
Abstract
Objective:
To provide the first Australian population-based estimates of the association between bullying and adverse mental health outcomes and suicidality among Australian adolescents.
Method:
Analysis of data from 3537 adolescents, aged 14–15 years from Wave 6 of the K-cohort of Longitudinal Study of Australian Children was conducted. We used Poisson and linear regression to estimate associations between bullying type (none, relational-verbal, physical, both types) and role (no role, victim, bully, victim and bully), and mental health (measured by the Strengths and Difficulties Questionnaire, symptoms of anxiety and depression) and suicidality.
Results:
Adolescents involved in bullying had significantly increased Strengths and Difficulties Questionnaire, depression and anxiety scores in all bullying roles and types. In terms of self-harm and suicidality, bully-victims had the highest risk of self-harm (prevalence rate ratio 4.7, 95% confidence interval [3.26, 6.83]), suicidal ideation (prevalence rate ratio 4.3, 95% confidence interval [2.83, 6.49]), suicidal plan (prevalence rate ratio 4.1, 95% confidence interval [2.54, 6.58]) and attempts (prevalence rate ratio 2.7, 95% confidence interval [1.39, 5.13]), followed by victims then bullies. The experience of both relational-verbal and physical bullying was associated with the highest risk of self-harm (prevalence rate ratio 4.6, 95% confidence interval [3.15, 6.60]), suicidal ideation or plans (prevalence rate ratio 4.6, 95% confidence interval [3.05, 6.95]; and 4.8, 95% confidence interval [3.01, 7.64], respectively) or suicide attempts (prevalence rate ratio 3.5, 95% confidence interval [1.90, 6.30]).
Conclusion:
This study presents the first national, population-based estimates of the associations between bullying by peers and mental health outcomes in Australian adolescents. The markedly increased risk of poor mental health outcomes, self-harm and suicidal ideation and behaviours among adolescents who experienced bullying highlights the importance of addressing bullying in school settings.
Introduction
In Australia and internationally, mental disorders make a major contribution to ill health among adolescents (Mathews et al., 2011; Patton et al., 2016). Self-harm also makes a significant contribution to the burden of disease and is the second leading cause of death among 15- to 24-year-old Australians (Mathews et al., 2011; Patton et al., 2016). In 12- to 17-year-old Australians, the 12-month prevalence of depression and anxiety were recently estimated to be 5% and 7%, respectively (Lawrence et al., 2015). In Australia, 1 in 10 teenagers have self-harmed, 1 in 13 teenagers have contemplated suicide, 1 in 20 have made a plan to take their own life and 1 in 40 have attempted suicide (Lawrence et al., 2015). Reducing mental ill health and self-harm among adolescents is an urgent public health problem in Australia and elsewhere.
Scott and colleagues argue that bullying is one of the most modifiable risk factors for mental illness that could be targeted at a population level (Scott et al., 2013). Bullying among school-aged children is now recognised as a major public health problem in developed countries (Klomek et al., 2010). Bullying is defined when an adolescent is exposed to, repeatedly over time, negative actions on the part of one or more other students, between whom there is an imbalance of power or strength (Olweus, 2013). One in four Australia school students aged 8–14 years old experiences bullying-victimisation frequently (Cross et al., 2009; Forero et al., 1999). Bullying may take many different forms including physical (physical threats and harm), relational (excluding and spreading rumours) and verbal (teasing and name calling) (Smith et al., 2002), although it must be noted that there is inconsistency in the literature regarding how these are defined. In the Victorian Adolescent Health and Wellbeing Survey, 31% of adolescents experienced verbal bullying, 11% physical bullying, 14% were socially excluded and 18% had rumours spread about them (Thomas et al., 2015). Boys experience more physical victimisation, such as hitting and shoving, and girls more indirect, relational victimisation, such as social exclusion and rumour spreading (Cullerton-Sen and Crick, 2005). Bullying behaviour can also be classified according to the adolescent’s role in bullying, with the principle roles defined as victim, bully, bully-victim (those who are themselves victims and also bully others) (Haynie et al., 2001) and bystanders or uninvolved students (Salmivalli, 1999).
Internationally, the impact of bullying on children and adolescents has been associated with poor mental health including overall psychological health (Rigby, 2003), low self-regard (Egan and Perry, 1998), depression and anxiety (Arseneault et al., 2006) and violent behaviour (Nansel et al., 2003). These associations have been reported in longitudinal studies (Moore et al., 2014; Wolke et al., 2013), suggesting a causal relationship. There also appears to be a dose–response relationship, with children who suffer prolonged bullying having worse mental health outcomes (Rigby, 2003; Scott et al., 2013). Experiencing bullying is also a risk factor for suicide and suicidal behaviours (Holt et al., 2015; Kim et al., 2005; Klomek et al., 2009; Van Geel et al., 2014), and in some cases, these operate independently of other suicide risk factors such as depression, sex, socioeconomic status and family structure (Kaltiala-Heino et al., 1999; Kim et al., 2005). There is also previous evidence that different roles in bullying, and different forms of bullying, have different patterns of associations with negative outcomes. For example, bully-victims are most vulnerable to the negative outcomes of bullying (Holt et al., 2015; Swearer et al., 2001), compared to those who only bully or are only victims. Relational victimisation has been associated with worse mental health outcomes, such as depression, than physical victimisation (Baldry, 2004).
Evidence regarding the relationships between bullying and mental health and suicidality are largely from the international literature. Studies in Australia have mainly been state-wide, focused on one type of bullying (such as cyberbullying [Hemphill et al., 2015] or relational bullying [Zimmer-Gembeck and Pronk, 2012]), or risk factors, such as school climate (Turner et al., 2014) or internalising or externalising problems (Kelly et al., 2015). In this paper, we use data from the Longitudinal Study of Australian Children (LSAC) to provide the first Australian population-based estimates of the relationships between bullying and mental health and suicidal behaviour. We extend previous studies by investigating the relationships between bullying type and role, and a range of mental health outcomes and self-harm and suicidality.
Method
Data source
We used Wave 6 data from the LSAC Kindergarten (K) cohort – a nationally representative longitudinal study of Australian children. Details of the methods have been described elsewhere (Soloff et al., 2005). Data collection commenced in 2004 with two cohorts: 5107 children aged 3–19 months (Cohort B) and 4983 children aged 4 years 3 months to 5 years 7 months (Cohort K) and has been repeated biennially. This analysis focused on Cohort K, who were aged 14–15 years in Wave 6. Study informants included the child, parents, carers and teachers. Data collection methods included self-completed questionnaires, face-to-face interviews and computer-assisted interviews (Australian Institute of Family Studies [AIFS], 2014). The sampling frame was the Medicare Australia database which has near complete coverage of Australian residents (Soloff et al., 2005). Children were randomly sampled from 311 randomly selected postcodes in Wave 1 (Soloff et al., 2005). The response fraction was 59% with 4983 children recruited in Wave 1; retention has been above 80% for subsequent waves (AIFS, 2014). At Wave 6, there were 3537 participants.
