
Abstract
Objectives:
Anorexia nervosa is a severe psychiatric disorder with high mortality rates. While its aetiology is poorly understood, there is evidence of a significant genetic component. The Anorexia Nervosa Genetics Initiative is an international collaboration which aims to understand the genetic basis of the disorder. This paper describes the recruitment and characteristics of the Australasian Anorexia Nervosa Genetics Initiative sample, the largest sample of individuals with anorexia nervosa ever assembled across Australia and New Zealand.
Methods:
Participants completed an online questionnaire based on the Structured Clinical Interview Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV) eating disorders section. Participants who met specified case criteria for lifetime anorexia nervosa were requested to provide a DNA sample for genetic analysis.
Results:
Overall, the study recruited 3414 Australians and 543 New Zealanders meeting the lifetime anorexia nervosa case criteria by using a variety of conventional and social media recruitment methods. At the time of questionnaire completion, 28% had a body mass index ⩽ 18.5 kg/m2. Fasting and exercise were the most commonly employed methods of weight control, and were associated with the youngest reported ages of onset. At the time of the study, 32% of participants meeting lifetime anorexia nervosa case criteria were under the care of a medical practitioner; those with current body mass index < 18.5 kg/m2 were more likely to be currently receiving medical care (56%) than those with current body mass index ⩾ 18.5 kg/m2 (23%). Professional treatment for eating disorders was most likely to have been received from general practitioners (45% of study participants), dietitians (42%) and outpatient programmes (42%).
Conclusions:
This study was effective in assembling the largest community sample of people with lifetime anorexia nervosa in Australia and New Zealand to date. The proportion of people with anorexia nervosa currently receiving medical care, and the most common sources of treatment accessed, indicates the importance of training for general practitioners and dietitians in treating anorexia nervosa.
Introduction
Anorexia nervosa (AN) imposes a major health burden in Australasia and worldwide, and has a higher mortality rate than any other psychiatric disorder (Deloitte Access Economics, 2012). Community-based estimates of incidence and lifetime prevalence vary between countries, and are affected by variations in definitions of AN and statistical power limitations (Smink et al., 2012). An Australian study of female twins has estimated the lifetime prevalence of AN (using Diagnostic and Statistical Manual of Mental Disorders [4th ed.; DSM-IV] criteria (American Psychiatric Association, 1994)) at 1.9%, with a further 2.4% meeting all criteria except amenorrhoea (Wade et al., 2006). The lifetime prevalence of AN (using DSM-IV criteria) in New Zealand women has been estimated at 1.0%, and in New Zealand men at 0.1% (Oakley Browne et al., 2006). The causes of AN are still largely unknown; however, twin studies have estimated its heritability to be around 60% (Bulik et al., 2006; Wade et al., 1999, 2000), intermediate between depression (~40%) (Flint and Kendler, 2014) and schizophrenia (~80%) (Sullivan et al., 2003).
Genome-wide association studies (GWAS) have recently been shown to be an effective method of finding genes for some psychiatric disorders, including schizophrenia, autism and bipolar disorder, where very large samples of cases and controls (36,989 cases, 113,075 controls in the case of schizophrenia) have identified multiple loci meeting genome-wide significance (Cross-Disorder Group of the Psychiatric Genomics Consortium, 2013; Schizophrenia Working Group of the Psychiatric Genomics Consortium, 2014). A GWAS conducted on 1033 AN cases and 3773 paediatric controls in the United States found a number of association signals that the authors deemed worthy of follow-up, including near ZNF804B, CSRP2BP, NTNG1, AKAP6 and CDH9, but none that met genome-wide association significance (Wang et al., 2011). Pilot genome-wide association analyses in a sample of 2564 female twins conducted in Australia (Wade et al., 2013) identified six genomic regions with suggestive significance for eating disorders, including four for AN: near the CLEC5A, LOC136242, TSHZ1, and SYTL5 loci (p < 5 × 10−7). Both studies concluded that much larger samples were needed to identify genes for eating disorders at a genome-wide significance level of p < 5 × 10−8. In 2014, an international consortium performed GWAS on AN patients from 17 countries. Despite recruiting 2907 AN cases and 14,860 controls, no findings reached genome-wide significance (Boraska et al., 2014) and the authors concluded that this sample, although the largest yet reported, was still underpowered.
Thus, there is an urgent need to collect much larger samples of genotyped AN cases and controls if we are to convincingly elucidate the genetic basis of AN. The Anorexia Nervosa Genetics Initiative (ANGI) is an international collaboration which aimed to collect diagnostic data and blood samples from over 13,000 individuals with AN in Australia, the United States, Sweden and Denmark. The purpose of this paper is to report on the methods of recruitment used by the Australian site and describe the features and treatment experiences of a large community sample of people with AN in Australia and New Zealand. This is the largest sample of people with lifetime AN collected in Australasia to date, and these results will improve our understanding of the care of patients with AN, as well as inform research that is aiming to recruit large samples of participants in other areas of psychiatry.
Methods
Study population
Participants for this study were Australian and New Zealand women and men who self-reported having had AN at any point in their lifetime. Prospective participants under the age of 18 were recruited only if parental permission was obtained. Recruitment was conducted from May 2013 to July 2016 by public appeal through networks from professional organisations (e.g. Australia and New Zealand Academy for Eating Disorders), press conferences, conventional media (newspaper, radio and television), promotional materials distributed through eating disorder clinics, mailouts to discharged hospital patients who had a diagnosis of AN, conferences and support groups, social media (Facebook, Twitter and blogs) and word-of-mouth. These were supported on several occasions by public relations campaigns, either nationally or in targeted geographic areas, and public lectures. These recruitment methods were not designed to generate a population cohort that is either random or population-based, as these are not requirements for GWAS. Rather, they were designed to preferentially attract prospective participants to the study who are most likely to meet case criteria.
Instrument
The online questionnaire used was adapted from the Structured Clinical Interview for DSM-IV, section H Eating Disorders (SCID-H for Diagnostic and Statistical Manual of Mental Disorders [4th ed., text rev.; DSM-IV-TR]) (First et al., 2002). A total of 65 items were included in the questionnaire, but as this was branched, not all participants answered all items. The initial items focussed around case criteria, as outlined in Table 1. Other items concerned binge-eating behaviours, methods of weight control and the presence of amenorrhoea during episodes of low weight. Amenorrhoea is not a diagnostic criterion for AN under Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) (American Psychiatric Association, 2013) and was not required for participation in the study. The final section of the questionnaire included extra items not adapted from SCID-H, regarding medical care and treatment for the participant’s eating disorder, and how the participant was recruited to the study. Ancestry data were requested from all participants meeting AN case criteria. Six ancestry categories were provided for response (European, Middle Eastern, Asian, African, Pacific Islander, South American), with participants able to provide up to two ancestries for each grandparent.
