
Abstract
Objective:
Is an increased focus on eating disorders during the past few decades reflected by increasing occurrence in the psychiatric health service system.
Method:
All first-time diagnoses of eating disorders identified in the Danish Central Psychiatric Research Register 1970–2008 constitute the present research database. Age-standardized rates per 100,000 inhabitants were calculated and autoregressive models were fitted for males and females separately as well as for in- and outpatients.
Results:
The incidence of eating disorders diagnosed in Danish psychiatric secondary healthcare has increased considerably during a nearly 40-year period of observation both within the general category of eating disorders and also specifically for anorexia nervosa. The steepest increase is seen within females aged 15–19 years, where the highest incidences are also found. Anorexia nervosa constitutes the vast majority of all eating disorders. Throughout the time interval investigated, the number of males, however, is negligible compared to females. Most patients are seen in outpatient services, increasing towards recent years. However, the number of patients being treated as inpatients has increased linearly through the entire four decenniums investigated.
Conclusions:
Changes in registration principles, public awareness and higher acceptance of mental disorders in the public is the most obvious explanation for the incidence increase of anorexia nervosa and other eating disorders. This study does not answer whether there has been an increase in true incidence in the population.
Introduction
During recent years, attention to eating disorders has increased, especially in western Europe and the United States, in the population as well as in the healthcare services.
Few studies have examined trends in the incidence of eating disorders over several decades from secondary healthcare in defined geographical areas. Lucas et al. (1991) investigated trends in the incidence of anorexia nervosa (AN) over 50 years in Rochester, Minneapolis, USA, finding an increase in incidence over time from 1935 to 1984 in females aged 15–24 years. The authors found this increasing trend to continue from 1984 to 1989 in a later study (Lucas et al., 1999). Similarly, Eagles et al. (1995) found an increase in incidence in northeast Scotland from 1965 to 1991, with a mean annual increase of 5.3%.
A study covering four decades (1956–1995) was published by Milos et al. (2004) describing a significant increase in the admitted incidence of severe AN during the 1960s and 1970s in a Swiss region.
Hsu’s review (1996) of literature published in the period 1985–1995, including case register studies, two stage studies, population studies and longitudinal studies, covering a 1935–1991 time span, concluded an increasing trend. Hsu concluded that eating disorders were more common in the 10-year study period in western cultures, though the rate was relatively low and may have reached a plateau.
Fombonne (1995) concluded in his review, including hospitalized cases as well as community surveys, that AN is a rare disorder with no evidence of an increase in incidence in the studies included, covering a period from 1931 to 1989. A recent review by Smink et al. (2012) includes some newer studies from primary as well as secondary healthcare up to the year 2000. They conclude a stable overall incidence rate over the past decades, but an increase in 15–19-year-old girls – the age group with the highest incidence.
A recent register-based study by Micali et al. (2013) found a stable incidence of AN in the UK from 2000 to 2009, although the overall incidence of eating disorders in general increased significantly.
Three nationwide incidence studies of AN and other eating disorders in secondary healthcare have been performed in Denmark – Nielsen (1990), Møller-Madsen et al. (1992) and Munk-Jørgensen et al. (1995) – since the electronic version of the Danish Central Psychiatric Research Register (DCPRR) was established in April 1969 (Mors et al., 2011; Munk-Jørgensen and Mortensen, 1997).
Nielsen’s study (1990) covered the period from 1973 to 1987 in a nationwide register study of psychiatric admission for AN in Denmark. The incidence for both males and females did not show any significant changes throughout the study period. The inclusion criteria were main and auxiliary AN diagnoses appearing for the first time, and the average incidence rate found for the period was 1.9 per 100,000 per year for females and 0.17 for males. The sex-specific incidence rates for the 10–24-year-olds were 6.8 per 100,000 per year for females and 0.6 for males. For females, the maximum incidence rates were in the 15–19 years group, whereas the males were younger with a maximum incidence among the age group 10–14 years. The study revealed a trend towards an increase of rates of diagnoses of AN in the context of psychiatric admissions.
Møller-Madsen et al. (1992) examined eating disorders in Denmark between 1970 and 1989, analyzing time trends for first lifetime admissions, using the main diagnoses of eating disorders (ICD-8: 306.50–59). The incidence of AN and other eating disorders was 0.42 in 1970, 1.36 in 1988 and 1.17 in 1989 per 100,000. In the 15–24-year-old females especially an increase was seen, where the incidence rose from 3.37 in 1970 to 11.96 in 1987.
