
Abstract
Objective:
Many patients with anorexia nervosa develop an intractable and debilitating illness course. Our aims were to (i) conduct a systematic review of randomised controlled trials (RCTs) of treatment for chronic anorexia nervosa participants, and (ii) identify research informing novel therapeutic approaches for this group.
Methods:
Systematic search (SCOPUS plus previous reviews date 2011) of literature for (i) RCTs of treatment that included anorexia nervosa participants with a mean duration of illness of at least 3 years, (ii) studies reporting new treatments addressing factors associated with chronicity.
Results:
Evidence of efficacy for treatment approaches in severe and enduring anorexia nervosa is limited. Only one unpublished RCT designed to test a specific psychological approach for these patients was identified. There is a probable advantage for specialist psychotherapy over treatment as usual, and a promising study of relapse prevention with cognitive behaviour therapy (CBT) for anorexia nervosa (CBT-AN). Open trials have, however, reported developments in psychological therapies that warrant further specific evaluation. These include forms of CBT modified for anorexia nervosa, cognitive remediation therapy with emotion skills training, the Maudsley Model for Treatment of Adults with Anorexia Nervosa, the Community Outreach Partnership Program, Specialist Supportive Clinical Management and the approach of Strober with its emphasis on therapeutic alliance and flexible goals.
Conclusions:
Treatment trials need to move beyond targeting core eating disorder pathology (primarily weight restoration) and examine efficacy and effectiveness in minimising harm and reducing personal and social costs of chronic illness. There is also a need to develop better definitions of chronicity, with or without treatment ‘resistance’ specifiers.
Introduction
It has been said that ‘if there is one uncontroversial fact about anorexia nervosa, it is that only rarely does it resolve quickly’ (Strober, 2010). Anorexia nervosa is one of the earliest psychiatric conditions to be identified, with definitive accounts made in the 19th century by Gull (1874) and Lasègue (1873) expressing optimism about outcome following the re-feeding treatments of the time. Since then, whilst there have been many claims of successful treatment over the years these have lacked real evidence and beyond the clear need to reverse the starvation state, little research attention has been directed to clinical treatment trials in anorexia nervosa (Lock and Fitzpatrick, 2009). In addition, many patients fail to ever present themselves for treatment (up to 50% in one study (Keski-Rahkonen et al., 2007)), may appear to have had little benefit from treatment (Ben-Tovim et al., 2001), and develop a persistent course. A comprehensive review of 119 studies of 5590 people with a follow-up period of 1–29 years has reported that whilst a mean of 47% of people recovered (range 0–92%) and 34% improved (range 0–75%), 5% died and 21% developed a chronic eating disorder (range 0–79%) (Steinhausen, 2002). It is this group that is the focus of the present paper, namely those with severe and enduring illness, many of whom may have failed treatment.
Patients with severe and enduring anorexia nervosa have one of the most challenging disorders in mental health care (Strober, 2010). They have the highest mortality rate of any mental illness with markedly reduced life expectancy (Harbottle et al., 2008). At 20 years the mortality rate is 20%, and given the young age of onset this results in many young adults dying in their 30s, and a further 5–10% every decade thereafter (Steinhausen, 2002). Severe and enduring anorexia nervosa also imposes a heavy burden on health and other public services. Patients are often under- or unemployed, on sickness benefits, suffer multiple medical complications (renal, liver, cardiac failure and osteoporosis), have repeated admissions to general and specialist medical facilities, and are frequent users of primary care services (Birmingham and Treasure, 2010; Robinson, 2009). Furthermore, they pose a significant burden to parents and carers (Treasure et al., 2001).