Criteria required to qualify as AN case. a
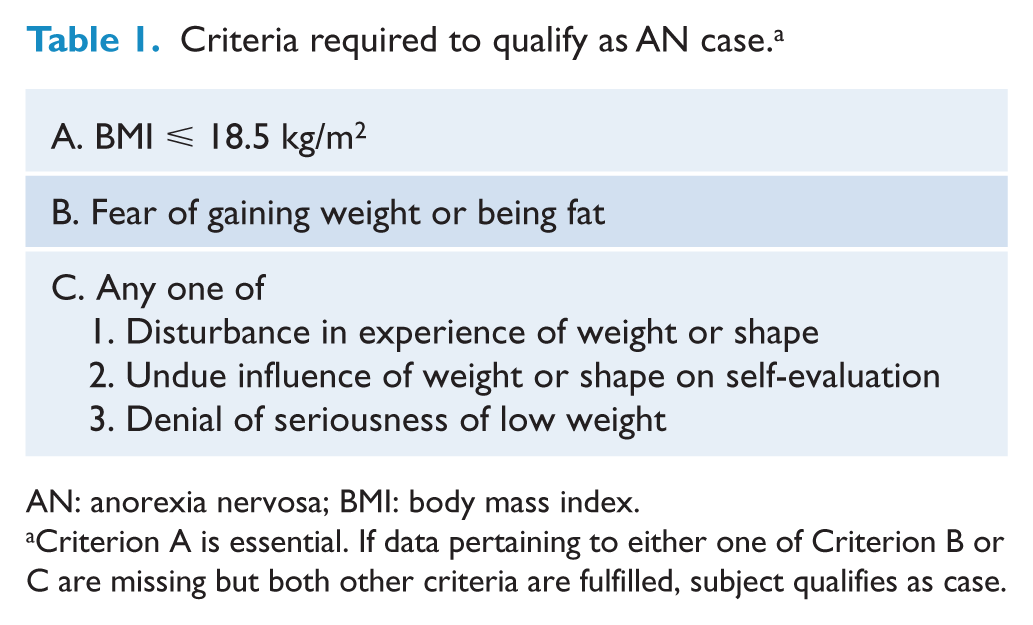
AN: anorexia nervosa; BMI: body mass index.
Criterion A is essential. If data pertaining to either one of Criterion B or C are missing but both other criteria are fulfilled, subject qualifies as case.
Data collection
Participants were invited to access the study website for their country and complete the online questionnaire. In Australia, individuals meeting the criteria specified in Table 1 were then invited by email to provide a blood sample. A blood collection kit, containing 3 × 10 mL blood collection tubes with ethylenediamine tetraacetic acid (EDTA) anticoagulant, was sent to the participant. Study personnel contacted participants by telephone and/or email to facilitate and track the blood collection process through local pathology clinics. Blood samples collected at the pathology clinic were couriered within 48 hours to the laboratory using pre-paid satchels included in the collection kit. In New Zealand, eligible participants were contacted and face-to-face or video-call meetings were arranged to go through the study and to obtain witnessed consent. Once consent forms were returned, participants were posted blood kits which they took to their local phlebotomy laboratory for sample collection. An existing New Zealand-wide laboratory collection courier system was utilised to return the chilled samples to Christchurch where they were frozen, before shipping in batches to Australia.
Of the three 10 mL EDTA tubes collected per participant, two were de-identified and sent as frozen whole blood to the Rutgers University Cell and DNA Repository (RUCDR) in the United States, with the remainder processed and stored locally. For a small number of Australian study participants unwilling or unable to provide a blood sample, a saliva sampling kit was posted to them for return by pre-paid post.
Since the relative effectiveness of a range of participant recruitment methods was of interest in this study, particular attention was paid to the categorisation of information sources nominated by participants as being involved in their recruitment. Participants were classified as having been recruited by ‘online news’ if they provided a text-based response to the questionnaire item ‘How did you find out about this study?’ that included the term ‘online news’ or nominated a particular online news website. Similarly, responses were classified as ‘social media’ if they referenced Facebook, Twitter, blogs, LinkedIn or Tumblr. More generic responses such as ‘internet’, ‘online’, ‘website’ and ‘email’ were classified as ‘other online sources’. Similarly, participants who indicated that their recruitment occurred via an eating disorders interest or support group (e.g. Butterfly Foundation, Eating Disorders Association of New Zealand [EDANZ]) or eating disorders conference had their responses coded as ‘interest/support group’ and ‘conference’ respectively.
Data analysis
Data analysis for this study was performed using SPSS Statistics 22.0.0.0 (IBM Corporation, Armonk, New York) and Excel 2010 14.0.7166.5000 (Microsoft Corporation, Redmond, Washington).
Research ethics and participant consent
All participants provided informed written consent, including consent for publication of de-identified study results. For Australian participants, written consent was via online submission. Prospective participants younger than 18 years of age then completed a paper questionnaire which required co-signature by a parent/guardian. New Zealand participants completed a paper-based consent form, which for prospective participants under 18 years of age required parent/guardian co-signature. Ethical approval for the Australian component of the study was provided by the QIMR Berghofer Human Research Ethics Committee. Ethical approval for the New Zealand component of the study was provided by the Health and Disability Ethics Committee of the New Zealand Ministry of Health.
Results
Participants meeting lifetime AN case criteria
Lifetime AN case criteria (Table 1) were met by 3414 Australian participants (average age 32 years; standard deviation [SD] = 13 years) and 543 New Zealand participants (average age 34 years; SD = 14 years). A total of 3348 Australian participants and 537 New Zealand participants met all three case criteria. A further 66 Australian participants and six New Zealand participants qualified as cases although they had missing data for criterion B (fear of gaining weight), but qualified for criteria A (body mass index [BMI] ⩽ 18.5 kg/m2) and C (disturbance in experience of weight or shape, undue influence or weight or shape on self-evaluation, denial of seriousness of low weight). No participants qualified as cases with missing data for criterion C.
The majority of study participants meeting lifetime AN case criteria came from New South Wales, followed by Victoria, Queensland, New Zealand, Western Australia, South Australia, Australian Capital Territory, Tasmania and Northern Territory. The highest lifetime AN case study recruitment rates (per 100,000 population) were observed in Australian Capital Territory, Queensland and Tasmania (Figure 1).
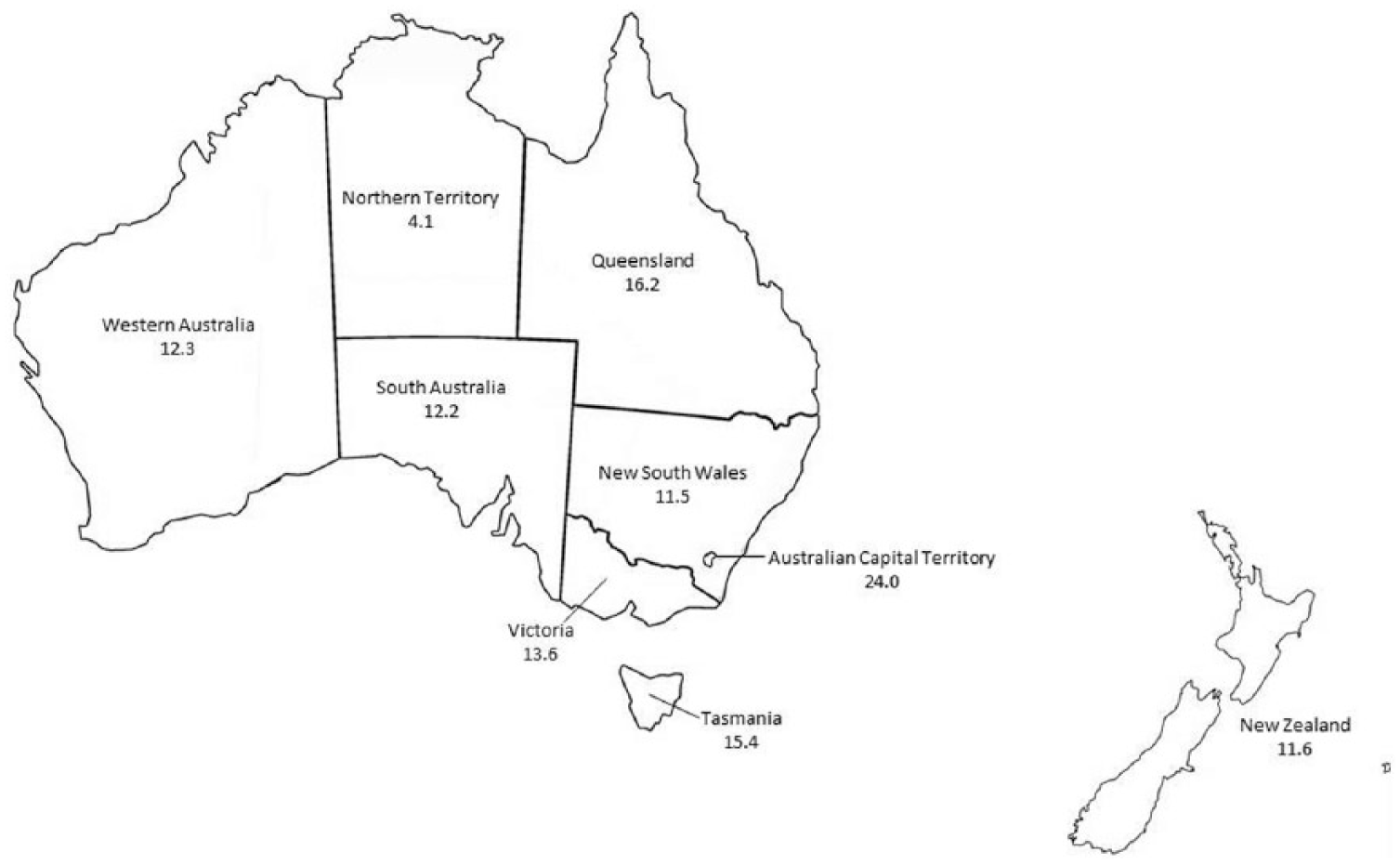
ANGI study registration rate per 100,000 population. Population estimates as of March 2016 for Australia (Australian Bureau of Statistics, 2016a) and June 2016 for New Zealand (Statistics New Zealand, 2016b).
