
Abstract
Keywords
Introduction
Problems of medication adherence are not unique to patients with bipolar disorder as it is an issue that impacts in many long-term conditions. The World Health Organization has reported that 50% of patients from developed countries with chronic disease do not use their medications as recommended (World Health Organization, 2003). Low adherence with prescribed treatments for any medical condition is very common (Haynes et al., 2005). In chronic illnesses generally adherence appears not to be significantly related to the type or severity of disease, quality of information provided to the patient or socio-demographic variables (Horne, 2006). Adherence is generally defined as “the extent to which patients follow instructions they are given for prescribed treatment” (Haynes et al., 2005).
Numerous interventions have been studied in an attempt to improve medication adherence in long-term conditions – automated telephone and computer-assisted monitoring, telephone follow-up, family interventions, simplified dosing, programmed reminders, special reminder pill packaging, reinforcement for adherence, crisis intervention, augmented pharmacy services – but in a Cochrane review (Haynes et al., 2005) it was found that less than half the interventions tested were associated with statistically increased medication adherence. Only 44% of the interventions studied were associated with improvements in adherence, with only 32% leading to improved treatment outcomes.
Most of the studies of interventions for improving adherence in patients with mental disorders have been conducted with people who had a diagnosis of schizophrenia or depression, and most studies had reporting issues or the numbers were too small to include in the Cochrane review (Haynes et al., 2005). Overall the interventions for long-term conditions that led to improved medication adherence were complex and involved a number of strategies and even the most effective interventions did not lead to large improvements in adherence and treatment outcomes (Haynes et al., 2005).
For bipolar disorder, Scott (2002) noted that between 30% and 50% of individuals prescribed a prophylactic mood stabilizer stopped taking medication against medical advice at least once over the course of a year. These rates of non-adherence have probably not changed since the first introduction of psychotropic medications in the 1950s, despite vast numbers of new compounds being marketed (Tacchi and Scott, 2005). In bipolar disorder non-adherence to medication has been associated with a range of poor clinical outcomes including higher rates of hospital admissions, higher rates of suicide, and recurrence of acute episodes, particularly mania (Scott, 2000). A range of factors has been identified as negatively influencing adherence: younger age, single status, male gender and low educational level (Colom and Vieta, 2002; Sajatovic et al., 2007); duration of being prescribed a mood stabilizer (Scott and Pope, 2002); polypharmacy (Patel and Anthony, 2007); and comorbid disorders such as personality disorders and substance use disorders (Colom et al., 2000). In a study of self-reported non-adherence in 429 patients with bipolar disorder, Baldessarini et al. (2008) ranked the factors significantly associated with non-adherence in multivariate modelling: alcohol dependence > youth > greater affective morbidity > various side-effects ≥ comorbid obsessive-compulsive disorder ≥ recovering from mania-hypomania.
Clinicians’ understanding of the reasons for non-adherence may be inaccurate. One study suggested that clinicians often misunderstood the reasons patients were not adherent with medication and had inaccurately identified that patients missed highs or felt well as the reasons for non-adherence (Pope and Scott, 2003). Adams and Scott (2000) found that highly adherent and partially adherent subjects differed significantly in their perception of illness severity, their beliefs about themselves and their control over the disorder and their concerns about future hospitalizations; and that perceived severity of illness and perceived benefits of treatment explained 43% of the variance in adherence and non-adherence. Two studies (Sajatovic et al., 2009a; Zeber et al., 2008) identified that access to treatment and the way in which treatment was delivered also influenced adherence. Studies examining the factors that patients identify as affecting adherence can be grouped into: illness factors (Clatworthy et al., 2007; Sajatovic et al., 2008, 2009b), personal attitudes and beliefs (Adams and Scott, 2000; Clatworthy et al., 2009; Pope and Scott, 2003; Scott, 2002), medication-related factors (Bowskill et al., 2007; Jonsdottir et al., 2009; Rosa et al., 2007) and environmental (relationship) factors (Darling et al., 2008; Zeber et al., 2008).