Generally it is presumed that recovery and even meaningful symptomatic improvement in long-standing anorexia nervosa is less likely than in an anorexic illness with a shorter duration (NICE, 2004; Steinhausen, 2002). The poor treatment outcomes observed in patients with enduring anorexia nervosa are thought due to their extreme ambivalence about change and ego-syntonic attachment to maintaining low weight. A qualitative study (Arkell and Robinson, 2008) using in-depth interviews of 11 patients with anorexia nervosa of more than 10 years’ duration (mean age 37.7 years, SD 8, mean body mass index (BMI) 15.8 kg/m2, SD 2.0) identified five positive features of the eating disorder. These were interpersonal avoidance (e.g. ‘avoids having to cope with life’), intrapersonal avoidance (e.g. ‘avoids having to face feelings’), control (e.g. ‘I am disciplined’), sense of achievement, and self-punishment (e.g. ‘It’s like a self-destruct button and this has been what I wanted sometimes’). This counters any motivation to change despite recognition of the adverse effects of chronic illness on quality of life, extreme isolation, withdrawal and mood. In addition to poor motivation, Treasure and Russell (2011) have proposed a neurobiological explanation of the known poor outcome for family or individual therapy in adolescents with chronic illness of 3 or more years. They argue that combined effects of starvation and stress on the brain occur at a time when both structural (dendrite pruning and myelination) and functional development is occurring and the prefrontal maturation, important for executive function and emotion regulation, of later adolescence is impeded.
Current diagnostic schemes do not delineate severity and/or chronicity (Maguire et al., 2011) and the assumption of poor response to treatment in chronic anorexia nervosa is based on extrapolations from general longitudinal follow-up data, or clinical consensus, the latter of which is difficult to achieve (Tierney and Fox, 2009). Conclusions are also drawn from treatment outcomes in programmes devised for all patients but particularly those in the acute phase of anorexia nervosa (Steinhausen, 2002). This can lead to what may be unwarranted therapeutic nihilism in treatment and indeed debate as to the role, if any, of ‘palliative’ care for selected treatment-resistant patients. Previous systematic reviews of any therapies (Bulik et al., 2007), pharmacotherapy (Hay and Claudino, 2012), family therapy (Fisher et al., 2010) and psychotherapies in adults (Hay et al., 2003) have identified little robust evidence of effective treatments in anorexia nervosa, excepting that non-specialist ‘treatment as usual’ fares poorly compared to family therapy in adolescents (Fisher et al., 2010) (or specialised individual psychotherapy in adults (Hay et al., 2003)). In only one of these reviews were analyses of subgroup by chronicity reported to be possible, and this was for only one trial of family therapy (Eisler et al., 1997; Russell et al., 1987). In this trial patients who had regained weight with inpatient therapy were randomised to individual or family therapy. Randomisation was then stratified by illness onset and chronicity. As Treasure and Russell (2011) highlighted above, at 5 years both therapies were associated with a poor outcome in those with early onset and long duration of illness (over 3 years). This was in comparison to a better outcome for family therapy in the short-duration group.
In this paper we present the first results of a systematic review of randomised controlled trials (RCTs) of treatments for chronic anorexia nervosa participants. Our second aim was to identify research presenting information on putative novel approaches that address issues relevant to poor outcome. We have not included in the review literature pertaining to palliative care as this is an approach that is very rare, necessarily results in a poor outcome, and is controversial (Lopez et al., 2010; Starzomska, 2010). We refer interested readers to the text by Carney et al. (2006).
Materials and methods
For the purpose of this paper we conducted a SCOPUS search (date 1997 to August 2011) supplemented by reference list review of earlier systematic treatment reviews (Bulik et al., 2007; Fisher et al., 2010; Hay and Claudino, 2012; Hay et al., 2003) (search dates to 2007) to identify and evaluate published English language RCTs. Inclusion criteria were RCTs that included anorexia nervosa participants with a mean duration of illness of at least 3 years and that applied a standardised outcome assessment. Three years was selected as the duration beyond which response to treatment was poorer in the former identified trial (Eisler et al., 1997; Russell et al., 1987).
The search string ‘anorexia nervosa AND (treatment OR therapy OR psychotherapy OR pharmacotherapy)’ was applied. This yielded 3386 titles, of which a more detailed abstract and full-text search was conducted. In trials where the mean duration of illness was not specified, authors were contacted via email requesting this information. In trials where the mean duration of illness was greater than 3 years, authors were contacted for additional information including (i) the proportion of participants who had anorexia nervosa for at least 3 years, (ii) whether the results varied according to the duration of illness, (iii) if the results were available separately for those participants with anorexia nervosa for at least 3 years, and (iv) the proportion of these participants who had previously received treatment. Studies were assessed for risk of bias by two review authors (RS, PH). RCTs were assessed for adequacy of allocation concealment, randomisation method (sequence generation) and blinding.
