
Abstract
Deliberate self-harm (DSH) including deliberate self-injury and deliberate self-poisoning (DSP) is common, costly and strongly associated with repetition of DSH and subsequent suicide [1]. Although UK rates of hospital-treated DSH have waxed and then waned in recent years, the rates of repetition may have been steadily increasing [2]. Clinical Practice Guidelines have been developed to assist clinicians in the management of this common reason for hospital presentation [3–5]. For the DSH and suicide attempt behaviours of patients with borderline personality disorder (BPD), two different treatments have been reported to be effective: a day hospital, psychodynamic, mentalization program [6,7] and Dialectical Behaviour Therapy, in the standard form an outpatient, team-based approach using individual therapy, group-based skills training and out of hours telephone coaching [8,9].
DSH subjects with any personality disorder have more suicide attempts than those without personality disorder [10]. In people diagnosed with BPD, DSH, repetition of DSH and suicide are also common [11]. The BPD population may have more DSH events than depressed subjects [12]; however, DSH is also one of the more changeable and less frequent of the Diagnostic and Statistical Manual-IV (DSM-IV) criteria for BPD [13]. Nonetheless, unless death by suicide or other cause occurs, people diagnosed with BPD have a reasonable prognosis, with most patients no longer meeting diagnostic criteria for BPD after 10 years follow-up [11]. BPD patients with hospital-treated DSH have a range of suicidal ideation associated with any given DSH event and the clinical judgement of the level of suicidal ideation at the time of clinical assessment has an impact on the after care arrangements that are made [14].
Understanding the reasons for DSH events, whether suicidal or non-suicidal in intention, has been an important but difficult task for clinicians and researchers for many years. An early study of 128 DSP subjects [15] found multiple reasons for the event: 44% indicated that they had wanted to die, 33% were seeking help, 42% escaping from the situation, 52% obtaining relief from a terrible state of mind and 19% trying to influence someone else. The authors concluded that a large proportion of those indicating suicidal intent do so either to gain social acceptability for their act or to influence helping agencies [15]. In a subsequent study, psychiatric assessors determined the most common reasons for the DSP event were: 71% communicating hostility, and 54% influencing others; however, these were the reasons chosen least frequently by the DSP subjects themselves [16]. Moreover, the patient's motives, attributed by health professionals, affect the clinical judgments by the health professionals about the need for care. For motives of two principal types, manipulative (i.e. aimed at eliciting a response from others) and depressive (i.e. communicating despair and aimed at withdrawal, escape or death), depressive motives were more acceptable and evoked more sympathy or readiness to help in both doctors and nurses than manipulative motives [17]. One difficulty with the notion that DSH is only manipulative, and attention seeking, is that it is of limited help in increasing our understanding of the patient's experience or behaviour. Such conceptualisations in the literature have not led to improvements in treatment or reduced the incidence of DSH. Other authors have conceptualised DSH as a coping strategy used to relieve severe emotional distress and overwhelming psychological pain [18] and a recent review suggested that in outpatients with BPD, chronic suicidal behaviour can be best understood as a way of communicating distress [19].
Aims
The present study used the Parasuicidal History Interview, version 2 (PHI-2) in an Australian sample of BPD patients to:
compare the reasons given for suicidal deliberate self-harm (S-DSH) vs. non-suicidal deliberate self-harm (NS-DSH) events; and
develop multivariate models for the independent predictors for S-DSH events.
We have used the term DSH, instead of parasuicide (from the PHI-2) throughout for consistency and ease of reading. We also use the terms NS-DSH and S-DSH instead of non-suicidal parasuicide and suicide attempt, respectively [20].
Method
Participants
Participants were 70 females with BPD and recurrent DSH recruited to a randomised controlled trial (RCT) of Dialectical Behavior Therapy, by referral to the Centre for Psychotherapy, Newcastle (a specialist outpatient treatment clinic) from the catchment area of: Newcastle, Lake Macquarie, Port Stephens and the lower and upper Hunter local government areas. Full details of the participants and original RCT study design can be found elsewhere [21].
Inclusion criteria were: female, aged more than 18 years, meeting DSM-IV criteria for BPD [22] and had experienced a minimum of three events of DSH in the previous year. Exclusion criteria were: younger than 18 years old, suffered from a disabling organic condition or psychotic illness (i.e. schizophrenia, bipolar affective disorder, psychotic depression), behaviour that posed a significant threat to staff, developmentally disabled, living more than 2 hours drive from the treatment centre in Newcastle, unable to speak or read English, or if they had previously been treated with DBT. Co-morbid misuse of drugs or alcohol was not grounds for exclusion unless the participant was unable to commit to attending prescribed therapy sessions.
Instruments
PHI-2: Suicidal intention, reasons for DSH and features of the DSH event
The PHI-2 is a 48-item semi-structured questionnaire used to investigate events of self-injury. The original Parasuicide History Interview (PHI) was subsequently modified and developed into the PHI-2 [20] and more recently into the Suicide Attempt and Self-Injury Interview (SASSI) [23]. Versions of the PHI have been used by clinical researchers investigating the efficacy and effectiveness of treatments for BPD, in participants who intentionally self-injure or self-poison [8,24–27].
