
Abstract
Objective:
Distinguished authors in the field have repeatedly alerted psychiatrists of the alarming trends in the treatment of bipolar disorders: decline of lithium use, paralleled by the increase of prescribing anticonvulsants and second-generation antipsychotic drugs. Research has been conducted in order to explore the factors that led to this development and to provide arguments for the need to reverse this trend.
Method:
This paper represents a narrative review of the literature containing retrieved research articles focusing on the efficacy of lithium. The papers included in this overview were published prior to June 2016; additional papers were identified by searching the reference lists of reviewed articles. Taking into account the amount of literature available, no search can be exhaustive; on the other hand, the studies consulted, all of which explore the effectiveness of various compounds, may have their own limitations as well.
Results:
The evidence of the effectiveness of lithium in the treatment of acute mania, acute bipolar depression and the prevention of manic and depressive episodes is compelling. Lithium is the most effective augmentation agent in treatment-resistant depression. Its anti-suicidal effects are well established. The neuroprotective effects of lithium have been demonstrated in case-control studies and in population-based research. It has been established that starting lithium early in the course of the disorder reduces the rates of treatment non-response.
Conclusions:
Despite abundant evidence regarding the efficacy of lithium and its effectiveness in the treatment of bipolar disorders, its use is declining at the beginning of the 21st century. It is of paramount importance to keep reminding psychiatrists and educating physicians about the unique properties of lithium and about monitoring patients treated with lithium, since it has been suggested that lithium should once again become the first-line treatment for bipolar disorders.
It’s terrible … to think that all I’ve suffered, and all the suffering I’ve caused, might have arisen from the lack of a little salt in my brain.
Half a century ago …
Psychiatry started to change in 1949 after the introduction of lithium and continued changing over subsequent decades owing to the discoveries of neuroleptics and antidepressants (ADs).
During the 1970s and 1980s, lithium was truly the first-line choice for the treatment of bipolar disorder, while carbamazepine was used for patients who did not respond to lithium therapy or could not tolerate it. The term ‘mood stabilizer’ was not in use.
During episodes of acute mania, agitated patients were often treated with neuroleptic drugs needed to calm them, help them sleep and provide the time overlay for the psychiatrist to do the necessary work-up before starting treatment with lithium. Psychiatry residents were being educated about the serious side effects of neuroleptics. They were also warned about the susceptibility of patients with bipolar disorder to developing extrapyramidal symptoms (EPS) and the risk of tardive dyskinesia (TD), which was substantially greater compared to patients with schizophrenia. As soon as the acute episode subsided and the stabilization period started, the psychiatrist would gradually taper antipsychotic medications and lithium monotherapy was then continued in a considerable number of patients.
Bipolar depression, which is often severe and melancholic, was treated with the only medications available at the time: tricyclic ADs (TCA) or heterocyclic ADs. Well aware of the risk of the switch, psychiatrists always combined TCAs with lithium (or carbamazepine) to reduce that risk. After the resolution of depression and the period of stabilization, lithium monotherapy was again recommended to a greater number of patients as continuation treatment. At that time, there were only a few agents available to treat manic-depressive illness, while treatment guidelines did not exist.
Trends in the treatment of bipolar disorders (Is more less?)
Over the past 30 years, we have witnessed dramatic changes in the psychopharmacological armamentarium. A large number of treatments have been evaluated and found to be effective in the treatment of different phases of bipolar disorders. Those medications differ significantly with respect to the presumed mechanisms of action and side effects. There is a wide range of choice of medications and the number of possible combinations is even greater. Occasionally, treatment regimes and combinations are insufficiently supported by empirical results (Gitlin and Frye, 2012; Malhi et al., 2012a). Numerous guidelines have been published and are being frequently updated in an attempt to synthesize a large quantity of new information. However, the guidelines are not always easy to implement in everyday clinical practice, among other reasons also due to the fact that they are based on evidence coming from studies in which participants are not representative of the patients in real-world clinical situations (Grunze, 2013; Licht, 2001).
New ADs of several classes have emerged. These drugs have been announced ‘safe’ and having a favorable side-effect profile. There have been reports of some of them being associated with a reduced risk of switch in comparison with TCAs (Parker and Parker, 2003; Peet, 1994). Also, some of these drugs have been claimed to be effective in the treatment of subgroups of patients with bipolar depression (Altshuler et al., 2003) and were therefore being widely prescribed. The notion of the ‘safety’ of new ADs in the treatment of bipolar depression was later disputed and doubts were raised about their safety and efficacy (Ghaemi, 2008; Ghaemi et al., 2003; Goldberg and Ghaemi, 2005; Leverich et al., 2007). Regardless of this, however, a large number of patients with bipolar disorders still receive them as monotherapy (Baldessarini et al., 2007).