Munk-Jørgensen et al. (1995) found an incidence of eating disorders in Denmark between 1970 and 1993. The incidence of all eating disorders, and specifically of AN, increased for females during the study period. This increase was most apparent in the age group 15–19 years. No significant changes during the study period were detected in the rates of incidence for males for all eating disorders in general or specifically for AN.
Overall, the three Danish studies of treated incidence on eating disorders thus show conflicting results. Møller-Madsen et al. (1992) and Munk-Jørgensen et al. (1995) found increasing incidence, whereas Nielsen (1990) found a constant incidence. These differences are most likely due to inclusion criteria which are broader in Møller-Madsen et al. and Munk-Jørgensen et al. than in Nielsen.
Aims of the study
The aim of the present study was to investigate if the increase in incidence of eating disorders previously shown in Denmark and internationally in secondary healthcare has continued in Denmark until recent years.
Methods
Design
The study is a register-based epidemiological study covering the entire of Denmark (5.5 million inhabitants) using data from the DCPRR (Mors et al., 2011; Munk-Jørgensen and Mortensen, 1997).
Sample
Data were extracted from the DCPRR (Mors et al., 2011; Munk-Jørgensen and Mortensen, 1997) and included all patients diagnosed with at least one of the eating disorder diagnoses listed in ICD-8 (Sundhedsstyrelsen (Danish National Board of Health), 1971) and ICD-10 (World Health Organization, 1992) from 1 January 1970 through 31 December 2008. Only main diagnoses were included. Diagnostic code, date of admission, date of birth and sex were registered for each person. In this report, we analyzed all eating disorders (ICD-8: 306.5x/ICD-10: F50.x) and AN, including anorexia nervosa atypical (ICD-8: 306.50, ICD-10: F50.0 and ICD-10: F50.1) separately.
A dataset was created including all patients admitted with one of the eating disorders as main diagnosis for the first time regardless of the number of previous admissions.
The International Classification of Diseases (ICD) is used in Denmark for diagnosing psychiatric patients. The current version is the ICD-10, implemented on 1 January 1994. ICD-8 was the official diagnostic classification system before 1994. ICD-9 was never implemented in Denmark.
Bulimia nervosa (BN) did not have a separate code in the ICD system until the ICD-10 version. In the ICD-8 version, the disease was included in the diagnostic code 306.58, defined as ‘other eating disorders’. This categorization limits the validity of estimating trends for the incidence of BN prior to 1994, which therefore has not been analyzed.
Statistics
General information about the Danish population was obtained from Statistics Denmark (Statbank (www.statbank.dk) data per 1.1.1974, 1.1.1984, etc).
The yearly rates of treated incidence were calculated per 100,000 person-years and standardized with respect to the age distribution of the general population for that year for males and females, respectively. To take the serial correlation of the standardized observations into account, an autoregressive model of order 1 was fitted for AN and all eating disorder diagnoses, for contacts of any type and inpatient contacts only, and for each sex separately. For the analyses of inpatient contacts, regression was performed for the years 1970–2008, while for contacts of any type regression was performed on data from 1995 to 2008 to take into account the fact that outpatient contacts were included in registers only from 1995. No further explanatory variables were used. The order of the autoregressive model was chosen based on plots of the partial autocorrelation function for each analysis (not shown).
The autoregressive regression used fits the model xt = φxt–1 + c. A φ close to 0 means that the influence on the present observation from the previous is small, and the estimates of number of cases will all lie close to the constant c. A φ close to 1 or −1 indicates that the correlation between two successive observations is large compared to the effect of the constant; the estimated number of cases will be almost solely dependent on the previous observation.
All analyses were performed in Stata 12.0 for Windows (College Station, TX: StataCorp LP, 2011).
Results
Figure 1 shows increasing age-standardized incidences for AN included as inpatients from 1970 through 2008. The curves for all eating disorders (not shown) follow the shape of the AN curves, but are higher in the diagram. The total sample of AN constitutes 77.9% and 76.7% of all eating disorders for males and females, respectively. The statistical specifications are shown in Table 1.