The PHI-2 was developed utilising self-injuring female clinical populations to assess characteristics of self-injurious behaviour, hence instrument items were designed to facilitate description of an act of self-injury and to determine associated suicidal intent. The instrument has been shown to have good internal reliability for the measurement of suicidal intent (Cronbach's α= 0.93). Other PHI-2 items provide a standard format for obtaining supplementary descriptive information concerning self-injury events such as reasons for injury and method used to injure [23]. The PHI-2 consists of forced choice, open-ended quantitative and qualitative questions. Participants answer most questions, while the interviewer rates other items. In development of the PHI-2, the list of 31 reasons for DSH (item 28) that was ultimately selected was generated by sampling participant-generated responses until saturation occurred, and no new reasons were provided [23]. The use of participant derived responses, rather than reasons generated and imposed by clinicians or researchers, is considered to be a strength of the PHI-2.
Preliminary PHI-2 analyses
A principal component factor analysis of the reasons for DSH from item 28 of the PHI-2 was conducted using oblique (non-orthogonal) rotation and Kaiser normalisation. In keeping with Brown et al. [20], any reasons endorsed by less than 10% of the participants were omitted: reason 4 (5.5%), ‘to gain admission into a hospital or treatment program’; reason 9 (1.4%), ‘to get out of doing something’; reason 10 (2.7%), ‘to shock or impress others’; reason 12 (8.2%), ‘to give you something, anything to do’; reason 21 (4.1%), ‘to demonstrate to others how wrong they are/were’; reason 22 (0%), ‘to feel sexual arousal’; and reason 30 (1.4%), ‘other’). Reason 5, ‘to die’, was also omitted because it was closely related to the dependent variable, S-DSH. An examination of 3-, 4- and 5-factor solutions suggested a 4-factor solution was optimal. Only reasons with loadings greater than or equal to ±0.30 were retained in the 4-factor solution. The four factor labels and associated internal consistency (Cronbach's α) coefficients were as follows: ‘relief of acute painful emotions’ (eight reasons, 0.79); ‘interpersonal communication and influence’ (seven reasons, 0.81); ‘relief of chronic emotional discomfort’ (five reasons, 0.62); and ‘avoidance/escape’ (three reasons, 0.28). Further details about the factor analysis are available from the authors on request.
CIDI and IPDEQ: Psychiatric morbidity
Computerised versions of the demographic and diagnostic instruments were used in a similar fashion to the National Survey of Mental Health and Wellbeing (NSMHW) [28]. The Composite International Diagnostic Interview (CIDI v 2.1) was used to assess the presence of high prevalence psychiatric disorders using the DSM-IV classification [22]. Personality disorders were assessed using the International Personality Disorder Examination Questionnaire – (IPDEQ), which is a brief screening instrument developed as an addendum to the comprehensive IPDE [29]. The authors calculated cluster scores that simulate the classification system of the DSM-IV, which produced three personality disorder cluster scores, (A: odd/eccentric, B: dramatic/emotional and C: anxious/fearful).
Clinical interview
A clinical interview by one of three consultant psychiatrists (HJ, NP, NB) was undertaken to determine the diagnosis of BPD according to DSM-IV criteria.
Raters
The raters for all instruments were either Masters of Clinical Psychology or Psychology PhD students.
Dependent variable: suicidal deliberate self-harm
The index event for study was the most recent DSH event preceding recruitment into the (Hunter DBT) RCT [21]. Suicidal intention was measured by three PHI-2 questions: item 14, a self-report item that asked participants if they considered the DSH event a suicide attempt at the time of injury (requiring a dichotomous yes/no response); item 15, a self-report item that asked participants if they now considered (‘looking back’) the DSH event to be a suicide attempt (requiring a dichotomous yes/no response); and item 46, an interviewer rated item that assessed intention based on all information from the PHI-2 interview. The latter item was rated on a five-level ordinal scale, collapsed in the present study to form a dichotomous variable using a previous definition [20] of NS-DSH and S-DSH. The scale points 1 (obviously no intent) and 2 (only minimal intent) were collapsed to form NS-DSH; while scale points 3 (definite intent but very ambivalent), 4 (serious intent) and 5 (extreme intent, careful planning and every expectation of death) were collapsed to form S-DSH. There was a high level of agreement (95.9%) between the data generated from the two self-report items, as well as substantial agreement between the first self-report item and interviewer based assessments of intent item (chance-corrected κ = 0.77 n = 70, P < 0.001). Given the substantial agreement rate, a hybrid variable was not made, with self-reported assessment of intention ‘at the time of injury’ used as the dependent variable.
Independent variables
Covariates
Variables reflecting characteristics of the subjects included: age, treated as a continuous variable, other demographic data (education, employment and marital status) and psychiatric co-morbidity (axis I and axis II), as categorical variables, extracted from the NSMHWB computerised interview; number of DSM-IV criteria for BPD, from the clinical interview; and number of lifetime DSH events, extracted from the PHI-2 and treated as continuous variables.