Atypical antipsychotics (AAPs) are at present widely used in the treatment of bipolar disorders. A ‘more favorable side-effects profile’ of AAPs has been reported regarding the reduced risk of EPS and TDs, which strongly encouraged physicians to use these antipsychotics in the treatment of bipolar disorder, not simply in the treatment of acute mania, but also as augmentation in the treatment of depression (Valenstein et al., 2006), as well as in maintenance treatment. As a result, a large number of patients with bipolar disorder receive AAPs over the prolonged period of time (Malhi et al., 2011), although the risk of EPSs and TDs is substantial and many AAPs are related with the occurrence of metabolic syndrome. AAPs are increasingly used for long-term treatment of bipolar disorders in spite of the fact that there is no convincing evidence for long-term prophylaxis of any of them (Malhi et al., 2011). The number of long-term trials regarding their efficacy is not large and the majority of these trials use enrichment design. In addition, none of the tested AAPs have the same degree of independent replication for maintenance treatment as lithium does. For that reason, the role of AAPs as mood stabilizers is still uncertain (Geddes and Miklowitz, 2013).
The term ‘mood stabilizers’, introduced in the 1990s, became popular despite the fact that it does not depict the mechanism of action of a drug but rather some of its clinical effects. Furthermore, there is considerable disagreement about the proper definition of a mood stabilizer. According to less restrictive definitions (a drug that decreases the frequency or severity of any type of episode and does not worsen the severity or frequency of others; a drug that possesses the efficacy in treating both manic and depressive symptoms), a large number of different medications could be included in this group, such as antipsychotics and anticonvulsants (AC). On the other hand, using a more restrictive definition (a drug with antimanic efficacy, AD efficacy and efficacy in the prevention of manic and depressive symptoms), the number of ‘mood stabilizers’ reduces to one only: lithium (Bauer and Mitchner, 2004; Malhi et al., 2009; Malhi and Goodwin, 2007).
What is a classic?
All guidelines and textbooks dedicated to the treatment of bipolar disorders refer to lithium as a first-line treatment, as a treatment of choice or a gold standard. Lithium is considered to be a ‘classic drug for classic disorder’ (Gershon et al., 2009). Regardless of this fact, the use of lithium in the treatment of bipolar disorders has declined substantially over the past three decades (Baldessarini et al., 2007, 2008a; Blanco et al., 2002; Fieve, 1999; Gershon et al., 2009; Goodwin et al., 2003; Malhi and Berk, 2012; Young and Hammond, 2007). The current situation is well described by R Fieve (1999): ‘lithium, for a number of patients not receiving it, is a drug of choice’ (p. 70). Mark Twain said that ‘the classic is a book that everybody talks about, but nobody reads it’. To paraphrase, the classic drug would be the drug that everybody recommends, but nobody prescribes.
What is going on? And what is going wrong?
Over the past three decades, we have witnessed a substantial decline in the use of lithium in the treatment of bipolar disorders, while the use of ACs and AAPs has increased considerably. The rates of polypharmacy are also rising (Blanco et al., 2002; Hayes et al., 2011; Levine et al., 2000). Non-adherence is still an important issue (Baldessarini et al., 2008a; Sajatovic et al., 2007).
Although a large number of effective pharmacological treatments are currently available and described in numerous guidelines, bipolar disorders are to this day one of the leading causes of disability and long-term unemployment. Life expectancy of patients with bipolar disorders is shorter compared to the general population due to the high rates of medical comorbidities, attempted and completed suicide, and high rates of mortality related to other causes. Patients spend almost half of their life symptomatic and many of their needs are still unmet (Collins et al., 2011; Judd et al., 2002; Leboyer and Kupfer, 2010; Leverich et al., 2003; McIntyre, 2009).
The use of lithium is declining, the rates of polypharmacy are increasing
Blanco et al. (2002) analyzed the data regarding medications prescribed to patients with bipolar disorder during outpatients’ visits by psychiatrists in the National Ambulatory Care Survey over the periods 1992–1995 and 1996–1999. The results indicated that one-third of the patients were not prescribed any of the mood-stabilizing drugs. Roughly half of the patients received an AD, with over 20% of those patients receiving it without a mood stabilizer. The prescription of antipsychotic drugs was prevalent and increased from 22% to 29%. The rates of combination treatment were initially high and continued to rise to almost half of the sample by the end of the study. Over the study period, the use of lithium decreased by 40%, while the use of valproate rose by 240%.
Goodwin et al. (2003) demonstrated a significant change in prescribing patterns for patients with bipolar disorder during the period from 1994 to 2001. The ratio of initial prescriptions for lithium compared to valproate shifted from 6:1 at the beginning of the observation period to 1:2 by the end of the study.
Baldessarini et al. (2008b) investigated prescribing practices for patients with bipolar disorder in the United States over the period of 1 year. The results showed high rates of polypharmacy at the beginning and at the end of the study (1/3). In all, 70% of the patients received AD medication both at the beginning and at the end of the observation period. At the start of the treatment, less than one-third of the patients received mood-stabilizing drugs. Approximately one-fourth of them received AC, while lithium was prescribed to less than one in 10 patients. The patients who received lithium were more likely to stay in treatment, less likely to have add-ons or their medication changed, and less likely to receive AD, AAP, AC or hypnotic medication.
