
Abstract
Objective:
Prospective study designs ideally allow patients to be followed from the first manifestations of the illness or even from an at-risk stage. It can thus provide data on the predictive value of changes in clinical symptomatology, cognition or further biological markers to broaden our understanding of the etiopathology and symptomatic trajectory of bipolar disorders. The scope of this narrative review is to summarize evidence from prospectively collected data on psychopathological and other clinical and biological changes in the early developmental course of bipolar disorders.
Methods:
The narrative review was based on a literature search conducted in February 2016 within the PubMed library for prospective study data of persons in antecedent and early manifest stages of manifest bipolar disorder published within the last 15 years.
Results:
A total of 19 prospective studies were included. Regarding psychopathological features; personality, temperament and character traits as well as changes in sleep and circadian rhythm, the evidence suggests that risk factors for the development of bipolar disorder can already be described and should be studied further to understand their interaction, mediation with other factors and timing in the developmental process of bipolar disorder. Apart from the positive family history, childhood anxiety, sleep problems, subthreshold (hypo)manic symptoms and certain character traits/emotionality should be identified and monitored already in clinical practice as their presence likely increases risk of bipolar disorder. Up to date no substantiated evidence was found from prospective studies addressing cognitive features, life events, immunological parameters and morphological central nervous system changes as potential risk factors for bipolar disorder.
Conclusion:
For an improved understanding of episodic disorders, longitudinal data collection is essential. Since the etiology of bipolar disorders is complex, a number of potential risk factors have been proposed. Prospective studies addressing this spectrum and resilience factors are critical and will be best conducted within multi-site research networks or initiatives.
Introduction
Bipolar illness constitutes a severe mental disorder that manifests in most cases in late adolescence or young adulthood with a mean age of onset of 17.5 years (Kupfer et al., 2002; Lish et al., 1994; Perlis et al., 2004). The severe consequences for the individual are compounded by the fact that it is only diagnosed in a majority of patients years after first symptoms have evolved (with a delay of about 10 years; Hirschfeld et al., 2003; Lish et al., 1994; Morken et al., 2009; Oedegaard et al., 2009; Perlis et al., 2004; Pfennig et al., 2011; Post et al., 2008) with evidence for a negative influence of the duration of untreated illness on the course of the disease including psychosocial impairment (Berk et al., 2011a; Post et al., 2010, 2012). Early recognition and intervention is therefore a highly important topic of clinical research which is best informed by prospectively collected evidence. This design minimizes bias that is regularly limiting retrospective study data (such as selection and recall bias). Cross-sectional studies are even more prone to bias, are unable to substantiate the assumption of causation, and can only be of value for forming hypotheses. To investigate causation, in prospective studies, mediating and moderating factors and confounders have to be analyzed. Following patients from their first manifestations or even subjects with an increased risk to develop the disorder prospectively over long periods of time can provide data on the predictive value of changes in clinical symptomatology, cognition or further biological markers. This study design enables the analysis of the developmental perspective of the illness and the specific influence of certain risk factors in different periods of individual and disease development. Especially the diagnosis of bipolar disorder (BD), an illness characterized by an episodic course which most commonly first presents with a depressive episode instead of the distinguishing (hypo)manic one, can only be validated after observing the patient closely over long periods of time. Hence, the scope of this narrative review is to summarize evidence from prospectively collected data on psychopathological and other clinical as well as cognitive and further fluid or non-fluid biological changes in the developmental course of BD.
The frame of the review spans antecedent stages and early manifest disorder. Recently, first clinical staging models for BD are proposed (Frank et al., 2015; Scott et al., 2013), depicting these early phases as stage 0 (where a heightened risk, e.g., from a family history, was established without current symptomatology), stage 1 (with mild or moderate subthreshold symptoms) and stage 2 (with a first episode of full-blown disorder). However, there is a debate as to whether there is already sufficient evidence to develop a staging model at all since the development of BD seems to be more complex and different from that of psychosis, where the model is generalized from and important results from offspring studies have to be included into these staging efforts (see Duffy et al., 2017). Implications of the reviewed evidence for the future research questions and adequate designs will be delineated.
Methods
The narrative review was based on the literature search conducted in February 2016 within the PubMed library for prospective study data of people in antecedent (i.e. at-risk) stages and with early manifest BD published within the last 15 years. Search terms included the following: (bipolar, mani*, risk) and (psychopathol*, personality, sleep, circadian, cognition, life events, hormonal, immunologic*, anatomical or morphological). The search was intended to give a comprehensive overview and does not guarantee completeness. The search term ‘hormonal’ was added to be sure to find all information regarding changes in immunological features as potential risk factor for BD, and it was used with that narrow focus.
Results and discussion
Research questions for prospective studies on the longitudinal changes in the course of BD discussed within this review mostly originated from analyzing retrospective and cross-sectional data. Up to now only little prospective evidence is available, mainly due to the substantially higher resources needed to conduct longitudinal research over long periods of time.
See Table 1 for an overview of included study data into the following sections.
Publications providing data for article sections.
