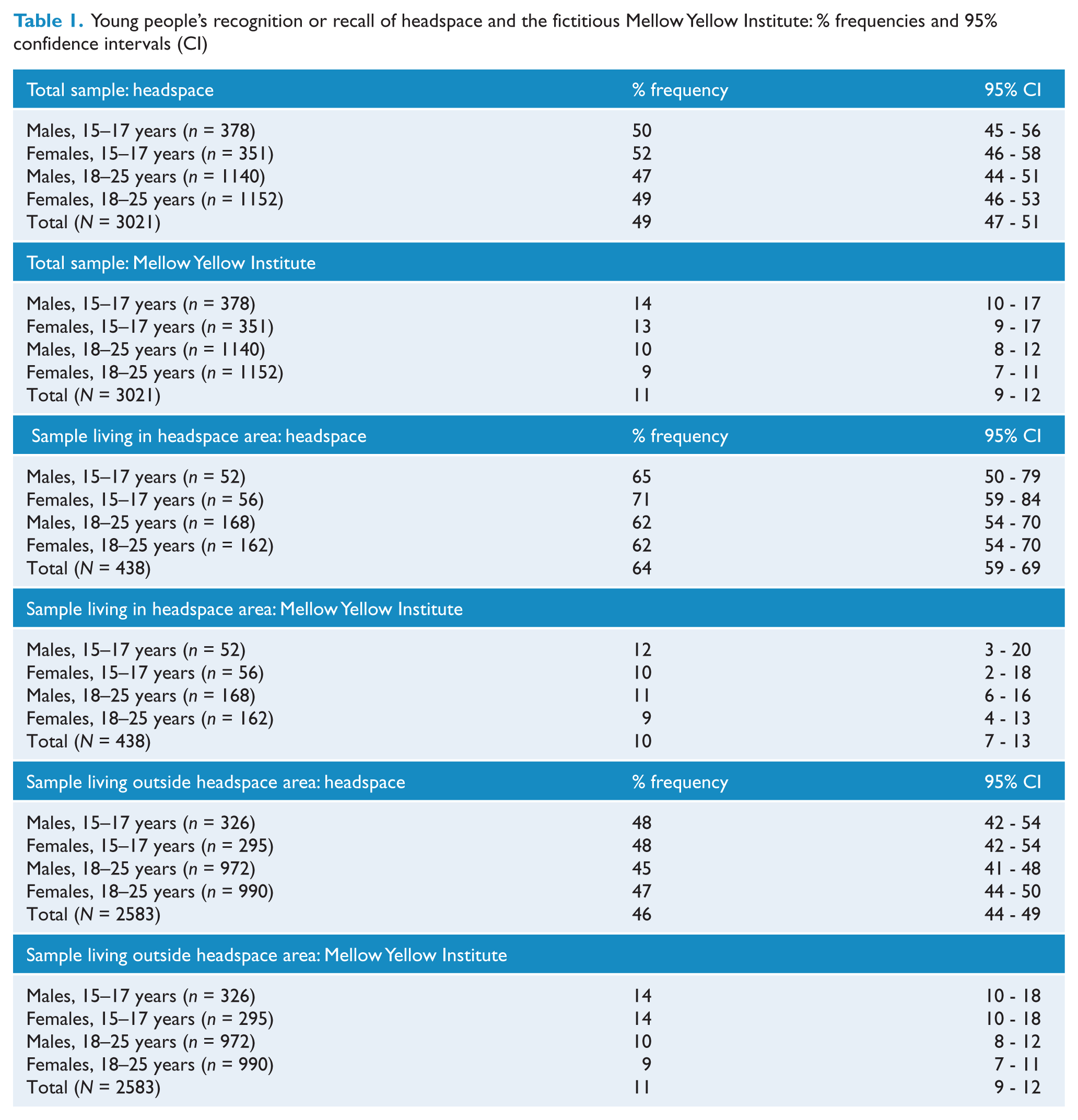
Table 2 shows the results of logistic regression analyses looking at participant characteristics that predict recognition or recall of headspace and the fictitious Mellow Yellow Institute. Recall or recognition of headspace decreased with age, but there was no gender difference in awareness. Awareness of headspace was greater in young people who lived in areas with headspace services, but was not associated with psychological distress. Increased (erroneous) recognition of Mellow Yellow was associated with higher levels of recent psychological distress and younger age, but no other significant predictors were found. Given that spontaneous mentions of headspace in the contexts of help-seeking and providing first aid to a peer were so infrequent, regression analyses were not conducted on these outcomes.