Hayes et al. (2011) examined prescribing practices for patients with bipolar disorders in primary care in Great Britain, from 1995 to 2009. They found that the percentage of patients treated for bipolar disorder almost doubled over time. The patients remained longer on medication and this increase was most noticeable among young women. Although the frequency of prescribing lithium did not change over time, the frequency of prescription of AAPs and valproate increased relative to lithium. The rates of lithium use as monotherapy decreased, and the rates of polypharmacy substantially increased. Patients receiving lithium and AAPs spend twice as much time on medication than those treated with ACs and AAPs. An alarming finding, according to the authors of the study, was that approximately one-third of women of childbearing age were treated with valproate before 2009.
A decline in lithium prescription was also documented in a recent population-based study examining changes in mood stabilizer prescription in Sweden between 2007 and 2013. The use of lithium decreased steadily over the study period in bipolar I and II patients of both sexes, while there was an increase in the use of lamotrigine and quetiapine (Karanti et al., 2016).
Similar changes in drug prescription in the treatment of bipolar disorders have been described in Denmark as well. A large, nationwide population-based study including over 3200 patients (Kessing et al., 2016) examined treatments prescribed for patients with bipolar disorders over the period 2000–2011. The authors demonstrated that major changes occurred in prescribing practices. Lithium went from being the first drug prescribed to being the last, while the prescribing of AAPs and ACs increased significantly: at the end of the study period, AAPs were the first class of drugs prescribed, followed by ACs. Moreover, combination therapy increased for all drug combinations, except for lithium combined with ADs.
Why is the use of lithium declining?
A variety of factors influencing drug prescription has been discussed and investigated (Jefferson, 2005). Among the factors that influence the provider’s choices of a drug are prior experience with the drug, knowledge and expertise in the illness and belief system. Regarding the choice of lithium, there are several factors that might negatively influence a physician but could, hopefully, be reverted.
In spite of extensive evidence confirming the efficacy of lithium, some authors have called this into question since the ‘lithium wars’ (Baastrup and Schou, 1968a, 1968b; Blackwell and Schou, 1970; Blackwell and Shepherd, 1968; for details see Shorter, 2009) until recently (Moncrieff, 1997). Many physicians are concerned about the side effects of lithium and believe that monitoring patients treated with lithium is complex and cumbersome (Malhi and Berk, 2012; Schou, 1989). Psychiatrists are exposed to various biases in study design and publication (i.e. lithium used as a comparator in enriched designs in favor of a sponsored drug, repeated publishing of positive trials of a new drug, non-publishing of negative studies) and aggressive marketing in favor of new compounds (Coryell, 2009). Finally, residents are not adequately educated about the efficacy of lithium and about monitoring patients using lithium (Gershon et al., 2009; Jefferson, 2005).
Why the use of lithium should not decline
Evidence suggesting that psychiatrists should continue to prescribe lithium is overwhelming and increasing (Young and Hammond, 2007).
Efficacy in the acute treatment
The antimanic efficacy of lithium was discovered serendipitously and described by John Cade (1949). Ever since, its efficacy has been restated in a number of studies employing various methodologies (Schou et al., 1954; Stokes et al., 1971 and others; for an overview, see Bauer and Mitchner, 2004 and Schou, 1999). The results of recently conducted meta-analyses strongly suggest the efficaciousness of lithium in the treatment of acute mania (Cipriani et al., 2011). However, since the effects of lithium in the treatment of acute mania may take 6–10 days, it is frequently administered along with an antipsychotic medication to provide a more rapid relief of symptoms such as agitation (Malhi et al., 2014).
The efficacy of lithium in the treatment of acute bipolar depression has been demonstrated in several studies (Baron et al., 1975; Goodwin et al., 1972; Mendels, 1976). Although its efficacy in treatment may be somewhat less robust than its antimanic effects, one should bear in mind that acute bipolar depression is a condition difficult to treat anyway (Gershon et al., 2009). Given that the AD effects of lithium can take up to 6 or 8 weeks to achieve remission, it is not considered to be the first choice as monotherapy in urgent cases (Malhi et al., 2014).
Efficacy in maintenance
The idea to prescribe lithium in order to sustain its beneficial therapeutic effect can be found in Cade’s (1949) original paper, in a case description: ‘he (the patient) left the hospital … with instructions to take a maintenance dose of lithium …’ (p. 350). Schou et al. (1954) recognized that with lithium, ‘many patients can be kept in a normal state by administration of a maintenance dose’ (p. 255). Subsequently, the efficacy of lithium in preventing not only manic but depressive episodes as well was documented and confirmed in randomized controlled studies and meta-analyses. Some of these studies deserve a short comment.
