
Abstract
Although clinicians have long been aware of dysfunctional exercise behaviour among individuals with anorexia nervosa (AN) and bulimia nervosa (BN) presenting for treatment [1], and whereas excessive exercise has been included in the diagnostic criteria for BN since the publication of DSM-III-R some two decades ago [2], it is only in recent years that researchers have begun to systematically examine the prevalence and correlates of excessive exercise in eating disorder patients.
Typically in this research, subgroups of patients classified as excessive or non-excessive exercisers have been compared on outcomes such as personality traits, levels of comorbid psychopathology and response to treatment [3–9]. Although the specific criteria used to define ‘excessive exercise’ have varied, most often exercise subgroups have been differentiated according to a frequency criterion, so that excessive exercisers have been those individuals who report frequent (e.g. daily) hard exercise primarily intended to influence weight or shape. The use of a frequency criterion may reflect, in part, a reliance on the definition of excessive exercise given in the original version of the Eating Disorder Examination (EDE) [10], namely, ‘intense exercising to control shape or weight on average at least five days a week’, because the EDE has come to be accepted as the gold standard by which to assign eating disorder diagnoses [11].
Two clear findings have emerged from this research. First, excessive exercise is common among eating disorder patients, with prevalence in the range of 30–70% [3–9]. Second, excessive exercise is more common among patients with AN than those with BN [3, 4, 7, 9]. Findings concerning the correlates of excessive exercise are more difficult to generalize because different outcomes have been assessed in different studies, but the available evidence suggests that, among AN patients at least, excessive exercise is associated with elevated levels of obsessive–compulsive, perfectionistic and addictive personality traits, higher levels of eating disorder psychopathology and general psychological distress, longer duration of inpatient treatment and poorer treatment outcome [3–9, 12, 13]. In addition, findings from one recent study suggested that the prevalence of excessive exercise may be higher among AN patients who report purging in the absence of binge eating than those who report both binge eating and purging or neither binge eating nor purging [9].
The question of how or in what ways the exercise behaviour of eating disorder patients might be considered excessive has received much less attention. Evidence from community-based studies suggests that frequency of exercise is a poor predictor of eating disorder psychopathology and impairment in psychosocial functioning when compared to other aspects of exercise behaviour, in particular, the experience of negative emotionality when exercise is missed or postponed and exercise that is undertaken solely or primarily to influence weight, shape or body tone [14–18]. Hence, behaviours of this kind may best characterize the nature of excessive exercise among individuals with eating disorders. Alternatively, the exercise behaviour of individuals with eating disorders may be excessive when it ‘significantly interferes with important activities, occurs at inappropriate times or in inappropriate settings, or continues despite injury or other medical complications’, as suggested in DSM-IV [19]. These criteria have been used in a number of studies, although there is little empirical evidence to support their validity [15, 17].
In order to elucidate the nature of excessive exercise among individuals with eating disorders, we compared eating disorder patients and healthy women on measures of obligatory exercise, motivation for exercise, and frequency of hard exercise for weight or shape reasons. Based on previous research in community samples, we hypothesized that exercising for weight, shape or body tone and the experience of guilt when exercise is missed would be the variables that most clearly differentiated the exercise behaviour of eating disorder patients from that of healthy women. A second aim of the study was to compare excessive exercise behaviour between subgroups of eating disorder patients. In view of the paucity of existing evidence, no specific hypotheses were formulated in this regard.
Method
The study was carried out in the Australian Capital Territory (ACT) region of Australia, a highly urbanized region that includes the city of Canberra (population 314 000 in 2002). Participants in the clinical sample were consecutive referrals to the ACT Eating Disorders Day Program, a specialist treatment facility established in 1999 and providing government-subsidized outpatient treatment for eating disorders. A self-report questionnaire was completed as part of the intake process by all individuals referred for treatment between March 2001 and March 2002. The questionnaire included measures of eating disorder psychopathology, quality of life, exercise behaviour and limited sociodemographic information [20]. Height and weight were measured as part of the intake assessment, enabling calculation of body mass index (BMI; kg m−2).