Predictors of recall or recognition of headspace and the fictitious Mellow Yellow Institute: odds ratios, 95% CIs and p-values (significant odds ratios are shown in bold)
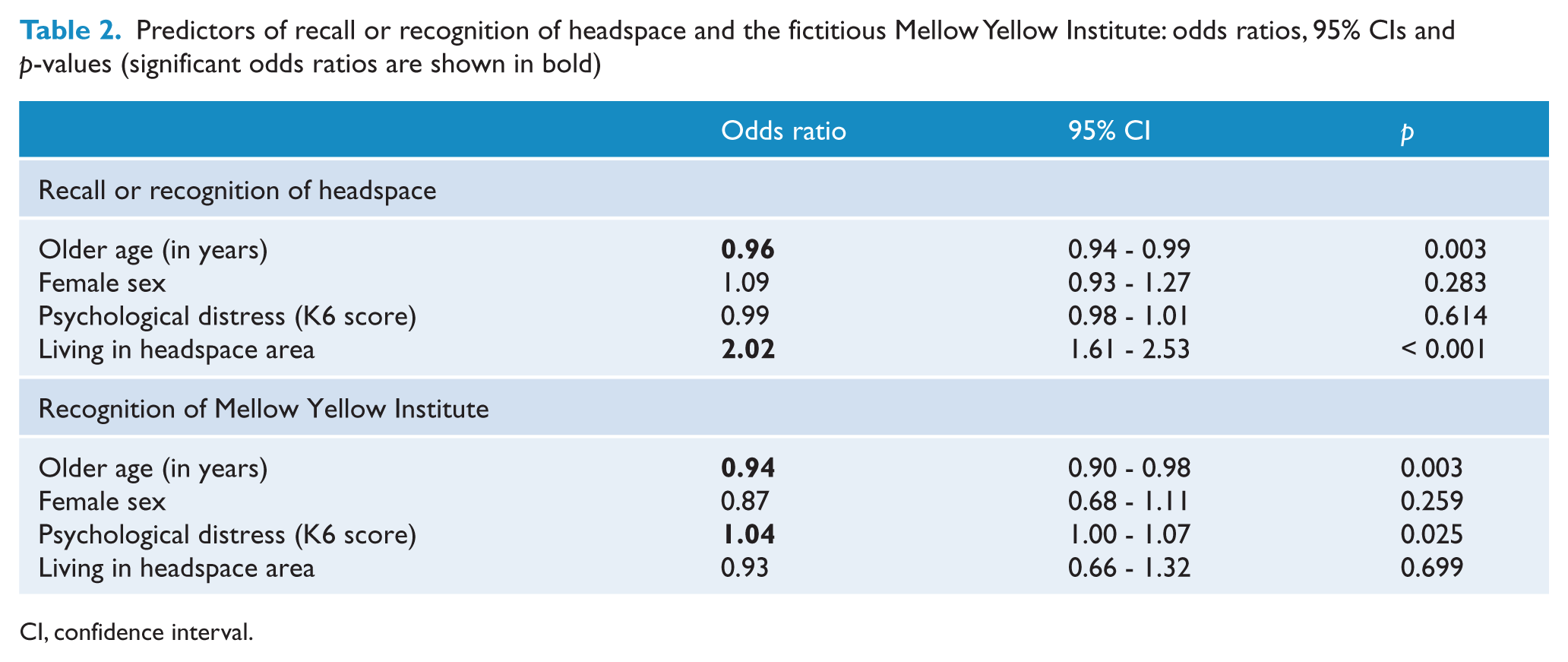
CI, confidence interval.
Discussion
Data from this national survey indicate that despite having 30 headspace centres now covering areas in which almost 15% of the survey sample lived, spontaneous recall or mentions of headspace as a mental health organization, as a service to go to, or a service to refer a friend to for a mental health problem, remain very low. Nonetheless, when prompted, almost half of the sample recognized headspace, especially those who lived in a headspace area.
The extremely low rate of spontaneous mentions of headspace as a mental health organization in this survey is in contrast to the 2.3% observed in a similar 2008 survey (Jorm, 2009). In particular, this is contrary to expectations that awareness of headspace would increase given that the number of centres had increased from 12 in 2008 to 30 in the 2011 survey. A few differences in the samples are worth noting. Firstly, the 2008 sample is a follow-up subsample from a national survey conducted in 2006, who had agreed to be re-contacted and actually completed the follow-up interview. Hence it is possible that they are less representative of Australian young people compared to the 2011 sample in the current study. In particular, young people with better mental health literacy or a greater interest in or exposure to mental health may be over-represented in the subsample. However, rates of spontaneous recall of a local clinic (2.3%) and phone helpline (unspecified; 2.1%) in the 2008 sample (Jorm, 2009) were very similar to parallel categories in the current study, namely local/community health service (2.47%) and helpline (2.22%).