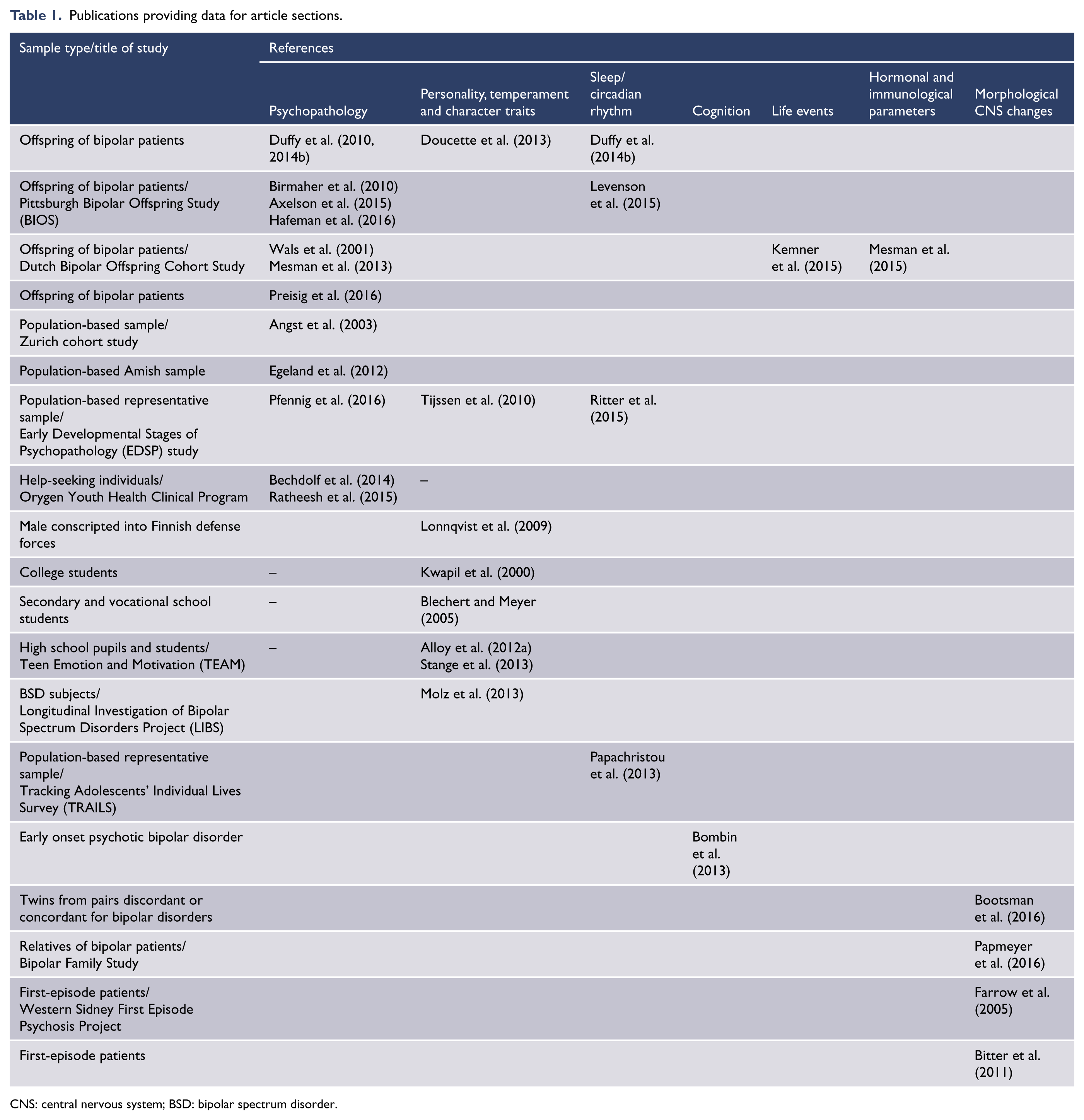
CNS: central nervous system; BSD: bipolar spectrum disorder.
Psychopathological features
For a diagnosis of BD, manic symptomatology reaching the criteria of an episode or depressive episodes combined with hypomanic symptoms again reaching criteria of an episode must have been occurred. Bipolar-specific subthreshold symptomatology could progress to threshold level and could therefore define an at-risk stage. Data from a retrospective study on n = 52 bipolar patients showed that mania manifested after gradual onset of symptoms with slow or rapid deterioration after a mean of 10.3 ± 14.4 months (Correll et al., 2014a). Unspecific symptoms or other manifest psychiatric disorders can also occur in the development of the illness. This developmental course could take years to evolve. Long-running prospective cohort studies with samples enriched for the risk to develop BD (as young persons with a positive family history or manifest depressive disorder) or not-enriched samples representative of the population or certain parts of the population are suited best to study the antecedents of the illness.
Data from four prospective offspring studies were included
Anne Duffy et al. are conducting an ongoing prospective Canadian offspring study, including high-risk children with at least one parent affected by BD type I. Control offspring without a family history of affective disorders were recruited from schools. At study intake, subjects were between 8 and 25 years old. All subjects are being followed-up by a psychiatrist masked to family affiliation at baseline and subsequently annually (on average) or anytime symptoms developed using the Schedule for Affective Disorders and Schizophrenia for School-Age Children-Present and Lifetime Version (K-SADS-PL/SADS-L; Endicott and Spitzer, 1978). Final Diagnostic and Statistical Manual of Mental Disorders-IV (DSM-IV) diagnoses in the offspring are made on the basis of blind consensus review using all available clinical information by at least two additional research psychiatrists. In a 2014 publication, data of 229 high-risk offspring from 113 families and 86 control offspring from 55 families were included that had been followed-up for up to 16 years. The authors found that in high-risk offspring that developed manifest BD, the early course started with non-specific non-mood disorders in childhood (i.e. anxiety), followed by minor mood and adjustment disorders in early adolescence, then major depressive episodes and finally hypomanic/manic episodes. The onset of anxiety was usually prior to 10 years of age and the onset of mood disorder was after 10 years in most cases. When including only major mood episodes, 90% (60/67) of subjects had major depression as their first mood episode. No subject manifested hypomania or mania prior to age 14 years, with an average latency of 3.5 ± 2.6 years, following the index depressive episode. The mean age of onset of the first hypomanic or manic episode was 19 ± 3.8 years. Childhood anxiety disorder more than doubled the risk to manifest BD (Duffy et al., 2010, 2014b).