Eating disorder diagnoses, based on clinical assessment at intake, were made according to DSM-IV criteria [19]. Therefore, individuals who had achieved marked loss of weight from an initially high BMI were eligible for the diagnosis of AN. This is a less stringent criterion than that specified in the most recent revision of the International Classification of Diseases (ICD-10; BMI≤17.5 kg m−2) [21] but is consistent with evidence suggesting that individuals who have lost significant amounts of weight and who otherwise meet criteria for AN present a similar clinical picture irrespective of pre-morbid weight [22]. Restricting and purging subtypes of AN were identified on the basis of participant self-reported eating disorder behaviours [23]. Specifically, individuals with AN who reported one or more episodes of purging (i.e. self-induced vomiting and/or misuse of laxatives or diuretics) during the preceding 4 weeks were classified as having AN purging subtype (ANP), whereas individuals who did not report episodes of purging were classified as having AN restricting subtype (ANR) [20].
Completed questionnaires were received from 135 patients. Data for 33 individuals who did not complete the sections of the questionnaire relating to exercise behaviour were excluded. This subgroup included 10 individuals who met criteria for the DSM-IV provisional diagnosis of binge eating disorder (BED) and a further eight individuals who met criteria for a subthreshold form of BED. By definition, these individuals did not engage in excessive exercise. Therefore, data for a total of 102 patients, all of whom were female, were included in the analysis. Their diagnoses were as follows: AN, n=28; BN, n=41; and eating disorder not otherwise specified (EDNOS), n=33. Of the 28 individuals with AN, 15 (53.6%) were classified as having ANR and 13 as having ANP. The mean (±SD) age in years of ANR, ANP, BN, and EDNOS patients were, respectively, 21.0±8.3, 23.6±8.3, 23.8±6.2, and 20.5±7.8 (χ=10.0, p<0.05). Their mean (±SD) BMIs were 17.1±1.7 kg m−2, 18.1±2.1 kg m−2, 23.5±4.5 kg m−2, and 22.2±4.8 (χ=38.5, p<0.01).
Recruitment of the community sample has been described in several previous studies [15, 24–26]. In brief, self-report questionnaires were posted or hand-delivered to a sample of 400 female ACT residents aged 18–45 years, selected at random from the Electoral Roll. The questionnaire was similar to that completed by the clinical sample, except that detailed sociodemographic information was obtained and participants’ BMI was calculated from self-reported height and weight [24]. Completed questionnaires were received from 232 individuals, which represented a response rate of 63.8% after addresses known to be incorrect were taken into account. Complete data were available for a subgroup of 184 individuals (79.3% of the total sample) who reported some form of exercise during the preceding 4 weeks. Their mean age was 33.3±9.1 years. Their mean BMI was 24.1±4.8 kg m−2. The sample was representative of the wider population of young adult women on a range of sociodemographic variables [27]. The collection of data from both community and clinical samples, and all other aspects of the study design, were approved by the ACT Human Research Ethics Committee.
Measures
Commitment to Exercise Scale
The Commitment to Exercise Scale (CES) is an eight-item measure designed to address obligatory aspects of exercise behaviour, such as exercising when tired or unwell, feeling guilty when exercise is missed or postponed, and priority given to exercise over other activities (Table 1) [28]. For each item, a cross is placed at the point on a horizontal line (150 mm) that best indicates the participant's level of agreement with the statement in question. Appropriate bipolar adjectives (e.g. ‘never’, ‘always’) appear at each end of the line. The distance from the beginning of the line to the point marked constitutes the score for each item, with higher scores indicating more obligatory behaviour.