The low rates of recall of headspace as a mental health organization are consistent with the low rates of nominating headspace as a service to which respondents would go for help or refer a friend in the context of a mental health problem. These low rates are in contrast to more frequent mentions of counsellors and GPs/doctors, and even helplines, psychiatrists and psychologists, which suggest that young people are aware of and have the intention to seek help from these more generic and not youth-specific services. Given that headspace is intentionally set up to cater to the specific needs of young people, it is unfortunate that its unique purpose does not seem to have effectively reached its target group in the community. It is noteworthy that amongst the few respondents who spontaneously nominated headspace as a service for themselves or a peer in the context of mental health problems, there seemed to be more young adults (aged 18–25) than adolescents (aged 15–17). This is consistent with prior research indicating that older age is associated with more professional help-seeking intentions (Jorm et al., 2007b), actual professional help-seeking behaviours (Reavley et al., 2011), and first aid intentions (Jorm et al., 2007a) and actual actions (Yap et al., 2011) involving encouraging or facilitating professional help-seeking.
In contrast to findings involving spontaneous recall of headspace, rates of recognition or recall of headspace as a mental health organization were much higher. This is true especially in areas where its services are operating, which reflects the fact that headspace promotion has had regional as well as national coverage. While this is encouraging, it remains of concern that elevated psychological distress was not associated with better recognition or recall of headspace, which replicates previous findings (Jorm, 2009). It is possible that despite elevated distress, these respondents were not yet at the stage where they are thinking about seeking help or aware of where help might be. Factors reflecting poor mental health literacy, such as lack of recognition of symptoms (Wright et al., 2007) and belief in self-reliance (Jorm et al., 2006) may contribute to this delay in help-seeking. Given that headspace provides services to the sub-group with mental health problems, awareness of these services needs to be greatest for those in need. As noted previously, some of the marketing of headspace has not explicitly indicated that the organization offers services for people with mental disorders (Jorm, 2009). The current findings suggest that future promotion of headspace may need to consider providing more explicit messages of its services to more effectively raise the awareness of young people with mental health problems that headspace is a good first port of call for them and their peers.
Although this study found that younger respondents had better recognition or recall of headspace as a mental health organization, findings involving spontaneous mentions of headspace indicate that this is largely attributable to prompted recognition. Furthermore, given that younger respondents were also more likely to wrongly recognize the fictitious Mellow Yellow Institute, which may simply indicate a general tendency for a higher false-positive recognition rate in younger respondents, the finding involving their better recognition of headspace needs to be interpreted with caution. Ironically, although young people with elevated psychological distress were not more aware of headspace, they were more susceptible to false-positive recognition of the fictitious organization. The reasons behind this surprising finding are unclear, but the possibility of a Type I error cannot be dismissed, especially given that the p-value is greater than 0.01, unlike the other three significant findings.
Strengths and limitations
This national survey is the first to examine young people’s awareness of headspace as a mental health organization and as a service to seek help from or refer a peer to for a mental health problem, using data from a large national sample of Australian youth. Nonetheless, the study has some limitations. Firstly, it was not possible to ascertain whether awareness of headspace accurately reflects young people’s actual help-seeking or first aid behaviours in the context of mental health problems in themselves or a peer. However, there is evidence from a 2-year follow-up of the 2006 sample showing that professional help-seeking intentions and first aid intentions that involved encouraging or facilitating professional help-seeking predicted subsequent actions (Reavley et al., 2011; Yap et al., 2011). Furthermore, an underlying assumption of this research is that awareness and in turn access of headspace services will benefit the mental health of the young person and will outweigh any possible negative effects such as stigma, but this has not yet been demonstrated. Nonetheless, an initial independent evaluation of headspace has reported some improvements in young people’s mental health, social well-being, and vocational engagement (Muir et al., 2009).
Conclusions
Findings from this national survey indicate that awareness of headspace amongst Australian young people remains inadequate. Given that help-seeking and first aid intentions have been found to predict subsequent help-seeking (Reavley et al., 2011) and first aid behaviours (Yap et al., 2011), it is concerning that so few young people spontaneously indicated an intention to seek help from headspace for themselves or their peers in the context of a mental health problem. It is also of particular concern that young people with elevated psychological distress, who are in most need of, and are the primary target sub-group for, headspace services, were not more aware of headspace. Future promotion of headspace needs to consider targeting this sub-group more explicitly to ensure that these young people are effectively reached by their services.
Footnotes
Funding
Funding for the study was provided by the Commonwealth Department of Health and Ageing and the NHMRC Australia Fellowship, awarded to Professor Jorm.
Declaration of Interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.