
Abstract
Keywords
At any one time approximately one in five people in the community suffer from an anxiety, depressive or substance use disorder [1]. Of concern, the majority do not seek or receive help for these disorders [1], [2]. Understanding the factors that influence help-seeking is an essential step towards improving the mental health of the community.
A variety of models have been used to guide research into the factors that may influence help-seeking. For example, the behavioural model of health services utilization proposes that people's use of health services is a function of their predisposition to use services, enabling factors such as availability, accessibility and cost of services, and need for services [3]. Predisposing characteristics, or factors that influence self-recognition of problems and attitudes towards treatment include health beliefs (the attitudes, values and knowledge that people have about health and health services) and a variety of demographic variables such as age, gender, and social structure measured by variables such as education, occupation and ethnicity.
The ease with which these three groups of factors can be changed, and help-seeking improved, varies considerably. For example, changing enabling factors requires systems change. By contrast, some predisposing factors may be influenced by intervention at an individual and/or population health level.
As regards predisposing characteristics, studies have consistently shown that among those with disorders, more women than men seek help [4–7]. Various explanations have been suggested to account for the effect of gender. First, it has been suggested women seek help more often because they experience more mental health problems than men. Large-scale epidemiological studies have found that while men and women differ in the types of disorders they experience, overall there is little difference in overall prevalence between the groups [2], [8]. A second suggestion has been that the effects of gender role socialization lead to the development of sex-typed personality traits, attitudes and behaviours [9], which underpin the differences in how men and women experience and respond to mental health concerns. Culture may be an additional and third explanation. In some cultures, men are taught that power, dominance, competition and control are essential to proving one's masculinity [10]. In such cultures, overt expressions of feelings, displays of emotion and demonstration of vulnerability are to be avoided. This is exemplified by the traditional stereotypic characterization of the ‘Aussie male’ [11]. Such male sex-role stereotyping and the ideology of self-reliance may present substantial barriers to help-seeking for mental health problems.
The aim of the present study was to add to existing research focusing on the reasons for gender differences in help-seeking by comparing the frequency among men and women of a number of individual and socioculturally influenced attitudinal factors that may influence help-seeking for mental health problems. Specifically, we examined the individual (personality) factors of alexithymia, and openness to experience, and the socially influenced factors of stoicism, perceived and personal stigma in men and women living in rural Victoria. We hypothesized that (i) men would score higher on the measures of alexithymia, stoicism personal and perceived stigma compared to women; and (ii) women would score higher on openness to experience compared to men.
Method
Sample
Subjects were recruited from a larger sample of adults (n = 7615) recruited randomly from the electoral roll who had participated in a survey of mental health and well-being in rural residents in 2002 [12]. Subjects in the original study who indicated their willingness to be involved in further research (n = 1238), were sent a self-report questionnaire containing the measures described here.
Measures
Sociodemographic details collected in earlier stages of the research included age, sex, marital status, highest level of education attained, and country of birth. Attitudinal factors were measured using the following instruments.
Liverpool Stoicism Scale
The Liverpool Stoicism Scale (LSS) is a 20-item self-report questionnaire that is designed to assess popular views of stoicism, including lack of emotional involvement, a dislike of free emotional expression, and an ability to endure emotion [13]. Higher scores on the LSS reflect greater stoicism. The scale demonstrated high internal reliability in the present study with a Cronbach's alpha of 0.86.
Toronto Alexithymia Scale
The Toronto Alexithymia Scale (TAS) is a 26-item self-report questionnaire designed to assess key features of alexithymia including difficulty identifying and describing feelings, an inability to distinguish between feelings and bodily sensations, a paucity of inner emotional and fantasy life [14]. The scale demonstrated adequate internal reliability with a Cronbach's alpha of 0.77.