Reviews of the literature on factors that influence adherence (Berk et al., 2010; Busby and Sajatovic, 2010; Crowe et al., 2011) identified that illness factors included perceptions of illness severity and acceptance of illness as well as the clinical features of substance abuse comorbidity and a history of past suicide attempts. Personal attitudes and beliefs reflected individual’s beliefs about themselves and their control over the disorder and adjusting to having a chronic disorder. Issues around medication included perceived benefits of medication, concerns about negative side-effects, dissatisfaction with information about medications, doubts about the need for medication, concerns about future adverse effects and generally feeling negative about medication. Environmental issues affecting adherence reflected family stress and family coping, experiencing barriers to care, having less intense follow-up and the degree of therapeutic relationship.
A review of the literature up to 2003, on interventions that enhance treatment adherence among patients with bipolar disorder (Sajatovic et al., 2004a) found that the literature was limited but that there was some preliminary data. It found that therapies which appeared to enhance adherence were interactional, patient-focused and included family members wherever possible. Such therapies occur in the context of long-term management of the disorder that incorporates a good understanding of medications and their risks and benefits as well as education about illness awareness and illness self-management. However there have been further studies of interventions to improve medication adherence in bipolar disorder. The aim of this review is to examine studies published after the 2003 review and to update the findings.
Methods
The objective of this review was to identify which interventions enhance medication adherence in bipolar disorder, from the published literature of controlled trials between 2003 and 2011. The temporal parameters of the review were determined by a comprehensive review of similar literature published before 2003 (Sajatovic et al., 2004). A MEDLINE search for studies published in English up to May 2011 was undertaken and followed up with a manual search of references cited in articles identified by the MEDLINE search. Key search words were bipolar disorder, manic-depressive disorder, medication adherence, compliance and interventions. The abstracts of 190 articles were reviewed to identify if they met key inclusion criteria: (i) trials of interventions aimed at improving medication adherence in bipolar disorder, (ii) participants were adults (the issues of children and adolescents could be expected to be different), (iii) medication adherence as a primary or secondary outcome measure, (iv) intervention described and able to be replicated, (v) published between 2003 and May 2011, and (vi) controlled study design. Eleven studies met these criteria and were identified for systematic review. Information was then extracted on types of intervention, measurements used, participants and results.
Results
Overview of studies
Eleven studies that met inclusion criteria had been published since 2003 (Table 1). Most interventions were manualized structured interventions with some focus on psychoeducation. Three incorporated psychoeducation into a cognitive therapy model (Ball et al., 2006; Lam et al., 2005; Zaretsky et al., 2008), two into a family-focused therapy (Miklowitz et al., 2003; Rea et al., 2003) and one into an interpersonal and social rhythm therapy (Frank et al., 2005). Four interventions used structured psychoeducation programmes (Colom et al., 2005; Depp et al., 2007; D’Souza et al., 2010; Sajatovic et al., 2009c). One intervention was a two-hour facilitated discussion on future treatment preferences (Wilder et al., 2010).