Predictor variables
Variables identifying characteristics of the index DSH event were extracted from the PHI-2: (1) methods used for DSH (item 8), used as a three level categorical variable: external damage to skin or tissue (superficial cutting or burning), self-poisoning, and other methods (jumping, stabbing or hanging); (2) disinhibition: the use of drugs or alcohol prior to the DSH event (items 9 and 10), used as a binary variable: present or absent; (3) impulsiveness: impulsive to premeditated action of DSH (item 31), a seven-point scale treated as a continuous variable; (4) rescue contact: any rescue sought after DSH event (item 35), used as binary variable: sought or not sought; (5) reasons for DSH event (item 28), where endorsement of each of the 31 reasons was indicated by ‘yes’ or ‘no’, and these were further developed into four factors (see factor analysis reported earlier), with endorsement rates ranging from 0 to 1 (0: none of the reasons endorsed, to 1: all of the reasons within that factor endorsed); and (6) effectiveness of resolution of reasons for the DSH event (item 29), using aggregated ratings on a five-point scale for each of the individual reasons comprising the four DSH factors, and also as an aggregated additional variable, effectiveness of resolution of reasons for DSH event (overall), using the overall means.
Analyses
Univariate analyses of NS-DSH vs. S-DSH
Comparisons of subject characteristics and DSH event characteristics were made for NS-DSH vs. S-DSH outcomes using chi-square analysis for differences in proportions for the categorical data and two-tailed t-tests for the continuous data. Independent predictor variables with a P value of less than or equal to 0.08 were individually analysed using a binary logistic regression analysis to produce unadjusted Odds Ratios (OR) and 95% confidence intervals (95% CI).
Multivariate analyses: predicting S-DSH
We examined independent variables that reflected both subject characteristics and DSH event characteristics. Because most subjects had experienced multiple DSH events, sometimes with suicidal intent and sometimes with non-suicidal intent, the comparison of subject characteristics (classified by index NS-DSH vs. S-DSH event) was made in order to identify possible subject based confounders (in examining relationships between DSH event characteristics and S-DSH vs. NS-DSH). Any significant differences in subject characteristics were used as covariates in multivariate models (logistic regression) of DSH event characteristics predicting S-DSH.
Possible interaction terms for significant univariate predictor variables were developed and tested for possible inclusion in the multivariate models, though none were ultimately included. One three level categorical hybrid variable (from method and rescue contact) was developed and entered in the multivariate models: method of external damage to the skin with no rescue contact sought; method of external damage to the skin (with rescue contact sought); and method of poisoning or other method.