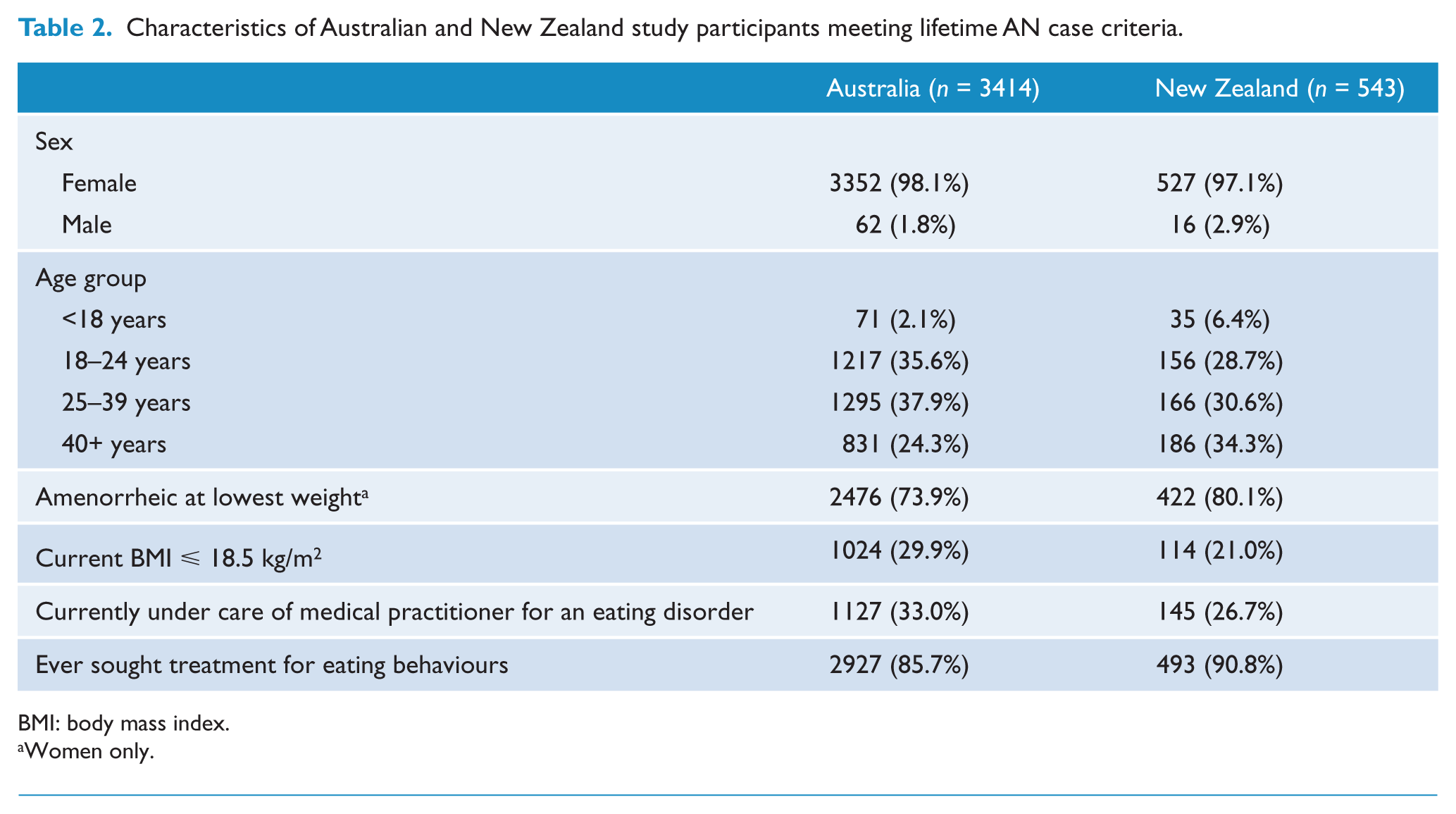
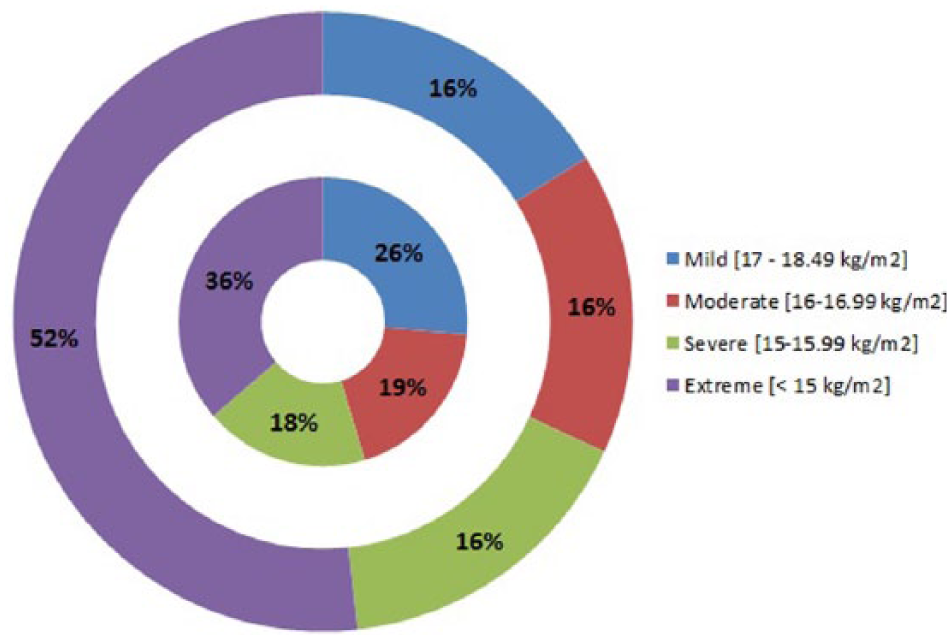
The average BMI at the time of the questionnaire was 20.3 kg/m2 (SD = 3.7 kg/m2) for Australian participants meeting lifetime AN case criteria, and 20.9 kg/m2 (SD = 3.7 kg/m2) for New Zealand participants meeting lifetime AN case criteria. The average lowest adult BMI for participants meeting lifetime AN case criteria was 16.6 kg/m2 (SD = 3.4 kg/m2) for Australian participants, and 14.9 kg/m2 (SD = 2.0 kg/m2) for New Zealand participants. Other characteristics of participants meeting lifetime AN case criteria from each country are shown in Table 2. Figure 2 shows the distribution of AN severity for participants meeting lifetime AN case criteria as adults, according to DSM-5 criteria based on lowest BMI since age 18 (American Psychiatric Association, 2013) (mild is over 17 kg/m2, moderate is 16–16.99 kg/m2, severe is 15–15.99 kg/m2, extreme is lower than 15 kg/m2). On average, New Zealand participants meeting lifetime AN case criteria had lower minimum adult BMI than Australian participants meeting these criteria (
Characteristics of Australian and New Zealand study participants meeting lifetime AN case criteria.