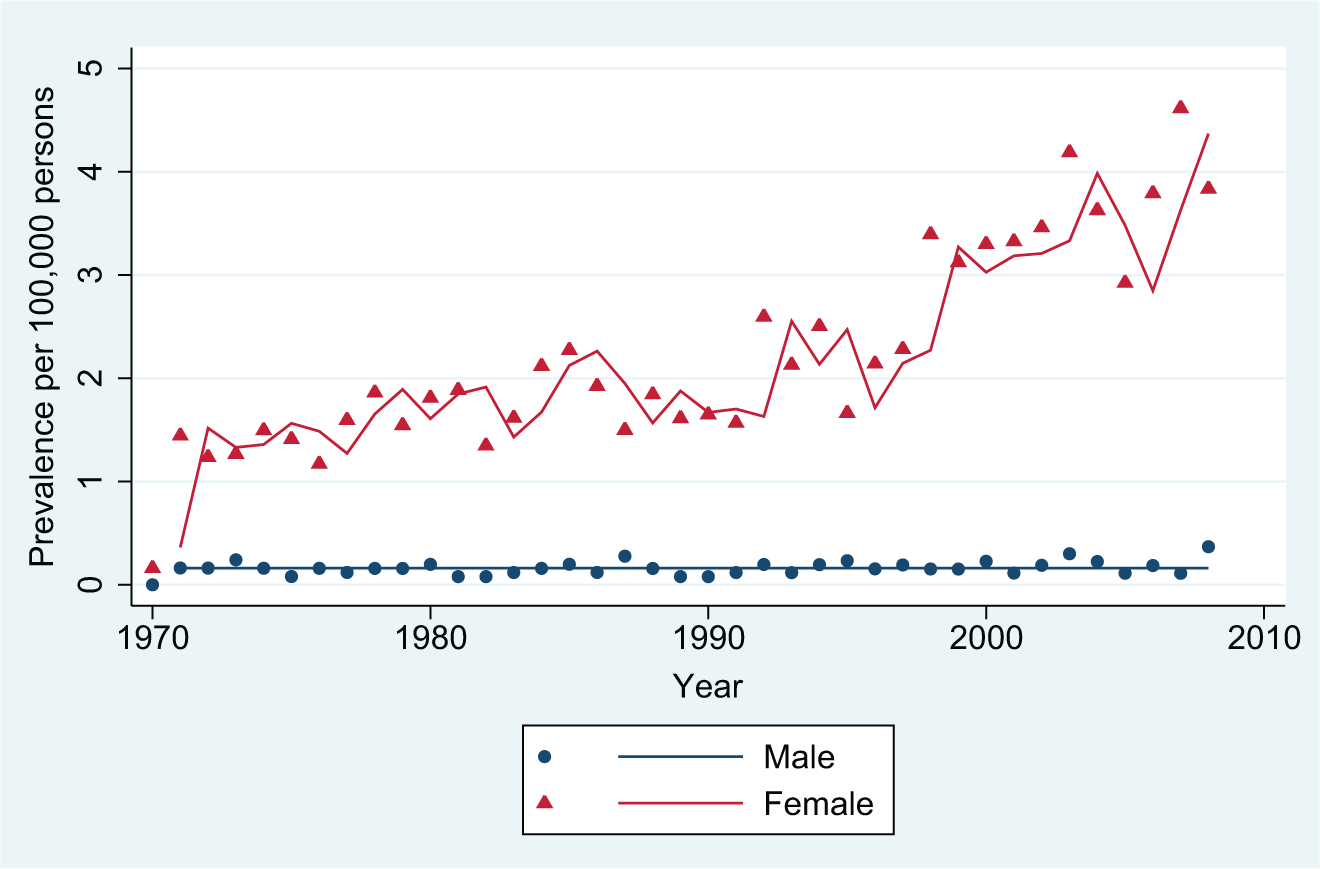
Inpatient incident contacts: anorexia nervosa.
Results of autoregressive regression per 100,000 people in the population.
EDs: eating disorders; AN: anorexia nervosa.