Study characteristics
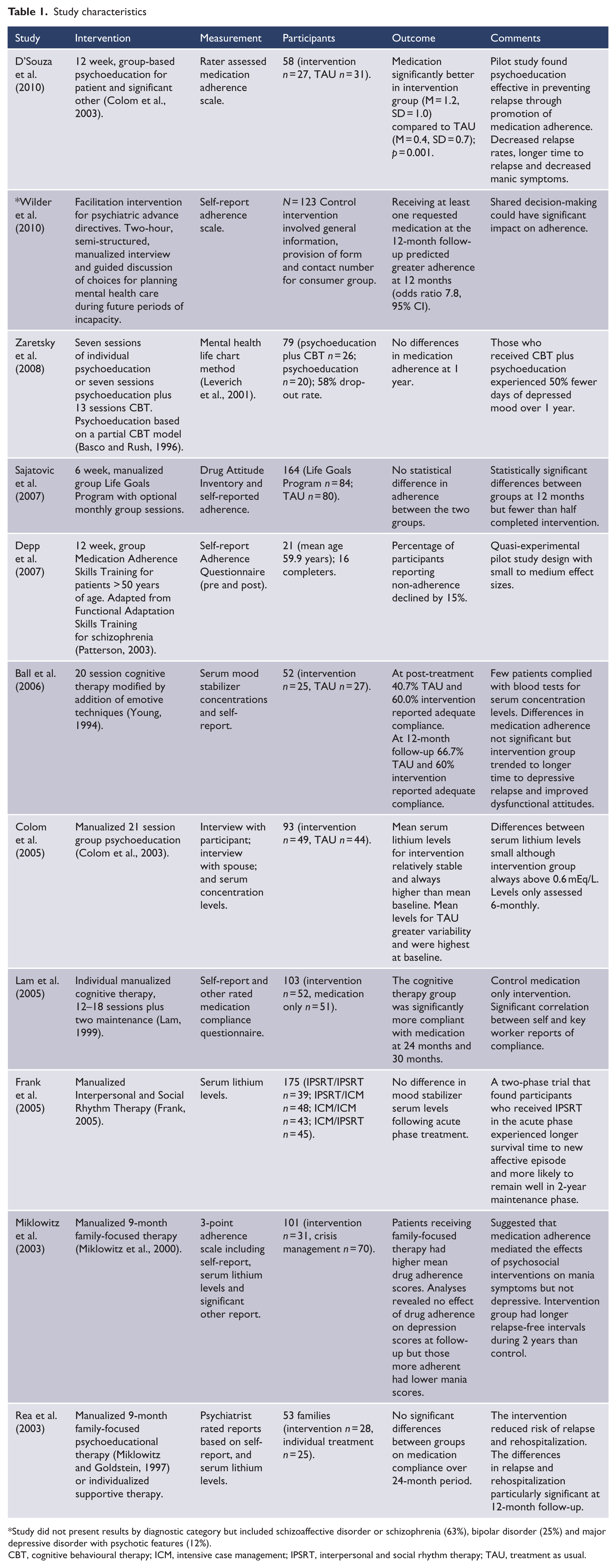
Study did not present results by diagnostic category but included schizoaffective disorder or schizophrenia (63%), bipolar disorder (25%) and major depressive disorder with psychotic features (12%).
CBT, cognitive behavioural therapy; ICM, intensive case management; IPSRT, interpersonal and social rhythm therapy; TAU, treatment as usual.
Four interventions were delivered in a group format, five in an individual format, and two in a family format. One study was included (Wilder et al., 2010) despite not providing a separation of results according to diagnostic category (schizophrenia or schizoaffective disorder, bipolar disorder, and depression with psychotic features) because it was a study with a simple but effective intervention. Most studies used non-standardized self-report measures using Likert scales, with half of the studies supplementing these with serum concentration levels. The sample sizes of the studies included in this review ranged from 21 to 175.
The studies were all randomized controlled trials apart from the Depp et al. (2007) 12-week Medication Adherence Skills Training Programme for elderly adults, which measured pre- and post-adherence. Only one study had adherence as its primary outcome measurement while the others had clinical outcomes. Differences in relation to inclusion criteria, length of intervention and measurement occurred across all studies. The length of euthymia required for participation varied from 1 to 6 months. The family-focused therapy studies (Miklowitz et al., 2003) required patients to be actively involved with their families or significant others and one other study required a companion to be available (D’Souza et al., 2010). Most of these studies excluded patients with substance use disorder. It could be expected that patients with longer periods of euthymia, who did not have substance use disorders and/or had active family involvement, may respond better to psychosocial interventions.
Effects on adherence
Five studies reported significant improvements in adherence as a result of their disorder-specific psychosocial interventions. In a small (n = 58) pilot study (D’Souza et al., 2010) of group-based psychoeducation and treatment as usual, significant improvement in medication adherence was found in the psychoeducation group. This intervention of 12 × 90 minute sessions was based on Colom and Vieta’s (2006) manual with follow-up conducted at 60 weeks. Another study based on the same model of psychoeducation provided in a group format found in a sub-analysis of data (Colom et al., 2005) that the mean serum levels for the intervention were significantly higher at 6, 18 and 24 months. The one cognitive therapy intervention (Lam et al., 2005) demonstrating improvement found that a 20-session cognitive therapy intervention versus medication demonstrated improved compliance at 30 months. The study of family-focused therapy (Miklowitz et al., 2003) that involved 9 months of family-focused psychoeducation and crisis management found that patients who received the intervention had higher mean drug adherence scores at 2 years. The Wilder et al. study used an intervention which involved a 2-hour facilitated advance directive (Wilder et al., 2010). This could not really be classified as a disorder-specific psychosocial intervention and data are not available for the separate group of bipolar disorder (Wilder, personal communication). The study did show that if patients were given the opportunity to state their medication preferences in an advance directive they were more likely to be adherent.