Results
Randomised controlled trials that included participants with long-standing anorexia nervosa
A total of 11 studies (10 newly identified (Barbarich et al., 2004; Birmingham et al., 2004; Bissada et al., 2008; Dare et al., 2001; Fassino et al., 2002; Miller et al., 2011; Mondraty et al., 2005; Pike et al., 2003; Walsh et al., 2006; Whitney et al., 2012) plus the Russell et al. (1987) trial) summarised in Table 1 satisfied the inclusion criteria for our review. Nine authors replied to our email, and six were able to provide additional information. All but three studies (Barbarich et al., 2004; Birmingham et al., 2004; Whitney et al., 2012) applied DSM-IV (American Psychiatric Association, 1994) diagnostic criteria. Whitney et al. (2012) alone described their patients as treatment resistant, although in the Miller et al. (2011) study one participant with large weight gain was excluded from analyses and despite ongoing treatment from their usual care teams weight did not change for the remaining participants. Only two trials (Barbarich et al., 2004; Fassino et al., 2002) did not specify the method of randomisation and four (Bissada et al., 2008; Miller et al., 2011; Walsh et al., 2006; Whitney et al., 2012) specified adequate allocation concealment and all but Whitney et al., (2012) of these four specified blinding. In all but five studies (Barbarich et al., 2004; Birmingham et al., 2004; Dare et al., 2001; Fassino et al., 2002; Pike et al., 2003) reasons for non-completion were provided.
Features of randomised controlled trials that included participants with long-standing anorexia nervosa
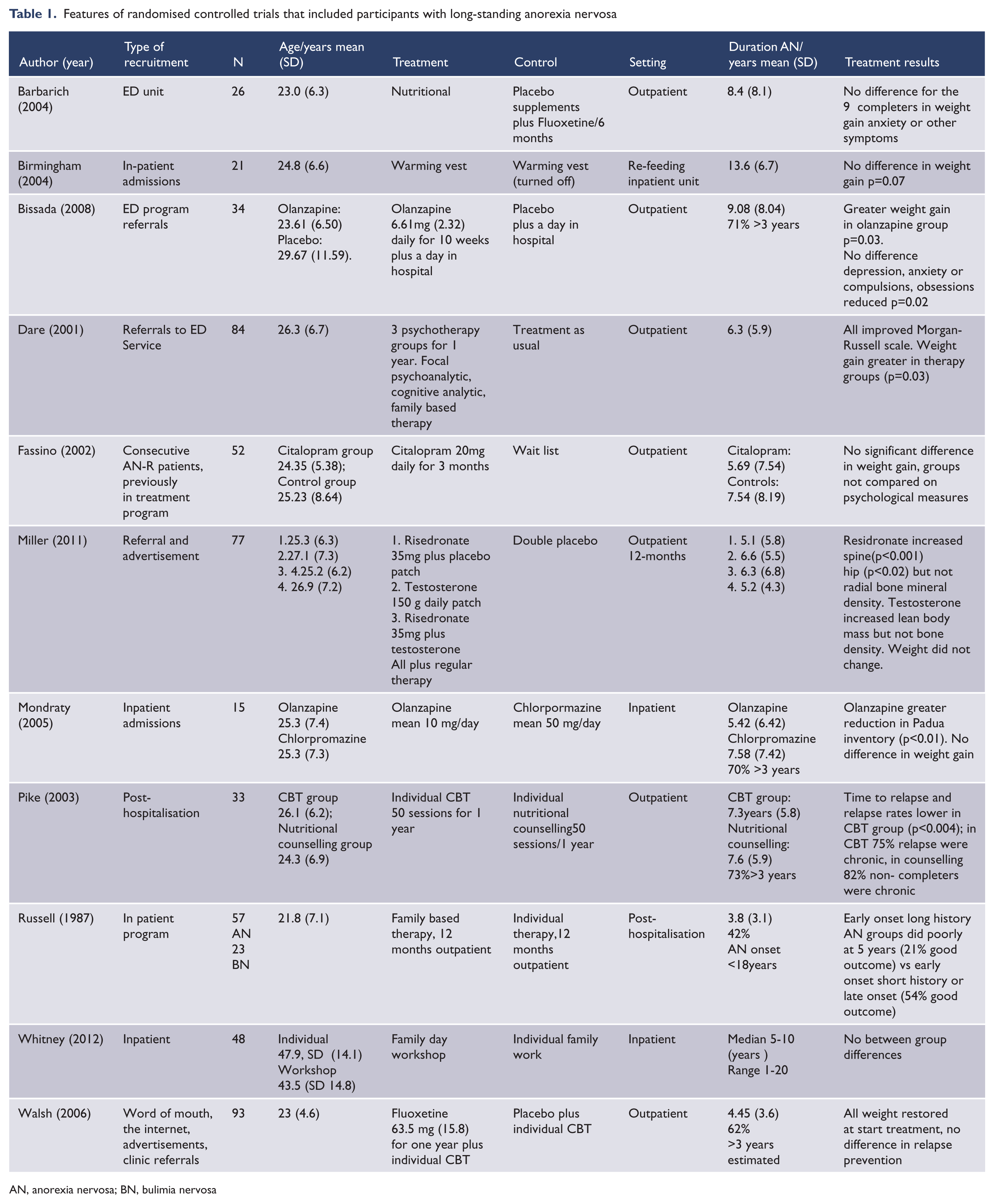
AN, anorexia nervosa; BN, bulimia nervosa