Exercise behaviours of eating disorder patients and healthy women
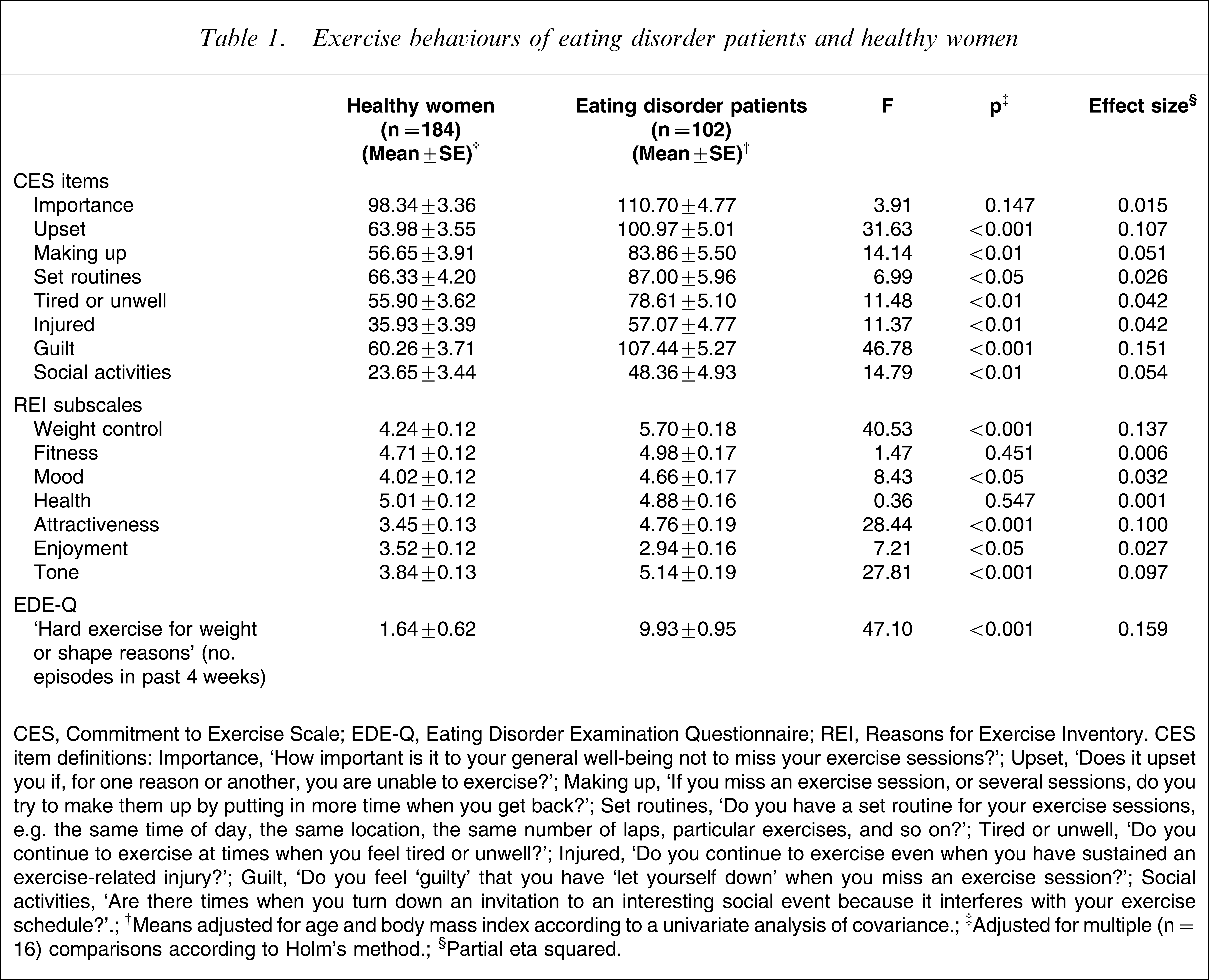
CES, Commitment to Exercise Scale; EDE-Q, Eating Disorder Examination Questionnaire; REI, Reasons for Exercise Inventory.
CES Item definitions: Importance, ‘How important is it to your general well-being not to miss your exercise sessions?’; Upset, ‘Does it upset you if, for one reason or another, you are unable to exercise?’; Making up, ‘If you miss an exercise session, or several sessions, do you try to make them up by putting in more time when you get back?’; Set routines, ‘Do you have a set routine for your exercise sessions, e.g. the same time of day, the same location, the same number of laps, particular exercises, and so on?’; Tired or unwell, ‘Do you continue to exercise at times when you feel tired or unwell?’; Injured, ‘Do you continue to exercise even when you have sustained an exercise-related injury?’; Guilt, ‘Do you feel ‘guilty’ that you have ‘let yourself down’ when you miss an exercise session?’; Social activities, ‘Are there times when you turn down an invitation to an interesting social event because it interferes with your exercise schedule?’.
†Means adjusted for age and body mass index according to a univariate analysis of covariance.
‡Adjusted for multiple (n=16) comparisons according to Holm's method.
§Partial eta squared.
Reasons for Exercise Inventory
The Reasons for Exercise Inventory (REI) is a 24-item scale assessing reasons for exercising in each of seven domains (here referred to as subscales): weight control; fitness; health; body tone; physical attractiveness; mood; and enjoyment [29]. Items are scored on a 7-point scale, with a score of 1 indicating that the item descriptor is ‘not at all important’ as a reason for exercise and a score of 7 indicating that the descriptor is ‘extremely important’. Mean scores are calculated for each subscale.