Lithium works in studies
In a study by Baastrup et al. (1970), 84 patients with manic-depressive illness and recurrent depression were treated with lithium versus placebo in a randomized double blind fashion. Over the period of 5 months, all 21 relapses were registered in the placebo group. Interestingly, four patients from the placebo group were excluded from the study, due to the fact that although they were receiving placebo, they had substantial levels of lithium in the serum and it was later revealed that they kept some of their former medication, or were obtaining lithium elsewhere (the paper represents an excellent example of quantitative research combined with qualitative research).
Coppen et al. (1971) introduced add-on treatment in the methodology: 65 patients were randomized to receive lithium or placebo for a period of 112 weeks; antimanic or AD agents or electroconvulsive therapy (ECT) were added when clinically indicated by blinded psychiatrists. All add-on treatments were significantly less frequent in the lithium group; ECT was administered to 43% of patients in the placebo group, while none of the patients taking lithium received ECT.
In the early meta-analysis (Geddes et al., 2004), lithium proved to be superior to placebo in the prevention of any mood episodes (p < 0.0001) and manic episodes (p = 0.008), while its effect on the prevention of depressive episodes was close to reaching statistical significance (p = 0.06). In a recent, updated meta-analysis (Severus et al., 2014), lithium was significantly superior to placebo in the prevention of any mood episodes, manic and depressive episodes. The results of network meta-analysis (Miura et al., 2014) examining 17 treatments from 33 randomized controlled trials (RCTs) revealed that in comparison to placebo, only lithium and quetiapine in monotherapy prevented any mood episodes, as well as manic and depressive episodes. It should be pointed out that while the data for lithium came from trials with non-enriched designs, quetiapine data came from the trials enriched for quetiapine (Nolen, 2015). The authors conclude that lithium seems to be the most reasonable candidate for a first-line treatment option for the long-term treatment of bipolar disorder (Miura et al., 2014).
Lithium works in the real world, too
In a study of unique methodology, resembling real-world conditions (Bipolar Affective Disorder: Lithium/ANtiConvulsant Evaluation [BALANCE] study Geddes et al., 2010), the efficacy of lithium, valproate and lithium/valproate combination were compared in the prevention of mood episodes over a period of 2 years. The results of the study demonstrated that lithium was superior to valproate in the prevention of any mood episodes (p = 0.0472). The advantage of lithium was most evident for depressive relapses (p = 0.0331).
The superiority of lithium versus valproate was recently also demonstrated in a large nationwide register population-based study, which included more than 4000 participants over the period from 1995 to 2006 (Kessing et al., 2011). Patients receiving lithium were significantly less likely to be hospitalized for a mood episode or to have their treatment modified (change or add-on) than those treated with valproate.
It has been pointed out that in naturalistic settings, the effectiveness of long-term lithium treatment is lower than in controlled studies and meta-analyses (Goldberg et al., 1995; Harrow et al., 1990; Keller et al., 1993) or that it diminishes over time (Maj et al., 1989). However, in a recent prospective naturalistic study observing the morbidity index of a total of 346 bipolar I or II patients over the period of 10 years, it was demonstrated that response to long-term maintenance treatment with lithium remains stable over time (Berghöfer et al., 2013).
Data confirming the efficacy of lithium in maintenance treatment of bipolar disorder continue to emerge. Hayes et al. (2016) demonstrated that lithium is superior to valproate, olanzapine and quetiapine as monotherapy in maintenance treatment of bipolar disorder. In this large population-based cohort study examining the rates of monotherapy treatment failure in real-world clinical practice, the duration of successful monotherapy (time to add-on of a mood-stabilizing or antipsychotic agent or stopping treatment) was shown to be significantly longer for lithium monotherapy than for other medications examined.
Efficacy in augmentation
Augmentation, that is, addition to AD therapy to increase its effectiveness in reducing the core symptoms of depression, is another well-known and commonly recommended indication for lithium. From among the numerous strategies for augmentation, adding lithium to an AD treatment is the strategy with a strongest research support (Valenstein et al., 2006). This effect of lithium was described in 1980s (De Montigny et al., 1981) and later confirmed in RCTs (Bauer et al., 2000) and meta-analysis (Crosley and Bauer, 2007). It has been demonstrated that lithium is as effective augmentation to second-generation ADs as it is for TCAs (Nelson et al., 2014). In a study examining the treatment of a large sample of depressed patients with different augmenting agents (a total of 244,859 patients), out of 22% of patients who received augmentation treatment, only 0.5% were prescribed lithium while the remaining patients received another AD or AAP (Valenstein et al., 2006).