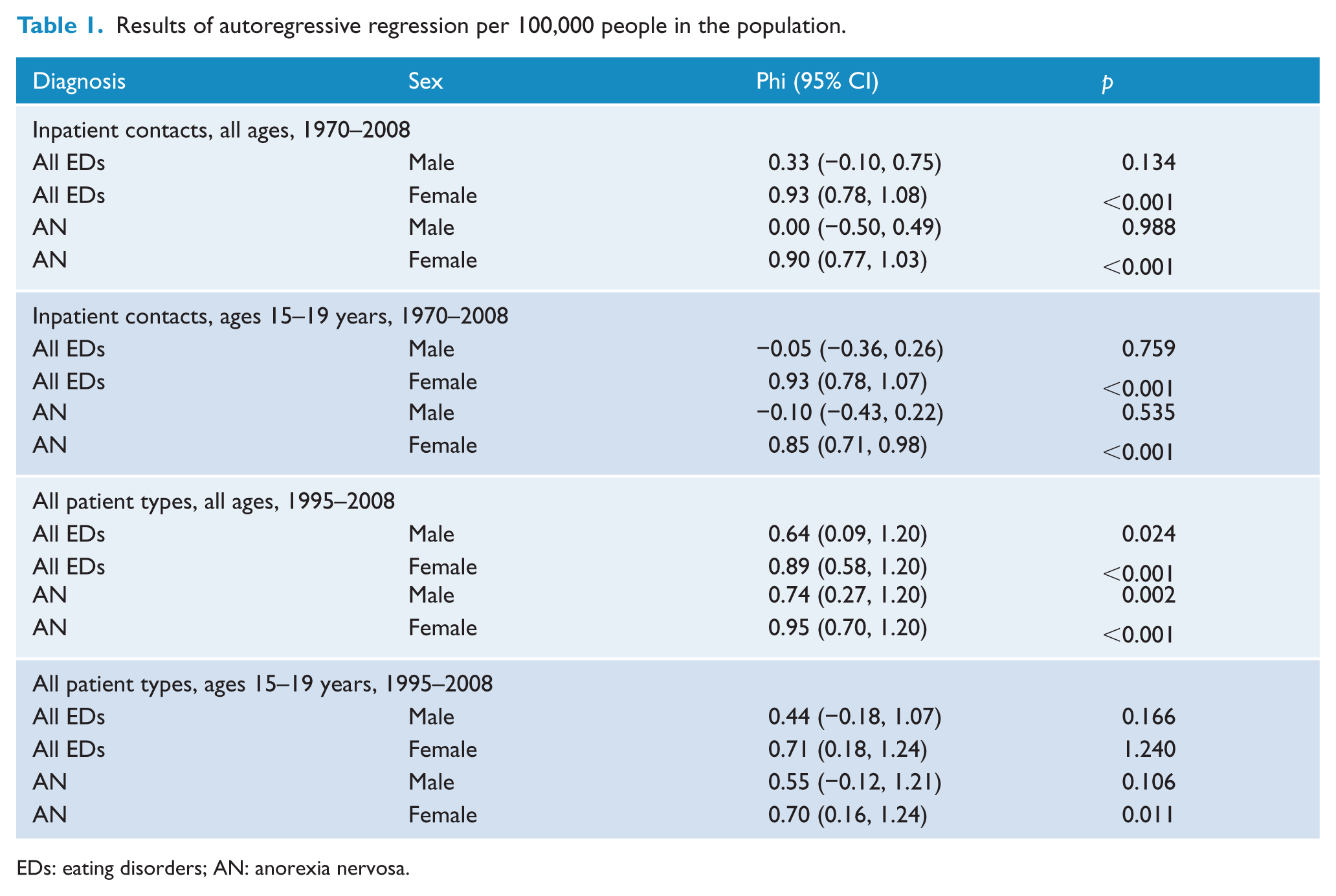
The highest incidences of AN inpatient contacts occur in the age group 15–19 years. Figure 2 shows the age-specific rates for this age group. The statistical specifications are shown in Table 1.
Inpatient incident contacts: anorexia nervosa, ages 15–19 years.
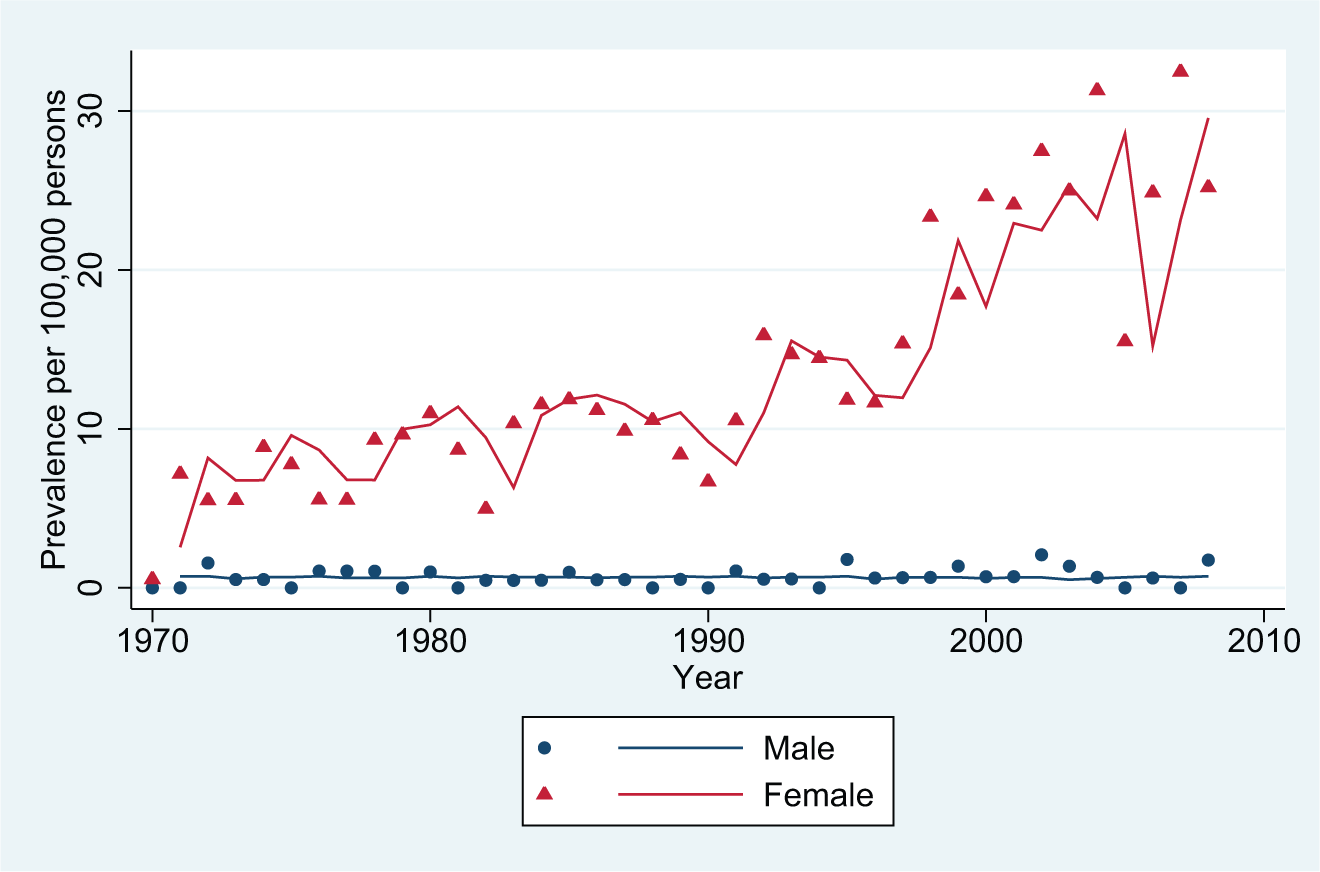
Figure 3 shows the incidences of AN over the period 1995 through 2008, now also including patients identified with a first-time diagnosis in connection with an outpatient treatment period which was registered mandatorily since 1995 (also, emergency visits are included, registered mandatorily since 1995). The first year of ICD-10, 1994, is not included in the analysis. The statistical specifications are shown in Table 1.
All types of incident contacts: anorexia nervosa.
As in Figure 1, we have not shown the curves for all eating disorders as they follow the shapes of the AN cases, constituting 51.3% and 45.3% of all eating disorders for males and females, respectively. The statistical specifications are shown in Table 1.
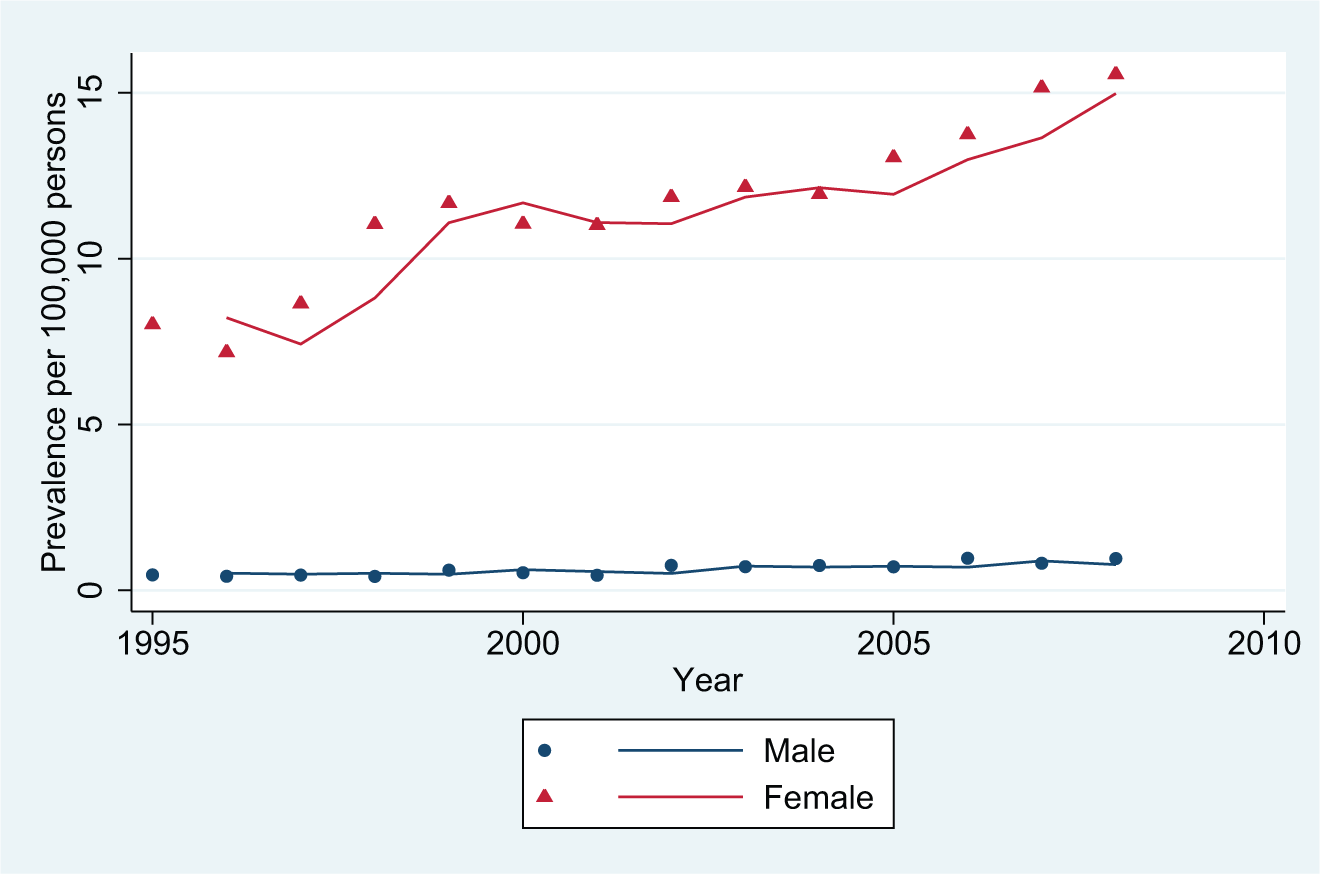
Figure 4 shows the age-specific incidences of AN as well as of all eating disorders for the age group 15–19 years. The statistical specifications are shown in Table 1.
