
Abstract
Objective:
Mood instability is common in the general population. Mood instability is a precursor to mental illness and associated with a range of negative health outcomes. Sleep disturbance appears to be closely linked with mood instability. This study assesses the association between mood instability and sleep disturbance and the link with suicidal ideation and behaviour in a general population sample in England.
Method:
The Adult Psychiatric Morbidity Survey, 2007 collected detailed information about mental health symptoms and correlates in a representative sample of adult household residents living in England (n = 7303). Mood instability was assessed using the Structured Clinical Interview for DSM-IV Axis-II. Sleep problems were defined as sleeping more than usual or less than usual during the past month. Other dependent variables included medication use and suicidal ideation and behaviour (response rate 57%). Generalized linear modelling was used to estimate the prevalence of mood instability and sleep problems. Logistic regression was used to estimate odds ratios. All estimates were weighted.
Results:
The prevalence of mood instability was 14.7% (95% confidence interval [13.6%, 15.7%]). Sleep problems occurred in 69.8% (95% confidence interval: [66.6%, 73.1%]) of those with mood instability versus 37.6% (95% confidence interval: [36.2%, 39.1%]) of those without mood instability. The use of sedating and non-sedating medications did not influence the association. Sleep problems were significantly associated with suicidal ideation and behaviour even after adjusting for mood instability.
Conclusion:
Sleep problems are highly prevalent in the general population, particularly among those with mood instability. Sleep problems are strongly associated with suicidal ideation and behaviour. Treatments that target risk and maintenance factors that transcend diagnostic boundaries, such as therapies that target sleep disturbance, may be particularly valuable for preventing and addressing complications related to mood instability such as suicide.
Introduction
Mood instability (MI) is a poorly understood, but common, mental health problem in the general population (Marwaha et al., 2013b). MI is a risk factor for suicidal behaviour in the general population (Marwaha et al., 2013a). It has been linked with a number of psychiatric conditions such as mood, personality and anxiety disorders (Marwaha et al., 2014; Patel et al., 2015). Although commonly a symptom of psychiatric disorders, it can occur independent of and may be a precursor to mental illness. Given the significance of MI in psychopathology, it is important to understand its nature and correlates
Sleep may play a key role in affective regulation. Mood changes are often preceded by and co-occurring with sleep disturbance (Bauer et al., 2008) and poor sleep may contribute to or worsen MI (Bowen et al., 2013). In bipolar disorder, sleep disturbance has been identified as the most robust prodrome of mania (Jackson et al., 2003) and has been associated with more severe course of illness including recurrence of major mood episodes, history of psychosis and number of suicide attempts (Sylvia et al., 2012). In unipolar depression, sleep appears to be a mediator of the association between MI and depression (Marwaha et al., 2015). It is unclear to what extent this association is limited to diagnosed psychiatric disorder or whether it is a more pervasive pattern observed in the population more generally.
A major advantage of population surveys is that they are capable of capturing a representative sample of the population. Clinical investigations and administrative data represent only individuals who have been in contact with health services and therefore miss a large portion of the population. Studying MI in this type of survey allows a unique opportunity to examine individuals who may have subsyndromal mood symptoms or who are at risk of future clinical illness, and to identify potential transdiagnostic processes.
The aim of this study was to examine the association between sleep problems and MI and the link with suicidal ideation and behaviour in a general population sample. We hypothesized that (a) sleep problems are positively associated with MI, (b) individuals with MI who are using psychotropic medications are less likely to have sleep problems than individuals with MI not taking psychotropic medication and (c) sleep problems are positively associated with suicidal behaviour, particularly in those with MI. To our knowledge, this is the first study to examine MI and sleep disturbance in a general population sample.
Method
Adult Psychiatric Morbidity Survey, 2007
Data were from Phase 1 of the Adult Psychiatric Morbidity Survey, 2007 (APMS 2007), a cross-sectional survey of sociodemographic features, mental health and morbidity and correlates in adults aged 16 and older living in private households in England. Data were collected via multi-stage stratified random sampling between October 2006 and December 2007. Interviews were completed in person by trained lay interviewers. Details of the survey have been published elsewhere (Bebbington et al., 2009; National Centre for Social Research, 2011). The overall response rate for Phase 1 of the survey was 57%, for a final sample size of 7403 respondents. Data are available from the UK Data Archive; further information is available online (www.hscic.gov.uk/pubs/psychiatricmorbidity07). The Royal Free Hospital and Medical School Research Ethics Committee provided ethical approval for APMS 2007.