The prospective Pittsburgh Bipolar Offspring Study (BIOS) included offspring of bipolar I or II patients (n = 433) and community controls (n = 301) aged 6–18 years. Psychiatric diagnoses were assessed using the Structured Clinical Interview for DSM-IV (SCID; First et al., 1997) and several sections from the K-SADS-PL (Birmaher et al., 2010). Axelson et al. (2015) reported from a mean follow-up duration of 6.8 (±2.2) years. As Duffy et al., they found that the majority of individuals that later developed BD started with depression (69%) at a mean age of 12.5 years (±4.6). They also registered anxiety disorders, disruptive behavior disorder and attention deficit hyperactivity disorder (ADHD) prior to (hypo)mania. However, sensitivity analyses restricted to prospectively collected data found only subthreshold (hypo)manic episodes (that was present in 36% of the later bipolar cases) significantly associated with later manifestation of (hypo)mania (Axelson et al., 2015). Hafeman et al. (2016) recently published data from a mean follow-up of 8 years using factor and regression analyses to identify dimensional predictors for onset of BD. They found that parent-reported internalizing symptoms, child-reported affective lability and anxiety/depression at baseline significantly predicted new-onset bipolar spectrum disorder (BSD). As best predictors of conversion at the next visit elevated child-reported affective lability and the presence of manic symptoms (and here irritability, hyperactivity and distractibility) were identified. Path analysis showed that baseline child-reported affective lability significantly contributed to higher Mania Rating Scale scores at the visit prior to conversion. Youth without anxiety/depression, affective lability and mania had a 2% predicted chance of manifesting BD, those with all risk factors had a 49% predicted chance (Hafeman et al., 2016). The Dutch Bipolar Offspring Cohort Study followed 140 offspring from 86 families with one bipolar parent (74% bipolar I, 26% bipolar II) recruited in an age range from 12 to 21 years (Mesman et al., 2013; Wals et al., 2001). Assessments were conducted at baseline and at 1, 5 and 12 years of follow-up. Offspring were evaluated psychiatrically at baseline and after 1 year using the K-SADS-PL and after 5 years applying the SCID-I. Overall, 13% of offspring manifested BSD. In 88%, the disorder began with a depressive episode with a mean age, at first episode, of 14.6 (±4.7) years. The first (hypo)manic episode followed 5.3 (±4.3) years later. Overall, 53% had comorbid anxiety disorder, in about halve of that, this was present before or at the onset of mood disorder (Mesman et al., 2013).
Preisig et al. (2016) published data from a controlled 10-year follow-up study on offspring of bipolar patients, a subsample from a large family study of mood disorders conducted in the French-speaking part of Switzerland (Vandeleur et al., 2012, 2014). Included in the subsample were 145 offspring of bipolar patients and 112 control offspring (as well as 115 patients with major depressive disorder [MDD]) aged 6 to almost 18 years at baseline. Follow-up was conducted at subject’s ages 7, 10, 13, 16, 19, 22, 25, 28, 31 and 34 years, by applying the semi-structured Diagnostic Interview for Genetic Studies (DIGS; Nurnberger Jr et al., 1994) and the K-SADS. Offspring of patients with early onset of BD (before age 22) showed a higher risk for development of BD than those of patients with a later onset and controls (Preisig et al., 2016).
Data from three population-based studies and one study with help-seeking people were included
Adding to the above mentioned data on mood lability, there is some evidence that mood swings (frequent ups and downs, indicating impaired mood regulation) may precede the first affective episode. Jules Angst et al. (2003) screened 4547 people representative of the canton of Zurich in Switzerland in the Zurich cohort study using the Symptom-Checklist-90-Revised (SCL-90-R, Derogatis, 1977). They interviewed a subsample of 591 subjects (2/3 with high scores in the SCL-90-R and 1/3 randomly chosen from lower scorers Angst et al., 2003). In an analysis of prospective data of 15 years of follow-up, they found ‘ups and downs’ to be the most influential risk factor for onset of BSD (odds ratio [OR], 14.3 ± 7.8).
Egeland et al. (2012) reported 16-year follow-up data from an Amish cohort study sampling 115 offspring of bipolar patients and 106 controls from matched control families. They were assessed using the CARE Interview instrument, consisting of parts covering birth record, medical and development, parents concerns for the health and well-being of the offspring and potential prodromal symptoms. Risk rating and diagnoses were formulated by a panel of five clinicians. Nine offspring developed mania; of that, eight were bipolar offspring. The mean age of mania onset was 15 years. The highest ranked antecedents for onset of BD were crying and being anxious/worried, being hyper-alert, being sensitive, decreased sleep, somatic complaints, being fearful and medical/physical problems (Egeland et al., 2012).
The Early Developmental Stages of Psychopathology (EDSP) study consists of a representative community sample of originally 3021 adolescents and young adults aged 14–24 years at baseline from the greater Munich area in Germany that was assessed until now up to four times over 10 years (Lieb et al., 2000; Wittchen et al., 1998b, 1998c). Assessment of symptoms was conducted by clinically trained interviewers using the standardized Munich-Composite International Diagnostic Interview (M-CIDI; Wittchen et al., 1998a; Wittchen and Pfister, 1997). As in the offspring studies, more than half of the patients that developed BD had a depressive rather than (hypo)manic episode as first manifestation. The question as to whether depressive episodes occurring in persons who later convert to BD are symptomatically distinct from episodes of unipolar depression cases, Pfennig et al. compared symptom profiles of depressive episodes between subject that subsequently developed (hypo)manic episodes (n = 35) or remained unipolar depressive (n = 659). It could be shown that the initial depressive episode among later converters was characterized by significantly increased suicidality (OR = 2.31), higher rates of feelings of worthlessness and excessive guilt (OR = 2.52), complete loss of pleasure (OR = 2.53) and diurnal variation (OR = 4.30). Counter to prevailing assumptions, no differences were found for hyperphagia, hypersomnia and psychomotor alterations (Pfennig et al., 2016).