A binary logistic regression model was developed for the predictors of S-DSH using a forced entry method, using any independent predictor variables at the level of P ≤ 0.08. A second binary logistic regression model was developed using backward step wise elimination (retention P < 0.05), for the same outcome variable, S-DSH. Results are reported as adjusted odds ratios (AORs) with 95% confidence intervals (95% CI). The perceived effectiveness of the resolution of reasons for DSH (overall) was the only ‘effectiveness rating’ retained in these analyses as it was available for all individuals.
Results
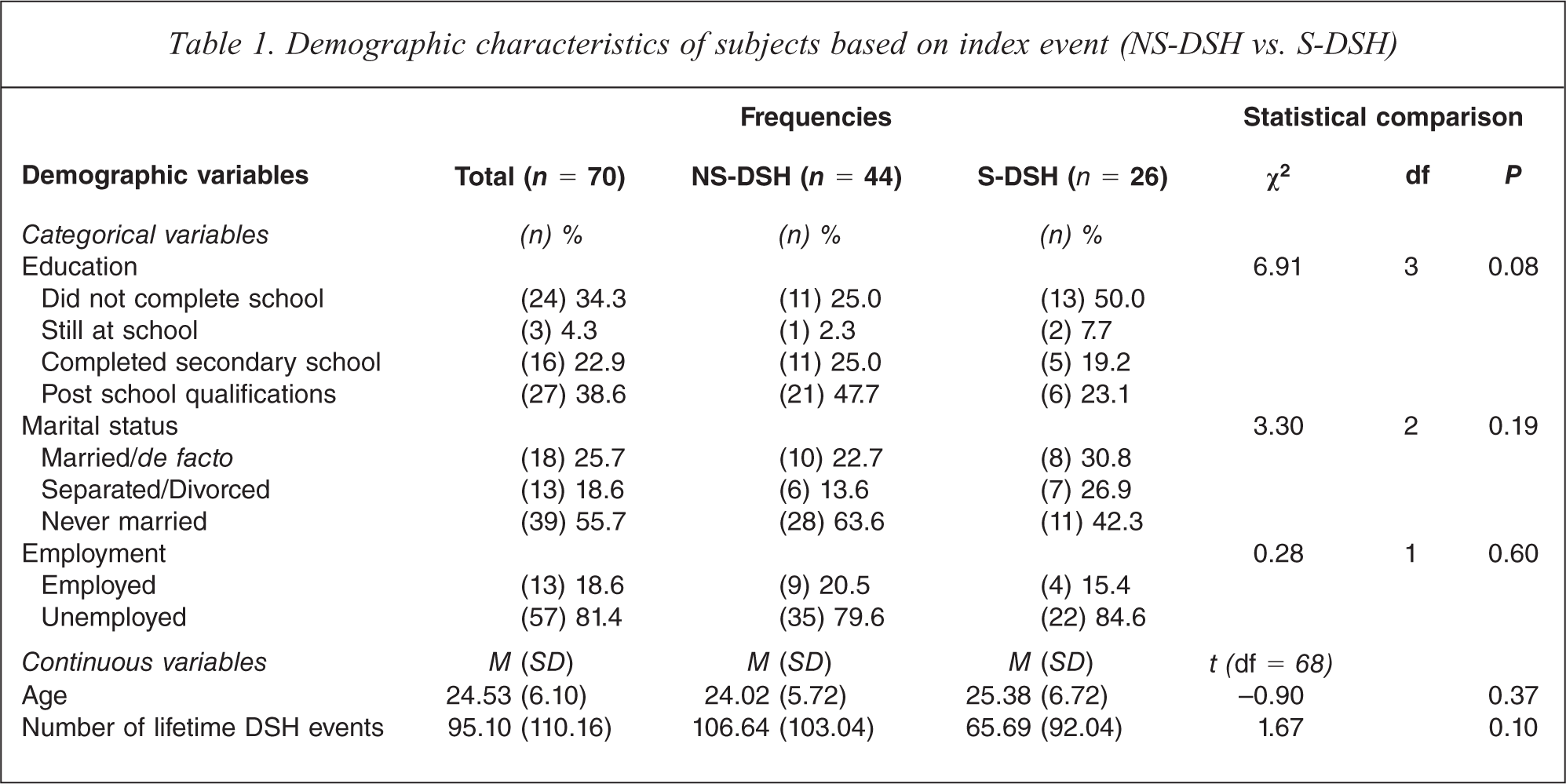
Table 1 details the demographic characteristics of the subgroups and the overall sample. There were no significant differences in demographics or lifetime DSH events. However, education level was significant at the P = 0.08 level and, consequently, was retained in the logistic regression model as a covariate. Moreover, there were no significant NS-DSH vs. S-DSH differences in the number of BPD criteria met (7.07, SD 1.06; vs. 7.29, SD 0.90; t (62) = −0.80, P = 0.42), in CIDI derived axis I psychiatric co-morbidity (any anxiety disorder, 88.6 vs. 88.5%, χ2 (1) = 0.00, P = 0.98; any mood disorder, 68.2 vs. 80.8%, χ2 (1) = 1.31, P = 0.25; and any substance disorder, 68.2 vs. 69.2, χ2 (1) = 0.01, P = 0.93), or in the proportions for axis II co-morbidity for IPDEQ derived personality disorder (any cluster A disorder, 70.5 vs. 50.0%, χ2 (1) = 2.93, P = 0.09; any cluster B disorder, 70.5 vs. 76.9%, χ2 (1) = 0.35, P = 0.56; any cluster C disorder, 75.0 vs. 84.6%, χ2 (1) = 0.90, P = 0.34; or for any personality disorder, 86.4 vs. 92.3%, χ2 (1) = 0.57, P = 0.45).
Demographic characteristics of subjects based on index event (NS-DSH vs. S-DSH)
Reasons for DSH are reported in Table 2, based on PHI-2 item 28 responses with greater than 10% endorsement. The mean endorsement rates for each reason are shown together with the average endorsement rates for the associated factors. Overall, 66 respondents (94.2%) endorsed at least one of the reasons within the ‘relief of acute painful emotions’ factor, with the corresponding rates for the other factors: 47 (67.1%), ‘interpersonal communication and influence’; 53 (75.8%), ‘relief of chronic emotional discomfort’; and 37 (52.9%), ‘avoidance/escape’. As shown in the right-hand columns of Table 2, the S-DSH subgroup had a higher average endorsement rate for the reasons within the avoidance/escape factor (P = 0.02), and there was also a tendency for the same subgroup to endorse more of the reasons within the interpersonal communications and influence factor (P = 0.07).