The LSAC is conducted in a partnership between the Department of Social Services (DSS), the AIFS and the Australian Bureau of Statistics (ABS). The study has ethics approval from the (AIFS, 2015) Ethics Committee. Full and informed written consent was obtained from caregivers for Wave 1, and both caregivers and children for Wave 6.
Exposure variables – experience of bullying
In Wave 6, adolescents were asked 11 questions about their experiences of bullying. These items were drawn from the School Climate Bullying Scale (Cornell, 2011; Cornell and Brockenbrough, 2004) and the Edinburgh Study of Youth Transitions and Crime (Smith et al., 2001), and were modified slightly for the Australian context. Questions were introduced with For the next questions, please think about things that might have happened to you at school, or out of school. Include texts, Facebook etc. as well as face-to- face contact. Do not include things that happened with your close family members (such as brothers and sisters).
The questions were first asked about experiences in the past year, and then the past month. In this paper, we used responses from questions in the last month only. The stem question was ‘Did the following happen in the past month (30 days)?’, with the following types of bullying listed: someone hit or kicked me on purpose, someone grabbed or shoved me on purpose, someone threatened to hurt me, someone threatened to take my things, someone said mean things to me or called me names, someone tried to keep others from being my friend, someone did not let me join in what they were doing, someone used force to steal something from me, someone hurt me or tried to hurt me with a weapon, someone stole me things to be mean to me and someone forced me to do something I didn’t want to do.
The response options were yes or no.
Participants were also asked whether they had bullied anyone (yes/no) using the same 13 forms of bullying asked in relation to perpetration (i.e. In the last month, did you grab/shove someone on purpose?).
Categorical variables were constructed to classify bullying type and role. Bullying type was classified as none, relational-verbal bullying, physical bullying and both physical and relational-verbal, using the School Climate Scale classification of bullying (Cornell, 2011). Physical bullying included being hit, kicked, grabbed, shoved, hurt, having something stolen by force and having things stolen. Relational bullying included keeping others from being the victim’s friend and stopping the victim from joining in. Verbal bullying included threatening the victim and saying mean things/calling names. Given the overlap between the verbal and relational constructs, we followed the precedent set by Yen et al. (2015), and combined them to form a construct that encompassed both types (verbal and relational) and named this ‘relational-verbal’ bullying.
For bullying roles, victimisation was defined as having been the victim of one or more of the 13 bullying behaviours described above in the last month. If respondents indicated that they had bullied in the past month on any of the 13 bullying behaviours, they were classified as bullies. Bullying role was defined as non-involved (children who neither bullied nor were bullied in the past month), victims (children who were bullied in the past month, but did not bully), bullies (children who bullied in the past month, but were not victims) and bully-victims (children who were both bullied and bullied others in the past month).
Outcome variables
A range of outcomes relating to mental health (including depression, anxiety, suicidality) and general psychological wellbeing were examined in relation to bullying type and role.
Social and emotional wellbeing
Adolescent socio-emotional difficulties were assessed using the Strengths and Difficulties Questionnaire (SDQ). The SDQ contains 25 items across five domains: emotional symptoms, conduct problems, hyperactivity-inattention, peer problems and pro-social behaviour (Goodman, 1997). Respondents rated the frequency with which the different behaviours occurred in the previous 6 months, using a 3-point scale: 0 (not true), 1 (somewhat true) and 2 (certainly true). Responses to questions from the first four domains were summed to produce a total difficulty score ranging from 0 to 40 (Goodman, n.d.), with higher scores indicating more problems. The total difficulties score has been shown to have dimensionality as a measure of children’s mental health (Goodman and Goodman, 2009), with those classified as borderline or abnormal at higher risk of psychopathology (Goodman and Scott, 1999), and is well correlated with other measures of psychopathology among children (Goodman and Scott, 1999).
Anxiety
Symptoms of anxiety were assessed using Children’s Anxiety Scale, 8 items (CAS-8), which has eight questions that are modified versions of items on the Spence Anxiety Scale (short form) (Spence, 1998). CAS-8 included questions such as: ‘I worry about things’, ‘I feel afraid’, ‘I feel nervous’ and ‘I wake up feeling scared’. Potential answers were never, sometimes, often and always. CAS-8 has good internal consistency (α = 0.80) (Spence et al., 2003).
Depression
Depressive symptoms were measured using the Short Mood and Feelings Questionnaire (Short MFQ) for children (based on the Diagnostic and Statistical Manual of Mental Disorders, Third Edition [DSM-III] criteria for depression; Angold et al., 1995). The Short MFQ is a self-report depression checklist of core symptoms for children and adolescents aged 8–16 years (Angold et al., 1995). The short MFQ is a 13-item single-factor scale derived from a 34-item long MFQ (Costello et al., 1991) and items include ‘I felt miserable or unhappy’, ‘I didn’t enjoy anything at all’ and ‘I felt I was no good anymore’. Response options were true, sometimes, not true. While not diagnostic, these questions serve as an indicator of depressive symptoms, and demonstrate good reliability (Angold et al., 1995).
Means and standard deviations with 95% confidence intervals (CIs) were calculated for total scores on the SDQ, depression and anxiety scales, with higher scores indicating an adolescent at a higher risk of mental health disorders. The proportions of adolescents in the high-risk SDQ and depression categories who were also involved in bullying were also calculated (Online Appendix). The anxiety scale did not have cut-offs and thus analysis was only linear.
Self-harm and suicide
Questions regarding self-harm and suicide in Wave 6 were drawn from the National Survey of Mental Health and Wellbeing (Slade et al., 2009). Respondents were asked whether, during the past 12 months, they had considered self-harm such as overdosing on pills or cutting or burning oneself. They were then asked whether they had self-harmed in the past 12 months using the same methods. Response options were yes or no. Only reports of performing self-harm (not thoughts of self-harming) were included in analyses.
Three items measuring suicidality were used: suicide ideation, suicidal planning and suicide attempt. Respondents were asked whether they had, in the past 12 months, thought of suicide or made a plan to attempt suicide. They could select yes or no. Responses from these questions informed the suicide ideation and suicide plan variables, respectively. They were then asked how many times in the past 12 months they had attempted suicide. Potential answers included zero times, one time, two or three times, four or five times, and six or more times. Responses were re-categorised into a binary variable: none vs any attempts.