Measures
MI was measured using a single item from the borderline module of the Structured Clinical Interview for DSM-IV Axis-II (SCID-II): ‘Do you often have a lot of sudden mood changes?’ (First et al., 1997). This item was answered by all respondents.
Self-reported sleep problems included (a) sleeping less than usual, ‘In the past month, have you been having problems with trying to get to sleep or with getting back to sleep if you woke up or were woken up’? and (b) sleeping more than usual, ‘Has sleeping more than you usually been a problem for you in the past month’? For the purpose of this study, any sleep problem includes all respondents who experienced sleeping more than usual or sleeping less than usual.
Income represents equivalized annual household income (total household income divided by a score computed based on the number, age and relationships of household members). Body mass index (BMI) was calculated from self-reported height and weight of the respondent. Prescribed medications were self-reported and verified by the interviewer by examining the medication packages, and included commonly prescribed medications (antipsychotics, antidepressants, sedative-hypnotics and lithium) for psychiatric symptoms. We then grouped medications by those with high risk of sedation (sedating) and medications with low risk of sedating effects (non-sedating). The Alcohol Use Disorders Identification Test (AUDIT) is a 10-item screening test designed to assess patterns of alcohol consumption. Higher scores indicate more hazardous drinking patterns (Saunders et al., 1993). Alcohol and substance dependence were measured using questions based on the diagnostic interview schedule (DIS; Compton and Cottler, 2004).
Statistical analysis
Demographic features were described as frequencies and proportions with 95% confidence intervals. Prevalence of MI and sleep problems were estimated using generalized linear modelling of the binomial family with a log link function. To examine whether having any sleep problem was associated with MI independently or whether it was influenced by psychiatric disorder, we calculated the odds ratio (OR) of any sleep problem in those with MI and psychiatric condition, with MI and no psychiatric condition, and psychiatric condition without MI against the reference group without MI or a psychiatric condition. Using the same reference group allows direct comparison of the relative influence of MI and psychiatric diagnosis on the association with sleep problems. We also explored the influence of taking psychotropic medications on the association between sleep problems and MI. We compared models including any medication, sedating medications, and non-sedating medications to crude models. Finally, we explored the association between sleep problems and suicide in those with and without any sleep problem. ORs were calculated using logistic regression. Analyses were assessed for age and sex interactions and confounding, including the possible influence of quadratic age trends. Potential modifiers of the association were determined using Wald tests. The presence of a potential confounder was assessed by comparing the adjusted and crude estimates; if the two estimates were meaningfully different, the variable was considered a confounder. All statistical tests used a 5% significance level.
Since a multi-phase stratified sampling design was used, all analyses were weighted using the svy commands (using Taylor linearized variance and scaled variance for singleton strata) in order to produce corrected variance estimates and results that are more representative of the target population. Analyses were carried out in Stata version 11 (StataCorp, 2009).
Results
The weighted sample size was 7393. All sample sizes and statistics presented in this paper are weighted and sample sizes are rounded to the nearest whole number. Proportions of missing data for each major subgroup (MI, professionally diagnosed psychiatric condition, any sleep problem) were less than 1%.
Demographic features and selected covariates of sleep problems in the subsamples are shown in Table 1. Those who were female, single, employed part-time and those with a lower income more frequently reported MI. MI was also very common among those with alcohol or substance use problems.
Frequencies and percents of those with mood instability (n = 1073) and sleep problems (n = 3299) reporting levels of selected demographic features and possible covariates.