Endorsement rates for PHI-2 (item 28) reasons for DSH, and associated factors: NS-DSH vs. S-DSH
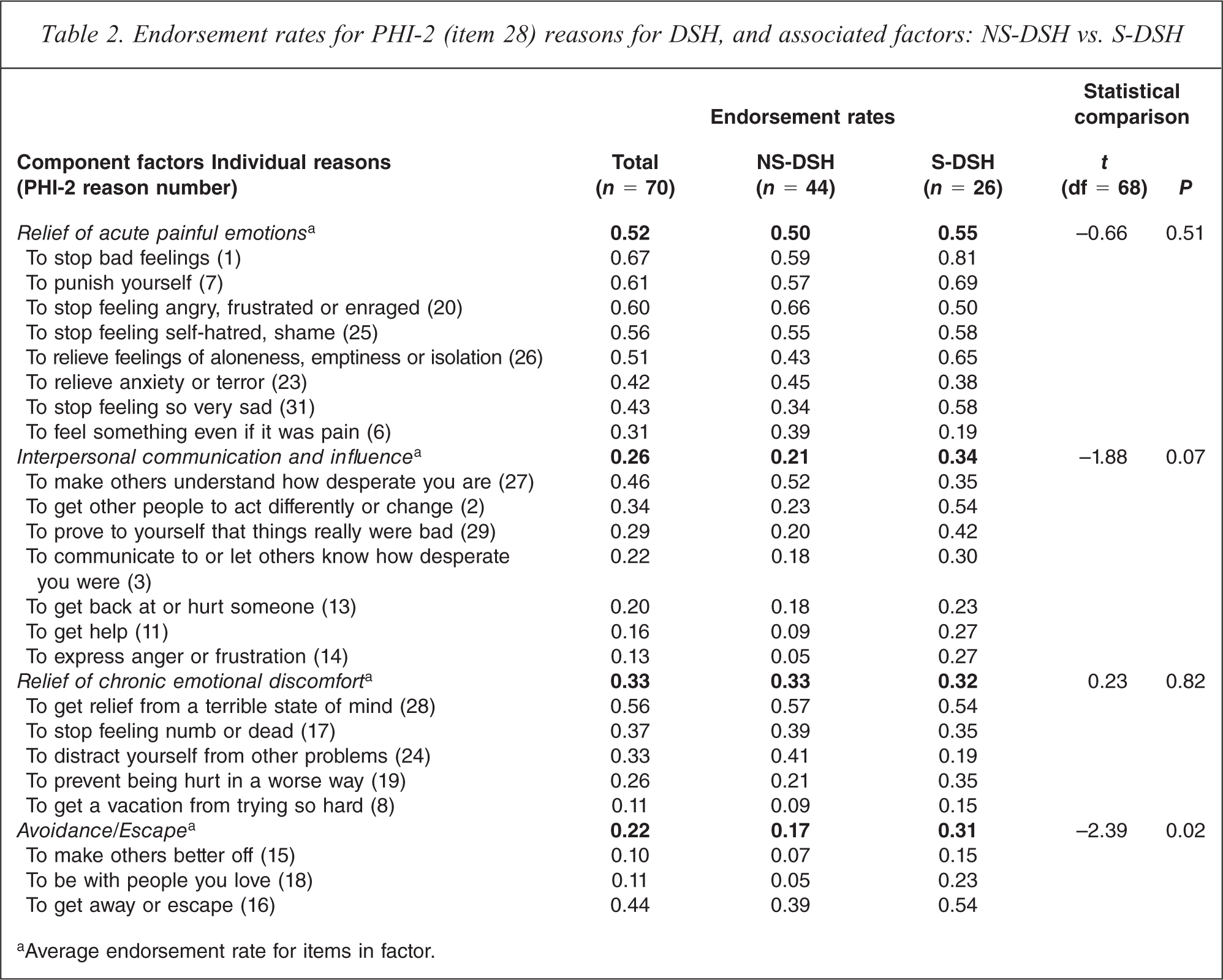
aAverage endorsement rate for items in factor.
Other DSH event characteristics derived from the PHI-2 were used to examine the differences in NS-DSH vs. S-DSH events and can be seen in Table 3. The method of DSH was significantly associated with NS-DSH vs. S-DSH, with external damage to skin more common in NS-DSH and self-poisoning more common in S-DSH events. Rescue contact was significantly more likely to be sought after S-DSH events. Disinhibition by drugs or alcohol and impulsivity were not associated with NS-DSH vs. S-DSH. The overall effective resolution of the reasons for the DSH event was significantly negatively associated, as were two of the constituent factors, effective resolution of acute painful emotions and resolution of avoidance/escape. In each case, there was a lower level of effective resolution of the reasons for DSH event reported in the S-DSH event group.