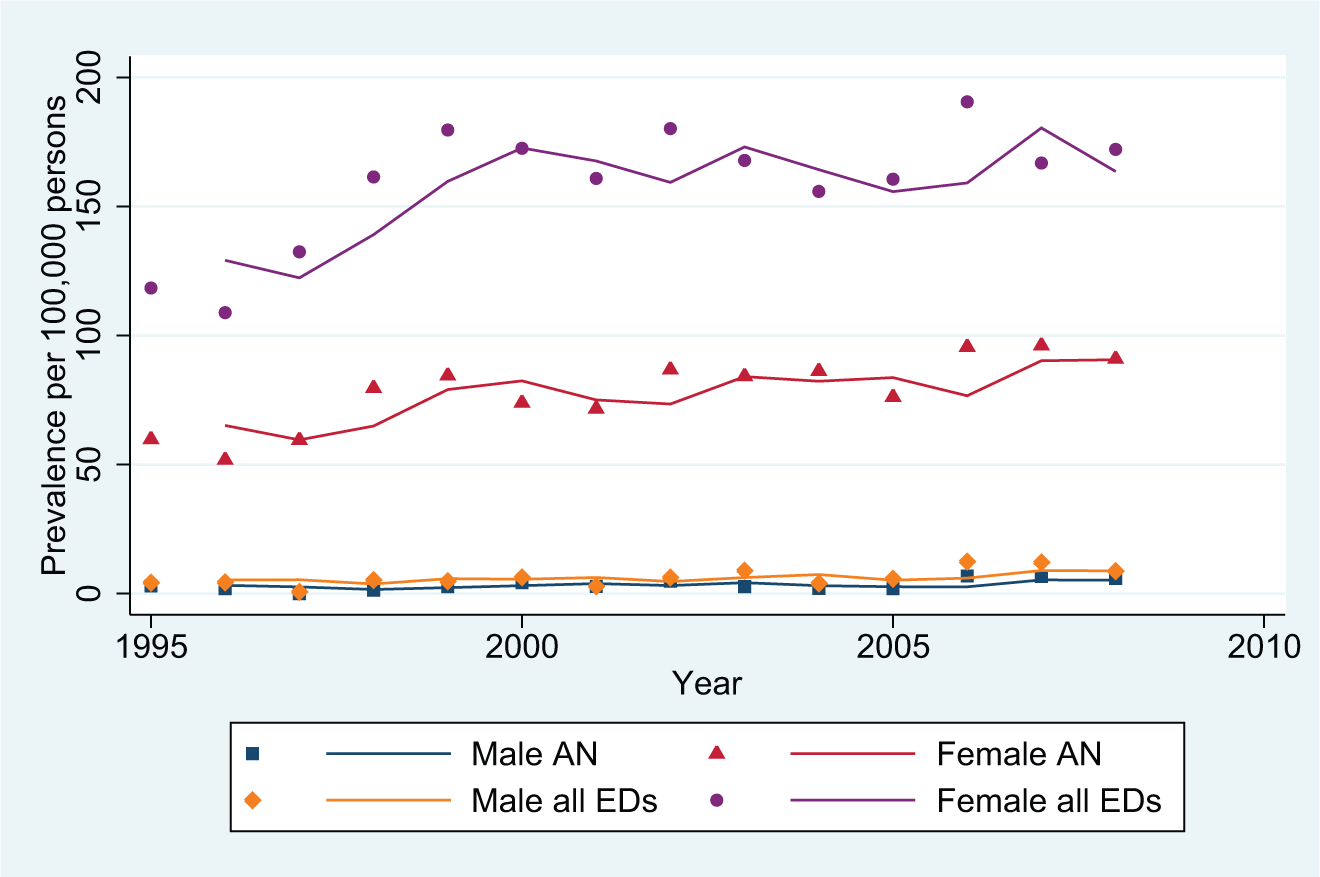
All types of incident contacts: anorexia nervosa and all eating disorders, ages 15–19 years.
Discussion
This study investigates the incidence of persons with eating disorders in the Danish secondary healthcare system as registered in the nationwide DCPRR for the first time. It is based on a national registry and shows that the treatment incidence for eating disorders has increased considerably during a nearly 40-year period of observation both within the general category of eating disorders and specifically for AN. These data capture admissions to psychiatric hospitals (outpatient and inpatient facilities), whereas patients managed in private psychiatric practice, general practice and in non-psychiatric settings were not included. The investigation covers the period 1970–2008. The study reveals a steep increase in females during the mid-years of the 1990s when, first, ICD-10 was introduced in 1994 and, second, registrations of outpatient visits were made mandatory by the Danish National Board of Health in 1995. The most prominent rise was registered for the age range 15–19 years.