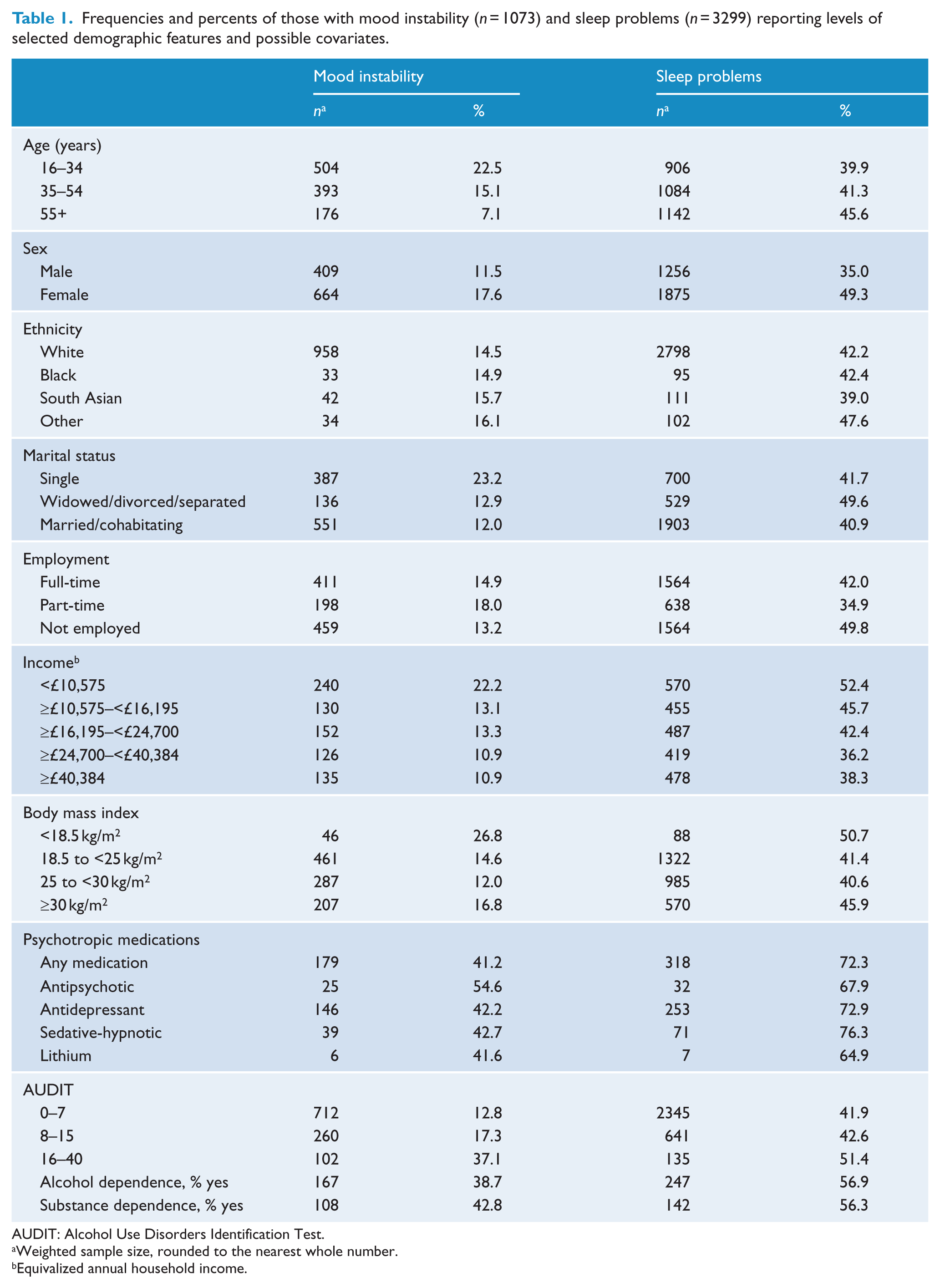
AUDIT: Alcohol Use Disorders Identification Test.
Weighted sample size, rounded to the nearest whole number.
Equivalized annual household income.
The estimated lifetime prevalence of MI was 14.7% (95% confidence interval [CI]: [13.6%, 15.7%]). Estimated prevalence was significantly higher in females (17.6%, 95% CI: [16.1%, 19.1%]) compared with males (11.5%, 95% CI: [10.1%, 12.9%]) and decreased approximately linearly with age (by about 1% prevalence per year of age) for both sexes.
Among those with MI, approximately 69.8% (95% CI: [66.6%, 73.2%]) reported sleeping more or sleeping less than usual, considerably higher than 37.6% (95% CI: [36.2%, 39.1%]) of those without MI.
The estimated odds of having any sleep problem in those with MI versus those without MI depended on gender. In males, the association between having a sleep problem and MI was modified by quadratic age. After accounting for quadratic age, there was no significant association between sleep problems and MI in males. Neither quadratic age nor linear age terms modified or confounded the relationship among females. In females, the odds of having a sleep problem were significantly higher in those with MI than in those without MI (OR = 2.8, 95% CI: [2.3, 3.6]).
Compared with the reference group (having no diagnosed psychiatric condition or MI), the OR of any sleep problem for those with both MI and a diagnosis was highest, followed by MI without a diagnosis, than a diagnosis without MI (Table 2). Similar trends were observed for both genders; however, the strength of relationship in males appeared stronger at all levels. OR did not depend on age for these subgroups.