Openness subscale from the NEO Personality Inventory
The Openness subscale from the NEO Personality Inventory (NEO-O) [15] measures one of the five factors (Openness to experience) described in the five-factor personality model [16]. Openness involves the active seeking and appreciation of experiences for their own sake. The NEO-O self-report captures the six facets of Openness to experience: O1 Fantasy, openness to fantasy, daydreaming and imagination; O2 Aesthetics, appreciation of art and beauty; O3: Feelings, receptivity to one's own inner feelings and emotions (high scorers experience deeper and more differentiated emotional states, while low scorers have somewhat blunted affects and do not believe that feeling states are of much importance); O4 Actions, willingness to try different activities, go new places or eat unusual foods; O5 Ideas, intellectual curiosity and willingness to consider new, perhaps unconventional ideas; and O6 Values, readiness to re-examine social, political, and religious values. The subscales demonstrated adequate internal reliability for the present study with Cronbach's alphas for the subscales as follows: Fantasy (0.74), Aesthetics (0.82), Feelings (0.78), Actions (0.69), Ideas (0.79), and Values (0.67).
Personal stigma
This was measured using the Depression Stigma Scale–personal, a subscale of the Depression Stigma Scale (DSS) [17]. This nine-item subscale measures an individual's own stigmatizing attitudes (e.g. depression is a sign of personal weakness; depression is not a real illness). Higher scores indicate greater personal stigma. The scale has a reported high internal stability with Cronbach's alpha of 0.79 [17]. For the present study the Cronbach's alpha was 0.83.
Perceived stigma
This was measured using the Depression Stigma Scale–perceived, a subscale of the DSS [17]. This nine-item subscale measures an individual's beliefs about the stigmatizing attitudes of other people (e.g. most people believe depression is a sign of personal weakness; most people believe depression is not a real medical illness). Higher scores indicate greater perceived stigma. The scale has a reported high internal stability with Cronbach's alpha of 0.82 [17]. For the present study the Cronbach's alpha was 0.88.
Statistics
To determine group differences based on categorical variables, Pearson χ2 analysis was used. Independent sample t-tests were used to determine group differences based on continuous measures. A multivariate analysis of variance was performed to find any group differences based on a linear combination of the measures of interest, that is, LSS, TAS-26, the six facets of the NEO-O, and the two subscales of the DSS. Independent analysis of variance (ANOVA) was used to find group differences on each of the separate measures. Prior to analysis the dataset was examined for normality, and multicollinearity. The significance level was set at the 0.05 level. All data analysis was conducted using the SPSS 13.0 statistical package (SPSS, Chicago, IL, USA).
Results
Of the 1238 individuals who were sent questionnaires, 122 were identified as lost to follow up (i.e., changed address/deceased), thus the total pool of potential participants consisted of 1116 individuals. Of these, 579 individuals returned completed questionnaires, yielding a response rate of 51.9%. The sample consisted of 244 men (42.1%) and 335 women (57.9%). Three hundred and sixty-seven (63.4%) were from farms or small rural towns and 212 (36.6%) were from a large regional city.
Representativeness of the total sample (including responders and non-responders) was assessed by comparison with the 2001 Commonwealth Census data. Mean age of the current study sample was approximately 57.0 years compared with 47.3 years in the complete census data. In the census 50.3% of adults were female and 87.5% were born in Australia. In the current study sample 54.8% were female and 92.7% were born in Australia.
Responders were compared to non-responders on sociodemographic characteristics obtained in the previous stage of the research. Compared to non-responders, responders had significantly more years (i.e. ≥13 years) of formal education, 39.6% versus 46.6%, respectively (p < 0.05). The two groups did not differ on age, marital status, employment status, country of birth, or length of stay in current residence. The results comparing responders and non-responders are presented in Table 1.