Clinical outcomes
Despite only five studies demonstrating improved adherence, all studies (apart from the facilitated advance directive one that did not publish clinical outcomes) demonstrated improved clinical outcomes. In a subsequent report on the clinical outcomes of the psychoeducational intervention, Colom et al. (2009) found that at the 5-year follow-up, time to any recurrence was longer for the psychoeducation group, they had fewer recurrences of any type and they spent less time acutely ill. D’Souza et al. (2010) demonstrated that 12 × 90 minute sessions of psychoeducation delivered to the patient and a companion decreased relapse rates, had longer time to relapse and decreased manic symptoms. The study of psychoeducation compared with psychoeducation plus cognitive behavioural therapy (Zaretsky et al., 2008) found that those who received cognitive behavioural therapy plus psychoeducation experienced 50% fewer days of depressed mood over 1 year. Cognitive therapy was also effective in improving time to depressive relapse in Ball et al.’s (2006) study. However another study (Lam et al., 2005) found that while the cognitive therapy group had significantly better outcome in terms of time to relapse in the first year, this was less apparent at 30 month follow-up. In their two-phase trial of IPSRT, Frank et al. (2005) found that participants who received IPSRT in the acute phase experienced longer survival time to a new affective episode and were more likely to remain well in a 2-year maintenance phase. In the trials of family-focused therapy (Miklowitz et al., 2003; Rea et al., 2003) the intervention groups had longer relapse-free intervals over 2 years.
Discussion
The review identified 11 studies since the review of Sajatovic et al. (2004), which were sufficiently rigorous to add to the literature on psychosocial interventions to improve adherence in bipolar disorder. Similarly to the Sajatovic et al. (2004) review we found that while many interventions did not improve adherence they did improve clinical outcomes. No features of the therapy or of the clinical group reliably differentiated between the five studies which improved compliance and the six which did not. An interesting and new intervention, a 2-hour facilitated advanced directive, demonstrated that if patients were prescribed > 1 medication identified in the directive they were more likely to be adherent. However, this study only had a relatively small number of patients with bipolar disorder (n = 31), which is too small a number for meaningful sub-analysis.
Characteristics of studies with positive outcome
No characteristics of the psychosocial intervention, mode of delivery, length of delivery or method of measurement appeared to differentiate the studies with a positive outcome from those that showed no improvement. The studies demonstrating a positive outcome used psychoeducation, cognitive therapy and family-focused therapy but there were other studies of these interventions that were unable to show an improvement in adherence (Ball et al., 2006; Depp and Jeste, 2004; Rea et al., 2003; Sajatovic et al., 2009c; Zaretsky et al., 2008). Apart from the Wilder et al. (2010) and the Lam et al. (2005) studies, the mode of delivery for successful interventions was either group or family, but these modes were also used in the studies that demonstrated no improvement (Depp and Jeste, 2004; Rea et al., 2003; Sajatovic et al., 2009c).
The interventions across all studies were similar in that they were structured, manualized and involved < 21 sessions. They all incorporated psychoeducation about the symptoms of bipolar disorder, promoted lifestyle regularity and encouraged patients to identify personal triggers and early warning signs. The control interventions were mostly treatment as usual (three of the five in those studies with improved adherence and four of the other six). Two studies that used the same treatment (Miklowitz et al., 2003; Rea et al., 2003) with different outcomes both used active control interventions (individual management and crisis management).
One study (Wilder et al., 2010) used facilitated psychiatric advance directives, legal documents that allow individuals with severe mental illness to document preferences for future treatment if they lose decisional capacity during a psychiatric crisis. Facilitated advance directives are patient-centred plans to coordinate future treatment in a forum that encourages patients to express their preferences about psychiatric medication in a non-confrontational manner. None of the other studies described adherence in terms of patient preference. However, as noted, this study was not specific to bipolar disorder.
Definition and measurement
The definition of adherence in the studies reviewed was not always articulated and can only be assumed from the measurement tool used, i.e. number of missed doses or serum levels. This does not identify if patient preferences were included in the process of prescribing but it is reasonable to assume that it was congruent with the way in which adherence has been defined by the World Health Organization as the extent to which the patient’s behaviour follows the recommendations of the healthcare provider (Sabate, 2003). Others have suggested that adherence is a more collaborative process in which the patient is an active decision-maker rather than a passive recipient of clinical recommendations. It may also be useful to consider adherence as not static but a dynamic process responsive to patient, illness and environmental factors (Crowe et al., 2011).