Neuroprotective effects
The neuroprotective effects of lithium have been demonstrated in case-control studies and confirmed in population-based research. In a study conducted by Nunes et al. (2007) on a subgroup of patients with bipolar disorder chronically treated with lithium, the risk of dementia was no greater than in the general population, in contrast to the subgroup of patients who did not receive lithium (5% vs 33%, p < 0.001). Crucially, this reduced risk was not a consequence of the reduction of the number of mood episodes. In a nationwide population-based study (Kessing et al., 2008), more than one prescription of lithium was significantly related to the reduction of the risk of dementia (quite unlike the treatment with AC). Recent research has demonstrated that lithium influences mood, cognition and brain structure through several sophisticated and interrelated processes (Malhi et al., 2013). It may reduce cognitive decline in patients with bipolar disorder. On a macroscopic level, regarding brain structure, it appears to preserve or increase the volume of structures involved in emotional regulation (prefrontal cortex, amygdala and hippocampus). Lithium has been shown to act upon various neurotransmitter systems and second messenger cascades. It influences glycogen syntetase kinase 3β and inositol monophosphatase. On the intracellular and molecular level, it reduces excitatory neurotransmission (dopamine and glutamate) and enhances inhibitory neurotransmission (gamma-amino butyric acid [GABA]). Lithium reduces oxidative stress, which occurs during multiple episodes of mania and depression. It inhibits apoptosis through the inhibition of glycogen syntetase kinase 3β and increases the synthesis of protective proteins such as brain-derived neurotrophic factor and B-cell lymphoma 2 (Malhi et al., 2014).
Anti-suicidal effect
The anti-suicidal effect of lithium is another unique property of this medication. This effect has been demonstrated in observational studies and confirmed in randomized trials and meta-analyses. Based on an 11-year follow-up study, Coppen et al. (1991) indicated that lithium reduces excess mortality associated with recurrent mood disorders, including suicide mortality. In a meta-analysis, Tondo et al. (2001) found that suicide risk in lithium-treated patients was reduced by the factor of 8.85. The anti-suicidal effect has been more pronounced in lithium responders, but it is also present in patients in whom recurrence-related response to lithium was moderate or poor. This leads to the conclusion that the anti-suicidal effect extends beyond mood stabilization (Ahrens and Müller-Oerlinghausen, 2001). In a randomized placebo controlled trial of patients with a recent suicide attempt in the context of mood spectrum disorders, Lauterbach et al. (2008) concluded that lithium may be effective in reducing the risk of completed suicide. In a previous and updated meta-analysis by Cipriani et al. (2005, 2013), lithium was shown to be superior to placebo as well as to active comparators in reducing the rates of suicide and all-cause mortality in bipolar and non-bipolar depressed patients. In their more recent study (Cipriani et al., 2013), the anti-suicidal effect of lithium was greater than its effects on mood episodes, which might suggest that this effect is mediated through a reduction in impulsivity or aggression. Interestingly, trace amounts of lithium in drinking water have also been linked to the reduction of suicide and all-cause mortality rates (see below).
‘Nobody is perfect’
Lithium does have side effects, which have been described from the early lithium studies until now. However, some of the risks reported previously may have been overestimated. A recent meta-analysis (McKnight et al., 2012) demonstrated that lithium may reduce urinary concentrating ability, can cause hypothyroidism and hyperparathyroidism, induces weight gain, but the risk of end-stage renal failure is low. With respect to congenital abnormalities, the risk is uncertain. No risk of alopecia and other skin abnormalities has been demonstrated. In addition, weight gain associated with the lithium treatment appears to be less pronounced than the one associated with treatment with AAPs and ACs (Malhi et al., 2012a). Having in mind the risk/benefit ratio, during the pregnancy, if treatment is necessary, lithium may be a safer option in comparison to ACs and some AAPs (Khan et al., 2016). The risk of relapse in postpartum period is substantial in women with preexisting bipolar disorder (66% in medication-free patients [Wesseloo et al., 2016]). Lithium prophylaxis may significantly reduce the risk of postpartum episodes in women with bipolar disorder, as well as in women with previous episodes of postpartum psychosis (Bergink et al., 2012). Bergink et al. (2015) demonstrated that lithium monotherapy is more effective in sustaining remission following treatment of postpartum psychosis than antipsychotic monotherapy over the period of 9 months. They concluded that lithium maintenance may be most beneficial for relapse prevention in postpartum. Since the efficacy of other agents in the prevention of postpartum episodes has not been demonstrated (in fact, cf. negative results for valproic acid (Wisner et al., 2004) and estrogen (Kumar et al., 2003) and equivocal results for olanzapine (Sharma et al., 2006)). On the other hand, valproic acid has been shown to have teratogenic effects, which leaves lithium as the first choice prophylactic agent for women in their childbearing ages.
Monitoring patients on lithium, prior to its commencement and later on, with respect to renal function, thyroid function, calcium levels and cardiovascular status has been discussed in detail (Malhi et al., 2012b; Shine et al., 2015).
It is essential to keep lithium levels in an adequate range to ensure a long-term therapeutic effect (0.6–0.8mmol/L for maintenance, Malhi et al., 2014). The original recommendation to sustain lithium levels of at least 0.6 mmol/L (Schou and Baastrup, 1967) has been corroborated recently (Nolen and Weisler, 2013).