Subject sociodemographic characteristics
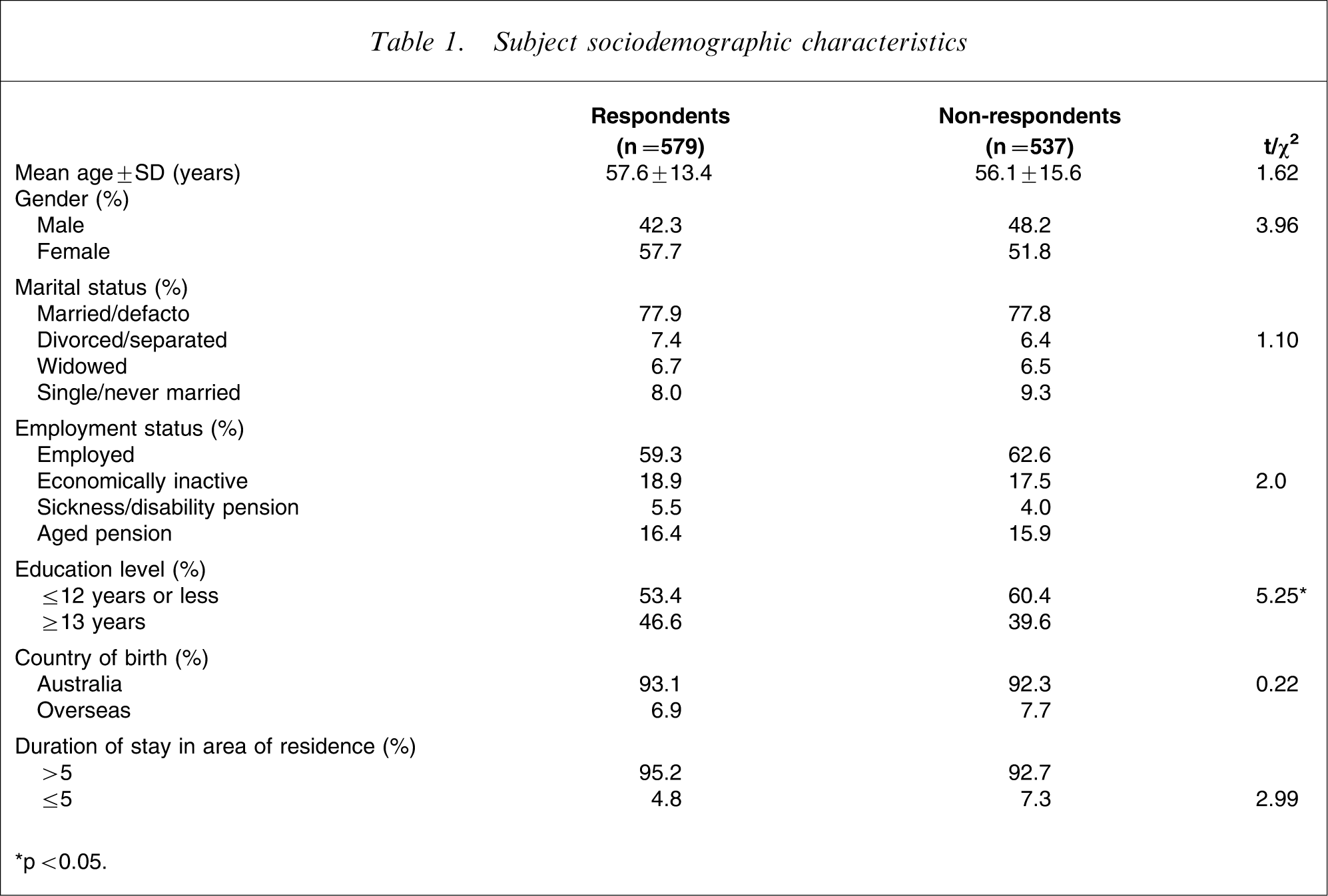
∗p < 0.05.
Effects of gender
A correlation matrix was run including all the following variables: alexithymia, stoicism, personal stigma, perceived stigma, aesthetics, feelings, actions, values, ideas, fantasy, and gender. Female gender correlated significantly with stoicism (r = − 0.47), personal stigma (r = − 0.31), and aesthetics (r = 0.32), feelings (r = 0.25), actions(r = 0.21), and values (r = 0.12).
The matrix correlation also indicated that perceived stigma was the most independent scale, correlating r ≤ 0.14 with the remaining variables. In contrast, personal stigma shared greater commonality with four of the scales: openness to feelings (r = − 0.37), openness to values (r = − 0.35), openness to aesthetics (r = − 0.30), and stoicism (r = 0.47). The two stigma scales were poorly correlated (r = 0.14). As regards stoicism, it correlated negatively with all six facets of the Openness scale and moderately or better with three of those subscales, namely, Aesthetics (r = − 0.44), Feelings (r = − 0.53), and Actions (r = − 0. 45). Scores on the stoicism scale were positively correlated with alexithymia scores (r = 0.33). Five of the six facets of Openness (but not Values), correlated negatively with alexithymia scores (r = − 0.34 to −0.40). In the main, the six facets of Openness were positively correlated and moderately correlated with one another.