Roe et al. (2009) found that people who stop taking psychiatric medication go through a process of conflict and ambivalence regarding their medications and that the decision to take medications or not was influenced by the process in which it was prescribed. Zeber et al. (2008) also found that better clinical relationships improved adherence. In particular, providers who conveyed confidence in patients’ ability to participate in treatment and advocated keeping in regular contact proved to be highly influential on good adherence. This was also supported by Gaudiano et al. (2008), who found that the patient’s treatment expectancies and therapeutic alliance in pharmacotherapy were predictive of outcomes in bipolar disorder.
The method for measurement of adherence did not differentiate the successful interventions from the unsuccessful ones in this review. The studies reviewed used a variety of measures to assess adherence including self-report, other report and serum levels. There is some ambiguity in the literature regarding reliance on self-reports. Expert guidelines (Velligan et al., 2009) for improving adherence in serious mental disorders suggest that objective measures of adherence such as pill counts, pharmacy records and serum levels where possible be used to assess adherence. However, in a naturalistic study of patients with either schizophrenia or bipolar disorder, it was found that using the MARS-5 (Horne, 2006) as a self-report measure, the correlation between self-report and serum concentration at 0.52 was reasonably high given variations in drug metabolizing (Jonsdottir et al., 2010). Scott (2000) has also found that self-report correlated highly with serum levels. While all measures of adherence have their problems and inaccuracies it has been suggested that self-report in the context of a collaborative relationship is a practical strategy for assessing adherence (Osterberg and Blaschke, 2005). It is also relevant that one study in our review (Ball et al., 2006) was unable to collect serum levels because of patients’ resistance.
Clinical implications
According to clinical guidelines after the resolution of an acute illness episode in bipolar disorder, long-term prophylaxis is required to prevent recurrence (Royal Australian and New Zealand College of Psychiatrists Clinical Practice Guidelines Team for Bipolar Disorder, 2004). However rates of relapse in bipolar disorder (even when taking prophylaxis) are as high as 40% in the first year, 60% in the second year and 73% over 5 years or more (Gitlin et al., 1995). Perlis et al. (2006) have identified that even patients receiving optimal medication are likely to have recurrences, have trouble holding jobs, maintaining relationships and getting along with significant others. While appropriate drug treatment is critical, attention must be given to psychosocial contributors and consequences (Royal Australian and New Zealand College of Psychiatrists Clinical Practice Guidelines Team for Bipolar Disorder, 2004).
It is routine clinical practice to measure serum levels of lithium carbonate and sodium valproate but it is not clinically feasible to routinely measure for other mood stabilizers, antipsychotics or benzodiazepines. Reliance on serum levels to measure adherence is thus somewhat limited to two mood stabilizers, and can be manipulated by patients who can take extra doses in the days coming up to measurement. In clinical practice self-report in the context of a collaborative relationship becomes a more feasible option. Also most of the studies in this review were reporting the results of efficacy rather than effectiveness studies. The degree to which these results apply to real-life clinical populations is not well established. The studies are primarily limited to adherence to mood stabilizers (lithium and valproate) or combinations of all medications used, with little known about how patients may use other medications for symptom management. Some patients are often more willing to use symptomatic medication if they are unable or unwilling to tolerate prophylactic medication.
It is of clinical interest that most studies found that although their interventions did not improve adherence they did improve clinical outcomes. Sajatovic et al. (2010) have identified that data supporting the link between adherence and clinical outcome is equivocal. They have suggested that this may be related to the context of adherence measurement, problems associated with calculating average adherence to multiple medications and reliance on single measures of adherence. Consequently they have suggested assessing adherence for each medication separately and combining adherence measurements.
A Cochrane review (Haynes et al., 2005) of interventions to improve medication adherence in long-term conditions found that the common component to successful interventions was more frequent interaction with patients with attention to adherence. Shoemaker and de Oliveira (2008) have identified that the unremitting nature of chronic medication use often leads the individual to question the need for medication and subsequently seek to exert some control over their treatment experience by altering the way they take medication. Because of the complex issues associated with medication decision-making, a number of studies have highlighted the importance of the clinical relationship (Gaudiano et al., 2008). This relationship needs to focus on exploring the patient’s perceptions of the bipolar disorder and medication use. Sajatovic et al. (2006) have identified that the discrepancies between actual and hoped-for outcomes from medications had an important impact on adherence.