Having sad that lithium is not without side effects, it is worth mentioning that while choosing a medication for a presumably long-term treatment, a physician should compare the side effects demonstrated to be related to the use of lithium with the side effects of drugs commonly prescribed as an alternative (Table 1).
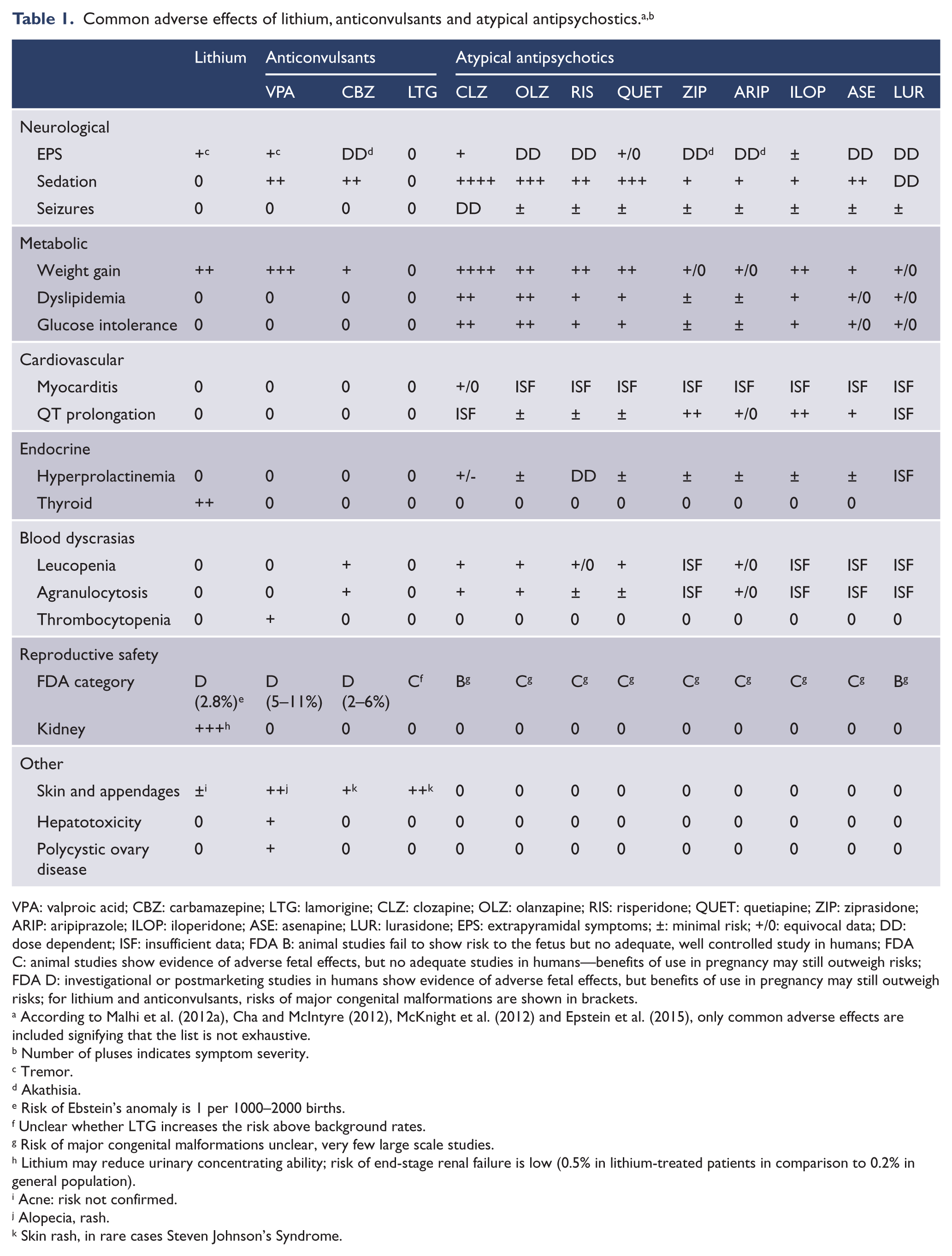
VPA: valproic acid; CBZ: carbamazepine; LTG: lamorigine; CLZ: clozapine; OLZ: olanzapine; RIS: risperidone; QUET: quetiapine; ZIP: ziprasidone; ARIP: aripiprazole; ILOP: iloperidone; ASE: asenapine; LUR: lurasidone; EPS: extrapyramidal symptoms; ±: minimal risk; +/0: equivocal data; DD: dose dependent; ISF: insufficient data; FDA B: animal studies fail to show risk to the fetus but no adequate, well controlled study in humans; FDA C: animal studies show evidence of adverse fetal effects, but no adequate studies in humans—benefits of use in pregnancy may still outweigh risks; FDA D: investigational or postmarketing studies in humans show evidence of adverse fetal effects, but benefits of use in pregnancy may still outweigh risks; for lithium and anticonvulsants, risks of major congenital malformations are shown in brackets.