Confounders
We considered several covariates to potentially act as confounders, predicting both bullying experiences, and the mental health and suicidality outcomes. Covariates included in regression models as potential confounders included sex (male/female), household type (one-parent, two-parent), language spoken at home (English, language other than English), household income (AUD1–AUD41,599; AUD41,600–AUD77,999; AUD78,000–AUD103,999; and AUD104,000+), parental education (at least one parent finished Year 12, no parent finished Year 12) and Aboriginal or Torres Strait Islander heritage (yes/no).
Missing data
After respondents with missing data on exposures, confounders and outcomes were excluded, the total analytical sample ranged between 2304 for models investigating self-harm and suicidal ideation, to 2324 for models involving depression. Missing data for specific variables were bullying-victimisation (5.7%, n = 202), bullying-perpetration (5.7%, n = 202), SDQ total score (5.4%, n = 192), depressive symptoms (5.5%, n = 193), anxiety symptoms (5.5%, n = 194), self-harming (6.1%, n = 216), suicidal ideation (6.1%, n = 215), suicidal plan (6.1%, n = 215), suicide attempts (5.9%, n = 209), parent’s education (0.5%, n = 16), household type (5.3%, n = 188), income (18%, n = 638) and Aboriginal or Torres Strait Islander descent (17.5%, n = 620). Missing data analysis demonstrated the exposures and outcomes did not vary by gender, parental education, household type or income. There was some evidence that missing data on exposures, outcomes and income were more likely in households where at least one parent in the household spoke a language other than English.
Statistical analysis
All analyses were conducted in Stata/SE 14 (StataCorp LP, 2012) using the ‘svy’ commands to accommodate sample design characteristics including stratification and sampling weights, although this was not used to analyse male suicide attempts because numbers were too low, and as such this outcome was not measured. The default setting for the svy command is VCE (robust).
The weighted prevalence of bullying for all mental health outcomes according to type of bullying (non, physical, relational-verbal or both) and role (bystander, victim only, bully only or bully-victim) was calculated. Poisson regression was used to examine the association between bullying type and role and self-harm and suicidality. Poisson regression yields estimates of the prevalence rate ratios (PRRs), which is a direct comparison of prevalence between groups. The PRR is recommended for cross-sectional studies particularly when the outcome is not rare. The magnitude of association is lower than the prevalence odds ratio (POR) with estimates converging with decreasing prevalence of an outcome (Zocchetti et al., 1997). Linear regression was used to obtain estimates of the association between the different bullying types and roles and SDQ, depressive and anxiety symptoms. The beta coefficients represent differences in the different outcomes on the linear scale. Regression models were adjusted for potential confounders including sex, household type, language spoken at home, household income, parental education and Aboriginal or Torres Strait Islander heritage. We conducted complete case analysis.
Results
Descriptive characteristics
The demographics of the sample are shown in Tables 1 and 2. Most adolescents came from two-parent households (72%), spoke English at home (64%) with at least one parent who had completed Year 12 (62%) and 49% were female. In all, 3% identified as Aboriginal or Torres Strait Islander. Over 50% of the sample lived in households with household incomes of more than AUD104,000. This reflects the fact that more advantaged households are over-represented in LSAC, although the sample is largely seen to be representative of the Australian population (Soloff et al., 2005).
Descriptive characteristics of Wave 6 of K-cohort of LSAC in analysis.
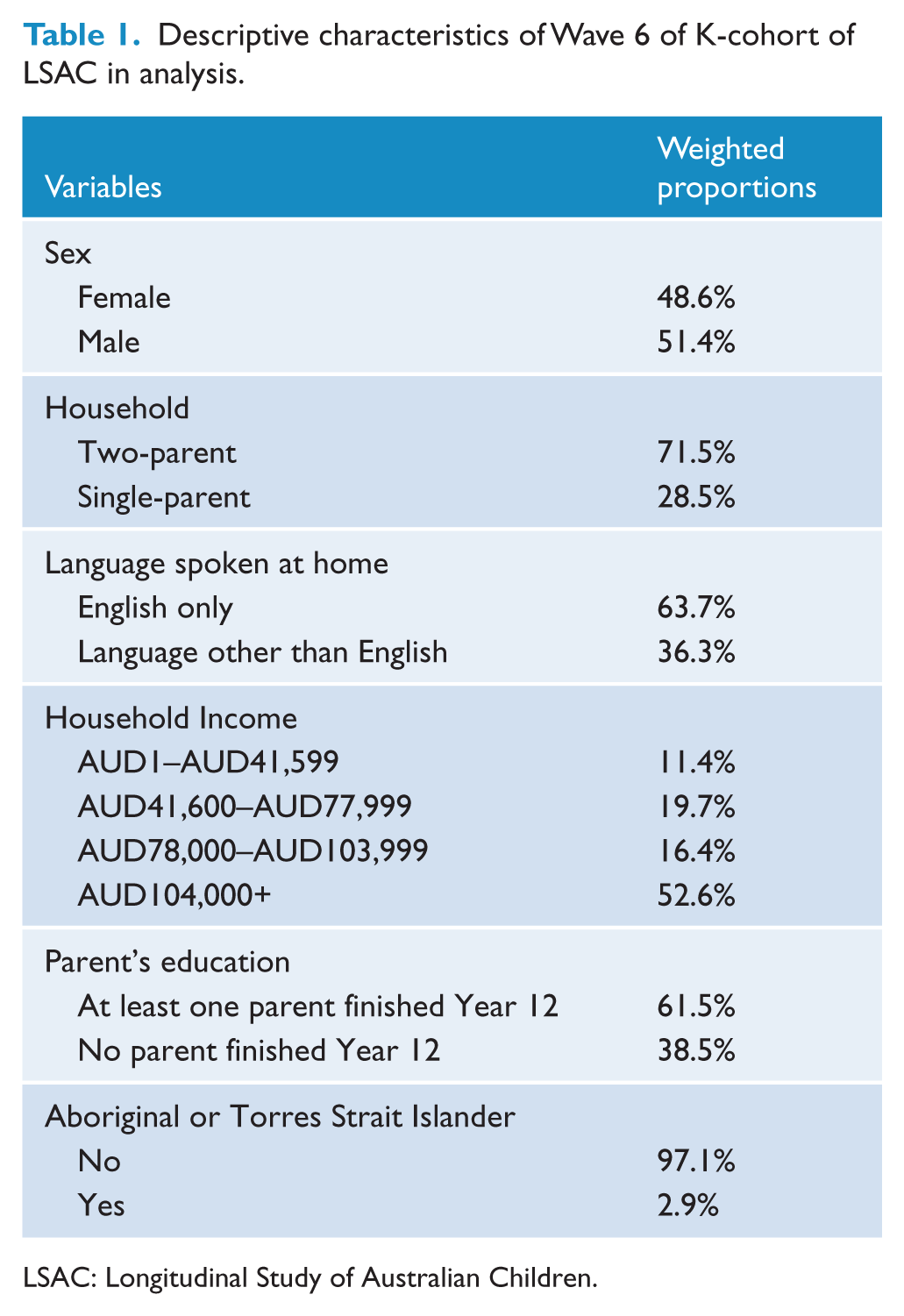
LSAC: Longitudinal Study of Australian Children.