BMI: body mass index.
Women only.
Severity of anorexia for AN cases using DSM-5 severity criteria based on lowest BMI since age 18 (AN cases ⩾ 18 years only; 2581 Australian participants and 508 New Zealand participants).
Methods of recruitment
Participants who completed the questionnaire were asked to report how they heard about the study, and were invited to select as many options as applied to them. Figure 3 shows the percentage of study recruitment nominations for each method by age group for people meeting lifetime AN case criteria for each country. Considerable variation existed across age groups; e.g., social media was most effective in recruiting the 18- to 24-year age group, whereas broadcast and print media were common in the 40 years and over age group. For the participants who endorsed ‘friend/family member’ or ‘doctor or other medical practitioner’ as a source of information about the study, it is not possible to determine the primary method by which this referring individual learned about the study.
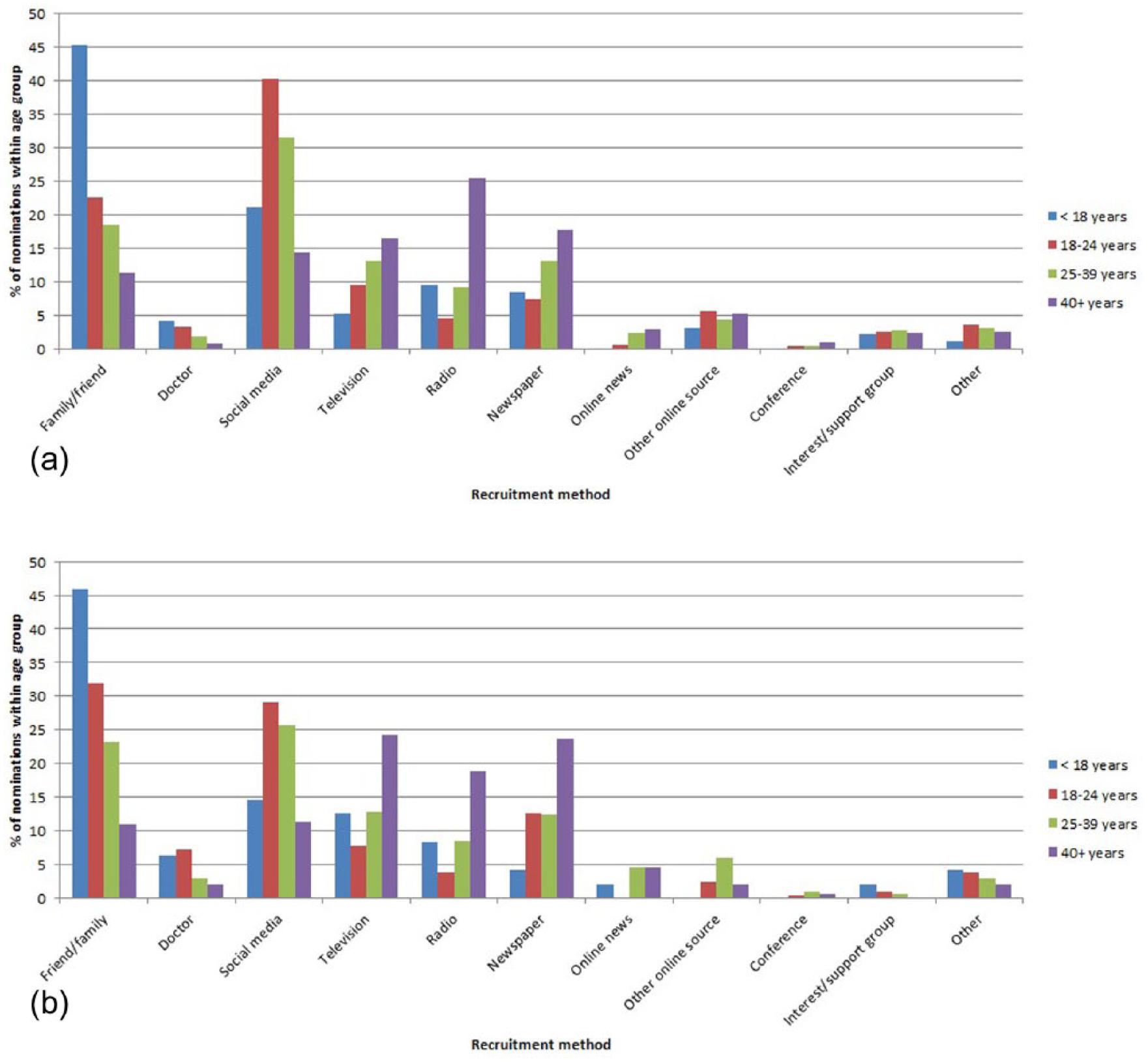
Recruitment methods nominated by participants meeting lifetime AN case criteria as having provided information about the study, by age group, for (a) Australia and (b) New Zealand.
Not explicitly shown in Figure 3 is the impact of public relations communications to boost study participation numbers. Figure 4 demonstrates the overall effectiveness and potential national reach of such campaigns, for the Australian component of the study only. The public relations campaigns conducted in May 2013, March 2015 and March/April 2016 were designed to reach the community by diverse communication methods, including conventional and social media channels. All targeted states and territories recorded increased participation immediately afterwards. The increase in participation in Queensland in April 2016 was boosted by a concurrent mailout of information about the study by Queensland Health to individuals who had been admitted to a Queensland hospital with a diagnosis of AN, and who had been discharged between 2007 and 2014.
