
Abstract
Introduction
Beyondblue: the national depression initiative was established in 2000 to address issues associated with depression, anxiety and related disorders across Australia (beyondblue, 2011a). Its initial focus was on promoting awareness and an effective response to depression in the community, but in more recent years it has increased its efforts targeting anxiety disorders. There is evidence that mental health literacy in Australia, especially depression literacy, has improved in the past decade (Jorm et al., 2005a). Based on evidence from various national surveys demonstrating associations between beyondblue awareness and better mental health literacy in the general population (Jorm et al., 2005b) and in young people (Morgan and Jorm, 2007), it seems that some of the improvement in depression literacy may be attributed to the efforts of beyondblue.
However, given beyondblue’s initial focus on depression, most evaluations of beyondblue to date have focused solely on depression literacy (Jorm et al., 2005a, 2005b; Morgan and Jorm, 2007). Hence little is known about the association of beyondblue awareness with anxiety literacy (i.e. literacy about anxiety disorders) and whether these associations are specific to depression and anxiety disorders, or generalizable to other disorders which are not its focus, e.g. psychosis. Moreover, while there is evidence indicating the associations of beyondblue awareness with recognition or accurate labelling of mental disorders (Wright and Jorm, 2009), stigma (Jorm et al., 2006), appreciation of its impact on functioning (Highet et al., 2006) and treatment beliefs (Morgan and Jorm, 2007), there is limited evidence about whether beyondblue awareness is related to first-aid skills.
Using data from a 2011 national survey of mental health literacy and stigma in young people aged 15–25, this paper sought to address some of these gaps in the evidence. Specifically, we present data on young people’s awareness of beyondblue as an organization related to mental health problems and three indices of mental health literacy: recognition of the disorder, quality of beliefs about the helpfulness or harmfulness of various interventions and first-aid actions for two depression vignettes (depression alone and depression with suicidal thoughts) and two anxiety vignettes [social phobia and post-traumatic stress disorder (PTSD)]. To assess whether the association between beyondblue awareness and mental health literacy is specific to such disorders, we also examined these indices for a psychosis vignette. Health professionals’ ratings of various treatments and first-aid actions obtained in a previous survey (Lubman et al., 2007a) were used as a standard by which to determine the quality of young people’s beliefs.
Methods
Participants
The youth survey involved computer-assisted telephone interviews with 3021 young people aged between 15 and 25. The survey was carried out by the survey company Social Research Centre, North Melbourne, Australia. The sample was contacted by random-digit dialling of both landlines and mobile phones covering the whole of Australia from January to May 2011. Up to six calls were made to establish contact. The response rate was 47.9%, defined as completed interviews (3021) out of sample members who could be contacted and were confirmed as in scope (6306). Interviewers ascertained whether there were residents in the household within the age range and, if there were multiple, selected one for interview using the nearest birthday method (Reavley and Jorm, 2011a; Reavley and Jorm, 2011b).
In the professional survey, clinicians were sent a questionnaire based on a vignette describing psychosis, depression, depression with alcohol misuse or social phobia (Lubman et al., 2007a). In 2006, surveys were posted to 428 psychiatrists listed in the Medicare provider file (Medicare is Australia’s national, government-funded health insurance programme), a random sample of 500 general practitioners (GPs) listed in the file, 407 Australian members of the Australian and New Zealand College of Mental Health Nurses and a random sample of 500 psychologists listed in the Victorian Psychologists Registration Board’s online database of registered psychologists. Surveys were completed anonymously and separate response cards with identification numbers were used to determine participation or refusal. GPs, psychiatrists and psychologists were sent one reminder letter to encourage participation. Completed surveys were received from 105 GPs (21% response rate), 155 psychiatrists (37%), 106 mental health nurses (26%) and 183 psychologists (41%).
Survey questions
The youth interview was based on a case vignette of a young person (John or Jenny) with a mental disorder. On a random basis, respondents were read one of six vignettes – depression, depression with suicidal thoughts, psychosis (early schizophrenia), social phobia, depression with alcohol abuse or PTSD – portraying a person aged 15 years (for participants aged 15–17 years) or 21 years (for participants aged 18–25 years) of the same sex as the respondent (Reavley and Jorm, 2011a). The vignettes were developed from previous work (Caldwell and Jorm, 2000; Jorm et al., 1997; Wright et al., 2005), reviewed by clinical researchers for face validity and conformity with the Diagnostic and Statistical Manual of Mental Disorders, 4th Edition (DSM-IV; American Psychiatric Association, 1994) and the International Classification of Diseases, 10th edition (ICD-10) diagnostic criteria, and validated with a survey of psychiatrists and psychologists (Lubman et al., 2007b; Wright and Jorm, 2009).
All respondents were then asked a series of questions that assessed sociodemographic characteristics, mental health literacy, stigma, exposure to mental disorders, beliefs about interventions and prevention for the mental disorder in the vignette, psychological distress [using the K6 screening scale (Kessler et al., 2002)] and exposure to mental health media campaigns.
The professional survey asked similar questions about mental health literacy but included four disorders which portrayed only male characters due to the small sample: depression, psychosis, social phobia and depression with alcohol abuse. Professionals were randomly given a vignette describing a 15- or 21-year-old.