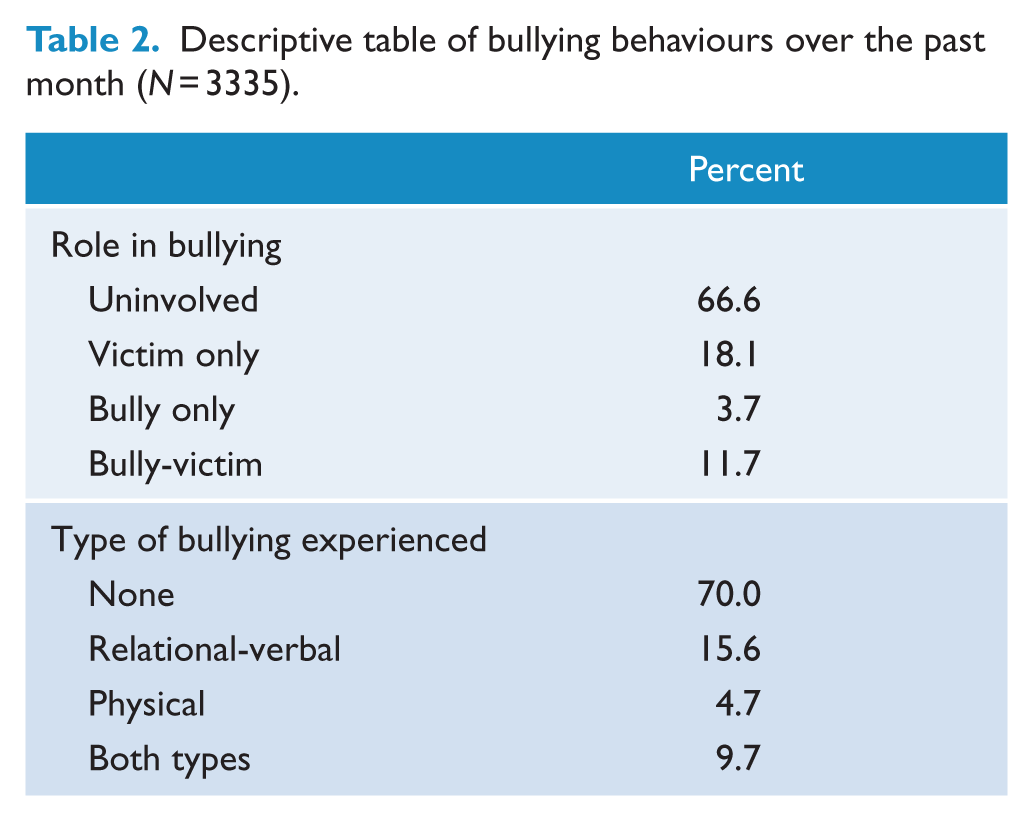
Descriptive table of bullying behaviours over the past month (N = 3335).
Prevalence of bullying roles and behaviours
Over one-third (33.9%) of respondents reported being involved in bullying behaviours in the past month (Table 2). Just over 18% were bullied by others (victims), 3.9% bullied others but were not bullied themselves (bullies) and 11.8% were both bullied and bullied others (bully-victims). A greater proportion of females reported being victims (58.2%) compared to males (41.8%) and more males reported being bullies compared to females (69.2% vs 30.8%). More males identified as being bully-victims than females (61.1% vs 38.9%). Regarding the type of bullying adolescents experienced, 15.6% adolescents said they experienced relational-verbal bullying, 4.7% physical bullying and 9.7% experienced both types. Relational-verbal bullying was reported by more females (67.1% vs 32.9%), while more males experienced physical bullying than females (79.2% vs 20.8%).
Mental health and bullying
Mental health and bullying roles
Adolescents involved in all bullying roles (victim, bully, bully-victim) scored higher on the anxiety and depressive symptoms scale and had higher SDQ scores (Tables 2–4) than non-involved adolescents (a higher SDQ score indicates poorer socio-emotional wellbeing). Bully-victims had the highest mean total SDQ score (14.3, 95% CI [13.6, 15.0]), compared to 8.3 (95% CI [8.0, 8.6]) for uninvolved adolescents. Victims had the highest mean scores in the anxiety scale and depressive symptoms scale (8.5, 95% CI [8.0, 9.0]; and 8.6, 95% CI [8.0, 9.3], respectively), compared to uninvolved adolescents’ mean scores of 5.0 (95% CI [4.8, 5.2]) and 4.1 (95% CI [3.9, 4.4]), respectively (see Table 3).
Associations between bullying (role and type) and anxiety, depression and SDQ scales (mean scores [95% CI]).