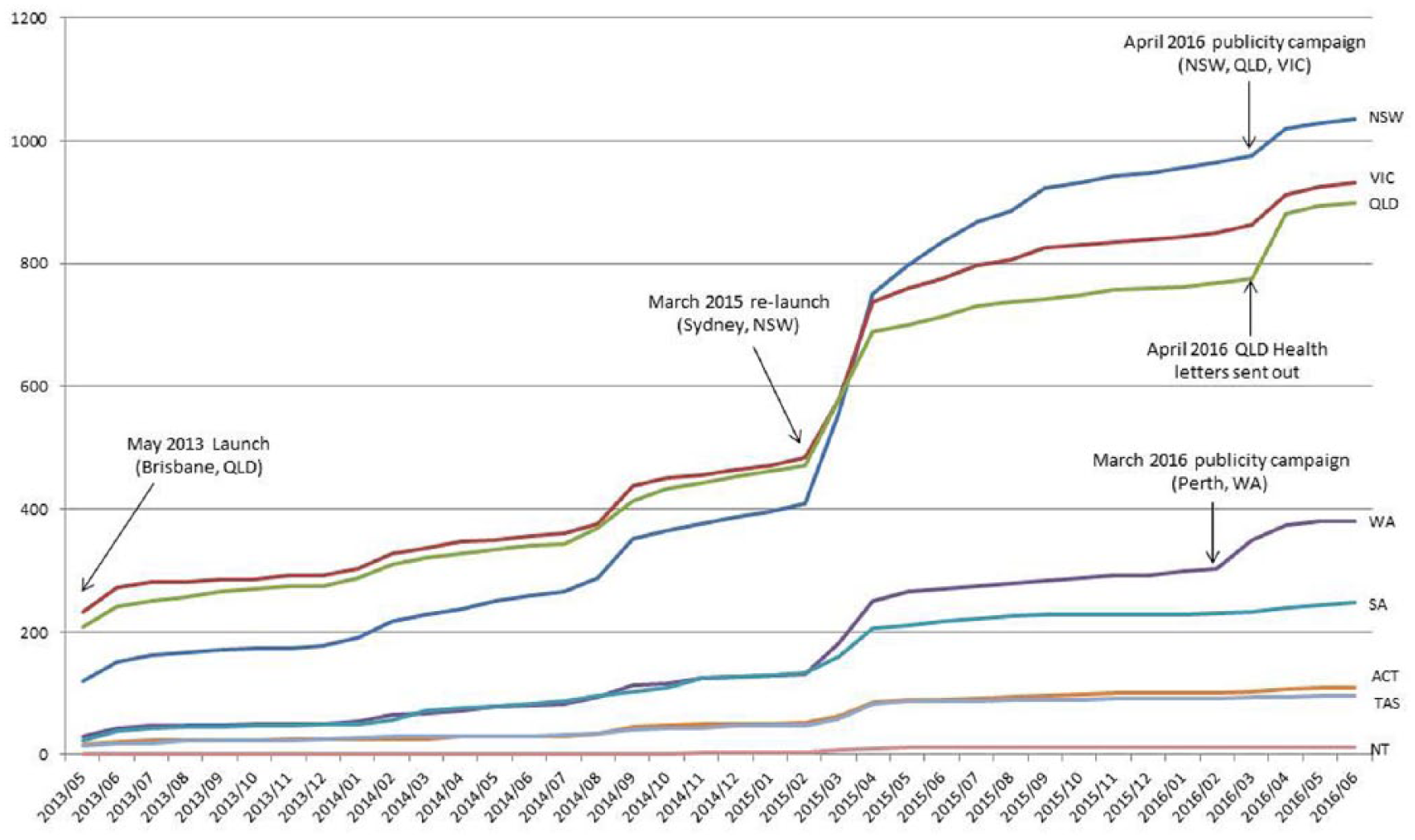
Questionnaires completed per state/territory of Australia.
For the Australian component of the ANGI study, 4638 people registered on the study website. Study retention rates across the various stages of the study (registration, questionnaire completion, meeting lifetime AN case criteria and providing a DNA sample) are shown in Figure 5. The lowest overall study retention rates were observed for the under-18 age group, with the major participation loss point being from study registration to questionnaire completion. The proportion of study participants meeting lifetime AN case criteria who returned DNA samples varied significantly by age group. Compared to participants in the 40+ age group meeting lifetime AN case criteria (in which 86% of cases returned DNA samples), participants meeting lifetime AN case criteria in the 18–24 age group (odds ratio [OR] 0.28, 95% confidence interval [CI]: [0.22, 0.35]) and the 25–29 age group (OR 0.44, 95% CI: [0.35, 0.55]) were significantly less likely to return DNA samples.
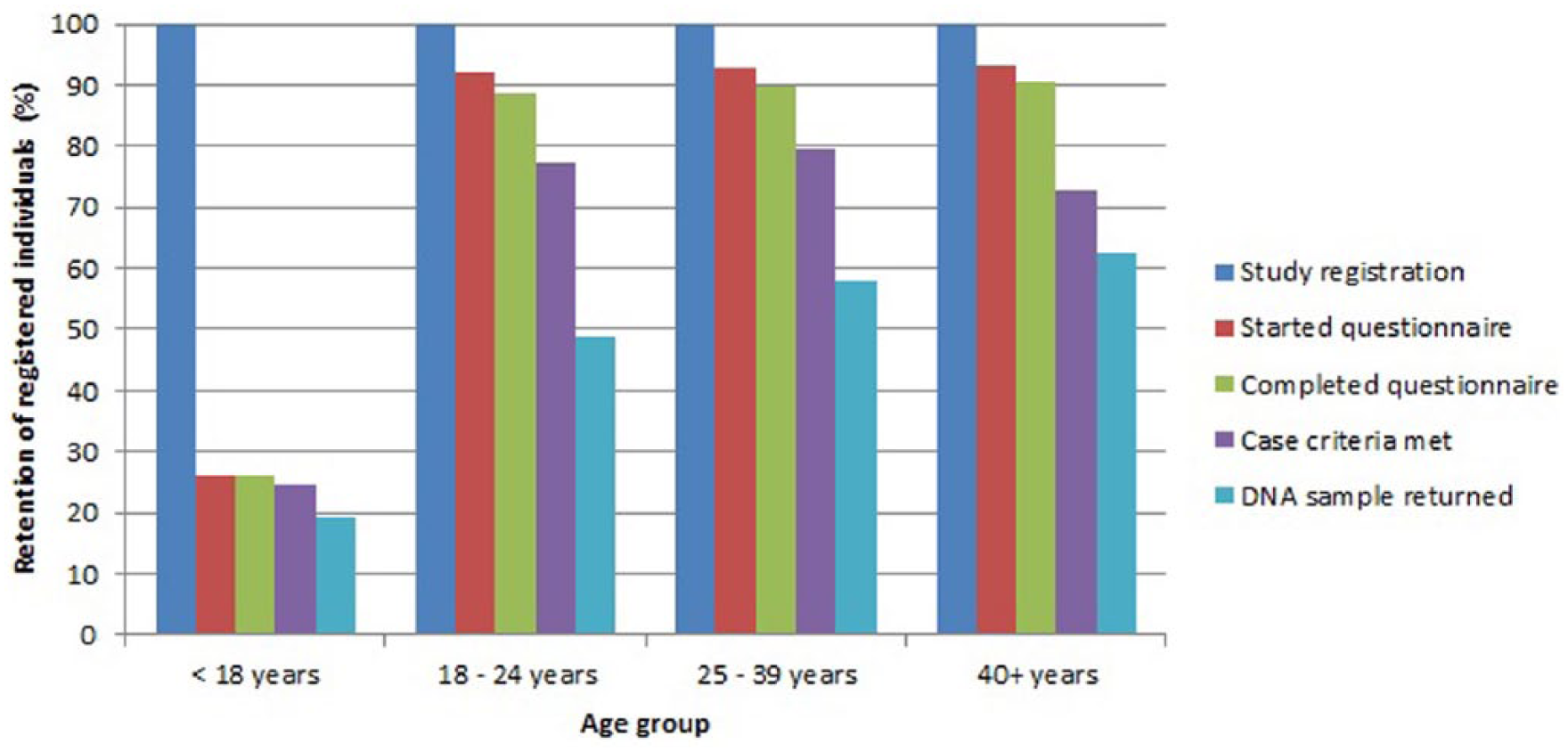
Study phase retention by age group for Australian component of study.