Comparison of PHI-2 profiles for index event (NS-DSH vs. S-DSH)
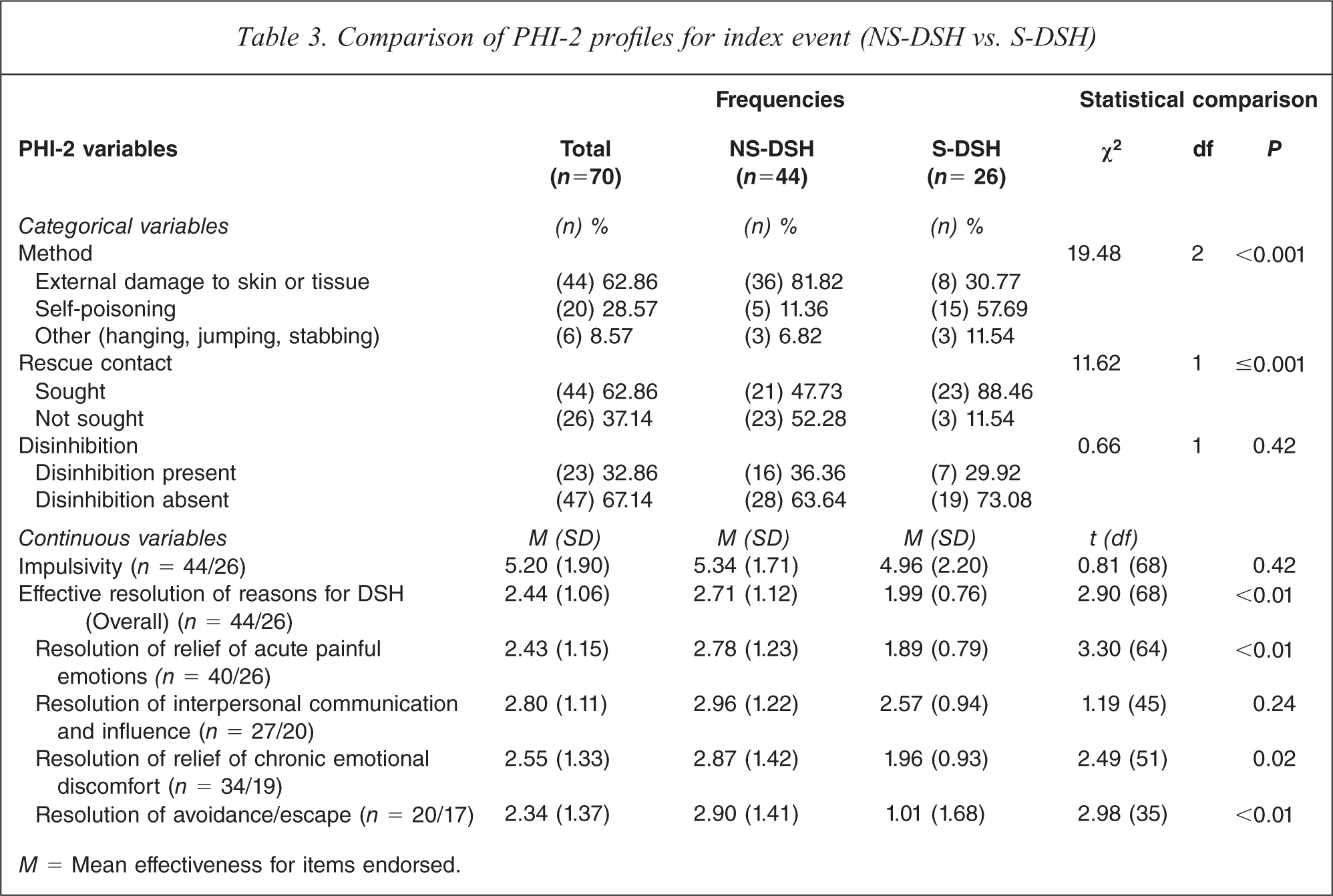
M = Mean effectiveness for items endorsed.
Predicting S-DSH (vs. NS-DSH) event from logistic regression models
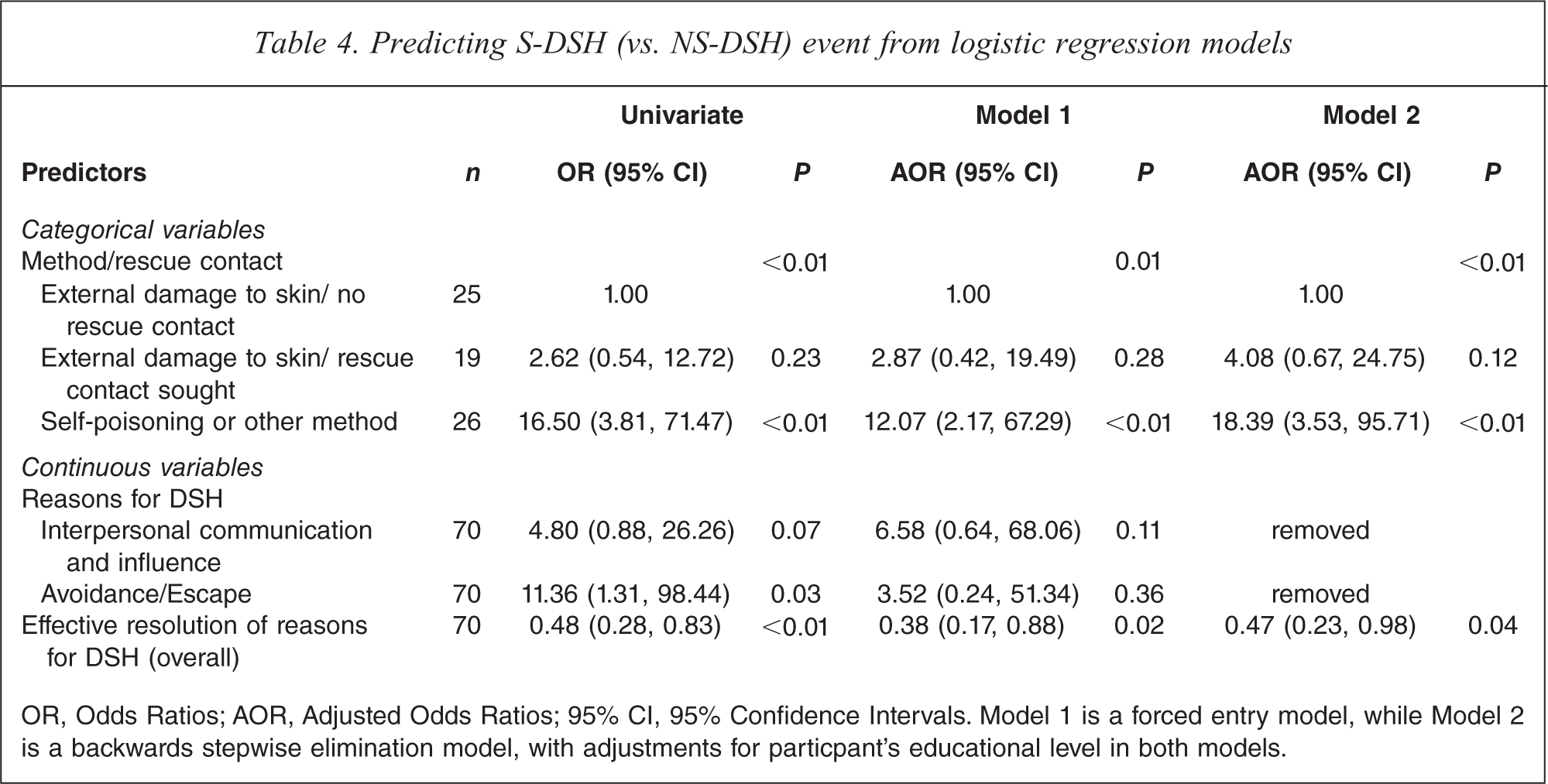
OR, Odds Ratios; AOR, Adjusted Odds Ratios; 95% CI, 95% Confidence Intervals. Model 1 is a forced entry model, while Model 2 is a backwards stepwise elimination model, with adjustments for particpant's educational level in both models.
The forced entry logistic regression model showed only two variables to be significantly associated with S-DSH. Self-poisoning or other method of DSH was more likely to be associated with a S-DSH event than the referent category external damage to skin with no rescue contact sought, AOR 12.07 (95% CI 2.17, 67.29). Effectiveness of resolution of overall reasons for DSH was also significantly negatively associated with a S-DSH event, AOR 0.34 (95% CI 0.14, 0.83), meaning that there was a one-third reduced risk of being a S-DSH event for each one unit increase in feeling that the DSH event helped to effectively resolve those reasons for the DSH event. In other words, the lower sense of effective resolution of the reasons for DSH (overall), the more likely the DSH event was to be suicidal in intention. A similar pattern of two significant predictor variables was found for the backward stepwise elimination model: AOR 18.39 (95% CI 3.53, 95.71) and AOR 0.47 (95% CI 0.23, 0.98), respectively.
Discussion
Strengths and weaknesses of the study