Even though the study identifies an increase also in males, the level of increase is very low and not significant for inpatients. However, eating disorders in males deserves more attention in future research.
The diagnostic system changed in 1994 from ICD-8 to ICD-10, and on 1 January 1995 registration of all outpatient visits to the DCPRR became mandatory for all public psychiatric departments. These two organizational changes, the shift of diagnostic system and the mandatory registration of outpatient visits, cannot, however, fully explain the increase in treatment incidence. After the steep increase in 1994 and 1995, the annual incidence rate continued to increase steadily. If the 1994–1995 increase were due to the two organizational changes only, one would have expected the shape of the curve to continue with the same β as seen in the years up to 1994–1995, which is not the case.
Some further possibilities for explaining the increase arise: a genuine increase in the population of individuals with an eating disorder, a lower threshold for help-seeking, an increased severity of the disorders, and increased possibilities for entering into treatment together with an increasing awareness of impairment of quality of life in eating disorders (Mond et al., 2012). Among these, an increased awareness and a lower threshold seem to be the most plausible. An increased vigilance towards eating disorders in the 1980s may, as a time effect, have contributed to a subsequent rise of incidence in the 1990s. The number of publications concerning eating disorders and the more specific bulimia nervosa rose internationally during the 1980s (Theander, 2002). Several studies have described sharp rises of incidence for bulimia nervosa during those decades (Lucas et al., 1991) and it has been concluded that the rising public awareness has resulted in many more patients seeking help (Fombonne, 1995). This trend may be even more pronounced in our data due to the additional registration of patients in outpatient services to the registry. A similar pattern as seen in the increased incidence of eating disorders is seen in schizophrenia (Tsuchiay and Munk-Jørgensen, 2002) and in specific early onset psychosis (Okkels et al., 2013) and borderline state (Ørts Clemmensen et al., 2013). This general trend makes it less plausible that a genuine increase of eating disorders in the population should be the explanation. Rather it might be caused by increased public interest; for instance, the establishment of patient and relative organizations – a clear increase in media interest followed by political awareness.