As shown in Table 1, we confirmed a majority of participants had illness duration of more than 3 years in only four of the 11 studies and no secondary data analyses were available. Information with regards treatment efficacy is thus limited. There is a possible adjunctive effect for olanzapine on weight gain and/or eating disorder psychopathology, a probable advantage for specialist psychotherapy over treatment as usual, a promising study of CBT for anorexia nervosa (CBT-AN) in prevention of relapse, and a promising study of residronate in improved bone mineral density. However, the quality of trials was variable and all require replication. There were no published trials specifically of treatment for long-standing anorexia nervosa and most outcomes were of those for acute illness, namely weight gain and/or reduction in eating disorder symptoms.
Case series and open trials of treatments for long-standing anorexia nervosa
The search also identified one case series of 13 treatment-resistant (mean duration of illness 6.3 years) anorexia nervosa outpatients which revisited a first-generation antipsychotic (Cassano et al., 2003), namely haloperidol. In this series significant eating disorder symptom improvements were found on the Eating Disorder Inventory and Eating Attitudes test, Clinical Global Improvement Scale scores and significant gains found in BMI. In addition, we found several more recent pertinent case reports and open studies of new psychotherapies being developed to address perpetuating factors for anorexia nervosa and treatment of the chronic patient. Relevant features of these are summarised on Table 2.
Features of psychological approaches that address barriers to change and/or symptom maintenance in severe and enduring anorexia nervosa. Therapeutic Domain and/or Psychopathology Addressed.
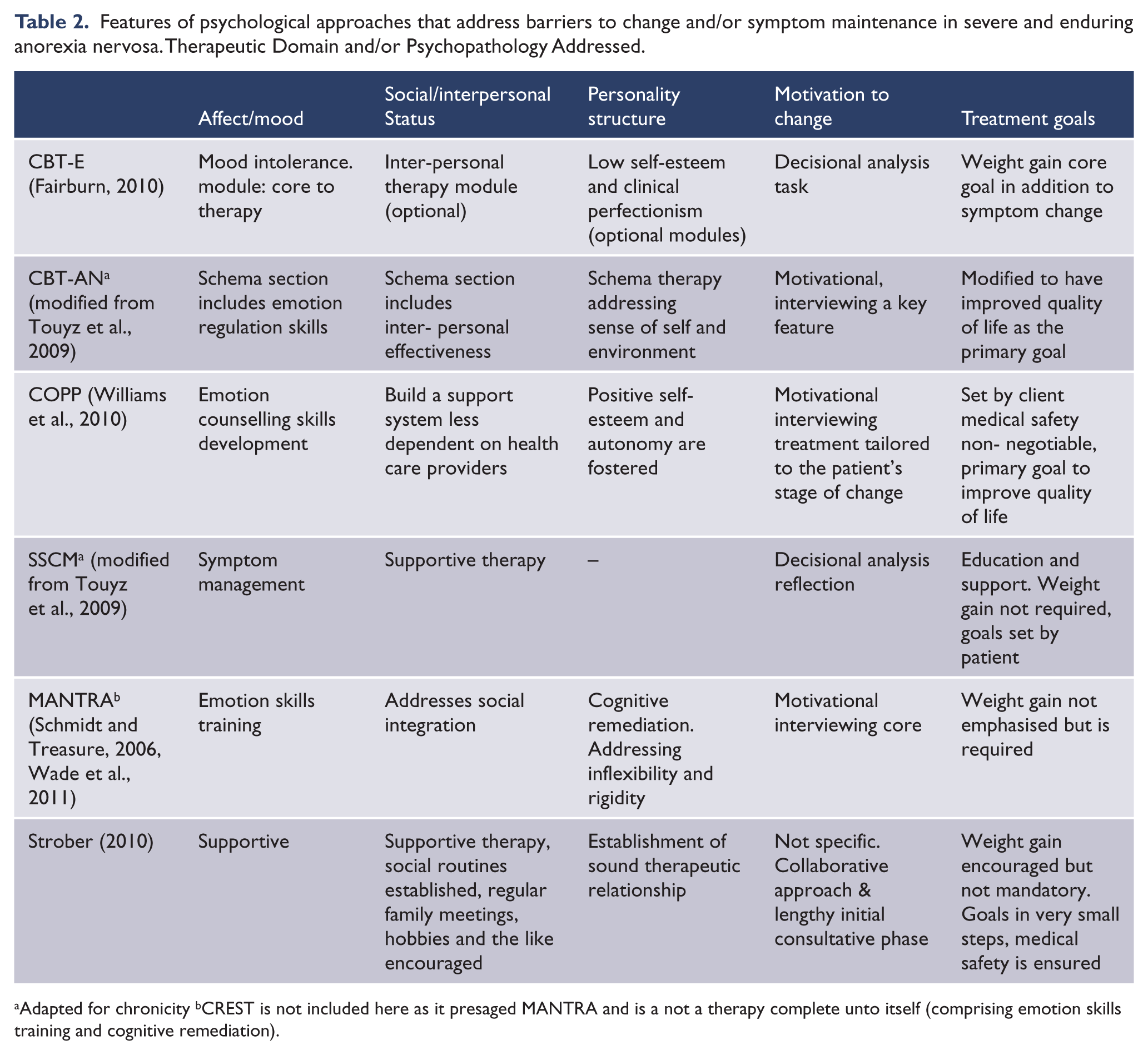