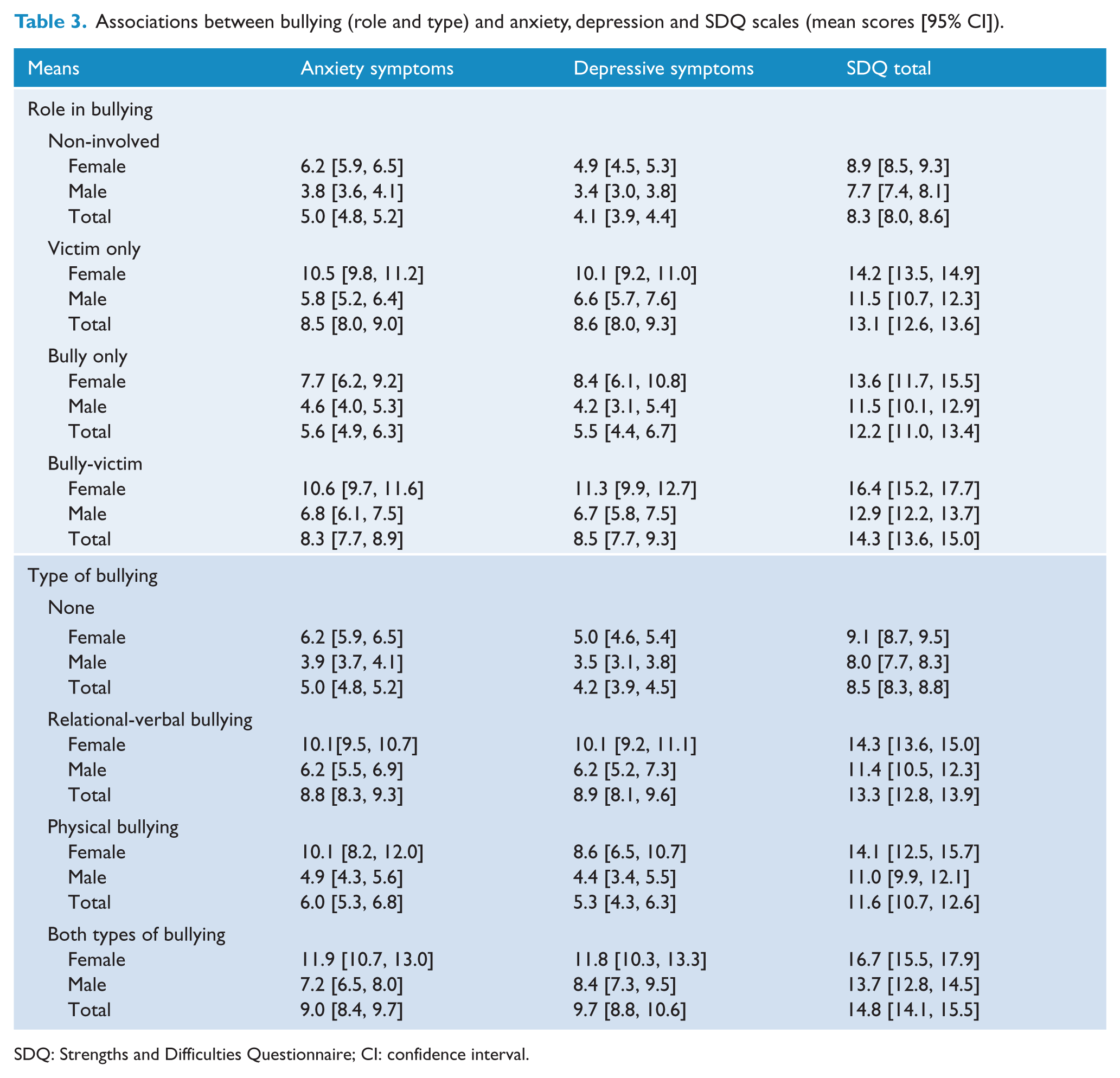
SDQ: Strengths and Difficulties Questionnaire; CI: confidence interval.
Multivariate linear regression (95% CI) of associations between bullying (role and type) and depression, anxiety and SDQ.
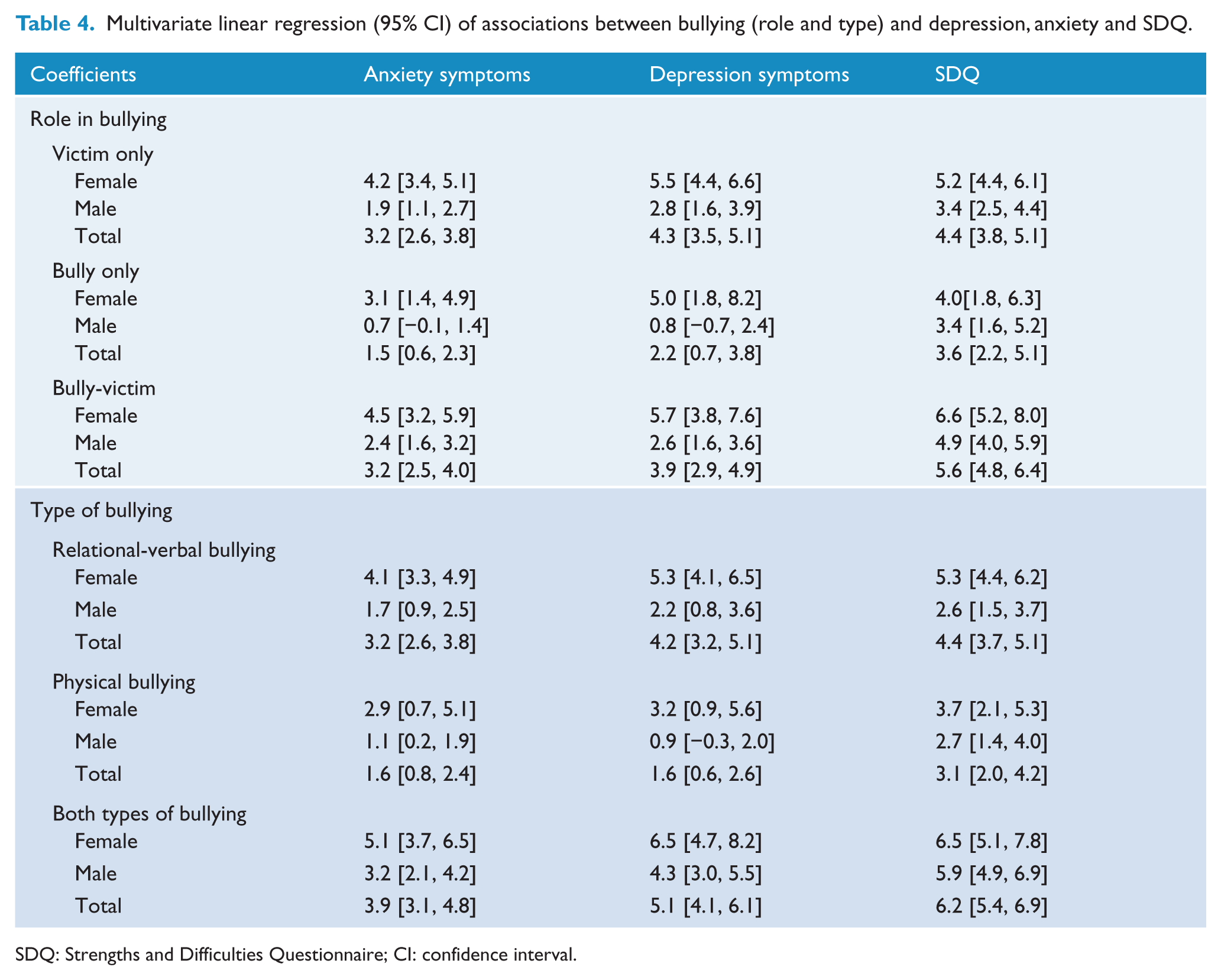
SDQ: Strengths and Difficulties Questionnaire; CI: confidence interval.
Linear regression analysis also demonstrated that mental health was worse among adolescents involved in bullying (refer to Table 4). After adjusting for potential confounders, anxiety and depressive symptoms were higher among victims, with an increase of 3.2 points (95% CI [2.6, 3.8]) in the anxiety scale and 4.3 points (95% CI [3.5, 5.1]) on the depression scale relative to those who were uninvolved. The mean SDQ scores of victims were 4.4 points higher (95% CI [3.9, 5.1]) than non-involved adolescents. Compared to uninvolved adolescents, bully-victims scored 3.2 points higher on the anxiety scale (95% CI [2.5, 4.0]), 3.9 points higher on the depressive scale (95% CI [2.9, 4.9]) and 5.6 points higher (95% CI [4.8, 6.4]) in SDQ score. In the analyses stratified by gender, boys and girls scored significantly higher on all mental health scales if they were involved in bullying than their same-sex peers who were not involved, with the exception of male bullies.