This study had several strengths that would be protective for the common threats to internal validity for a study of this kind; misclassification bias, measurement bias and confounding. The study used well-validated instruments to determine subject characteristics. It also used PHI-2, an instrument specifically designed for the evaluation of ‘parasuicide’-related phenomena in BPD subjects, to determine DSH event-related characteristics and the dependent variable for the study. Potential misclassification of DSH events was reduced by examining three different questions to determine the level of suicidal ideation and the agreement for each of these three variables was strong. All assessors and subjects were blind to the specific aims of the current study and all data was collected prospectively. Confounding was dealt with in the analyses by controlling for any subject characteristics (based on NS-DSH vs. S-DSH events classification), which were related to the dependent variable and by controlling for the effects of all univariate associated event-related variables.
The sample consisted of individuals from a highly specific clinical population; that is, women diagnosed with BPD and multiple DSH events, who were recruited into a RCT for DBT and who were all severely co-morbidly ill. This limits the level to which the present findings may be generalised to any other DSH populations. Further research aimed at assessing the validity and reliability of the four factors from the PHI-2, developed in the present study would also help determine the strength of the present findings.
Main findings
The existence and severity of suicidal intention itself is not always easily assessed; apparently contrasting suicidal ideas co-existing with the intention to survive may be commonly encountered in a state of ambivalence at the time of DSH events. However, using a specific cut point produced almost identical determinations of what could be classified as a NS-DSH and S-DSH event by participants and raters.