According to Malhi et al. (2012a), Cha and McIntyre (2012), McKnight et al. (2012) and Epstein et al. (2015), only common adverse effects are included signifying that the list is not exhaustive.
Number of pluses indicates symptom severity.
Tremor.
Akathisia.
Risk of Ebstein’s anomaly is 1 per 1000–2000 births.
Unclear whether LTG increases the risk above background rates.
Risk of major congenital malformations unclear, very few large scale studies.
Lithium may reduce urinary concentrating ability; risk of end-stage renal failure is low (0.5% in lithium-treated patients in comparison to 0.2% in general population).
Acne: risk not confirmed.
Alopecia, rash.
Skin rash, in rare cases Steven Johnson’s Syndrome.
What can we do?
Reminding psychiatrists and teaching residents about the effectiveness of lithium, about its side effects and adequate monitoring is crucial (Gershon et al., 2009; Jefferson, 2005).
Treating a patient with excellent, sustained response to lithium prophylaxis is one of the most gratifying experiences for a psychiatrist (Grof et al., 2009). The identification of excellent lithium responders might be facilitated by the presence/absence of typical and atypical features (Table 2). It has been demonstrated that the number of atypical features is related to a larger number of affective episodes during the follow-up, signifying that patients with atypical features should be monitored more carefully, since they may require additional mood-stabilizing agents (Pfennig et al., 2010).
International Group for the Study of Lithium-Treated Patients (IGSLi) typical and atypical features of affective illness (Berghöfer et al., 2008).
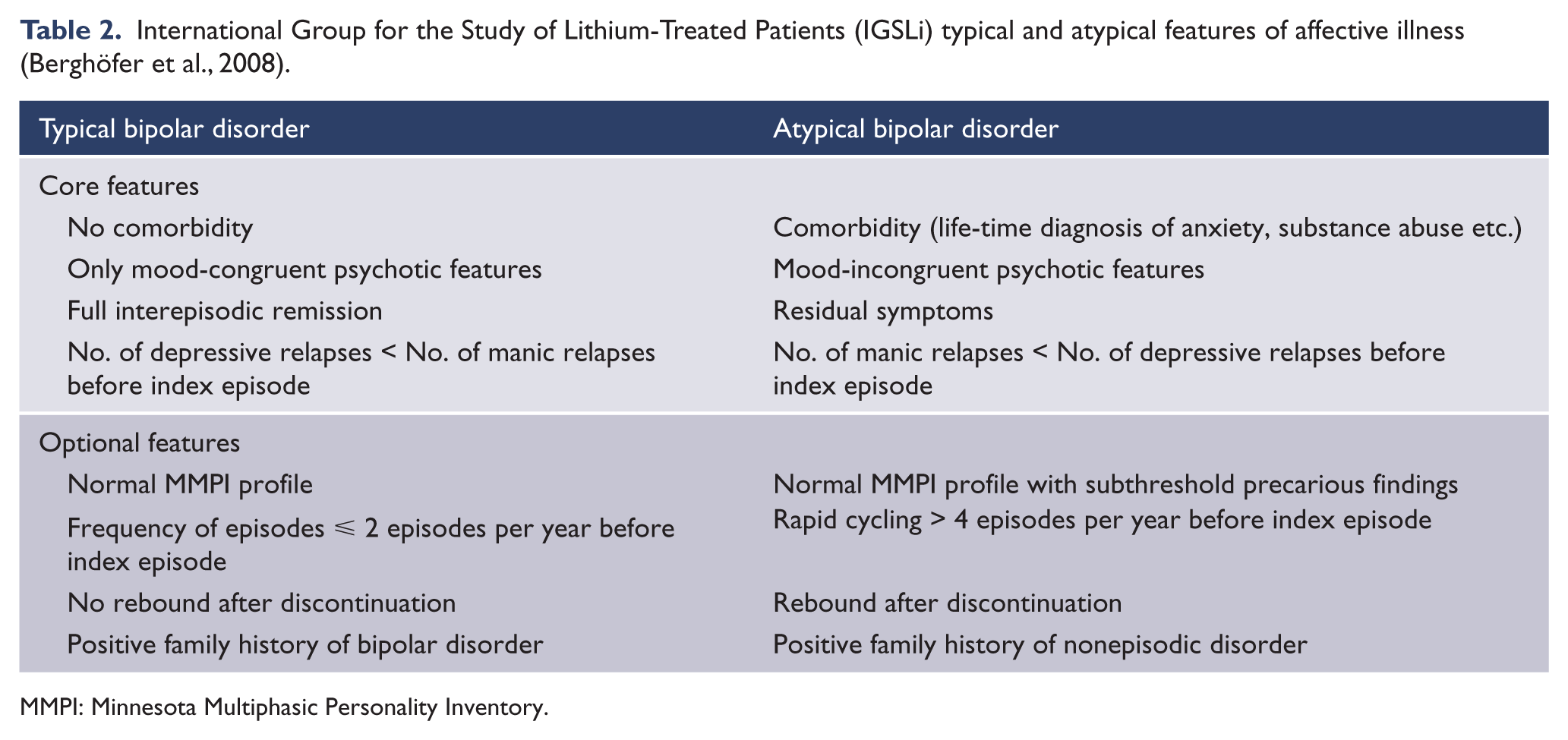
MMPI: Minnesota Multiphasic Personality Inventory.