Frequency of ‘hard exercise for weight or shape reasons’
Frequency of hard exercise for weight or shape reasons was assessed by two items of the Eating Disorder Examination Questionnaire (EDE-Q) [23]. Specifically, participants were asked whether they had ‘exercised hard as a means of controlling their shape or weight’ during the preceding 4 weeks and, if so, the number of occasions on which they had done so (here referred to as ‘frequency of hard exercise for weight or shape reasons’).
Statistical analysis
Analysis of covariance (ANCOVA) was used to compare exercise behaviours between eating disorder patients and healthy women, controlling for age and BMI. Discriminant function analysis was used to identify the exercise behaviours that best discriminated between eating disorder patients and healthy women. Independent variables for this analysis were those exercise behaviours found to differ significantly between groups in the ANCOVA. For the comparison of exercise behaviours between subgroups of patients, non-parametric methods, namely, the Kruskall–Wallis test, were used because the distributions of some variables were non-normal and sample sizes were small. Patients in the EDNOS subgroup were excluded for the purpose of this analysis because this subgroup is heterogeneous in terms of its clinical features [30]. Where a significant or near-significant overall effect (i.e. ANR vs ANP vs BN) was observed, pairwise Mann–Whitney U-tests were used to isolate the source of the difference. For comparisons between eating disorder patients and healthy women, observed p values were adjusted using Holm's method [31]. No correction for multiple tests was used for comparisons involving subgroups of eating disorder patients because these comparisons were intended to generate, rather than to test, hypotheses and because statistical power was necessarily limited by the small subgroup sample sizes [32]. A significance level of 0.05 was used for all tests, all tests were two-tailed, and all analysis was conducted using SPSS version 14.0 (SPSS, Chicago, IL, USA).
Results
Comparison of the exercise behaviours of eating disorder patients and healthy women is shown in Table 1. It can be seen that individuals with eating disorders scored higher than healthy women on seven of the eight CES items, after age and BMI were statistically controlled. It also can be seen that scores on four of the seven REI subscales, namely, weight control, attractiveness, body tone and mood, were significantly higher among eating disorder patients than among healthy women, whereas scores on the health and fitness subscales did not differ between groups. Scores on the enjoyment subscale of the REI were significantly higher among healthy women than among eating disorder patients. In addition, frequency of hard exercise for weight or shape reasons was significantly higher among eating disorder patients than among healthy women.
Results of the discriminant function analysis are given in Table 2. It can be seen that guilt when exercise is missed, frequency of hard exercise for weight or shape reasons, and exercising for weight control, physical attractiveness and body tone were the exercise behaviours that best distinguished between eating disorder patients and healthy women. The comparatively high loading of the CES ‘upset if unable to exercise’ item should be interpreted with caution because scores on this item are highly correlated with those of the ‘guilt when exercise is missed’ item [18]. Based on the discriminant function, 83.1% of non-cases and 76.6% of cases were correctly classified. Overall, 81.1% of participants were correctly classified.