Hay et al. (2012) conclude from their review of the literature that there has been limited progress in non-specialist treatment possibilities for AN. This, together with general awareness in the population and in primary care, may be an additional reason for an increasing number of eating disordered patients being referred to the secondary health service.
Other studies reporting an increased incidence of eating disorders have suggested that a more western and urban lifestyle may help in understanding these changes (Pavola et al., 2010). However, there is no reason to assume that lifestyles have changed very much in Denmark since 1990.
Moreover, the availability of psychiatric services has improved greatly in Denmark during the 40 years of observation. It is therefore difficult to tease apart the mere rise in incidence of eating disorders from a general increase of psychiatric treatment possibilities
Looking at these trends, however, as shown in non-published general data (Munk-Jørgensen, personal communication, 2013), reveals no parallelism. Rates of all first-contact inpatients to the psychiatric hospital system in Denmark decreased per 100,000 population between 1970 and 1993 (β = −5.517; 95% CI: −6.194, −4.839) for males as for females (β = −7.130; 95% CI: −7.769, −6.492). From 1995 to 2011 they both remain stable: males (β = 0.226; 95% CI: −0.548, 1.000) and females (β −0.333; 95% CI: −0.827, 0.160).
As the increase of inpatient-treated AN as well as all ED is significant over the total 1970–2008 period, we conclude, based on the lack of parallelism between AN/all ED and all first contacts, that the ED inpatient first-contact increase may not be explained (only) as part of a general trend in the populations’ use of psychiatric inpatient services.
Looking at all first contacts, no matter which diagnoses to Danish psychiatric services, including in- and outpatients as well as emergency ward contacts, we found a significant decrease in both sexes between 1970 and 1993 (when reporting outpatient visits was not mandatory and registration of emergency visits was not yet established). This was followed by a large increase between 1995 and 2011 among males (β = 11.675; 95% CI: 10.037, 13.313) as well as females (β = 7.658; 95% CI: 6.363, 8.952), indicating that the increase in AN/all ED may be part of a general increase in the use of psychiatric services, in particular outpatient treatments.
The increase in inpatient first-contact AN/all ED different from what is seen among all first inpatient contact may illustrate that AN/all ED are relatively serious and difficult treatable cases.
Strengths
The strength of this report is that it covers the hospital-based psychiatric service in the whole of Denmark over almost four decades. Further, it corrects for change in age distribution over time by analyzing age-standardized data. Otherwise, crude rates indicating changes in the number of patients with eating disorders over time could merely reflect differences in the demographic composition of a population as cohort effects (Fombonne, 1995; Williams and King, 1987).
Limitations
Being a register study, our findings have some limitations (Munk-Jørgensen and Østergaard, 2011). The diagnoses used are clinical diagnoses, not diagnoses given for research purposes and have not been validated in direct clinical examinations. The validity of diagnoses originating from the DCPRR, however, have been rather high in other diagnostic categories (Laurtisen et al., 2010), but no studies have specifically tested the validity of diagnoses of eating disorders in the Danish registry; however, one published study did report a manual crosscheck of a random and small sample (Vestergaard et al., 2002).
There is a high possibility for heterogeneity in how diagnostic criteria are used over the four decenniums the study covers. Also, geographical differences due to diverting cultures and tradition are the most important (Munk-Jørgensen et al., 2014). The ongoing changing of diagnostic principles, its international discussion and also that of the relevance of some diagnostic principles has recently been discussed by Hay (2013). Her arguments support our choice of analyzing only AN and all eating disorders without further sub-analyses.
Many cases with mild to moderate mental disorders are diagnosed and treated by general practitioners in Denmark and are thus not registered in the DCPRR. A proportion of patients with eating disorders are not treated by the psychiatric services and thus we suggest that the figures reported here still underestimate the treated incidence when aiming to include the whole spectrum of patients, ranging from mild to severe, in treatment for eating disorders.
Conclusion
With this national study based on data from a national registry, we report an increase of treated incidence both for all eating disorders and for AN. The age group with the steepest rise in incidence was girls between 15 and 19 years of age. Although the recording of health services information helps to understand trends for treatment incidence over time, we cannot rule out that changes in recording of the disorder in the registry, changes in diagnostic trends, availability of services and, finally, the increased vigilance of eating disorders among the public have all contributed to the findings presented here.
Footnotes
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.