Nevertheless, in a recent study by Kessing et al. (2014), early lithium treatment (following the first episode or first psychiatric contact) was demonstrated to significantly reduce the rate of lithium non-response. Therefore, if at all possible, giving lithium (and the patient) a chance early in the course of the disorder might be a prudent strategy, which might not only reduce the probability of treatment non-response, but provide the patient with an opportunity to benefit from anti-suicidal as well as neuroprotective properties of lithium.
What do the patients want?
The Understanding Needs, Interactions, Treatment, and Expectations Among individuals affected by bipolar disorder or schizophrenia (UNITE) study investigated the unmet needs of patients with bipolar disorders (McIntyre, 2009). Over 1300 patients from different countries, treated for bipolar disorder on an average of 8 years, received treatment with lithium (31%), AAPs (34%) and mood-stabilizing drugs other than lithium (45%). When asked about their satisfaction with the treatment, the participants reported that they would like to have a drug that is associated with a better treatment of depression, less weight gain, improved quality of life, better prevention of depression, lower risk of sleeping difficulties and of suicidal thoughts, diabetes, sedation and muscle stiffness.
Even hampered with its own limitations, lithium without a doubt represents a compound that may be able to satisfy the yet unmet needs of a considerable number of patients with bipolar disorders.
Fun facts for the end
Lithium is the lightest and oldest metal in the universe, probably present since the Big Bang. It floats on water. Trace amounts of it are found in the human body, but its physiological effects have not been sufficiently studied. It may be involved in a variety of physiological processes (Malhi et al., 2013).
The beneficial effects of waters rich in lithium for patients with mental disorders were described in Ancient times (Greece). In psychiatry, it was first used by Hammond in 1871 in the treatment of a patient with mania and by Carl and Frederick Lange in 1894 for the treatment of patients with recurrent depression (Shorter, 2009). Spas with waters rich in lithium were recommended as a remedy for various conditions, among others for mental depression, nervous irritability and as ‘nature’s antidote for liquor and opium habit’ (Buffalo Lithia waters were advertised to alleviate those conditions, even though it would be literally impossible to consume sufficient quantities of water to achieve therapeutic lithium levels). In the early 20th century, different beverages contained trace amounts of lithium—Lithia Beer, as well as popular 7 Up, advertised as a ‘hangover remedy’ and a drink that can help one to ‘keep smiling’. Until 1949, lithium was used as a salt replacement for cardiological patients but was withdrawn in the United States due to toxicity the same year Cade’s seminal paper was published. Over the following decades, the psychiatric effects of lithium were extensively investigated, and the contribution of Morgens Schou can only be portrayed as outstanding.
Since the 1970s, another line of lithium-related research began to emerge. Several studies found a relationship between trace amounts of lithium in the drinking water and decreased rates of suicide, homicide and drug-related arrests (Dawson et al., 1972). Early studies have been replicated recently in different parts of the world (Kapusta et al., 2011), some of them establishing an association of levels of lithium in drinking water with reduced mortality of any cause (Zarse et al., 2011). Moreover, preclinical research points to another interesting property of lithium: it reverses insulin resistance in muscle cells (of diabetic rats) to normal, similar to the effects of continued exercise (Tabata et al., 1994). So should we add lithium to tap water? The jury is still out on that. One thing is certain—the lithium story is far from over.
Ask not what lithium can do for you—ask what you can do for lithium!
Lithium can do a lot for patients with mood disorders. It has already done a lot for psychiatry: in the era of antipsychiatric movements, it has brought psychiatry back to medicine; it promotes the interest of psychiatrists in nosology, bringing us back to Kreapelin’s synthesis (being effective not only for patients with mania but also those with recurrent depressive episodes); it encourages research of the biological mechanisms of mental disorders; finally, it has started a psychopharmacological revolution, influencing strongly the development of research methodology (Goodwin and Ghaemi, 1999).
Having in mind the exceptional properties of this magic ion, a question comes to mind: Will lithium once more become the gold standard, the treatment of choice and the real first-line drug in the treatment of bipolar disorders (Nolen, 2015)?
It’s up to us.
Footnotes
Acknowledgements
I would like to thank my first tutor, Professor Edwin Till, who taught me how to prescribe lithium, and my patients, from whom I learn every day. I would also like to express my gratitude to the International Review of Psychosis & Bipolarity for the opportunity to discuss this topic. This work was, in part, presented by the author at the International Review of Psychosis & Bipolarity Conference in Rome, in May 2016.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.