This study focused on recognition of the disorder in the vignette, beliefs about the helpfulness of different interventions for the young person and a close friend or family with a similar problem to the vignette character, and exposure to beyondblue, so these are described in detail here. The depression with alcohol abuse vignette was not included in this paper because it comprises two co-morbid disorders whereas each of the other five vignettes of interest in this paper represents a single diagnostic group.
Recognition of the disorder portrayed in the vignette
In the youth survey, description of the vignette was followed by an open-ended question asking: ‘What, if anything, do you think is wrong with John (male version)/Jenny (female version)?’ Interviewers recorded verbatim responses according to pre-coded response categories (depression, schizophrenia, psychosis, mental illness, stress, nervous breakdown, psychological/ mental/emotional problem, has a problem, cancer, nothing, don’t know) derived from a content analysis of responses to the same questions in earlier surveys (Jorm et al., 1997; Wright et al., 2005).
A content analysis of responses that did not fit these pre-coded categories led to post-coding of 53 other categories, which have been detailed elsewhere (Reavley and Jorm, 2011a). Of interest for this paper, these included the most accurate responses for the anxiety disorder vignettes: anxiety/anxious, social anxiety/social phobia/anxiety disorder, post-traumatic stress/stress disorder/syndrome and trauma/traumatized/adverse life event.
Accurate labelling was defined as those labels that approximated the DSM-IV diagnostic label (American Psychiatric Association, 1994) upon which the vignettes were based and validated (Jorm et al., 1997; Wright et al., 2005). However, given the low rates of using the exact DSM-IV labels ‘social phobia’ and ‘PTSD’, we expanded our definition of ‘accurate’ label for social phobia to include any mention of anxiety, anxious, social anxiety/phobia and anxiety disorder, and, for PTSD, any mention of post-traumatic stress/stress disorder/syndrome, trauma, traumatized and adverse life event. ‘Depression’ or ‘depressed’ were the only accurate labels accepted for both depression vignettes. Mentions of psychosis/psychotic, schizophrenia/schizophrenic were accepted as accurate labels for the psychosis vignette.
Beliefs about interventions
In both the youth and professional surveys, we assessed the following interventions: consulting with a GP or family doctor, a teacher or lecturer (the former for 15–17- year-old respondents and the latter for 18–25-year-old respondents), a counsellor, a telephone counselling service such as Kids Helpline or Lifeline (the service varied by age group), a psychologist, a psychiatrist, other mental health professionals (occupational therapist, social worker or mental health nurse), a close family member or a close friend; dealing with the problem on their own; taking vitamins, St John’s wort, antidepressants, tranquillizers, antipsychotics, or sleeping pills; becoming more physically active; getting relaxation training; practising meditation; having regular massages; getting acupuncture; getting up early each morning and going out in the sunlight; receiving counselling by a health professional, receiving cognitive behavioural therapy; searching a website for information about the problem; reading a self-help book on the problem; joining a support group of people with similar problems; going to a local mental health service; being admitted to a psychiatric ward of a hospital; using alcohol to relax; smoking cigarettes to relax; using marijuana to relax; cutting down on the use of alcohol; cutting down on smoking cigarettes; and cutting down on use of marijuana. These interventions were selected on the basis of published surveys (Jorm et al., 1997; Wright et al., 2005), but supplemented by new complementary and self-help ones that have some evidence to support them (Jorm et al., 2002, 2004). Youth and professional respondents assessed interventions as ‘helpful’, ‘harmful’, ‘neither’, ‘depends’ or ‘don’t know’. Endorsement of an intervention as helpful was scored for responses of ‘helpful’ = 1 and all other responses = 0, whereas endorsement as harmful was scored as ‘harmful’ = 1 and all other responses = 0.
First-aid beliefs
Professionals were asked whether it would be helpful if a friend or family member were to do various first-aid actions, and youths were asked whether it would be helpful if they provided the first-aid response to someone they knew and cared about. The first-aid actions were:
Listen to their problems in an understanding way;
Talk to them firmly about getting their act together;
Suggest they seek professional help;
Make an appointment for them to see a GP;
Ask them whether they are feeling suicidal;
Suggest they have a few drinks to forget their troubles;
Rally friends to cheer them up;
Ignore them until they get over it;
Keep them busy to keep their mind off problems;
Encourage them to become more physically active.
Endorsement of a first-aid action as helpful was scored for responses of ‘helpful’ = 1 and all other responses = 0; whereas endorsement as harmful was scored as ‘harmful’ = 1 and all other responses = 0.
Beyondblue awareness
To assess awareness of beyondblue, youths were first asked: ‘Which organizations related to mental health problems, if any, can you think of? If beyondblue was not spontaneously recalled, respondents were prompted for recognition by asking: ‘Have you heard of beyondblue: the national depression initiative?’ Spontaneous nomination of beyondblue and ‘yes’ responses to the recognition question were coded as 1, and ‘no’, ‘don’t know’ or ‘refused’ responses were coded as 0. Beyondblue recognition or recall was coded as 1 if the respondent either spontaneously recalled beyondblue or responded ‘yes’ on prompting.