A multivariate analysis of variance (MANOVA) was then performed to investigate whether there was an effect of gender on alexithymia, stoicism, personal and perceived stigma and the six facets of Openness: Aesthetics, Feelings, Actions, Values, Fantasy and Ideals. The multivariate results indicated that there was an effect of gender on the variables of interest, Wilk's lamba (F10,396) = 19.6, p < 0.0001, partial η2=0.33. Examination of the univariate tests showed that there were significant differences between men and women on stoicism, personal stigma, and four facets of Openness (Aesthetics, Feelings, Actions, and Values subscales). The results of the univariate tests are presented in Table 2.
Univariate ANOVAs comparing men and women
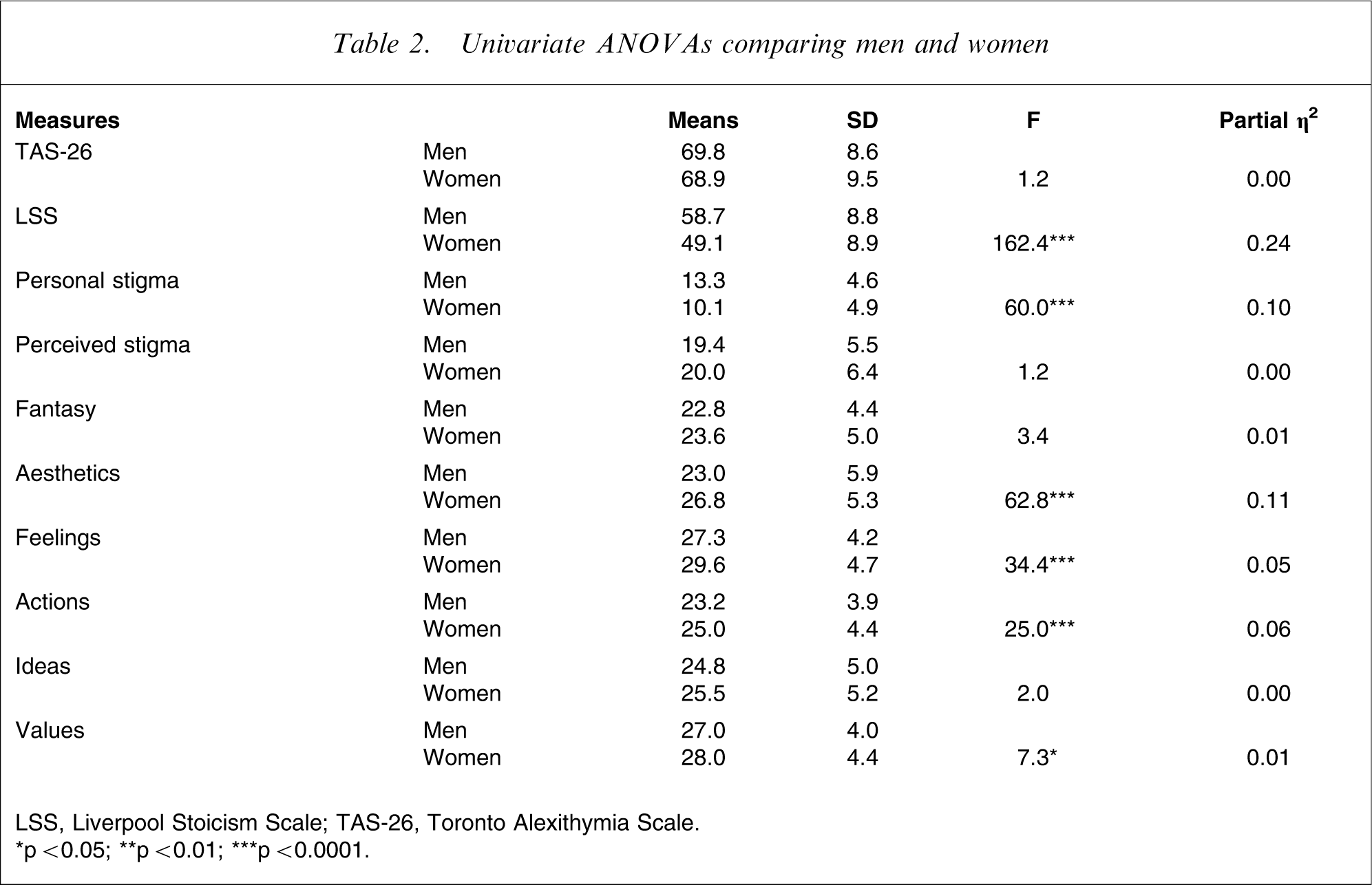
LSS, Liverpool Stoicism Scale; TAS-26, Toronto Alexithymia Scale.