BPD subjects endorse a complex range of reasons for a single DSH event. The six PHI-2 reasons that were endorsed by more than 50% of the sample related to personal feelings and reactions, as opposed to relationships with others: reason 1 (67%), stop bad feelings; reason 7 (61%), punish yourself; reason 20 (60%), stop anger and frustration; reason 25 (56%), stop self-hatred; reason 28 (56%), relief from a terrible state of mind; and reason 26 (51%), relieve feelings of emptiness. However, by-and-large, the pattern of reasons expressed did not clearly distinguish NS-DSH from S-DSH events. For example, three of the four factors (derived from reasons given) did not significantly distinguish between NS-DSH and S-DSH events. The only factor which did significantly distinguish the suicidal ideation condition was based on only three reasons and had the lowest Cronbach's α. This may show how difficult if not impossible it is in the clinical setting to infer suicidal intent from the specific reasons given for DSH events.
Comparisons of the NS-DSH vs. S-DSH results from the current study with the results of the Brown et al. study are difficult because of the differences in scale and item selection and analysis methods [20]. Due to the low alpha score, Brown et al. dropped the corresponding avoidance/escape scale from their endorsement rate analysis. For eight of the original 30 reasons, which they did not include in any of the four rationally derived scales, they also individually assessed any differences for the binary outcome of NS-DSH vs. S-DSH [20]. Despite these differences in methods, there were some similarities in findings to the current study; two of the three tested rationally derived scales and four of the eight individual items tested, did not distinguish NS-DSH from S-DSH events. However, there was significantly more endorsement for the individual reasons, expression of anger, self-punishment, and distraction in the NS-DSH events than the S-DSH events. There was a higher rate of endorsement for the reason, ‘to make others better off’ for S-DSH events, which was consistent with the findings in the current study.
From the current study, there may be limited implications for clinical assessment of BPD females after an episode of DSH. Using a self-poisoning method of DSH (referent group external damage to skin) and making any rescue contact (referent group no rescue contact sought) were associated with S-DSH events at the univariate level, suggesting that any BPD subject who reaches clinical services or who has been a DSP case is more likely to have had suicidal intention involved in the DSH event, even though the suicidal intention may have declined by the time of presentation at the Emergency Department or subsequent psychiatric examination [14]. In the multivariate models a hybrid methods/rescue variable was used wherein external damage to skin with rescue contact sought, showed an increased odds ratio, which was not significantly different in predicting a S-DSH event than the referent group external damage to skin with no rescue sought. This non-significant finding may be due to insufficient power and so the clinical implication may still be that if the patient has reached clinical services, the DSH event may still have been more likely to have had suicidal ideation at the time of the event. Where any other method of DSH was used, that patient should be considered as being at increased risk of having had some level of suicidal intention at the time of the DSH event. Similarly, when a patient indicates that the reasons for the DSH event have not been effectively resolved by the DSH event and its sequelae, the likelihood of the DSH event itself being considered as suicidal are increased. This suggests that clinicians might rely less on the reasons for a given DSH event in trying to determine suicidal intention and rely more on the methods used and the whether the reasons for the DSH event have resolved, ideas which could be incorporated into clinical assessments.
Conclusion
Developing a better understanding of the range of reasons given for DSH by those who engage in it may help reframe more helpful, less pejorative and more accurate attitudes towards all patients with non-fatal suicidal behaviours. Within BPD populations, DSH is a common, though maladaptive and often dangerous coping strategy used by individuals who experience extreme distress and who have not been able to utilise a more constructive approach to managing their distress. From this study, DSH is more likely to be explained by patients as being used to reduce distressing personal symptoms and less to influence the behaviour of others. This study does not address whether clinicians make the same attributions of the reasons for DSH offered by the patients. Changes in attitude toward DSH by clinicians may improve the treatment experience of those who self-harm and therefore make treatment compliance a more attractive option for the patient. Patients with BPD and DSH may engage in both NS-DSH and S-DSH events at different times, are motivated by a range of reasons, may or may not seek treatment and are also at increased risk of subsequent suicide. Further clinical questions can be developed about how to better understand and manage these DSH behaviours in BPD populations.
Footnotes
Acknowledgements
Our thanks go to several people for their contributions to the Hunter DBT Project; Dr Chris Hayes, University of Newcastle and Ms Susan Burgoyne as Investigators in the initial project development and to Peter Sneesby as Masters of Clinical Psychology student, University of Newcastle, assisting with initial phases of data collection. Our thanks also go to all the staff who contributed clinical services; Individual Therapists: Danielle Adams, Marianne Ayre, Dr Nick Bendit, Susan Burgoyne, Jennifer Evans, Dr Howard Johnson, Jennifer Koorey, Natalie McCall, Chris McCrory, Jane Taylor and Chris Willcox; and Skills Trainers: Marianne Ayre, Dr Nick Bendit, Linda Bragg, Michael Currie, Annabel Kelly, Michelle Meyer, Ruth Spence and Don Stewart; and also to Dr Howard Johnson, Dr Nick Bendit and Dr Neil Port who undertook the baseline clinical interviews. We also appreciated the input from external Honorary Consultants: Dr Marsha Linehan & Dr Kelly Koerner, University of Washington, USA, supplementary training of DBT therapists by Dr Kate Comtois and Dr Kelly Koerner University of Washington, USA and assistance with instrument scoring and data cleaning by Dr Kerrie Clover, University of Newcastle.