The Orygen Youth Health Clinical Program is a public mental health program for young people aged 15–24 years in metropolitan Melbourne, Australia. Referrals are taken from a range of sources, including general practitioners and other primary care services, educational support services, drug and alcohol services, carers, families and young people themselves. Based on Bell’s (1992) ‘close in strategy’, Bechdolf et al. proposed Bipolar at-risk (BAR) criteria. The first criterion was being at an age of 15–25 years, the second was having had within the last 12 months (1) subthreshold (hypo)mania (i.e. at least two consecutive but not 4 days of symptoms) or (2) at least 1 week of depression and cyclothymic features or (3) at least 1 week of depression and genetic risk (i.e. a first-degree relative with BD; Bechdolf et al., 2010). To assess the predictive validity of these criteria, 559 help-seeking patients were screened. Of the eligible participants, 59 (10.6%) met BAR criteria. In total, 35 participants were included in the BAR group and 35 matched participants were selected to be in the control group. Over a 12-month prospective follow-up, five BAR patients (14.3%) converted to first-episode (hypo)mania as opposed to none in the non-BAR group (p = 0.020). Three converters were in the subthreshold mania group, two in the depression and cyclothymic features group (Bechdolf et al., 2014). Further analyses of this study sample showed that having an alcohol use disorder at baseline (75% vs 8%) or a family history of substance use disorder (67% vs 12.5%) were associated with subsequent development of BD (Ratheesh et al., 2015).
Summary
Eight prospective studies contributed data regarding psychopathological features as potential risk factors for BD. In offspring of patients with BD, anxiety followed by minor mood symptoms seem to precede major depressive and finally (hypo)manic episodes. Childhood anxiety disorder more than doubles the risk for manifestation of BD. In population-based studies, it was shown that frequent ‘ups and downs’ are predictors of BSD. Crying and being anxious/worried, being hyper-alert, being sensitive, decreased sleep, somatic complaints, being fearful and medical/physical problems were antecedents for onset of BD. The initial depressive episode in patients that later on develop BD seems to be characterized by increased suicidality, higher rates of feeling excessive guilt, complete loss of pleasure and diurnal variation. Converters within 12 months showed subthreshold manic features (at least 2 but not 4 days) or (sub-)threshold depression and cyclothymia.
Personality, temperament and character traits
In the systematic review of Christensen and Kessing (2006), prospective study data published up to April 2004 were included. They discussed that neuroticism seemed to be a risk factor of the development of depressive disorder. A connection between personality traits and development of BD, and evidence of a personality-changing effect of affective episodes needed to be further investigated (Christensen and Kessing, 2006).
Data from seven prospective studies (one offspring study, two population-based studies, three studies observing students and one study with BSD subjects) were included
In the aforementioned Canadian offspring study, Duffy et al. assessed the association of temperament and psychopathology applying the 5-item emotionality and the 5-item shyness subscales from the Early Adolescent Temperament Scale (EAS; Buss and Plomin, 1984). In this analysis spanning 0–16 years of follow-up, n = 221 offspring 13 years of age or older were included. High emotionality significantly increased the risk of psychopathology and mood disorder in at risk offspring (hazard ratio [HR] offspring 1.36 and 1.24). Psychopathology included any DSM-IV major axis one disorder not including learning disorders or ADHD; mood disorder included any DSM-IV mood disorder: all BSDs, major depression, dysthymia, cyclothymia and minor depression (Doucette et al., 2013).
Assessing all five personality traits described in the big five model (openness to experience, conscientiousness, extraversion, agreeableness and neuroticism [Goldberg, 1990]), Lonnqvist et al. (2009) found in a follow-up study of 213,443 apparently healthy male subjects (mean age 20 years), conscripted into the Finnish Defense Forces during the period 1982–1987, linkage with the Finnish Hospital Discharge Register (mean follow-up time: 14.1 years [±1.7]) that high premorbid extraversion (assessed with the Minnesota Multiphasic Personality Inventory [MMPI]; Hathaway and McKinley, 1967) predicted the future onset of BD (OR = 1.37, n = 98 bipolar cases, effect size d = 0.32). The authors discussed their findings as being somewhat contrary to that found in a Swiss conscripts sample of 3019 subjects followed-up for 13 years (Clayton et al., 1994), where no association of premorbid personality traits including none of extraversion were found. They found it most likely that the low number of conversions seen in the Swiss sample (n = 26) could explain the difference. The authors suggest including distinct personality factors and their biological substrates in models of the etiology of BD (Lonnqvist et al., 2009).
Cloninger et al. (1993) suggested relatively stable temperament traits (novelty seeking, harm avoidance, reward dependence and persistence) and character traits developing through life (self-directedness, cooperativeness and self-transcendence) with each of the constructs being related substantially to at least one of the dimensions in the Five Factor Model (De Fruyt et al., 2000). Tijssen et al. (2010) found in an analysis of 8-year follow-up of the aforementioned EDSP study that the onset of manic symptoms was associated with novelty seeking, while persistence of these symptoms was negatively associated with novelty seeking. The authors suggested that symptoms occurring in participants in the presence of the risk factor novelty seeking are transitory. Harm avoidance was associated with persistence of depressive symptoms. The temperament and character traits had been assessed with the Tridimensional Personality Questionnaire (TPQ; Cloninger, 1987). And, De Fruyt had shown that novelty seeking is strongly associated with extraversion (De Fruyt et al., 2000), so that the results of both studies are in line.
Akiskal and Aiskal have introduced the concept of sub-affective temperaments. They suggested that cyclothymic or hyperthymic temperament precedes affective disorders (Akiskal and Aiskal, 1992). Cross-sectional data suggested that the frequency of hyperthymia is higher in bipolar patients and first-degree relatives compared to controls (Kesebir et al., 2005) as well as the frequency of cyclothymia in subjects with at least one sib or first-degree relative with BD compared to controls (Chiaroni et al., 2005). Akiskal et al. (2006) showed in a cross-sectional design comparing temperament profiles of Bipolar I, II, unipolar depressive patients and healthy controls that neuroticism in unipolar depressive patients appears largely accounted for by sub-depressive (dysthymia-like) symptomatology. Among Bipolar II patients, it seems to be their habitual mood lability in terms of biphasic cyclothymic (sub-depressive and hypomanic) fluctuations which is captured in high neuroticism scores. The authors therefore suggested that elevations on neuroticism can occur for very different reasons and that re-assorting pooled items from conventional scales might be sometimes needed (Akiskal et al., 2006).