Finally, given that age, sex and personal exposure to mental disorders have been found to be associated with mental health literacy (Jorm et al., 2007b, 2008a; Yap et al., 2011) and beyondblue awareness (Jorm and Wright 2008; Wright and Jorm, 2009) youths were asked a range of questions to ascertain this information for use as covariates in analyses. To assess their exposure to mental disorders, respondents were asked: ‘Has anyone in your family or close circle of friends ever had a problem similar to John’s/Jenny’s?’; ‘Have they received professional help or treatment for these problems?’; ‘Have you ever had a problem similar to John’s/Jenny’s?’; and ‘Have you received any professional help or treatment for these problems?’ All responses were coded as yes = 1 and no = 0, and were indices of lifetime exposure to mental health problems in family or friends, personal experience of mental health problems, exposure to friends or family who had received professional help and having received professional help personally. The professional help variables were coded so that no mental health problem or no treatment was coded as 0.
Scoring of quality of beliefs about interventions and first-aid actions
To evaluate the quality of youths’ beliefs about the helpfulness of various interventions and first-aid actions, their beliefs were scored against professionals’ beliefs as a measure of the degree of agreement. Given that the professional survey did not include the depression with suicidal thoughts and PTSD vignettes, the associations between beyondblue awareness and the quality of young people’s beliefs could only be evaluated for three vignettes, namely depression, social phobia and psychosis. Firstly, for each vignette we selected interventions and first-aid actions for which the mean agreement about the helpfulness or harmfulness across the four professions was 70% or higher. Professionally rated helpful interventions for depression included cutting down marijuana, cutting down alcohol, consulting a GP, consulting a psychologist and counselling. For social phobia, the list included consulting a psychologist, relaxation training, cutting down marijuana, cognitive behavioural therapy and cutting down alcohol. For psychosis, the list included consulting a psychiatrist, going to a local mental health service, consulting a GP, cutting down marijuana and cutting down alcohol (for the 15-year-old vignette) or antipsychotics (for the 21-year-old vignette).
Professionals also rated the following as harmful for all vignettes:
Using alcohol to relax;
Using cigarettes to relax;
Using marijuana to relax.
In addition, dealing with the problem on one’s own was rated as harmful specifically for psychosis.
For first-aid responses to the depression and psychosis vignettes, professionals rated listening in an understanding way, assessing for suicide risk, making a doctor’s appointment on the person’s behalf and suggesting professional help-seeking as helpful; and suggesting drinks, ignoring the person and talking firmly to the person as harmful. For social phobia, professionals rated listening in an understanding way and suggesting professional help-seeking as helpful; and suggesting drinks, ignoring the person and talking firmly to the person as harmful.
Youths’ quality of beliefs about interventions and first-aid actions were calculated by adding all professionally endorsed helpful and harmful ratings separately for each vignette and obtaining a percentage of agreement with professionals. Higher percentages indicate more agreement with professional views and are taken as an index of better mental health literacy about possible interventions for mental disorders.
Statistical analysis
Data on youths’ recognition are presented using percentage frequencies and 95% confidence intervals (CIs) to determine the rate of using the most accurate labels for each vignette. Data on the quality of youths’ beliefs about interventions and first-aid actions are presented using means, standard deviations and 95% CIs of the percent of agreement with professionals. These analyses used sample weights that took account of the number of in-scope persons in the household, phone type (mobile or landline), age group, sex and geographic location, and were conducted using Intercooled Stata 10 (StataCorp LP, College Station, Texas, USA).
To explore whether awareness of beyondblue predicted recognition of disorders, we conducted five binary logistic regressions, one for each vignette separately. In these regressions, the most accurate label was the dichotomous dependent variable. Age in years, sex, mental health problems in the respondent, mental health problems in a close friend or family, exposure to professional treatment for the respondent and for the friend or family member were entered as covariates in the first block, and beyondblue spontaneous recall and beyondblue recognition or recall were entered simultaneously in the second block. All predictors were dichotomous except for age in years, which was a continuous variable. Dichotomous predictors were dummy coded with males, no mental health problems in the self and other and no exposure to professional treatment in the self and other as reference groups.
To explore whether awareness of beyondblue predicted the quality of youths’ beliefs about interventions and first-aid actions, we conducted linear regressions separately for each vignette. In these regressions, the quality of belief variable was used as the ordinal dependent variable. The same predictors were entered in two blocks as described above. A regression analysis was conducted for each quality of belief score for each vignette, except for quality of beliefs about interventions for psychosis, which had a separate score for the 15-year-old versus the 21-year-old vignette. This resulted in a total of seven linear regressions, four for interventions and three for first-aid actions.
All regression analyses were conducted using PASW version 18 (SPSS Inc., Chicago, USA), and the p < 0.01 significance level was used to adjust for multiple analyses. Regression analyses were unweighted because the major weighting factors of age and sex were entered as covariates.
Ethics
Oral consent was obtained from all youth respondents before commencing the interview. Youth respondents aged below 18 could only commence their interviews after their parents provided oral consent. For the professional survey, consent was implied by return of the questionnaire. Both studies have been approved by the University of Melbourne Human Research Ethics Committee.
Results
Table 1 shows the descriptive statistics for all variables. Almost 35% of young people spontaneously nominated beyondblue as a mental health organization and another 35% recognized beyondblue when prompted. About 25% of youths reported having a similar problem to the vignette character, but less than 9% had received professional treatment. In contrast, more than half of respondents reported knowing someone who had experienced a mental health problem, with about 39% having received treatment. Accurate labelling of depression had the highest rates, followed by PTSD, psychosis and social phobia. Overall, youth beliefs about first-aid actions were more closely aligned to those of professionals than beliefs about interventions.