Discriminant function analysis of exercise behaviours of eating disorder patients and healthy women
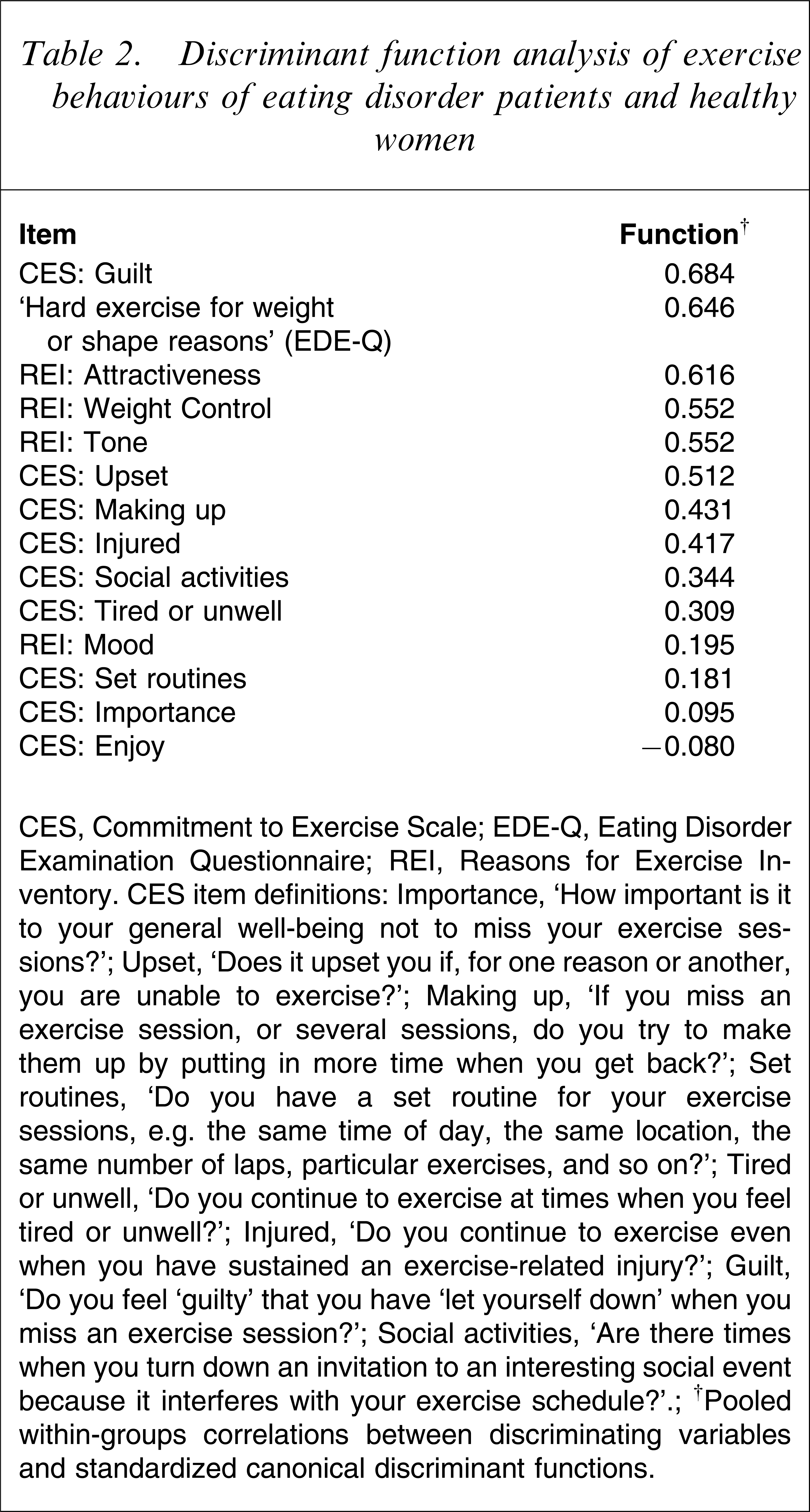
CES, Commitment to Exercise Scale; EDE-Q, Eating Disorder Examination Questionnaire; REI, Reasons for Exercise Inventory.
CES, item definitions: Importance, ‘How important is it to your general well-being not to miss your exercise sessions?’; Upset, ‘Does it upset you if, for one reason or another, you are unable to exercise?’; Making up, ‘If you miss an exercise session, or several sessions, do you try to make them up by putting in more time when you get back?’; Set routines, ‘Do you have a set routine for your exercise sessions, e.g. the same time of day, the same location, the same number of laps, particular exercises, and so on?’; Tired or unwell, ‘Do you continue to exercise at times when you feel tired or unwell?’; Injured, ‘Do you continue to exercise even when you have sustained an exercise-related injury?’; Guilt, ‘Do you feel ‘guilty’ that you have ‘let yourself down’ when you miss an exercise session?’; Social activities, ‘Are there times when you turn down an invitation to an interesting social event because it interferes with your exercise schedule?’.
†Pooled within-groups correlations between discriminating variables and standardized canonical discriminant functions.
Comparison of exercise behaviours between subgroups of eating disorder patients is shown in Table 3. It can be seen that differences between groups were observed on the CES item ‘If you miss an exercise session, or sessions, do you try to make them up by putting in more time when you get back?’ (item 3) and the weight control and attractiveness subscales of the REI. In addition, differences between groups on the CES items ‘Do you continue to exercise at times when you feel tired or unwell?’ (item 5) and ‘Are there times when you turn down an invitation to an interesting social event because it interferes with your exercise schedule?’ (item 8) and on the enjoyment subscale of the REI approached significance (p=0.09, p=0.07, p=0.09, respectively). Post-hoc comparisons indicated that ANP patients had higher scores than BN patients on CES items 3 and 5 and higher scores than ANR patients on CES item 8. ANP and BN patients had higher scores on the weight control and attractiveness subscales of the REI than ANR patients, whereas ANR patients had higher scores than BN patients on the REI enjoyment subscale.