Adapted for chronicity bCREST is not included here as it presaged MANTRA and is a not a therapy complete unto itself (comprising emotion skills training and cognitive remediation).
The first of the novel psychotherapies that specifically addresses some issues of chronicity is the transdiagnostic cognitive behaviour therapy extended (CBT-E) (Fairburn, 2010), which has been tested in an open trial that included patients with long-standing anorexia nervosa (Byrne et al., 2011). CBT-E extends CBT for bulimia nervosa to include modules addressing predisposing and (more relevant to severe and enduring anorexia nervosa) perpetuating or maintaining factors for all eating disorders. CBT-E has an additional core module for management of mood intolerance, three optional modules attending to issues in interpersonal relationships, clinical perfectionism, and low self-esteem and a module on therapy to address issues of underweight and under-eating entitled ‘Underweight and under-eating’. The focus is more on behavioural change (and monitoring of behaviours that reinforce the ED psychopathology such as body checking), and motivational enhancement strategies (excepting a decisional analysis) are not emphasised. Monitoring weight is essential and CBT-E is prescriptive of calorie needs, use of energy-dense drinks to help achieve this, and a goal to ‘maintenance’ BMI of 19–20 with a weight gain of approximately 500 g per week for outpatients. It also recommends involving care-givers so that they help support the patient with all matters regarding food and eating in both psychological and pragmatic ways, e.g. cooking with the patient. The open trial included 34 (27.2% of sample) outpatients with anorexia nervosa with mean duration of illness of 7.79 years (range 0.5–59) (Byrne et al., 2011). Twelve completed treatment and six achieved full or partial remission.