Overall, 2481 Australian participants who met lifetime AN case criteria provided a DNA sample (2469 blood samples, 12 saliva samples), and 543 New Zealand participants meeting lifetime AN case criteria provided a blood sample.
Ancestry
Full ancestry information (defined as ancestry information for all four grandparents) was provided by 2349 Australian participants (69%) and 490 New Zealand participants (90%) meeting lifetime AN case criteria. Partial ancestry information was provided by a further 109 Australian participants (3.2%) and 15 New Zealand participants (2.8%) meeting lifetime AN case criteria. Solely European ancestry was reported by 89% of Australian and 79% of New Zealand participants meeting lifetime AN case criteria who provided at least partial ancestry information. Other reported ancestry groups were Asian (Australia 5.3%, New Zealand 4.1%), Pacific Islander (Australia 3.5%, New Zealand 7.7%), Middle Eastern (Australia 1.6%, New Zealand 0.9%), South American (Australia 0.8%, New Zealand 0.5%) and African (Australia 1.0%, New Zealand 0.0%).
Weight control behaviours and binge eating
Figure 6 shows the prevalence of a variety of weight control behaviours (including exercise, fasting, self-induced vomiting and the use of diet pills and laxatives/diuretics) among individuals meeting lifetime AN criteria. The average age of onset for use of weight control methods by participants meeting lifetime AN case criteria is shown in Table 3. Exercise and fasting were the most utilised methods of weight control across all age groups in both countries, and these two methods were generally first employed at a younger age than the use of medications and self-induced vomiting. There were no differences between the Australian (reference group) and New Zealand cohorts in ever having used fasting (OR 0.90, 95% CI: [0.63, 1.28]), exercise (OR 0.98, 95% CI: [0.56, 1.70]) or self-induced vomiting (OR 0.90, 95% CI: [0.74, 1.08]) as a method of weight control. The use of diet pills was less common in New Zealand participants (OR 0.74, 95% CI: [0.62, 0.90]), while use of laxatives/diuretics was more common in New Zealand participants (OR 1.45, 95% CI: [1.21, 1.74]).
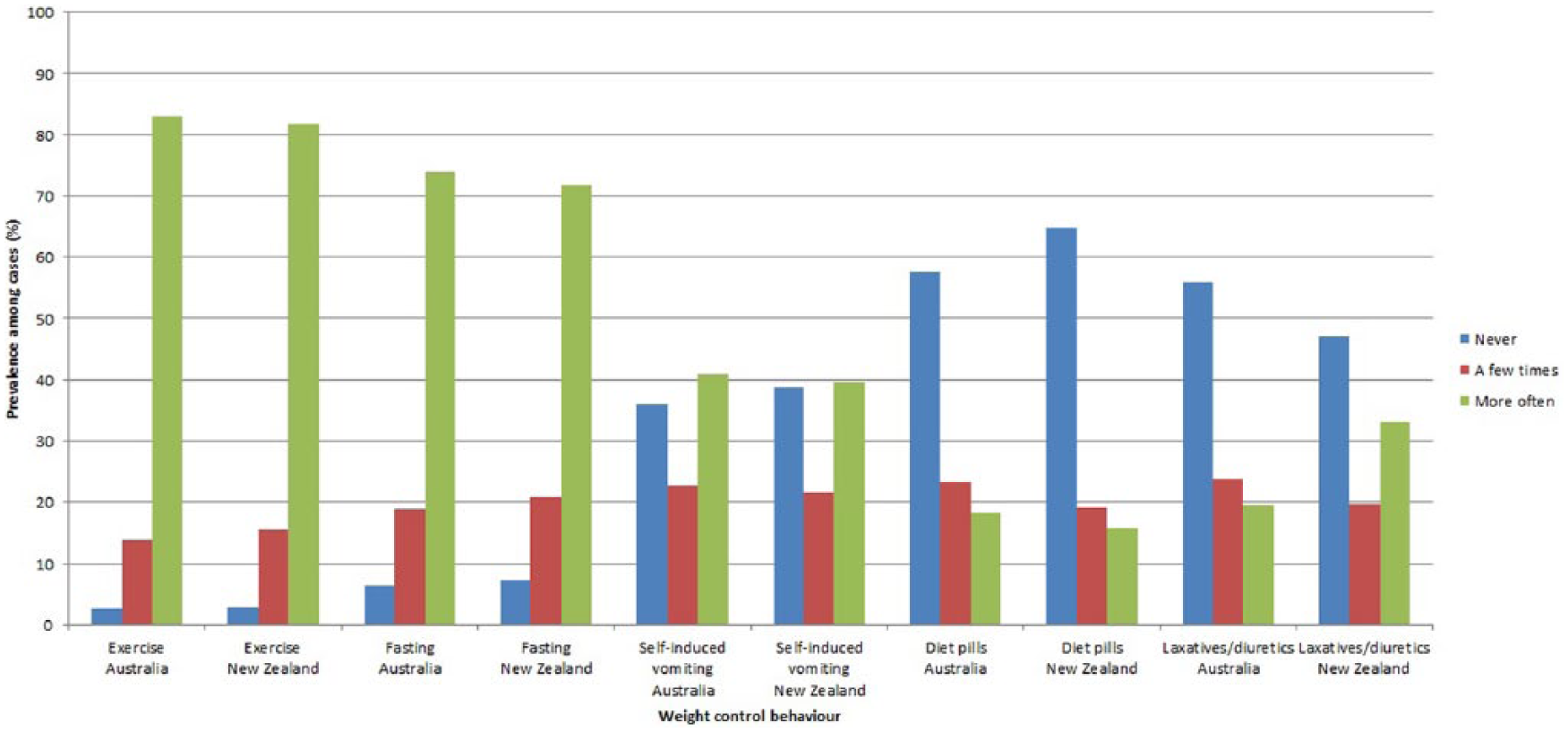
Prevalence of lifetime use of weight control behaviours among participants meeting AN case criteria in Australia (n = 3414) and New Zealand (n = 543).
Average ages of onset for weight control behaviours for participants meeting lifetime AN criteria.
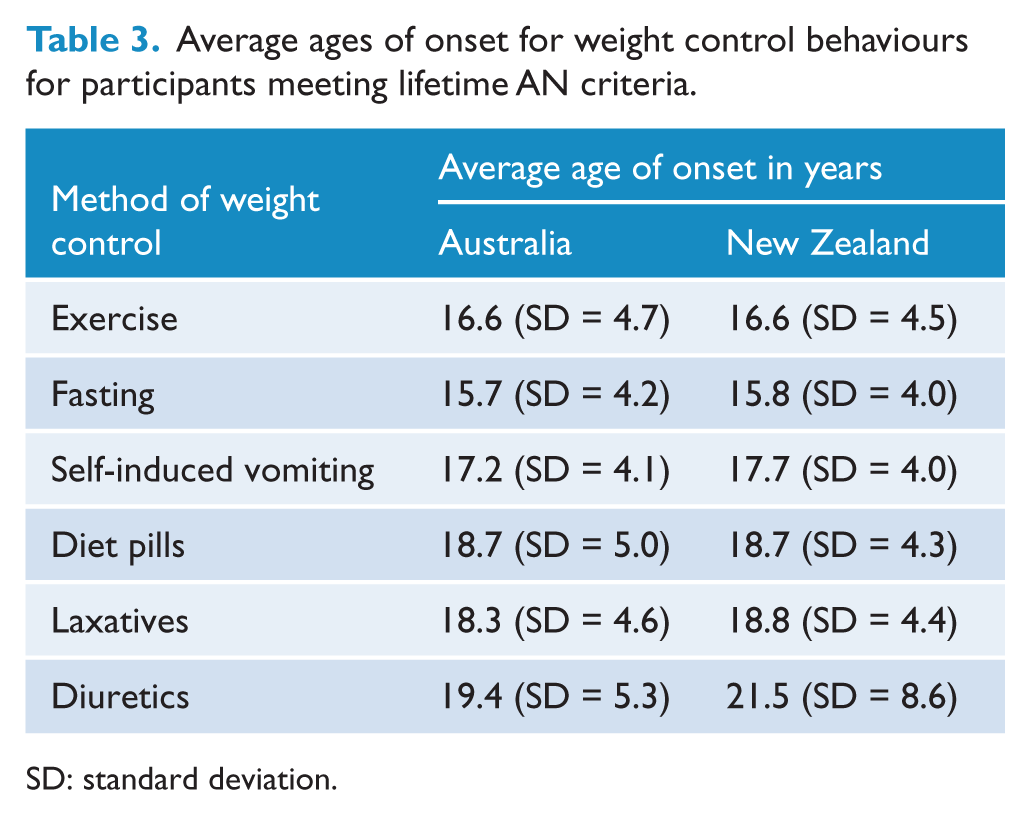
SD: standard deviation.