The following were adjusted for confounders: language of parents, parental education, Aboriginal or Torres Strait Island heritage, household type and household income.
Mental health scales and the different types of bullying
Adolescents who experienced any type of bullying also had higher mean scores on the mental health scales compared to those who were not bullied (Table 3). The highest scores across all three outcomes were found for those who experienced both types of bullying who scored 9.0 (95% CI [8.4, 9.7]), 9.7 (95% CI [8.8, 10.6]) and 14.8 (95% CI [14.1, 15.5]) for anxiety, depression and SDQ, respectively. The corresponding scores for no bullying (none) were 5.0 (95% CI [4.8, 5.2]), 4.2 (95% CI [3.9, 4.5]) and 8.5 (95% CI [8.3, 8.8]).
Linear regression (Table 4) demonstrated significant positive relationships between all types of bullying and the mental health scales. Those who experienced relational-verbal bullying, physical bullying or both types of bullying all had higher SDQ scores (4.4 points, 95% CI [3.7, 5.1]; 3.1 points, 95% CI [2.0, 4.2]; and 6.2 points, 95% CI [5.4, 6.9], respectively), depressive symptoms score (4.2 points, 95% CI [3.2, 5.1]; 1.6 points, 95% CI [0.6, 2.6]; and 5.1 points, 95% CI [4.1, 6.1], respectively) and anxiety symptoms (3.2 points, 95% CI [2.6, 3.8]; 1.6 points, 95% CI [0.8, 2.4]; and 3.9 points, 95% CI [3.1, 4.8], respectively) compared to those not bullied. The significantly higher scores on all outcomes were found for boys and girls when analyses were stratified by gender. When analysing the numbers of adolescents determined to be in the high-risk category for depression, and in the borderline and abnormal categories for SDQ, we found that there was a higher proportion of adolescents involved in bullying in these groups (Table Online Appendix).
Suicidality and bullying
Bullying role and suicidality
Adolescents involved in bullying had higher prevalence of self-harm and suicidal behaviour compared to non-involved adolescents (Tables 5 and 6). The prevalence of self-harm in victims, bullies and bully-victims was 18.6%, 10.3% and 20.2%, respectively, compared to 5.3% of uninvolved adolescents. Just over 15% of victims (15.2%), 13% of bullies and 19.9% of bully-victims had ideas of suicide compared to uninvolved adolescents (4.8%) and more victims, bullies and bully-victims had made a plan to attempt suicide in the last 12 months (13.7%, 7.9% and 17.3%) compared to those uninvolved (3.6%). In terms of actual suicide attempts, 3.0% of adolescents uninvolved in bullying had ever attempted suicide, while 6.9% of victims, 5.1% of bullies and 9.6% of bully-victims had attempted suicide.
Prevalence (%) (95% CI) – bullying and suicidal behaviour.
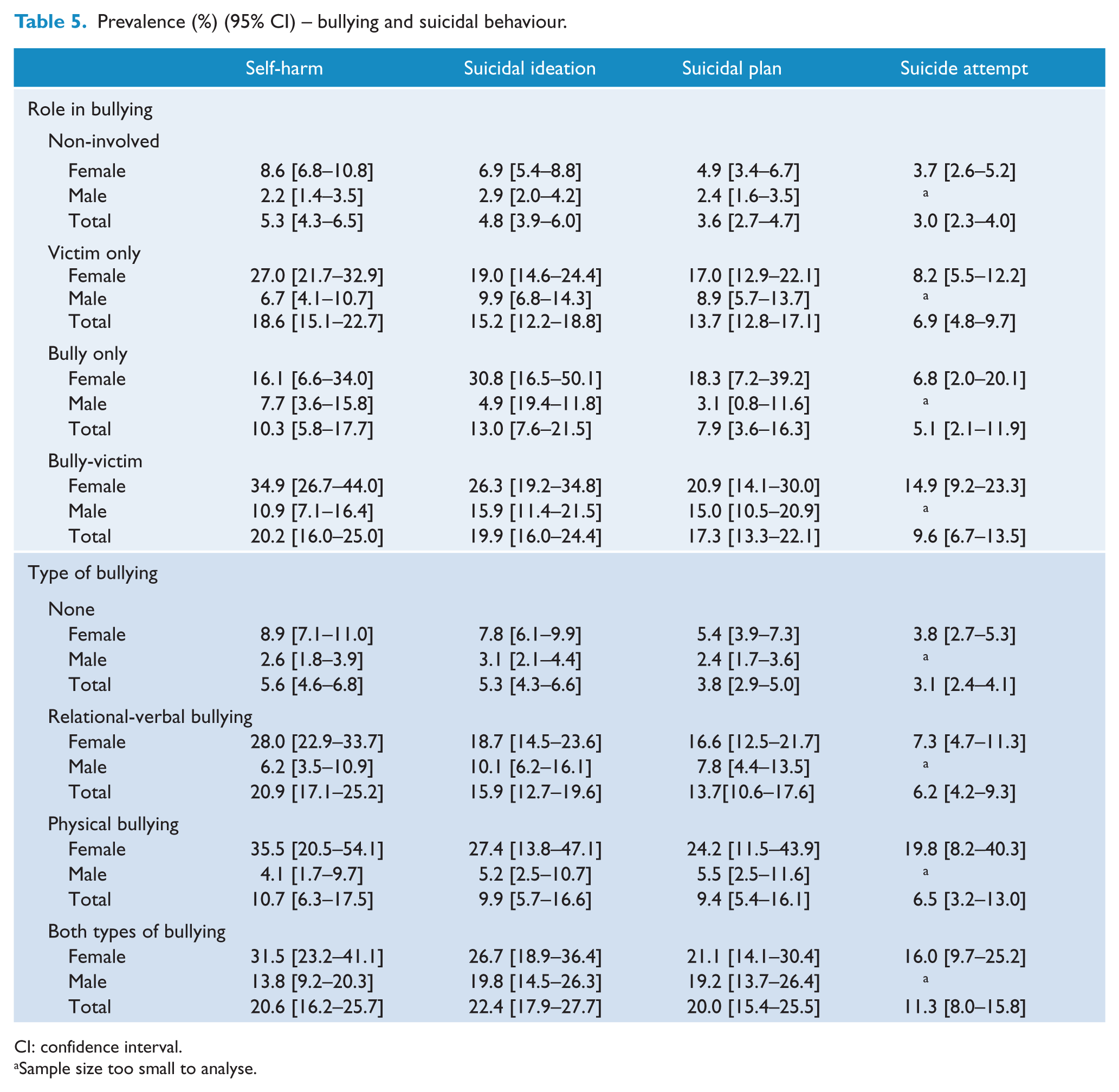
CI: confidence interval.