Descriptive statistics of all variables.
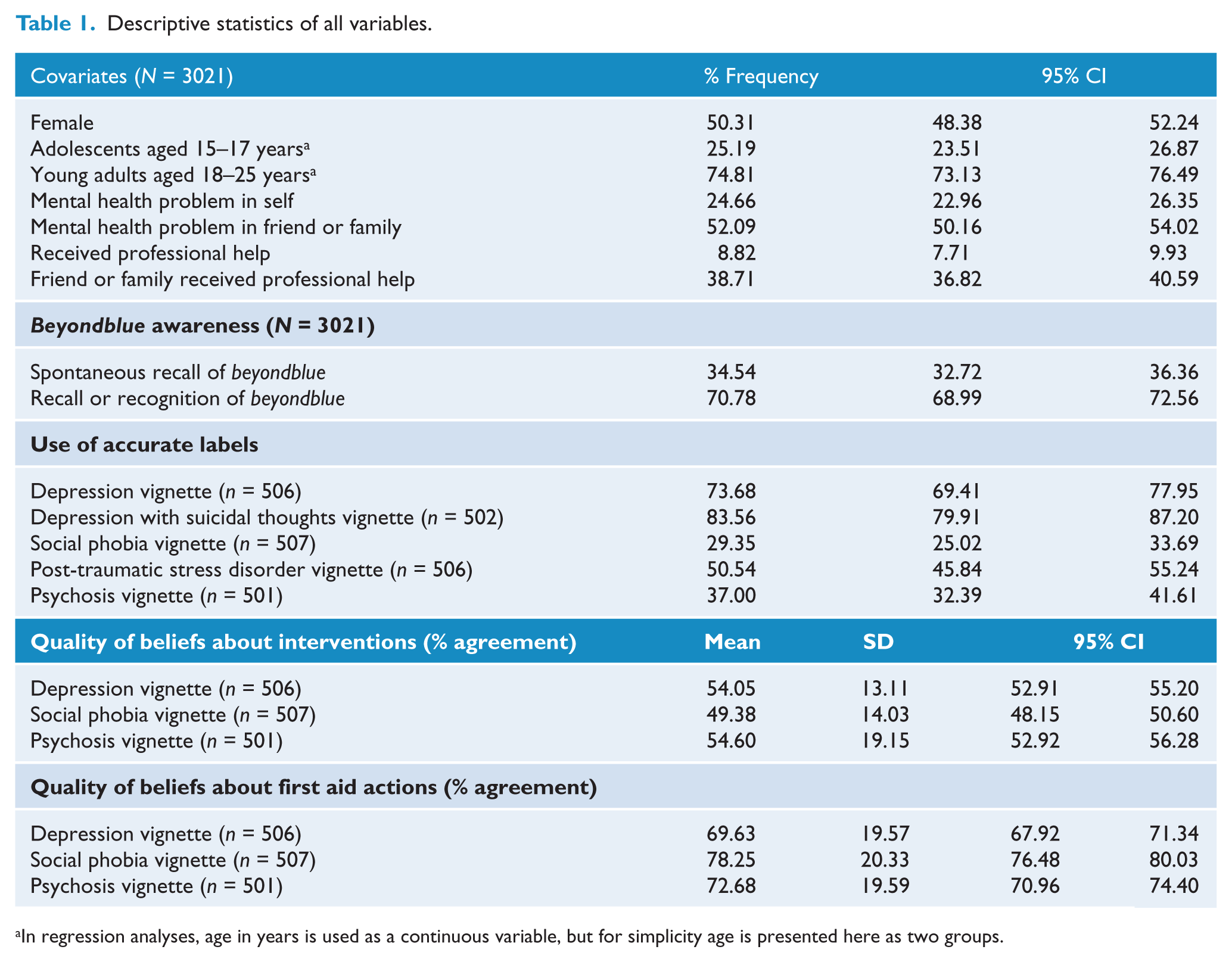
In regression analyses, age in years is used as a continuous variable, but for simplicity age is presented here as two groups.
As shown in Table 2, both beyondblue awareness variables significantly predicted accurate labelling of the depression vignette. Beyondblue recognition or recall predicted more accurate labelling of depression with suicidal thoughts or PTSD, while spontaneous recall of beyondblue predicted accurate labelling of psychosis; however, beyondblue awareness was unrelated to recognition of social phobia. Having received professional help for their own mental health problems predicted better recognition of the social phobia vignette. Older age was also associated with better recognition of psychosis.
Summary of logistic regressions predicting accurate labelling of disorders in each vignette with beyondblue awareness.