There was no observed relationship between method of weight control and DSM-5 severity criteria for lowest BMI in those over 18 years for Australian participants (fasting:
Professional medical treatment
Eating disorder treatment had been sought at some time by 86% of Australian participants and 91% of New Zealand participants meeting lifetime AN criteria, with the percentages for each category of treatment shown in Table 4. Participants could select as many treatment types as applied to them. Over half of the Australian participants meeting lifetime AN case criteria (1935; 57%) had received at least one of the four most common treatments (general practitioner, dietitian, outpatient treatment or specialised inpatient ward). Access rates for these treatments were higher for New Zealand participants meeting lifetime AN case criteria (OR 5.9, 95% CI: [4.5, 7.8]), with 481 (89%) having received at least one of the four most common treatments. Similar proportions of Australian (584; 17%) and New Zealand (93; 17%) participants meeting lifetime AN case criteria had received all four of these treatments at some time (OR = 1.00, 95% CI: [0.78, 1.27]). At the time of the study, 33% of Australian participants and 27% of New Zealand meeting lifetime AN case criteria were currently under the care of a medical practitioner for eating disorders. Significantly more individuals meeting lifetime AN case criteria who reported a current BMI < 18.5 kg/m2 (56% in Australia; 57% in New Zealand) were under current medical care for an eating disorder than those with a current BMI ⩾ 18.5 kg/m2 (23% in Australia, 19% in New Zealand).
Eating disorder treatments ever received by individuals meeting lifetime AN case criteria (more than one selection possible).
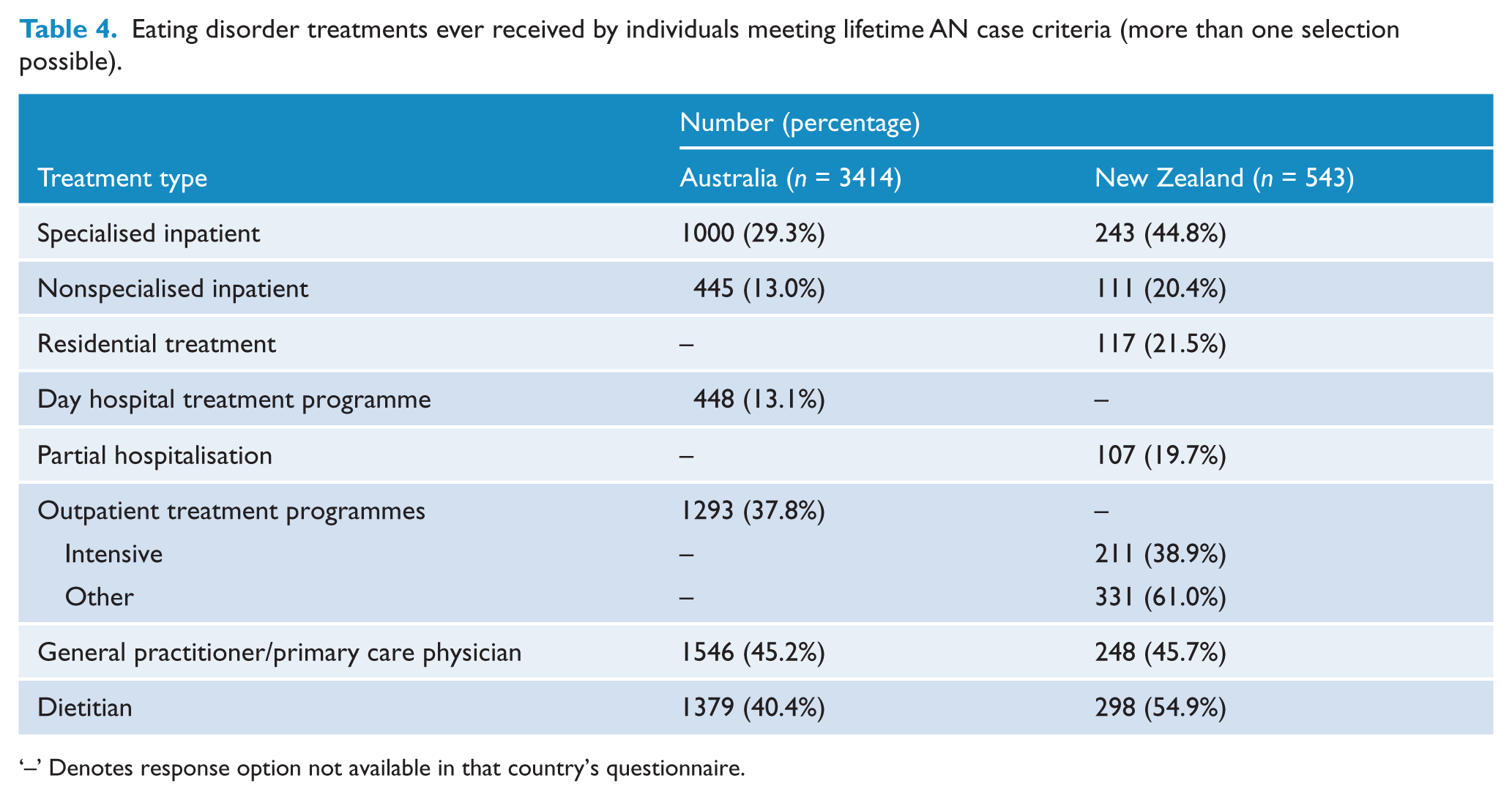
‘–’ Denotes response option not available in that country’s questionnaire.
Discussion
The present paper describes the characteristics of 3414 Australian and 543 New Zealand individuals meeting lifetime AN case criteria recruited for a GWAS to help unravel the genetic aetiology of AN. This is the largest sample from this region yet reported, and the recruitment success is likely to reflect the wide variety of study promotion methods across both conventional and social media platforms, and the high level of interest in the study demonstrated by those living with AN.
A key feature of this study is that it includes participants who met all AN criteria at the time of the study, as well as those in partial or full remission. An important interim finding of this study is that only 56% of people with lifetime AN with a current BMI less than 18.5 kg/m2 were under the care of a medical practitioner for an eating disorder at the time of the study. By comparison, a Finnish twin study (Keski-Rahkonen et al., 2007) found that approximately half of the people in their sample meeting lifetime case criteria had been previously detected in the health care system. Although the present study cohort is not epidemiologically representative, this result still indicates the importance of awareness, detection and intervention regarding weight control behaviours, especially given the young ages at which behaviours have potential to emerge.