Sample size too small to analyse.
Poisson regression (%) (95% CI) – bullying and suicidal behaviours.
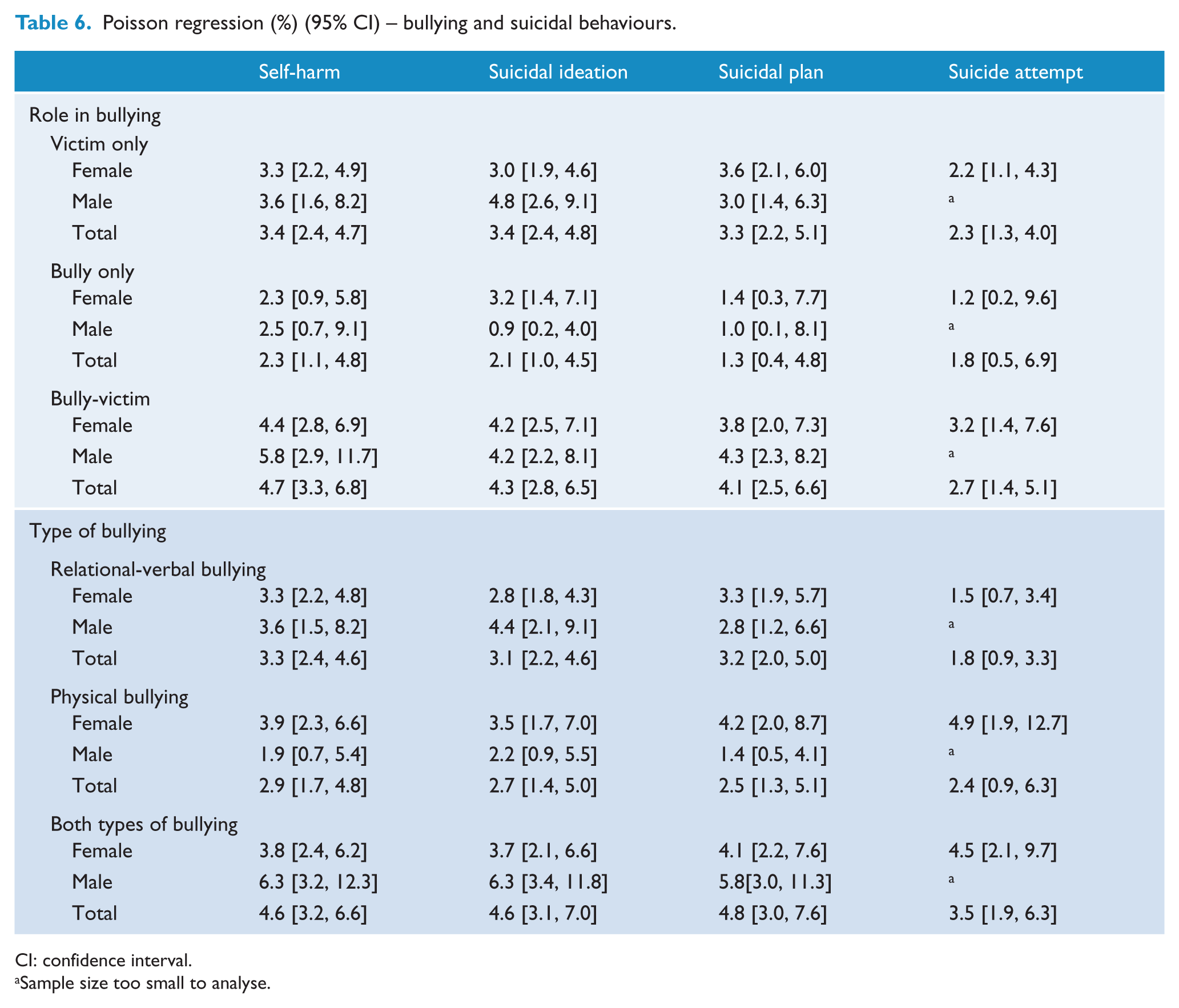
CI: confidence interval.
Sample size too small to analyse.
In Poisson regression analyses, there were significant associations between bullying and self-harm and suicidality (Table 6). Victims were more likely to have self-harmed (PRR 3.4, 95% CI [2.4, 4.7]), to have ideas about suicide (PRR 3.4, 95% CI [2.4, 4.8]) and made a plan to commit suicide (PRR 3.3, 95% CI [2.2, 5.1]) than adolescents uninvolved in bullying. They were also over twice as likely to have attempted suicide (PRR 2.3, 95% CI [1.3, 4.0]). Males who identified as victims were more likely to have self-harmed and to have ideas of suicide compared to uninvolved males. Bullies were 2.3 (95% CI [1.1, 4.8]) times more likely to have self-harmed than uninvolved adolescents, and 2.1 times (95% CI [1.0, 4.5]) more likely to have ideas of suicide. Bully-victims had the highest risk of self-harm and suicidality, being 4.7 times (95% CI [3.3, 6.8]) more likely to have self-harmed, 4.3 times (95% CI [2.8, 6.5]) more likely to have suicidal ideation, 4.1 times (95% CI [2.5, 6.6]) more likely to have made a plan to commit suicide and 2.7 times (95% CI [1.4, 5.1]) more likely to have attempted suicide. Male bully-victims were at the highest risk of self-harm, suicidal ideation and suicidal planning compared to uninvolved males.
The following were adjusted for confounders: language of parents, parental education, Aboriginal or Torres Strait Island heritage, household type and household income.
Bullying type and suicidality
Adolescents who experienced any type of bullying had a higher prevalence of self-harm and all suicidal behaviours (Table 5). Self-harm was most common among adolescents who experienced relational-verbal bullying (20.9%) or both relational-verbal bullying and physical bullying (20.6%). By comparison, just under 11% of adolescents who experienced only physical bullying self-harmed, and 5.6% of those who did not experience bullying self-harmed. The prevalence of suicidal ideation and plans were highest among adolescents who experienced both relational-verbal and physical bullying (22.4% and 20%) followed by relational-verbal only (15.9% and 13.7%), physical only (9.9% and 9.4%) with adolescents who were not bullied (5.3% and 3.8%) having the lowest prevalence.