Following the premise that cognitive capacity is adversely affected by chronicity, Davies and Tchanturia (2005) reported a case study of cognitive remediation therapy (CRT) in a 21-year-old female patient with more than 8 years of illness with inflexibility of thinking style. Treatment resistance was not specified. The patient was treated with ten 25-minute sessions over 4 weeks. This therapy was modelled on that developed for patients with schizophrenia (Delahunty and Morice, 1993) and was designed to improve executive functioning, in particular cognitive flexibility, working memory and planning skills. CRT was offered to the inpatient as an alternative to usual therapy in the ward (e.g. motivational and family work, CBT and cognitive analytic therapy). The patient continued to attend community groups, including occupational therapy of food preparation and reflexology. She demonstrated marked improvement in cognitive set-shifting skills as well as BMI gain from14.7 to 16.5. She commented that CRT had given her ‘.. a sense of achievement through positive encouragement from [the therapist], and increase in the ability to be more flexible…’ and ‘..an improvement of being able to multi-task, therefore enabling quicker and more flexible decision-making in everyday life..’ and ‘..accepting that it is OK to make less than accurate decisions, therefore reducing perfectionism in everyday life’.
The authors followed this up with a case series of 23 inpatients with long-standing anorexia nervosa (mean duration of illness 13.1 years) treated with CRT (sessions 45-min duration, twice a week). There were similar significant improvements in performance time of set-shifting tasks, reduction in perseverative errors in shifting tasks and improved performance on central coherence indices (Tchanturia et al., 2008). Whilst there were significant improvements in BMI, these did not correlate with changes in the neuropsychological tests and a previous study had found that weight gain alone without CRT did not lead to improvement in task performance (Tchanturia et al., 2004). The researchers have since expanded CRT to incorporate emotion skills training (CREST). CREST (Money et al., 2011) is a time-limited 10-session treatment package that primarily addresses emotion processing difficulties, one of the maintaining features of anorexia nervosa. CREST, like CRT, targets thinking styles, but also the recognition of emotions in the self and others, and includes strategies to manage emotions, and practice of emotion expression. In a case report of CREST therapy for a 19-year-old female with a 4-year history of repeated admissions the patient improved in regards to identifying emotions and using healthier emotion regulation strategies, as well as an increase in BMI and reduction in eating disorder symptoms (Money et al., 2011). CREST was proposed as a low-intensity intervention that might be used before proceeding to more comprehensive therapies such as CBT.
A further development following CREST with applicability to chronic illness is the Maudsley Model for Treatment of Adults with anorexia nervosa (MANTRA) (Wade et al., 2011). This addresses putative maintaining factors related to rigid thinking styles (i.e. perfectionism and obsessive-compulsive personality traits) and, as with CREST, the avoidance of strong emotion, pro-anorectic beliefs and responses of close others as well as elements of CRT (Schmidt and Treasure, 2006). It is a modularised treatment that maintains a focus on specific changes required in eating and weight within a motivational interviewing and CBT framework, including individualised case conceptualisation and summary letters from the therapists. Therapy is matched to the clinical symptoms, personality traits and neuropsychological profile of participants. Wade et al. (2011) reported a case series of 33 outpatients (82% completer) with long duration of illness 26% (n = 6) treated with MANTRA. In this series participants achieved a good outcome at 12 months with significant improvements in BMI, eating disorder symptoms and motivation to change. Treatment completers had mean duration of illness of 8.32 (SD 1.53) years. Duration of illness for those with a poor outcome was not significantly longer than those with a good or moderate outcome (9.65 versus 7.11 years, respectively).
Williams et al. (2010) have reported an alternate approach for patients with severe and enduring anorexia nervosa, namely the Community Outreach Partnership Program (COPP). The goal of therapy is to improve quality of life and minimise harm. Goals and pace of therapy are set by the client and the focus is on symptom management, skill development and understanding benefits and risks of symptoms. The therapy is set within the client’s community. Activities include emotion and nutritional counselling and there are ‘non-negotiables’ such as medical safety. Motivational interviewing is used to promote a therapeutic alliance that increases the patient’s self-awareness and self-acceptance, and places responsibility for change with the patient. In 18 patients with mean duration of illness 15.23 years there were significant improvements in eating disorder symptoms and BMI but not quality of life following a mean of 25 months of COPP.