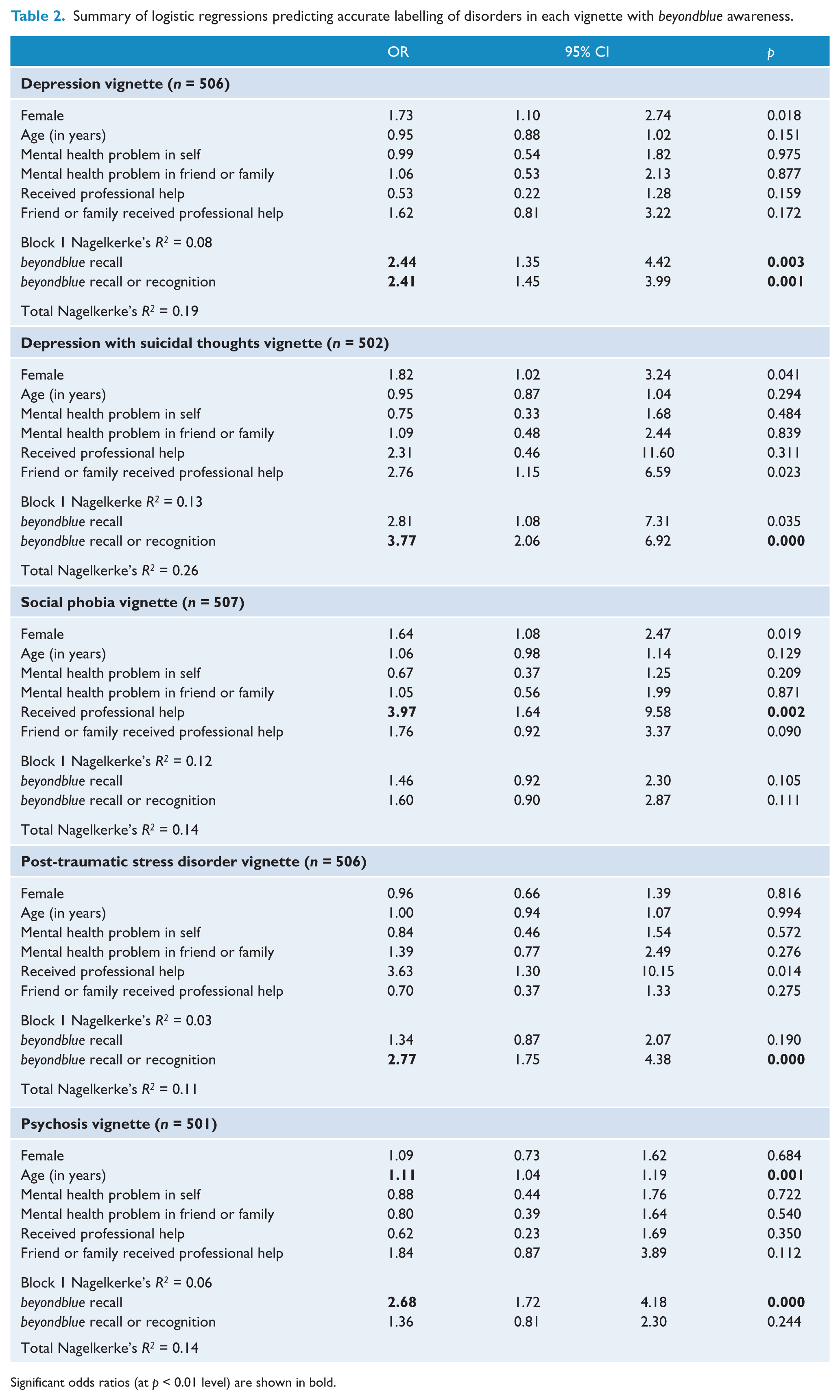
Significant odds ratios (at p < 0.01 level) are shown in bold.
As shown in Table 3, beyondblue awareness was largely unrelated to youths’ quality of beliefs about interventions, except for the psychosis vignette, where both beyondblue awareness variables were positively associated with quality of beliefs. Having had a similar problem to the character in the depression vignette was associated with beliefs that were more different from those of professionals, but knowing a friend or family member who had received professional help was associated with greater agreement with professional beliefs for both the depression and psychosis vignettes. Younger age was also associated with greater agreement with professional beliefs about interventions for psychosis.
Summary of linear regressions predicting quality of beliefs about interventions with beyondblue awareness.