Exercise behaviours
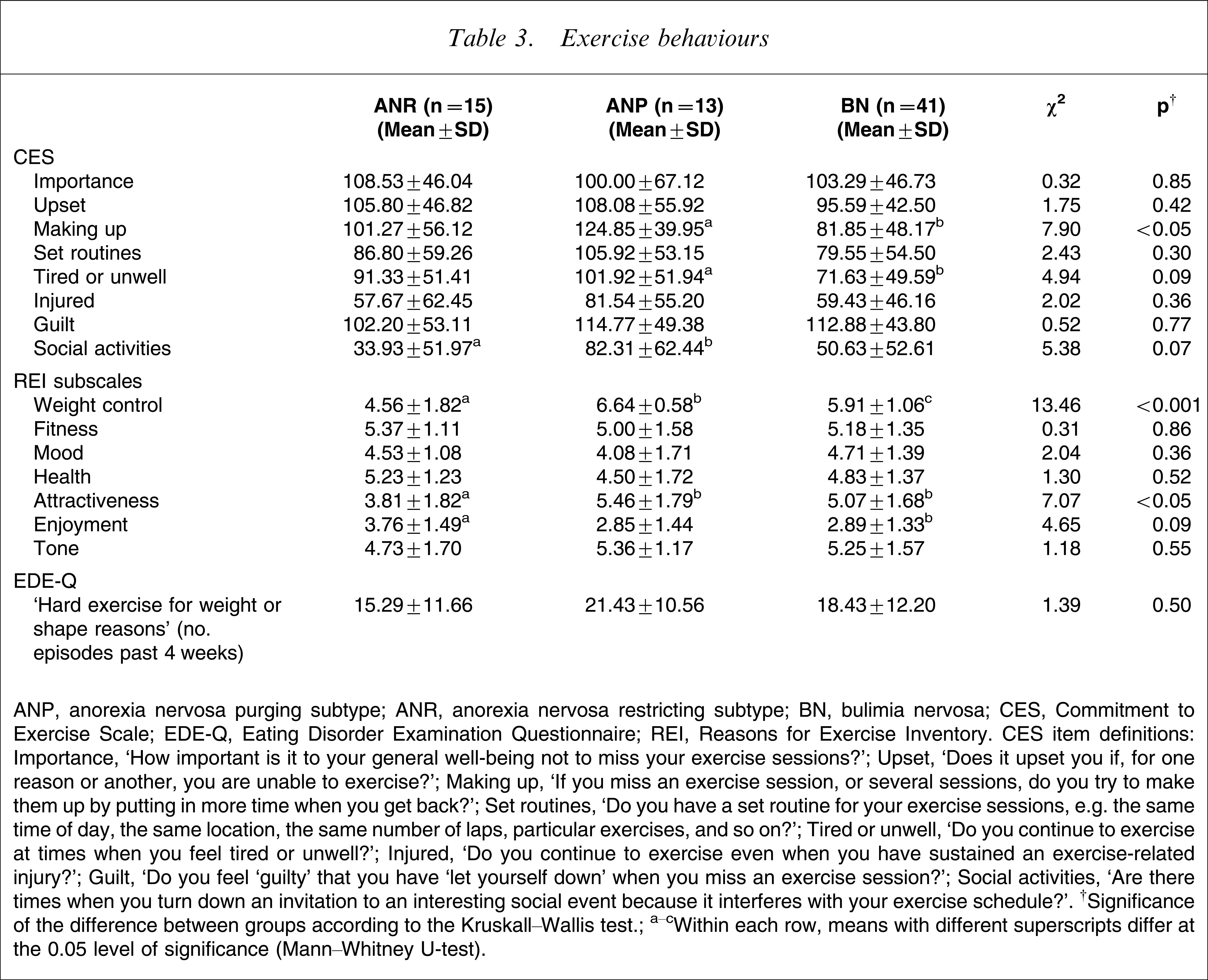
ANP, anorexia nervosa purging subtype; ANR, anorexia nervosa restricting subtype; BN, bulimia nervosa; CES, Commitment to Exercise Scale; EDE-Q, Eating Disorder Examination Questionnaire; REI, Reasons for Exercise Inventory.