COPP has commonalities with another promising therapy for severe and enduring anorexia nervosa, specialist supportive clinical management (SSCM) (McIntosh et al., 2006). SSCM was developed as a control therapy in an RCT where it compared favourably to CBT and to interpersonal psychotherapy (McIntosh et al., 2005). In this trial a chronic refractory course of anorexia nervosa was an exclusion criterion. SSCM has since been modified to be used in chronic anorexia nervosa (Touyz et al., 2009). In this form it aims to foster a therapeutic relationship that promotes adherence to treatment and, unlike its use in acute anorexia, it does not impose assumptions about change or argue for weight restoration. It includes education, care and support for changes that will improve quality of life and physical well-being. Hence the therapy may provide a therapeutic match to the chronic patient’s level of ambivalence, and a better match in general for a chronic illness where improvement in domains outside the core pathology can significantly affect patient well-being and disease burden. An RCT comparing SSCM to CBT-AN in patients with minimum duration of illness of 7 years and primary outcome of improved quality of life has since been conducted (Touyz et al., 2009), but results are yet to be reported. In this study modifications were also made to CBT-AN based on the premise that because patients with anorexia nervosa are extremely ambivalent about therapy and have starvation-related cognitive deficits, current change-oriented treatments may actually be counterproductive and give patients another experience of failure rather than being helpful. It was argued that CBT was developed first for an ego-dytonic illness, depression, and when adapted for anorexia nervosa it needs to account for its ego-syntonicity. Thus, unlike CBT-E described above, the CBT-AN manual in this trial allowed flexibility in approach and the motivational enhancement section of the manual continued as long as needed.
Strober (2010) has argued for a new therapeutic approach that resonates with the above and challenges the practice of treating all patients with anorexia nervosa with the same approach. In this ‘new kind of paradigm’ for chronic illness there is an emphasis on early treatment alliance and not hastening into a specific intervention, weight gain is not the principal objective, re-feeding is negotiated carefully and collaboratively. Nutritional improvement, however, is encouraged, routines of social activity are established, hobbies and pursuits encouraged, regular medical examinations done, and regular meetings are undertaken with family members and supportive others. He emphasises the professional challenge of working with these patients, the ability to ‘not require successes measured by patient progress…to face frailty and profound sickness with ease’ and therapists avoiding the ‘risks of treading too heavily on their (the patient’s) efforts at salvaging “marginal comforts.”’…
Principal conclusions
Evidence of efficacy for treatment approaches in severe and enduring anorexia nervosa is very limited. We identified only one RCT (Touyz et al., 2009) designed to test a specific approach and its results are not yet published. Promising support for atypical antipsychotics needs to be tempered with recent reports of olanzapine and risperidone in adolescents with anorexia nervosa having not supported their efficacy and raised concerns about metabolic adverse effects (Hagman et al., 2011; Kafantaris et al., 2011). Open trials have, however, reported newer psychotherapies which address important maintaining factors for patients with a chronic disorder.
Clinical and research implications
New developments in psychological therapies which may provide the way forward and warrant further specific evaluation include CBT-E (Fairburn, 2010), CBT-AN modified (Touyz et al., 2009), CREST (Tchanturia et al., 2004), MANTRA (Schmidt and Treasure, 2006; Wade et al., 2011), COPP (Williams et al., 2010), SSCM modified (Touyz et al., 2009) and the approach of Strober (2010). Goals of therapy also need to be re-thought. ‘Complete cure’ in chronic anorexia nervosa is extremely difficult to effect and attempts at such have been argued to be futile. Patients with long-standing illness often develop a history of negative treatment experiences and repeated treatment failures. Both patient and clinician typically experience a sense of hopelessness about the possibility of change. Treatment trials need to move beyond targeting core eating disorder pathology (primarily weight restoration) and examine effectiveness in minimising harm and reducing personal and social costs of chronic illness, such as medical morbidity, burden on health services, quality of life, depression and isolation. There is an imperative to develop and test appropriate treatments and better define chronicity, with or without treatment ‘resistance’ specifiers, which would also help guide new research endeavours (Steinhausen, 2002; Strober, 2010). The use of staging models with course as well as severity specifiers as discussed by Maguire et al. (2011) thus deserves attention.
Footnotes
Funding
RS was supported by a University of Western Sydney School of Medicine Summer Research Scholarship.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.