∗p < 0.05; ∗∗p < 0.01; ∗∗∗p < 0.0001.
As can be seen from Table 2, men scored significantly higher on stoicism and personal stigma than women, but lower on the Openness facets of Aesthetics, Feelings, Actions, and Values, although there was only a 1 point mean difference between the two groups for the Value subscale.
Discussion
In the present study we examined a number of attitudinal factors that may influence help-seeking for mental health problems. We sought to determine whether the reasons for the consistently observed gender differences in help-seeking might be due to differing attitudes of women and men.
Significant differences were found between male and female subjects. Men were found to be more stoic and more likely to feel personally discredited (personal stigma) by mental illness than women. Men also scored lower on the Openness scale of the NEO Personality Inventory, with lower scores than women on four facets: Feelings (i.e. receptivity to one's own inner feelings and emotions), Actions (i.e. willingness to try new activities), Aesthetics (i.e. appreciation of art and beauty), and Values (i.e. readiness to re-examine social, political, and religious values).
In contrast, no male: female differences were found on the alexithymia scale in the ANOVAs and alexithymia did not correlate with gender by itself. This is consistent with previous research [18], [19]. This suggests that men do not have more difficulty describing feelings than women but rather, they do not feel comfortable with overt expression of feelings or display of emotions.
The finding that differences between men and women were largely due to socially influenced attitudes may reflect longstanding gender role differences. Men's traditionally advantaged social status, greater control and decision-making power, and higher income than women, may make it difficult to accept a diagnosis of mental disorder and seek help for this. Socialization may teach men that lack of emotional involvement or expression (stoicism) is valued. The higher level of personal stigma (failure, weakness) associated with mental illness is consistent with this view.
These findings are consistent with the proposition that men fail to report [20], [21] or forget their depression [22] rather than necessarily experiencing less depression than women. Among those with defined mental disorders, men seek help less often than women [23], and suicide rates are greater for men than women [24]. In rural areas the problems appear to be exacerbated; the male: female disparity in help-seeking is greater [23] and suicide rates are higher in rural than urban men. These problems appear to particularly affect young rural men, perhaps the group most vulnerable to prevailing socioculturally influenced factors.
The present findings, however, must be considered within the methodological limitations of the project. While the study aimed to examine factors that might influence help-seeking for psychological problems, actual help-seeking behaviour of participants was not recorded, thus it remains unclear whether the variables examined might actually influence help-seeking and, if so, the nature of that influence. Further studies will be required to elucidate the nature of the relationship between the variables studied and the act of help-seeking. Also, participants in the present study were a highly self-selected group, having participated in a previous project.
Important implications flow from these findings. The present study suggests that there are characteristics of men that mitigate against self-recognition and acceptance of emotional problems and thus pose barriers to help-seeking for such problems. Further studies are needed to test this hypothesis. It is possible that these factors are more potent in among certain cultural groups and in different geographic locations, particularly those where gender inequality is marked. In order to improve help-seeking by men at risk, efforts will need to address these important gender differences and the causes underlying them. Addressing gender inequality by empowering women and improving their status in society may assist in reducing stoicism and personal stigma associated with mental health problems in men, thus enabling them to also appreciate the importance and acceptability of emotions.