CES, item definitions: Importance, ‘How important is it to your general well-being not to miss your exercise sessions?’; Upset, ‘Does it upset you if, for one reason or another, you are unable to exercise?’; Making up, ‘If you miss an exercise session, or several sessions, do you try to make them up by putting in more time when you get back?’; Set routines, ‘Do you have a set routine for your exercise sessions, e.g. the same time of day, the same location, the same number of laps, particular exercises, and so on?’; Tired or unwell, ‘Do you continue to exercise at times when you feel tired or unwell?’; Injured, ‘Do you continue to exercise even when you have sustained an exercise-related injury?’; Guilt, ‘Do you feel ‘guilty’ that you have ‘let yourself down’ when you miss an exercise session?’; Social activities, ‘Are there times when you turn down an invitation to an interesting social event because it interferes with your exercise schedule?’.
†Significance of the difference between groups according to the Kruskall–Wallis test.
a–cWithin each row, means with different superscripts differ at the 0.05 level of significance (Mann–Whitney U-test).
In view of the differences between diagnostic subgroups with respect to age and BMI, additional analysis, in which exercise behaviours were compared among subgroups of patients divided according to median splits of age and BMI, was conducted to determine whether findings relating to diagnostic subgroups might reflect, in part, between-group differences in age and BMI. Results of this analysis indicated that the findings could not be accounted for by between-group differences in age and BMI (details are available from the first author upon request).
Discussion
We examined differences between eating disorder patients and healthy women, and between subgroups of patients, on a range of dysfunctional exercise behaviours. Negative emotionality associated with exercise being missed or postponed and exercising for weight or shape reasons, including physical attractiveness, were the exercise behaviours that most clearly differentiated between women with eating disorders and healthy women. Purging AN patients tended to have higher levels of obligatory exercise than ANR and BN patients, and both ANP and BN patients reported exercising more for weight control and physical attractiveness, and less for enjoyment, than ANR patients.
Differences between ED patients and healthy women
The present findings converge with those of previous research, in that the same exercise behaviours that have been found to be most closely associated with elevated levels of eating disorder psychopathology and impairment in psychosocial functioning in community samples most clearly differentiated between the exercise behaviour of eating disorder patients and that of healthy women [15, 17, 18]. These behaviours were the experience of intense guilt when exercise is missed and exercising solely or primarily for weight or shape reasons, including physical attractiveness. Further, within the clinical sample, scores on the items assessing these behaviours were high when compared with other items, indicating that these aspects of excessive exercise were the most salient among individuals with eating disorders. The regular occurrence of ‘hard exercise for weight or shape reasons’, as assessed on the EDE-Q, was also characteristic of the exercise behaviour of eating disorder patients but not that of healthy women.
In contrast, differences between patients and healthy women on those items (of the CES) corresponding to the criteria for excessive exercise suggested in DSM-IV, namely, ‘Do you continue to exercise when you have sustained an exercise-related injury?’ and ‘Are there times when you turn down an invitation to an interesting social event because it interferes with your exercise schedule’?, were less pronounced and scores on these items were comparatively low. These findings, which also converge with those of our previous research [15, 17, 18], suggest that the definition of excessive exercise given in DSM-IV needs to be reconsidered.
These issues of definition are not merely academic. Inconsistency in the criteria used to define ‘excessive exercise’ complicates the interpretation of findings from epidemiological studies, in particular, estimates of the prevalence and correlates of the non-purging subtype of BN and its relation to purging BN and BED [15], and may reduce the likelihood that dysfunctional exercise behaviours are recognized as problematic by individuals affected and by health professionals [33]. The prevalence of excessive exercise among women in the community is surprisingly high and excessive exercise is the most common weight-control behaviour among individuals with BN and related disorders [17, 34]. The comparatively low significance attached to enjoyment as a reason for exercise among both patients and healthy women indicates the extent of the problem and suggests that information concerning those exercise behaviours found to be most strongly associated with eating disorder psychopathology and impairment in psychosocial functioning needs to be included in prevention programmes for both eating disorders and obesity [35].