The hypomanic personality scale (HPS) was constructed by Eckblad and Chapman (1986) to provide a psychometric measure of the vulnerability for BD that is similarly defined as the concept of hyperthymic temperament. In the scale, questions are aimed at finding upbeat, gregarious and energetic people who sometimes become too euphoric and overactive. In a prospective study, Kwapil et al. (2000) showed that college students scoring high in the HPS (n = 36) were at higher risk to develop BD over a period of 13 years than students scoring low (n = 31). Blechert and Meyer showed that of 114 secondary and vocational school students those with high scores in the HPS had more manic symptoms 2 years later compared to those with low scores. Impulsivity only improved prediction when acknowledging the interaction with the HPS scores. Interestingly, in subjects with high impulsivity, fewer symptoms were found (Blechert and Meyer, 2005).
Schalet et al. (2011) analyzed the multidimensional structure of the HPS using hierarchical cluster analysis and found among others that when using the scale for predictive purposes regarding conversion to BD, it would be worthwhile to analyze it by the clusters identified by their group since their analysis suppressed total score associations. The identified clusters addressed mood volatility, social vitality and excitement. The authors suggested e.g. that mood volatility, but not social vitality and more so not excitement, might predict the onset of manic episodes (Schalet et al., 2011).
To investigate the influence of Behavioral Approach System (BAS) dysregulation, Alloy et al. (2006) selected adolescents from Philadelphia area public high schools and colleges aged 14–19 years for the Project Teen Emotion and Motivation (TEAM). In total, 9991 students were screened, following the procedures in Alloy et al. (2006) with a demographics measure and two self-report BAS sensitivity measures. A random subsample of the adolescents who met the criteria for high BAS or moderate BAS status were invited for additional screening (n = 390), where participants were administered the mood and psychosis sections of an expanded Schedule for Affective Disorders and Schizophrenia—Lifetime (exp-SADS-L) interview, as well as the Beck Depression Inventory (BDI; Beck et al., 1979) and the Altman Self-Rating Mania Scale (ASRM; Altman et al., 1997). Consistent with the vulnerability hypothesis of the BAS model of BD, high BAS participants had a greater likelihood, and shorter time to onset, of BSD than moderate BAS participants across an average of 12.8 months of follow-up (12.9% vs 4.2%), controlling for baseline depressive and hypomanic symptoms, and family history of BD. High reward responsiveness on a behavioral task and ambitious goal-striving for popular fame and financial success, but not impulsivity, also predicted first onset of BSD controlling for the covariates and BAS risk group, and ambitious goal-striving partially mediated the BAS risk group effect (Alloy et al., 2012a). As a limitation, it is important to consider that using the bipolar spectrum (as opposed to full BD) as the outcome mixes predictors with outcome since bipolar spectrum symptoms are found as predictors of full disorder.
In an additional analysis of the TEAM data, Stange et al. (2013) found over an average of 274 days follow up, that having high levels of dysfunctional attitudes (i.e. dysfunctional beliefs regarding concerns about other’s approval and performance expectations) in combination with low levels of emotional clarity (i.e. how clearly subjects experience their feelings) or high levels of brooding (i.e. the extent to which subjects engage in moody pondering), may be particularly deleterious among individuals at risk for developing BD due to high BAS sensitivity.
Molz et al. (2013) examined rates of BAS-deactivating, BAS-activating, and anger-evoking life events over a period of up to 4.5 years as a function of levels of aggression and impulsivity in a sample of 104 individuals with BSD and 96 healthy controls from the Longitudinal Investigation of Bipolar Spectrum Disorders Project (LIBS; Alloy et al., 2012b). Trait level personality differences (of hostility and impulsivity) predicted stress generation, beyond bipolar diagnosis (Molz et al., 2013).
Summary
Seven prospective studies contributed data regarding personality, temperament and character traits as risk factors for BD. In offspring, high emotionality significantly increased the risk of psychopathology and mood disorder. In population-based studies, high premorbid extraversion predicted the future onset of BD. The onset of manic symptoms was associated with novelty seeking. Students with high scores in the HPS had a higher risk to develop BD than those with lower scores or to have more manic symptoms. Research on dysregulation of the BAS showed that high reward responsiveness and ambitious goal-striving predicted onset of BSD controlled for BAS risk status. High levels of dysfunctional attitudes combined with low levels of emotional clarity or high levels of brooding might be particularly unfavorable in at-risk subjects.
Sleep and circadian rhythm
Ritter et al. reviewed the mostly cross-sectional or retrospective evidence regarding changes in sleep as an early symptom of BD. They found that sleep disturbances frequently precede BD by several years and convey an elevated long-term risk for developing any kind of mood disorder. Disordered sleep appears to emerge about the time of puberty and remains persistently elevated in individuals at high-risk. The authors stated further research, especially longitudinal studies in individuals at high-risk, to be required to characterize the type and patterns more precisely (Ritter et al., 2011).
Data from four prospective studies (two population-based and two offspring studies) were included
Using data from the aforementioned prospective EDSP study, Ritter et al. assessed whether disturbed sleep constitutes a risk factor for the later onset of BD. Disturbed sleep at baseline was quantified utilizing the corresponding items from the SCL-90-R. The compound value (insomnia-score) as an ordinal parameter for the severity of sleep disturbances was used to assess associations with the incidence of BD among participants free of major mental disorder at baseline (n = 1943) using OR from logistic regressions. Poor sleep quality significantly increased the risk for the subsequent development of BD (OR = 1.75). Regarding individual sleep items, trouble falling asleep and early morning awakening were predictive for the subsequent onset of BD. Disturbed sleep in persons otherwise free of major mental disorders appeared to confer an increased risk for the subsequent onset of BD (Ritter et al., 2015).