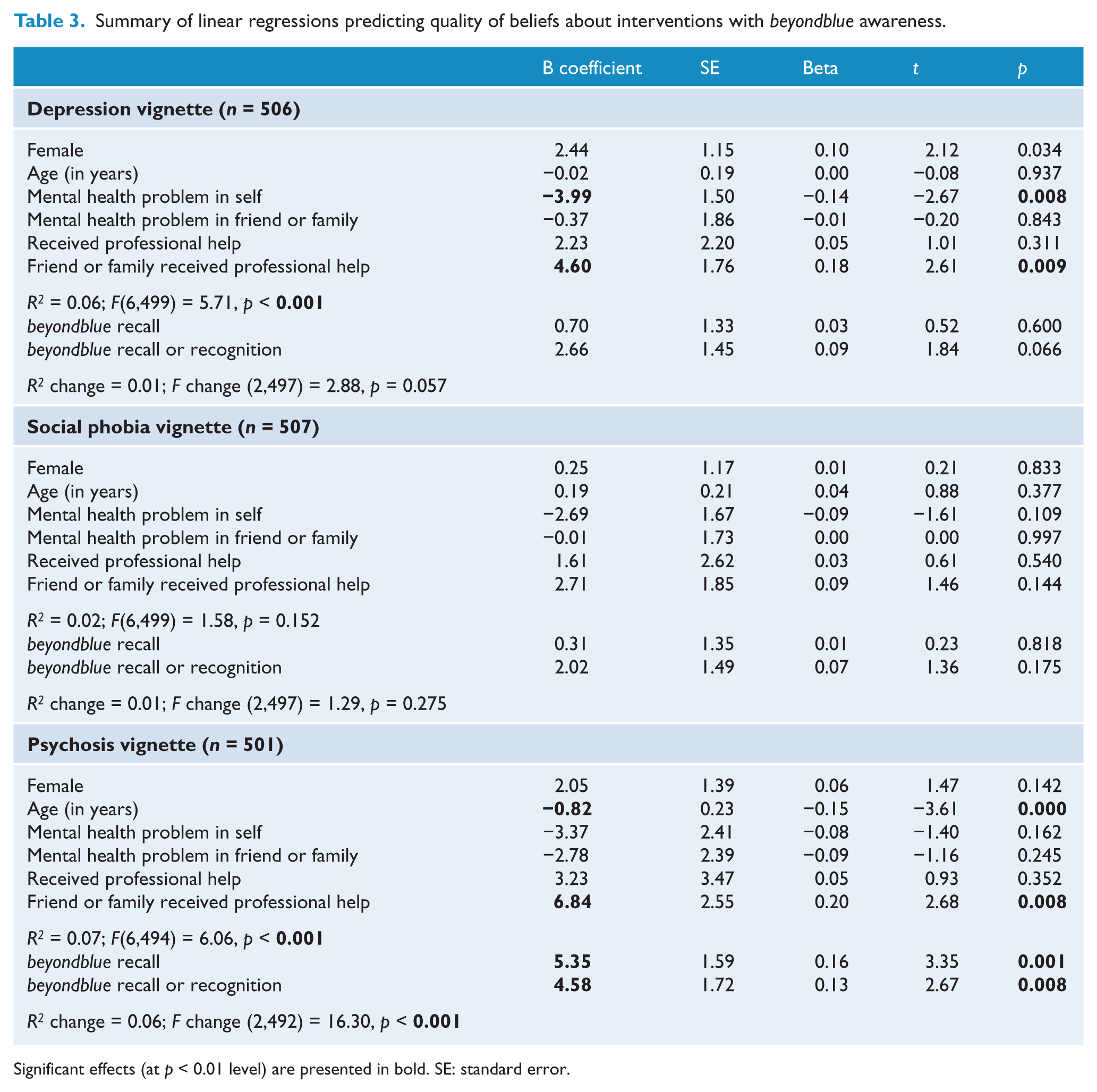
Significant effects (at p < 0.01 level) are presented in bold. SE: standard error.
In contrast, Table 4 shows that beyondblue awareness is related to the quality of youths’ beliefs about first-aid actions for all three vignettes. When considered as a ‘block’, both awareness variables predicted beliefs for social phobia, psychosis and depression that were more closely aligned to those of professionals. Being female was positively associated with quality of beliefs for the depression vignette. Having a friend or family member who had received professional help for a similar problem to the psychosis vignette character was positively associated with quality of beliefs.
Summary of linear regressions predicting quality of first-aid beliefs with beyondblue awareness.
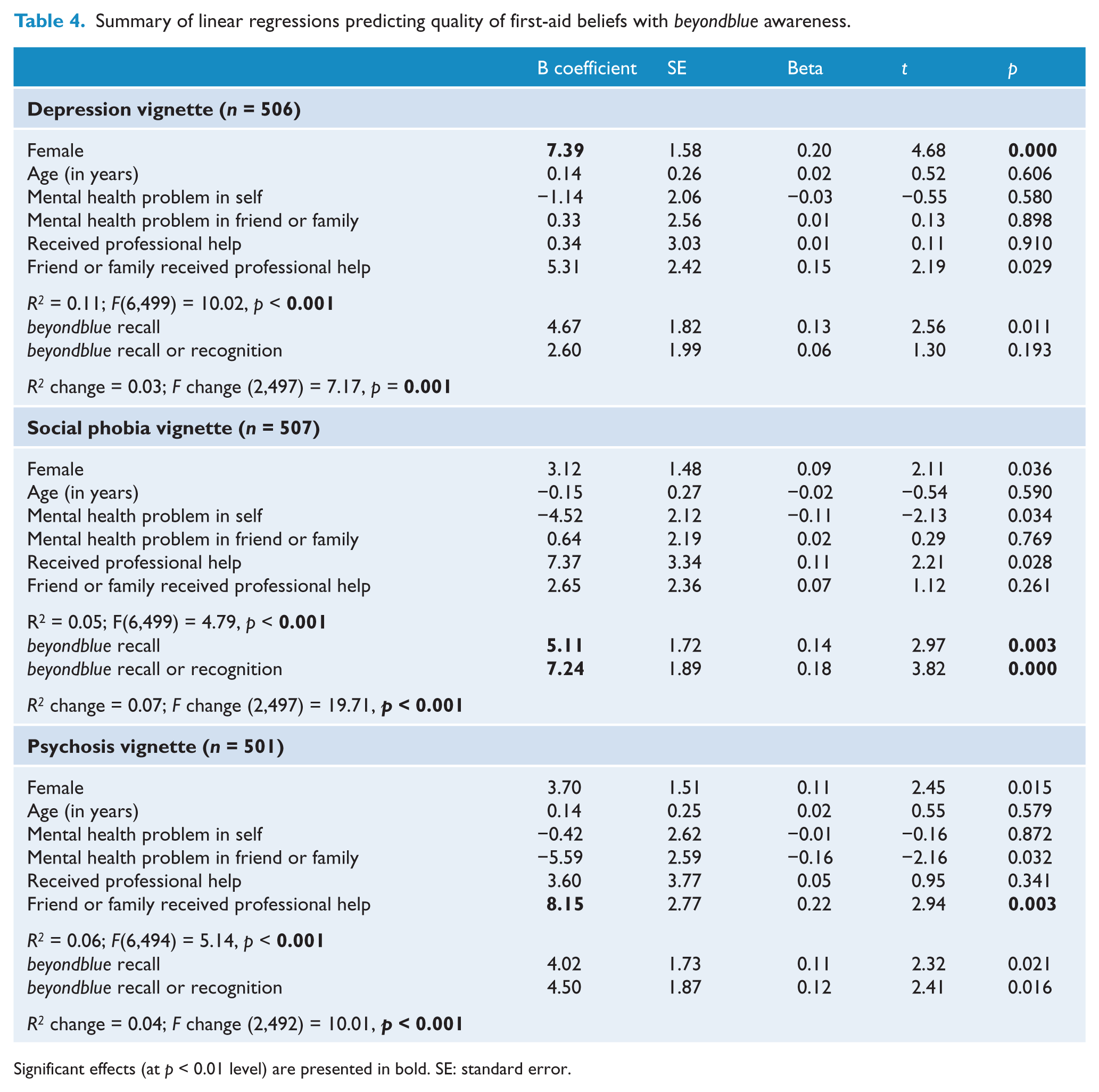
Significant effects (at p < 0.01 level) are presented in bold. SE: standard error.