There were few differences between the cohorts recruited from Australia and New Zealand. The average BMI values for participants at the time of the questionnaire were substantially lower than recent population estimates for women in both Australia (27.2 kg/m2; 95% CI: [27.0 kg/m2, 27.4 kg/m2]) (Australian Bureau of Statistics, 2015) and New Zealand (28.1 kg/m2; 95% CI: [27.9 kg/m2, 28.4 kg/m2]) (New Zealand Ministry of Health, 2015). New Zealand participants meeting lifetime AN case criteria had lower self-reported minimum BMI since age 18 than Australian participants, potentially indicating that the average AN severity in the New Zealand cohort was greater than in the Australian cohort. This may have occurred through differences in the recruitment strategies (or their effectiveness) between the two countries. Rates of ever having used particular methods of weight control (diet pills, laxatives and diuretics) also differed between the two cohorts. Again, this could be due to differences in study recruitment. However, it is noteworthy that the only methods of weight control displaying this difference are ones which require purchase of a medication. Therefore, the observed usage rate difference may reflect differences in availability or acceptance of these methods (now or in the past) between Australia and New Zealand.
In common with epidemiological studies (Fisher et al., 2001), the weight control methods of fasting and exercise had the earliest average ages of onset in this study. An Australian population-based study previously found driven exercise for the purposes of weight control occurring in over 50% of girls by the age of 14 years, with fasting occurring in 16% of female study participants of the same age (Patton et al., 1999). As in the present study, purging behaviours became more common in later teenage years, although the eating disorder symptom prevalence estimates were lower, possibly due to their sample not preferentially recruiting participants with AN. A study of New Zealand adolescent girls (Fear et al., 1996) aged 14–15 years has also previously found self-induced vomiting to be the most common purging method among that age group (12%) with use of laxatives, diuretics and diet pills being much less common (0.2–2.5%).
Treatment provided by general practitioners and dietitians was among the most common types of professional treatment received by participants in our study. This highlights the importance of providing relevant training to these groups in identifying and treating those with eating disorders. The percentage of Australians meeting lifetime AN case criteria who had received treatment was lower than that observed among New Zealanders meeting the same criteria. This could in part be due to geographical differences, with New Zealand having a higher average population density (15.8 people per km2 as compared to 3.1 people per km2 in Australia) (Australian Bureau of Statistics, 2016b; Statistics New Zealand, 2015). However, similarly high percentages of the two countries’ populations live in urban areas of 1000 or more people (Australian Bureau of Statistics, 2001), indicating that some of the differences may be due to relative availability of various types of services.
Our study has several limitations that should be considered. First, use of retrospective self-report data rather than clinical assessments may have affected the quality and accuracy of data collected, particularly with respect to recall of anthropometric measurements, age of symptom onset and use of weight control measures (Henry et al., 1994). Self-report height and weight have been previously shown to result in overall underestimate of BMI in a community sample (Fairburn and Beglin, 1994). However, studies of women with eating disorders have found that participants with AN tend to overestimate their body weight (Ciarapica et al., 2010; Meyer et al., 2009). A study comparing reporting methods for behavioural features of eating disorders found no statistically significant differences between interview and self-report measures of self-induced vomiting or laxative misuse in an AN patient sample, although a difference of marginal clinical significance was observed for reporting of laxative misuse in a community sample (Fairburn and Beglin, 1994). Second, low retention from initial registration to questionnaire completion was observed in this sample for prospective participants under the age of 18 years, as a result of requiring parental consent for participation. This is likely to have resulted in the experiences of younger AN being under-represented in the study sample. It is unknown whether the low rates of obtaining parental consent are due to parental objection to study participation, or young individuals being unwilling to discuss the study (and their disorder) with their parents; however, it is notable that the study participants in this age group nominated ‘family/friend’ as the most important source of study information. Third, this study has a low recruitment rate for male AN cases compared to local and international population-based estimates (Goodman et al., 2014; Hay et al., 2015; Qian et al., 2013; Yao et al., 2016). Study recruitment was not actively aimed towards males, for whom eating disorders are less well characterised (Strother et al., 2012). Fourth, the high percentage of participants who have sought eating disorder treatment at some time indicates that the sample is likely to be self-selected for treatment utilisation and/or severity of illness, as compared with population-based studies. Finally, the study recruitment methods used may have resulted in disproportionate recruitment from some geographical areas or ethnicities. Study participation rates from New Zealand and the various states and territories in Australia were not uniform, despite promotional campaigns being conducted out of some of the under-represented regions (e.g. New South Wales). Although the proportions of Australian study participants nominating non-European ancestries were broadly in line with Australian population estimates (Khoo et al., 2004), individuals nominating European-only ancestry may have been over-represented as compared with Australian census data. The New Zealand census collects ethnicity data rather than ancestry data; however, the results from the 2013 New Zealand Census (Statistics New Zealand, 2016a) (in which 61% of the population stated they had European-only ethnicity, and a further 9% of the population stated they had European ethnicity in combination with other ethnicities) indicate the potential for over-representation of individuals with European-only ancestry in the New Zealand cohort of this study as well.
The primary reason for participants not meeting case criteria in this study was self-reporting never having had a BMI less than 18.5 kg/m2. DSM-5 criteria for AN (American Psychiatric Association, 2013) include a requirement for a ‘significantly low body weight in the context of age, sex, developmental trajectory and physical health’, in recognition that normal weight range differs among individuals. Increasing numbers of individuals presenting with atypical AN (where all AN criteria are met except that significant weight loss has still resulted in a weight that is within or above normal range) have been noted in clinical practice (Sawyer et al., 2016), with findings that individuals with atypical AN may have physical and psychological morbidity as severe as individuals with full-threshold AN (Whitelaw et al., 2014). Recent research (Fairweather-Schmidt and Wade, 2014) has suggested that threshold eating disorders (AN, BN and binge-eating disorder) and other specified feeding and eating disorders (OSFED, including atypical AN) share a common genetic basis but possibly separate environmental influences. Further investigation of the aetiology of both AN and atypical AN is warranted (Hay et al., 2008; Sawyer et al., 2016). With the prevalence of eating disorders in Australia known to be increasing (Hay et al., 2008; Goodman et al., 2014), it is clear that continuing research into the causes of AN (e.g. ANGI) in the Australasian and international context is of significant importance.
Conclusion
This study has collated the largest sample of individuals with lifetime AN in Australasia to date, with the overarching purpose of finding genes which influence this severe disorder. Key findings relate to characteristics of lifetime AN in Australia and New Zealand, e.g., treatment-utilisation behaviours and age of onset of weight control behaviours. The study provides useful information relating to recruitment from the general population of eating disorder cases for GWAS and related studies.
Footnotes
Acknowledgements
We would like to thank VIVA! Communications for their efforts in promoting the study, and the Butterfly Foundation and June Alexander for their ongoing support of anorexia nervosa research in Australia, and EDANZ in New Zealand. Finally, we thank the women and men with anorexia nervosa for their participation in and support of our research.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Bulik is a grant recipient from Shire and has consulted for Ironshore. Warren Ward sits on an advisory board for Shire. Other authors declare that there is no conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a cooperative agreement from the Klarman Family Foundation to the University of North Carolina at Chapel Hill with a subcontract to QIMR Berghofer Medical Research Institute. A University of Otago Research grant was also used to fund some initial New Zealand samples.