Frangou et al. published data from the population-based representative Tracking Adolescents’ Individual Lives Survey (TRAILS) that assessed 2230 Dutch adolescents at the ages 11, 13 and 16 years with the Child Behavior Checklist—Mania Scale (CBCL-MS), at the age of 19 years, the CIDI was used to check for psychiatric disorders (Papachristou et al., 2013). They reported the compound variable ‘disrupted sleep’ (trouble sleeping, sleeps less than other kids) with a significantly higher mean score in participants that developed BD up to age 19 years than in those who were considered healthy up to that age.
Levenson et al. (2015) analyzed the predictive value of sleep problems reported by parents and/or offspring on conversion to BD in the aforementioned BIOS study and showed small to medium effects. The OR was 0.13 for subjects with parental report of having an extreme evening circadian preference (meaning that those who converted were 7.69 times less likely such an extreme evening type). Offspring that reported frequent waking during the night were 2.82 times more likely to convert to BD (Levenson et al., 2015).
In the aforementioned Canadian offspring study, Duffy et al. found that the cumulative incidence of sleeping disorders was significantly higher in offsprings from bipolar patients compared to offsprings of healthy subjects (HR = 28.21). They discussed that it is likely that sleeping disorders will confer an increased risk of BD spectrum psychopathology; however, they had not yet the power to show a statistically significant association (Duffy et al., 2014b).
In summary, four prospective studies contributed data regarding changes in sleep and circadian rhythm as a potential risk factor for BD. Population-based studies found that poor sleep quality (especially trouble falling asleep and early morning awakening) increased the risk to develop BD. Trouble sleeping and sleeping less than other kids was found more pronounced in those that developed BD than in healthy controls. Converters among offspring of bipolar patients were less likely to be an extreme evening type but reported more often frequent waking during the night.
Cognition
Cross-sectional data on cognitive deficits in first-degree relatives of bipolar patients (Volkert et al., 2016) suggest that reduced psychomotor speed could serve as a potential endophenotype for BD which, according to the authors, should be investigated along the developmental trajectory of this disorder, also to examine whether abnormalities therein precede onset of the first mood episode. Furthermore, the division of relatives into subgroups is suggested to aid in the identification of stable trait markers and high-risk bipolar groups and could enable early prevention strategies. As to that more research using distinct and homogeneous subgroups is stated to be necessary.
Data from one prospective study were included
Bombin et al. (2013) presented results of a prospective 2-year follow-up study on early onset psychosis patients including 17 patients with early onset psychotic BD (mean age at onset 16 ± 1 years). They found the impairment in all cognitive areas (attention, working memory, verbal learning and executive functions) to be rather stable over time with no difference to other diagnostic subgroups (Bombin et al., 2013). The study results cannot be generalized to first-episode bipolar patients since only early onset cases were included and all subjects had to present with psychotic symptoms.
In summary, only one study representing the subgroup of psychotic BD contributed data regarding cognition as a potential risk factor for BD. Up to date, there is no substantiated evidence from prospective studies addressing individuals at risk or early manifest bipolar patients in general.
Life events
Data from one prospective offspring study were included
The role of life events on the onset (and recurrence) of mood episodes in offspring of bipolar patients was analyzed in the aforementioned Dutch Bipolar Offspring Cohort Study. Life events were assessed at baseline and at 1, 5 and 12 years of follow-up applying the semi-structured investigator-based Bedford College Life Events and Difficulties Schedule (LEDS; Brown and Harris, 1978) adjusted for adolescents (Monck and Dobbs, 1985) and were rated on a yearly basis from the age of 4 years onwards. The authors found that the cumulative life events load up to the first mood episode was associated with a positive coefficient. The HR was 1.14 and indicated an increased relative risk for mood episode onset per increase in unit of the cumulative life events load. The authors discussed that because of the very small sample size of subjects that manifested BD (54% developed a mood disorder, of that 24% BSD), they were not able to run separate analyses for depressive and (hypo)manic episodes. From the psychological features and social support assessed in parallel, only a passive reacting coping style altered the coefficient by more than 10%, suggesting an increase of the risk of mood episode onset in offspring with that coping style (Kemner et al., 2015).
In summary, only one prospective study contributed data regarding life events as a potential risk factor for BD. In offspring of BD patients, the relative risk for a mood episode increased with the cumulative life events load, especially in subjects with a passive reacting coping style. However, because of the small number of BD manifestations, only depressive episode onset could be analyzed.
Immunological parameters
Duffy et al. (2014a) discuss that evidence supports the association of stress, depression and activation of immune and neuroendocrine systems (Berk et al., 2011b; Gibney and Drexhage, 2013; Woiciechowsky et al., 1999), but that it is still not clarified whether differential reactivity to stress reflects a predisposition or a marker of illness activity or both.
Data from one prospective offspring study were included
Mesman et al. used blood samples from the Dutch Bipolar Offspring Cohort Study mentioned above within a longitudinal context and compared each subsample (i.e. offspring in adolescence [baseline and 1-year-follow-up], in young adulthood [5-year-follow-up] and in adulthood [12-year-follow-up]) with health controls sampled cross-sectionally. In adolescence, monocyte gene transcription activation was high in bipolar offspring (89% of the studied genes were overexpressed), which gradually decreased over time with a moderately higher level in young adulthood (36% of the genes overexpressed) and normalized in adulthood (none of the genes overexpressed). The additionally high protein level of the cytokine pentraxin (PTX3) in serum despite several discussed limitations let the authors suggest an over-activated inflammatory response system in adolescence and early adulthood of offspring of bipolar patients (Mesman et al., 2015).
In summary, only one prospective study that used longitudinal data in comparison to cross-sectional control data contributed data regarding immunological parameters as a potential risk factor for BD. The analyses suggest that the inflammatory response system is over-activated in adolescence and early adulthood of offspring of bipolar patients. Up to date, there is no substantiated evidence from prospective studies addressing individuals at risk or early manifest bipolar patients.
Morphological central nervous system changes
Data from four prospective studies were included (one twin study, one offspring study and two studies with early manifest BD patients)
Bootsman et al. (2016) reported from a longitudinal study on 50 twins from pairs discordant or concordant for BD compared to matched twins from healthy twin pairs. Two magnetic resonance imaging (MRI) assessments were conducted within a follow-up time of 7.5 years (±1.5). The authors did not find an association between liability to BD and structural changes over time in cerebral gray matter or in total brain, cerebrum, lateral and third ventricles, total cortical surface, mean cortical thickness or total cortical volume. They discuss limitations of their data such as the rather small sample size.