Discussion
About 70% of young people were aware of beyondblue, half of whom spontaneously nominated it as a mental health organization without prompting. Beyondblue awareness was associated with better recognition of depression, PTSD and psychosis, but not social phobia. It was associated with beliefs about first aid that were more closely aligned to professional beliefs across all vignettes, but was related to quality of beliefs about interventions only for psychosis.
Beyondblue and depression literacy
Among youths presented with the depression vignettes, those who were aware of beyondblue had better recognition of the disorder portrayed and held beliefs about first-aid actions that were more closely aligned with those of professionals. The findings involving recognition are largely consistent with those from a similar 2006 national survey of young people aged 12–25 years (Wright and Jorm, 2009) involving the depression vignette, and replicate them in a new depression with suicidal thoughts vignette. Findings involving first-aid beliefs are novel and provide initial evidence of the association of beyondblue awareness with young people’s beliefs about what are helpful or harmful actions to take in response to someone they care about who is experiencing depression. These findings may in part reflect beyondblue’s ‘Look, listen, talk and seek help’ campaign which was first launched in 2009, and ongoing provision of related resources on the beyondblue (2011b) and youthbeyondblue (2011a) websites.
However, despite the range of resources readily available on the youthbeyondblue website which are specifically targeted to young people aged 12–25 years (youthbeyondblue, 2011b), beyondblue awareness was largely unrelated to quality of beliefs about depression treatment. These findings are somewhat consistent with an earlier report based on the 2006 survey (Morgan and Jorm, 2007), which found that beyondblue awareness was related to beliefs about the helpfulness of seeing a GP and reducing alcohol intake, but not the other three professionally endorsed helpful interventions (reducing marijuana consumption, seeing a psychologist and counselling). Harmfulness beliefs were not reported in the earlier study. Notably, youths with a personal history of mental health problems held beliefs that were more discrepant from professionals. Examination of the B coefficients in Table 3 revealed that this was largely due to the discrepant beliefs in those who had a problem but did not get help (a 3.99% difference). While there were also more discrepant beliefs in those who did get help, this difference is much smaller (a 1.76% difference).
This possibility is consistent with the finding that knowing a friend or family member who had received professional help was associated with beliefs about interventions that were more in agreement with professional beliefs.
Beyondblue and anxiety literacy
Among youths presented with the social phobia and PTSD vignettes, beyondblue awareness was associated with better recognition of PTSD but not social phobia, and beliefs about first aid for social phobia that were more closely aligned with professional beliefs. The non-significant association between beyondblue awareness and recognition of social phobia is contrary to the significant association reported in the 2006 survey (Wright and Jorm, 2009).
While this suggests that the previously reported association is not robust, the difference in findings could in part be due to methodological differences in the two surveys, including a younger age range in the 2006 survey (12–25 years versus 15–25 in the current study), and the definition of accurate label in the current study as comprising both the broad ‘anxiety/anxious’ and more accurate ‘anxiety disorder/social phobia/anxiety’ categories. Of note, the current study presents new data indicating that beyondblue awareness is associated with more accurate labelling of PTSD. Although beyondblue has provided community support training to local communities affected by various natural disasters (e.g. bush fires, flooding) (beyondblue, 2011c), these have been targeted to adults and promoted on the beyondblue website but not the youthbeyondblue website. Nonetheless, most mentions of beyondblue in terms of help-seeking options by respondents had been to beyondblue rather than youthbeyondblue specifically (data not shown), so it is possible that respondents who were aware of beyondblue may have been made more aware of PTSD-related issues through the main beyondblue website.