After adjusting for confounders, compared to those experiencing no bullying (none), relational-verbal bullying was associated with a 3.3 times (95% CI [2.4, 4.6]) increased prevalence of self-harm, 3.1 times (95% CI [2.2, 4.6]) higher prevalence of suicidal ideation and 3.2 times (95% CI [2.0, 5.0]) increased prevalence of suicidal planning. Relational-verbal bullying was not significantly associated with suicide attempts (p = 0.076) but still showed a positive relationship. Physical bullying was also associated with an increased risk of self-harm, suicidal ideation and planning, with PRRs of 2.9 (95% CI [1.7, 4.8]), 2.7 (95% CI [1.4, 5.0]) and 2.5 (95% CI [1.3, 5.1]), respectively. When compared to females who did not experience bullying, females who experienced physical bullying were significantly more likely to self-harm or display suicidal ideation or other suicidal behaviour. Adolescents who experienced both physical and relational-verbal bullying had an increased prevalence of self-harm (PRR 4.6, 95% CI [3.2, 6.6]), suicidal ideation (PRR 4.6, 95% CI [3.1, 7.0]), suicidal planning (PRR 4.8, 95% CI [3.0, 7.6]) and suicide attempts (PRR 3.5, 95% CI [1.9, 6.3]). Males and females who experienced both types of bullying had much higher risk of self-harm and suicidal behaviours.
Discussion
Using high-quality data from a large population-based study of Australian adolescents, we demonstrate that involvement in bullying – as a bully, victim or both – is associated with much worse mental health and an elevated risk of suicidality. These findings pertained to both males and females and were found across all mental health outcomes (anxiety, depression and socio-emotional difficulties) and all measures of self-harm and suicidal behaviours. Victims of bullying (victims only and bully-victims) were at highest risk of these adverse outcomes. Relational-verbal and physical bullying were associated with poor mental health and higher risk of self-harm and suicidal behaviour; however, the risks were higher for adolescents exposed to relational-verbal bullying only (e.g. name calling or social exclusion) or relation-verbal bullying as well as physical bullying (e.g. hitting, kicking). Given that one-third of 14- to 15-year-olds in our study reported involvement in bullying in the past month, the associations of bullying with these outcomes are highly concerning.
Our findings are consistent with previous international studies which have shown that bullies and victims are at a higher risk of poor mental health (Rigby, 2003) including depression and anxiety (Arseneault et al., 2006; Turner et al., 2014). Previous cross-sectional studies have also shown that children and adolescents involved in bullying have increased risk of suicidal ideation and suicidal behaviours (Holt et al., 2015; Roeger et al., 2010), a relationship that is consistent for younger and older age groups and males and females (Van Geel et al., 2014). Like our study, victims (Kaltiala-Heino et al., 1999; Rigby and Slee, 1999) and bully-victims (Kaltiala-Heino et al., 1999; Kim et al., 2005; Klomek et al., 2010) were at highest risk of self-harm and suicidal behaviour. In particular, bully-victims seem to be at high risk of all deleterious outcomes, adolescents who are characterised as having high levels of aggression and dysregulated emotions (Salmivalli and Nieminen, 2002). In terms of the types of bullying experienced, a recent study found that the experience of verbal and relational bullying, physical bullying or both increased the risk of suicidal ideation (Yen et al., 2015), although they found only adolescents who experienced verbal and relational bullying or both relational-verbal and physical bullying reported more suicide attempts. Relational victimisation has also previously been linked to poorer mental health on measures such as depression and anxiety (Zimmer-Gembeck and Pronk, 2012).
As the first population-based study of bullying in Australian adolescents, we provide the first comprehensive account of the deleterious effects of bullying on adolescent mental health and suicidality. An added strength of our study is our comprehensive analyses of the different roles and types of bullying on multiple mental health outcomes and suicidal behaviours and the stratification of results by gender. The fact that we find consistent associations between involvement in bullying and different mental health and suicidal outcomes provides weight to the study’s findings.
Limitations of this study include the over-representation of advantaged families in the LSAC sample. Rates of mental health or suicidal behaviours may be higher in more disadvantaged populations who are under-represented in this sample, potentially underestimating the true prevalence of outcomes. Post hoc analyses in this sample demonstrated that those in the lowest income category were likely to report higher levels of suicidal behaviours, poor mental health and bullying. Additionally, this analysis is cross-sectional and causality cannot be definitively ascertained. It is possible that these results are due to reverse causation, as adolescents with mental health issues may be more likely to report bullying. Bullying and mental health outcomes were self-reported and measurement error is likely. The LSAC does not provide a strict definition of bullying to respondents, and does not capture several key components of bullying, such as power imbalance and repetition. It is difficult to do so in a short instrument as necessitated by a large-scale population study. The concept of repeated exposure was not considered in this current paper; further exploration using LSAC follow-up questions on the frequency of experience or perpetration of behaviours may be an important next step to explore multiple exposures. As such, it is acknowledged that some of the items used in this present paper could be classified as criminal victimisation rather than bullying if they are isolated events. LSAC also does not assess the concept of perceived impact or severity of the bullying, considered an important aspect of defining bullying by some authors.
Missing data may also result in bias; however, missing data on bullying and mental health outcomes were only 5–6%. Missing data analysis (reported in the methods) showed no evidence that missing data on exposures or outcomes varied by key covariates. There was 18% missing data on income which could also introduce selection bias; however, we did not find that any variables predicted missingness on income, other than language spoken by parents, with children with at least one parent in the household who spoke a language other than English more likely to have missing income data (data not shown). Additionally, models where income was not included produced similar results.
These results identify many areas for further research. With further waves of data collection, longitudinal analyses could be conducted to examine trajectories of mental health and suicidal behaviour in relation to bullying over time. Longitudinal analyses would provide better evidence of the causal relationship between bullying and mental health and suicidality.
These results underscore the need for urgent attention to reduce bullying among Australian adolescents. This could involve the implementation of programmes to identify high-risk adolescents, such as bully-victims and evidence-based interventions, to reduce bullying in schools. For example, we calculated that a 20% reduction in bullying could be associated with a 11.4% reduction in the proportion of adolescents who self-harm, an 11.2% reduction in suicidal ideation, 11.8% in suicidal planning and 10.4% reduction in suicidal attempts (Online Appendix). This demonstrates the potential significant effects a reduction in bullying could have on Australian adolescents.
Conclusion
Among adolescents, bullying by peers is associated with poorer overall mental health, including an increased risk of depression and anxiety. Adolescents involved in or experiencing bullying, both male and female, are also at a higher risk of self-harm, suicidal ideation and attempts. Given that one-third of Australian adolescents are involved in bullying in the last month, our findings are of considerable public health importance and highlight the importance of addressing bullying through population-based interventions.
Footnotes
Declaration of Conflicting Interests
The views expressed in the submitted article are the authors own and not an official position of the institution or funder.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.