Papmeyer et al. (2016) published data on a sample of the Scottish Bipolar Family Study (Sprooten et al., 2011; Whalley et al., 2012). Here, there were 111 initially unaffected young adults (aged around 21±3 years) with a family history of BD (at least one first or second degree relative with BD type I) and 93 healthy controls. MRI was conducted at baseline and after 2 years. During the follow-up, 20 high-risk subjects developed MDD and two BD. Since the last mentioned were so few, they were excluded from the analysis. There were no significant differences between groups (high-risk subjects with development of MDD, high-risk subjects without development of MDD, healthy controls) in volumes of the lateral ventricles, caudate, putamen, pallidum, thalamus, hippocampus and amygdala. Additionally, no significant differences emerged between groups over time. The authors suggested to use the future planned follow-up assessments to see, which further subjects go on to develop BD to then re-analyze the data (Papmeyer et al., 2016).
Regarding morphological brain changes in early manifest patients, Farrow et al. (2005) accessed eight patients with newly diagnosed BD at baseline and after 24 months in comparison to matched healthy controls and first-episode schizophrenia patients via MRI. Patients had been recruited out of all young patients aged 13–25 years that presented 1999 or 2000 to mental health services in a region of western Sidney with psychotic symptoms and were included into the Western Sidney First Episode Psychosis Project (Harris et al., 2005). BD subjects showed progressive gray matter reduction in the anterior cingulate gyrus, which was not an area that initially differentiated them from healthy controls. The authors discussed the differences in change between early bipolar and schizophrenic disorder to be consistent with the hypothesis that while both may have a neurodevelopmental origin leading to pre-symptom onset gray matter volumetric loss, in schizophrenia continued neurodegeneration progresses in the same areas, while in BD neurodegeneration afflicts different regions (Farrow et al., 2005). Again, results cannot be generalized to BD patients since to be included into this study, they had to present with psychotic features. In conclusion of a narrative review analyzing differences of the central nervous system (CNS) changes in schizophrenic and bipolar illness, Liberg et al. (2016) proposed that a putative trajectory in BDs does not support changes at the whole brain level, while involvement of fronto-temporal cortices and insula resemble the changes seen in schizophrenia but to a lesser extent.
Bitter et al. (2011) reported on 30 adolescents aged 12 through 17 years hospitalized for their first manic/mixed episode associated with BD (recruited from the inpatient units of Cincinnati Children’s Hospital Medical Center) and 24 demographically matched healthy teens that underwent MRI scans focusing on amygdala volume at index assessment and approximately 12 months later. At baseline, there were no statistically significant differences among groups in left or right amygdala volumes. Change in left and right amygdala volumes from baseline to 12 months was significantly different among groups. Specifically, left amygdala volumes increased over time in healthy adolescents but not in adolescents with BD. Right amygdala volume did not change over time. The authors stated the need for further studies to examine the impact of prior depressive episodes or co-occurring anxiety disorders, as well as that of family history of mood disorders on amygdala volumes. Long-term prospective studies would be needed that investigate whether adults with adolescent onset BD exhibit similar amygdala abnormalities into adulthood (Bitter et al., 2011).
In general, when interpreting morphological CNS differences in an episodic illness as BD (and the argument concerns other potential markers too), it should be considered that state vs trait findings are possible (e.g. volumetric changes only present in an acute episode vs there are stable differences to healthy controls independent of the present state). Additionally, over the development of the disorder, there might be slight trait findings at the beginning with other state findings imposing themselves later on that then even differ in depressive and (hypo)manic episodes.
In summary, four prospective studies contributed data regarding morphological CNS changes as a potential risk factor for BD. No differences were found for any sub-cortical volume comparing young adults with a family history of BD that developed MDD, those that did not, and healthy controls and no differences subsequently emerged between groups over time. In first manic/mixed episode patients, no differences in left or right amygdala volumes compared to healthy controls was found at baseline. Within 12 months, however, left amygdala volumes increased in healthy but not in adolescents with BD. Right amygdala volume did not change over time. Another study showed progressive gray matter reduction in the anterior cingulate gyrus within 24 months.
Conclusion
The present review summarizes the prospective evidence base on potential risk factors for the development of BD published within the last 15 years. In total, 19 prospective studies contributed data (four offspring studies, five population-based studies, three studies observing pupils and students, one study including help-seeking subjects, three first-episode patients and three other studies).
Regarding psychopathological features, personality, temperament and character traits as well as changes in sleep and circadian rhythm, the evidence suggests that risk factors for the development of BD can already be described:
As for psychopathology, (1) childhood anxiety disorder, (2) impaired emotional regulation (frequent ‘ups and downs’), (3) crying and being anxious/worried, being hyper-alert, being sensitive, somatic complaints, being fearful and medical/physical problems and (4) an initial depressive episode with suicidality, feeling excessive guilt, complete loss of pleasure and diurnal variation and (5) proximal subthreshold (hypo)manic symptoms seem to be associated with manifestation of BD.
Character traits like high extraversion, novelty seeking, high reward responsiveness, ambitious goal-striving and a hyperthymic temperament seem to predict BD. In offspring, high emotionality increased the risk of psychopathology and mood disorder.
Looking at changes in sleep and circadian rhythm, poor sleep quality, especially trouble falling asleep, early morning awakening and frequent waking during the night, seem to increase the risk to develop BD.
These risk factors should be studied further to understand their interaction, mediation with other factors and timing in the developmental process of BD. Apart from the positive family history that is already part of the diagnostic process in symptomatic youth, childhood anxiety, and sleep problems, subthreshold (hypo)manic symptoms and certain character traits should be identified and monitored already in clinical practice as their presence likely increases risk of BD.