For youths presented with the social phobia vignette, beyondblue awareness was unrelated to quality of beliefs about interventions, but was associated with first-aid beliefs that were more closely aligned to professional views. These findings fill a gap in the literature on associations between beyondblue awareness and anxiety literacy, and indicate the need for future campaigns to focus on modifying beliefs about interventions for social phobia in addition to improving young people’s ability to recognize social phobia as a mental disorder (Wright and Jorm, 2009). In particular, consistent with earlier studies (Jorm et al., 2007a; Jorm and Wright, 2007), our findings indicate the need to target young people at a younger age, males and those who have not received professional help for mental health problems.
Beyondblue and mental health literacy – generalized effects?
Interestingly, although psychosis is not a focus of beyondblue, young people who were aware of beyondblue had better recognition of psychosis and beliefs about interventions (among youths aged 18–25 years) and first aid which were more closely aligned to professional views. These findings seem to suggest that associations between beyondblue awareness and mental health literacy may not be specific to disorders they focus on, but may generalize to mental illness more broadly. It is also possible in this cross-sectional study that youths with better mental health literacy are also more likely to be aware of mental health organizations such as beyondblue, suggesting that beyondblue awareness is not just a driver but may in fact be an effect (or indicator) of young people having better mental health literacy.
Nonetheless, the associations between beyondblue awareness and recognition seem to be stronger for the depression vignettes (accounting for 11% and 13% of the variance in accurate labelling for the depression and depression with suicidal thoughts vignettes respectively) compared to the PTSD and psychosis vignettes (7% each). While it is unsurprising that the associations are greater for depression, given beyondblue’s focus on depression since its inception, it is notable that its associations with recognition of anxiety disorders are only comparable to that of psychosis. In fact, as noted above, beyondblue awareness seems largely unrelated to social phobia recognition, despite it being one of the most common anxiety disorders among young people (Oakley Browne et al., 2006). In contrast, the associations of beyondblue awareness with first-aid beliefs were the strongest for social phobia, followed by psychosis and depression, although all associations were significant. This is unsurprising given that mental health first-aid guidelines are largely similar across mental disorders, with a few disorder-specific recommendations (Hart et al., 2009; Kingston et al., 2009; Langlands et al., 2008a, 2008b).
It is noteworthy that despite beyondblue’s efforts at improving community awareness about effective treatments and help seeking (beyondblue, 2011d, 2011e; Jorm et al., 2009; Purcell et al., 2010; Reavley et al., 2010), beyondblue awareness was largely unrelated to young people’s quality of beliefs about interventions, except for the psychosis vignette. Nonetheless, young people who had experienced a problem similar to the depression vignette character had beliefs about depression interventions that were more different to those of professionals. In addition, knowing a friend or family member who had received professional help seemed to be an important predictor of having beliefs that were more closely aligned to those of professionals, especially for the depression and psychosis vignettes. For the psychosis vignette, younger respondents were more likely to have beliefs that were more similar to those of professionals. This may be due to young people’s low endorsement of the helpfulness of antipsychotics (Jorm et al., 2008b), which was rated as helpful by professionals for young adults (in the 21-year-old vignette). It is also possible that beliefs about interventions are related to other factors such as perceived barriers to treatment (Jorm et al., 2007b) or parental beliefs (Jorm and Wright, 2007). Any effects of beyondblue on help seeking may also operate indirectly via recognition of the disorder, given previous findings that accurate labelling is associated with help-seeking beliefs (Wright et al., 2007).
Strengths and limitations
This national survey is the first to examine the associations between young people’s awareness of beyondblue as a mental health organization and various indices of mental health literacy across different mental disorders, using data from a large national sample of Australian youth. Nonetheless, the study has some limitations. Firstly, given its cross-sectional nature, it is not possible to ascertain the direction of effects between young people’s mental health literacy and beyondblue awareness. Secondly, this study could not ascertain whether awareness of beyondblue predicts young people’s actual help-seeking or first-aid behaviours in the context of mental health problems in themselves or a peer. However, there is evidence from a two-year follow-up of the 2006 sample showing that first-aid beliefs predicted subsequent actions (Yap and Jorm, in press). Furthermore, an underlying assumption of this research is that awareness and, in turn, access to beyondblue resources will benefit the mental health of the young person, but this has not yet been demonstrated. Indeed, the results of the current study support others that show that the percentage of young people with mental health problems who receive treatment is very low (Slade et al., 2009). It is likely that improving these low help-seeking rates can only be done by addressing contributing factors such as the availability of services, the level of mental health literacy, stigmatizing attitudes, emotional competence and supportive social interactions (Rickwood et al., 2005). There is some evidence that young people perceive their peers as having a higher need for help than themselves (Raviv et al., 2009), and the results of the current study, which show that beyondblue awareness is more likely to be linked to quality of first-aid beliefs than quality of beliefs about interventions, suggest that efforts to narrow this gap may be beneficial.
Conclusions
Findings from this national survey indicate that awareness of beyondblue among Australian young people is high and that it is associated with better mental health literacy across disorders, including psychosis. In particular, while beyondblue awareness is associated with better recognition of disorders and first-aid beliefs that are more closely aligned to professional beliefs, our findings suggest that future beyondblue campaigns may need to focus on influencing young people’s treatment beliefs. In addition, recognition of social phobia remains inadequate and should be a focus of future beyondblue efforts, especially among young people at a younger age, and among males.
Footnotes
Funding
Funding for the study was provided by the Australian Government Department of Health and Ageing and the NHMRC Australia Fellowship awarded to Professor Jorm.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.