From a clinical perspective, more thought needs to be given to the significance and management of dysfunctional exercise behaviour in the treatment process. At present there exists little published literature concerning the management of excessive exercise in eating disorder patients, nor even a consensus that these behaviours warrant attention [36]. The issue is important because the presence of excessive exercise, and its persistence following discharge, has been found to predict poor outcome in AN as well as conferring an increased risk of serious medical complications [12, 13, 9]. One of the authors (RMC) has developed a programme specifically designed to replace ‘mindless’ exercise, which encompasses the full spectrum of dysfunctional exercise behaviours, with ‘mindful’ exercise behaviours, designed to promote both physical and mental health as well as give enjoyment and pleasure [36]. Preliminary findings from the application of this programme to patients attending a residential treatment facility have been promising [37]. The present findings indicate specific targets for programmes of this kind.
Subgroups of patients
Comparison of exercise behaviours between subgroups of eating disorder patients yielded some interesting additional findings. ANP patients tended to have higher levels of obligatory exercise than both ANR and BN patients, and both purging AN and BN patients tended to report exercising more for reasons of weight control and physical attractiveness, and less for enjoyment, than ANR patients. Frequency of hard exercise for weight or shape reasons also tended to be higher among ANP and BN patients than among ANR patients.
Although any conclusions in this regard are tentative, given the small sample sizes involved, it is reasonable to posit that differences of this kind, to the extent that they are replicable, reflect the personality and clinical variables that distinguish ANR from ANP and BN. In particular, ANR typically occurs as an early phase of AN, in which ego-syntonic features of the disorder predominate [20]. It is possible that the anxious obsessionality characteristic of eating disorder patients who exercise excessively may be particularly common among individuals with the purging form of AN and that individuals in this subgroup may be more likely to use exercise as a means by which to modulate their negative affect [9, 38]. Alternatively, AN with excessive exercise may constitute a phenotype that cuts across the restrictor/purger distinction [8]. It also is unclear whether it is the presence of excessive exercise (or purging) per se, or the occurrence (or number) of multiple weight-control behaviours, both purging and non-purging, that indicates clinical severity [39, 40]. Further research in which subgroups of AN are differentiated and in which a broader range of exercise behaviours is assessed will be needed to address this issue, but the present findings suggest that important differences between subgroups may be obscured when excessive exercise is defined solely in terms of frequency.
Study limitations
At least three limitations of the present research need to be taken into account when interpreting the findings. First, given the small numbers of patients in the ANR and ANP subgroups, and the fact that no adjustment to the Type I error rate was made for comparisons involving subgroups of patients, the outcomes of these comparisons should be interpreted with caution. The findings do suggest that the comparison of exercise behaviour between subgroups of eating disorder patients is worthy of further investigation. Second, because exercise frequency per se – as opposed to frequency of hard exercise for weight or shape reasons – was not assessed in the clinical sample, it was not possible to compare exercise frequency between patients and healthy women or between subgroups of patients. Research conducted by the authors, however, and by others has shown that frequency of exercise has little or no association with either eating disorder psychopathology or psychosocial functioning [14–18, 41]. Finally, we did not have information concerning current or prior participation in competitive sports for either patients or healthy women. Because rates of participation in competitive sports are known to be elevated among eating disorder patients [42], the observed differences between patients and healthy women may reflect, in part, differences in athletic ability and/or endeavour.
In summary, the occurrence of intense guilt when exercise is missed and exercising solely or primarily to influence weight, shape or physical attractiveness were the variables that most clearly distinguished the exercise behaviour of eating disorder patients from that of healthy women. Further, these behaviours tended to be more common among ANP and BN patients than among ANR patients, although sample size precluded any firm conclusions in this regard. The findings suggest that research addressing the prevalence and correlates of excessive exercise in eating disorder patients would benefit from a broader assessment of exercise behaviour than has typically been used in previous studies. In addition, the findings may indicate specific targets for the clinical management of excessive exercise and for community-based health promotion initiatives.
Footnotes
Acknowledgements
The Health and Well-Being of Female ACT Residents Study was funded by The Canberra Hospital Private Practice Fund, ACT Health and Community Care and ACT Mental Health. Dr Mond is supported by a National Health and Medical Research Council Sidney Sax Fellowship. Thanks also to Drs David Saville PhD, Juliet Shaffer PhD, and Ross Crosby PhD, for their helpful comments on an earlier version of this manuscript.