Up to date no substantiated evidence was found from prospective studies addressing cognitive features, life events, immunological parameters and morphological CNS changes as potential risk factors for BD. Regarding cognition, it was suggested that cognitive deficits occur around manifestation of BD and are rather stable over the course of the disease, but were not found in at-risk subjects in cross-sectional data. This would be different compared to subjects with prodromal psychosis, where cognitive impairment is found frequently and would support the caution not to generalize the data of Bombin et al. (2013) reviewed here to all bipolar at-risk subjects. As to morphological CNS changes, to our knowledge, the publications were using data of offspring cross-sectionally, so that they were not included into the present review.
Overall, especially prospectively collected data are still quite rare. What has been published so far stimulated an integrative staging model showing a development from early, non-specific risk syndromes via childhood risk syndromes regarding anxiety and sleep to the onset of minor and later major depressive episodes before the onset of (hypo)mania in young people with an established family history (Duffy et al., 2014b).
Limitations of the presented review include the sparse overall evidence found and the narrative character of the review. Additionally, a pre-defined set of potential risk factors was reviewed; however, other factors have been examined in prospective studies too. For instance, Betts et al. (2016) studied childhood neurodevelopment in the prospective pre-birth cohort Mater University Study of Pregnancy (MUSP; Betts et al., 2016) following the children for over 20 years, so that the future reviews should be even more comprehensive. Also data on IQ/grades and creativity should then be included. And, as can be seen from the present review, there are a number of prospective cohort studies running that still observe their participants and analyze data, so that there are very recent publications that could not be included any more into the review. For instance, for the section of immunological parameters from the Canadian Offspring study, Duffy et al. reported prospective data regarding cortisol secretion reporting that in offspring of bipolar patients higher daytime and evening cortisol levels might increase the risk for new-onset mood disorder (Goodday et al., 2016). Because of the comprehensive topic of the presented paper, systematic reviews each focusing on parts of the complex story of the early phase of developing BD might have to be produced.
When critically examining the evidence presented, it has to be acknowledged that it was collected in different samples: (representative) community samples, offspring of bipolar patients or early stage bipolar patients. Adding to this, definitions of individuals ‘at-risk’ vary and diagnoses of early stage BD sometimes include BSD. Here, as mentioned above, it is important to consider that using BSD (as opposed to full BD) as the outcome mixes predictors with outcome since bipolar spectrum symptoms are found as predictors of full disorder. Follow-up periods in most studies are rather short, resulting in the risk of under-detection of conversion to manifest disorder or change in risk constellations. Next, since the development of BD is complex, so are the data collected and the statistical approaches needed. With effect sizes mostly in the lower and middle range, these facts result in the need of large study samples and adequate control cohorts. And, it should be acknowledged that some of the risk factors reviewed might be non-specific risk factors of adult mood disorder, not only of BD. Finally, it has to be critically considered that patients with a first episode of BD and more so subjects at-risk for the development of the disorder usually are adolescents or young adults. The time of puberty and adolescence is frequently marked by strong emotional and social developmental changes so that the differentiation between healthy and pathological features is even more difficult than it is already with psychiatric disorders. This is particularly true for hypomanic symptomatology. Here, additional information on further risk parameters, e.g., on family history of BD, can be helpful to section off psychopathology from normal variation.
As mentioned already, the prospective study design enables to study the developmental perspective and to analyze the specific influence of certain risk factors in different periods of individual and disease development. Substantially higher resources spend to conduct longitudinal research over long periods of time compared to the resources needed for cross-sectional or retrospective studies have to be justified by reasoned research protocols and conduct, including profound statistical analyses for these complex data.
To characterize subjects at-risk apart from describing the positive family history, scales such as the HPS were used. However, to collect information on the wide range of potential risk factors, specific instruments to collect risk constellations are needed. There are at least two instruments (the Bipolar Prodrome Symptom Interview and Scale [BPSS; Correll et al., 2014b] and the Early Phase Inventory for BDs, EPIbipolar [Leopold et al., 2012]) and one criteria catalog (BAR criteria; Bechdolf et al., 2012) in the validation process.
Prospective studies addressing the described range of potential risk factors will only be conducted successfully within multi-site research networks or initiatives. For this, common standards and sets of instruments to identify and characterize at-risk subjects are needed. In Germany, for instance, within the Research Network for Psychiatric Disorders, a multicenter project funded by the Ministry of Education and Research on subjects at risk for the development of BD and subjects within the first few years of manifestation of the disorder was started in 2015 (www.bipolife.org). Within the subproject on at-risk subjects nine clinical centers are collecting clinical, imaging and genetic data on help-seeking young people visiting early detection centers that were screened positive for features of heightened risk, young patients with (still) unipolar depression and subjects with ADHD. Additionally, subjects from a representative control sample are being assessed. All subjects will be followed-up for at least 2 years within the 4-year project and beyond depending on subsequent financial support. Included into the set of factors explored are potential resilience factors helping people (and among those subjects at higher risk to develop BD) to stay healthy, since there is even less evidence published on resilience factors compared to the presented potential risk factors. Here, for instance, the amount and profoundness of social interactions, the perception of and coping with stress, as well as lifestyle behaviors such as physical activity are studied.
To summarize, the prospective study design enables the study of the developmental perspective of BD and to analyze the specific influence of certain risk factors in different periods of individual and disease development. In episodic disorders with distinguishing features often manifesting later on in disease progression, longitudinal data collection is essential. Since the etiology of BD is complex, a number of potential risk factors have been proposed, studies addressing this spectrum and resilience factors will only be conducted successfully within multi-site research networks or initiatives. The results of prospective studies will enhance the staging models for BD developed so far and enable early detection and timely adequate counseling and treatment for people that are on a trajectory to develop BD or are in their early manifest stages and thus to minimize serious negative consequences including suicidal behavior and psychosocial impairment.
Footnotes
Acknowledgements
The publication was prepared in conjunction with the project ‘BipoLife’ financially supported by the German Ministry of Education and Research (BMBF).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.