A review of patients’ perception of medication adherence (Crowe et al., 2011) found that the patient’s perception of the severity of the disorder, their beliefs about themselves and the impact of the disorder and their perception of treatment influenced their decisions to be adherent or not. Treatment perception was related to accessibility of services and the quality of the relationship with their clinician. It would seem reasonable that the context of a disorder-specific psychosocial intervention is ideal for addressing these issues.
A meta-analysis (Miklowitz and Scott, 2009) has found that disorder-specific psychosocial interventions for bipolar disorder augment mood stabilizers in reducing rates of relapse over 1–2 years. This meta-analysis suggested that mediating mechanisms for increasing time to relapse include but are not limited to: increasing medication adherence, teaching self-monitoring, early intervention with emergent symptoms, enhancement of interpersonal functioning and family communication. Miklowitz and Scott (2009) have identified that a disorder-specific intervention for bipolar disorder needs to incorporate the following characteristics: an individualized formulation of the problems experienced with bipolar disorder; the model of therapy is shared openly with the patient; there is a clear rationale for the techniques used; and there is an emphasis on psychoeducation and skill development. Change is attributed to the efforts of the patient, not just those of the therapist, and the patient is encouraged to use illness management techniques post-therapy.
Negotiated adherence
Busby and Sajatovic (2010) have suggested that poor or suboptimal symptom response to treatment appears to be associated with reduced adherence, which emphasises the need for clinicians to be extremely responsive to patient perceptions of the value of medication treatments and the benefit-risk ratio of pharmacotherapy. One intervention that was less resource-intensive but effective in promoting adherence has potential either as a stand-alone intervention (which has been trialled) or in combination with other structured therapies (not yet trialled). This advance directive intervention (Wilder et al., 2010) places patient choice and patient participation as central to achieving adherence. Khazaal et al. (2009) have proposed a cognitive therapy approach to the development of advance directives that emphasises self-determination, acknowledges and values the meanings the patient attaches to the disorder and its symptoms (cognitive representational model) and promotes concordance. This effective approach reflects an emergent theme in the treatment of bipolar disorder, collaborative care.
Bauer (2001) has promoted a collaborative model as an organization of care that emphasizes (a) development in the patient of illness management skills and (b) support to provider capability and availability to engage patients in the timely joint decision making regarding their illness. Sajatovic et al. (2005) have identified that patients perceive the ideal collaborative model as one in which the individual has specific responsibilities, such as coming to appointments and sharing information, whereas the provider has specific responsibilities such as keeping abreast of current state-of-the-art prescribing practices and being a good listener. Participants in that study identified the importance of an interactional relationship that has the flexibility to allow for individual differences, fluctuations in illness severity and the demands and realities of everyday life. In this context there is more likely to be ‘buy-in’ for medication adherence. As Strauss and Johnson (2006) have identified, a strong treatment alliance encourages greater acceptance of bipolar disorder and psychopharmacological interventions and thus may contribute to improved medication adherence and clinical outcomes. This approach recognizes that patients with bipolar disorder often have a good understanding of what is needed to keep well (Russell and Browne, 2005). Our findings also suggest that it may be important to involve family members or significant others in interventions aimed at improving adherence.
Conclusion
Rates of medication non-adherence in bipolar disorder are not significantly different from those for other long-term conditions. While only a few of the interventions reviewed improved adherence, most improved clinical outcomes. This raises questions about the relationship of adherence to clinical outcome. Further research needs to explore this relationship in more detail with particular emphasis on how medication is prescribed and what options are available to the patient. This could include involving patients as active partners in decision-making rather than positioning them as passive recipients of medical orders. It may also mean more systematic use of symptomatic treatments for patients who do not respond to, or are unwilling to take, prophylactic medication. Given the increasing evidence for the efficacy of adjunctive psychosocial treatments for bipolar disorder, such interventions could incorporate negotiated adherence into their treatment protocols.
Footnotes
Declaration of Interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.