Estimated odds ratios (ORs) of having a sleep problem comparing three mood instability (MI) and professionally diagnosed psychiatric condition groups.
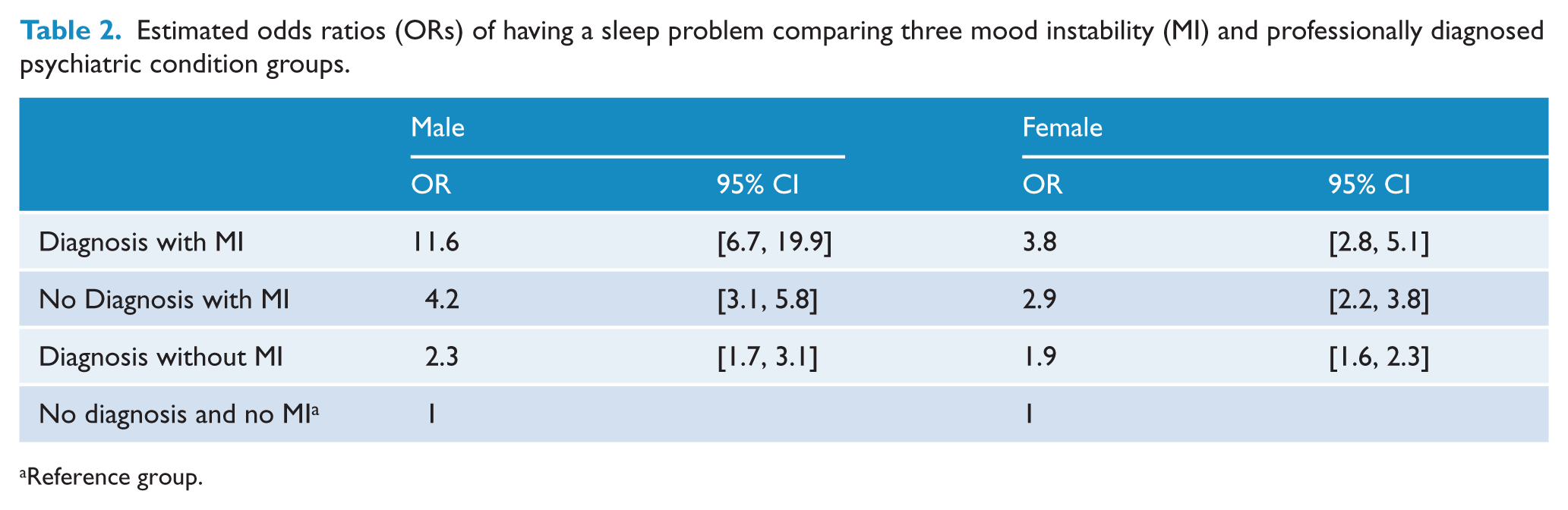
Reference group.
Sleeping less than usual and sleeping more than usual were significantly associated with MI. The association between sleeping less than usual and MI was stronger in males (OR = 4.2, 95% CI: [3.2, 5.4]) than females (OR = 2.6, 95% CI: [2.1, 3.2]). The OR of sleeping more than usual was similar for both males and females (OR = 4.5, 95% CI: [3.1, 6.6]). Age did not influence the estimate of association for either sleeping more or sleeping less than usual.
No significant associations between sleep problems and medication were observed.
The prevalence of suicide ideation in the total sample was 0.81% (95% CI: [0.6%, 1.0%]) during the past week, 4.3% (95% CI: [3.7%, 4.9%]) during the past year and 13.7% (95% CI: [12.8%, 14.7%]) during the lifetime. The prevalence of suicide attempt was 0.7% (95% CI: [0.4%, 0.9%]) during the past year, and 4.8% (95% CI: [4.2%, 5.4%]) during the lifetime (there was only n = 1 suicide attempt during the past week).
Estimates of the association between any sleep problem and suicidal ideation or behaviour are presented in Table 3. MI, age and sex were assessed to determine whether their inclusion in the model significantly changed the estimate of association using a combination of forward and backward selection. The relationship between sleep and suicidal ideation or behaviour did not appear to be influenced by age or sex and was not modified by the presence of MI. However, adjusting for mood did appear to diminish the strength of the association. Estimates for past week suicide attempt were unavailable owing to insufficient sample size.
Estimated odds ratios (ORs) of suicide ideation or attempt among individuals with any sleep problem versus no sleep problem.
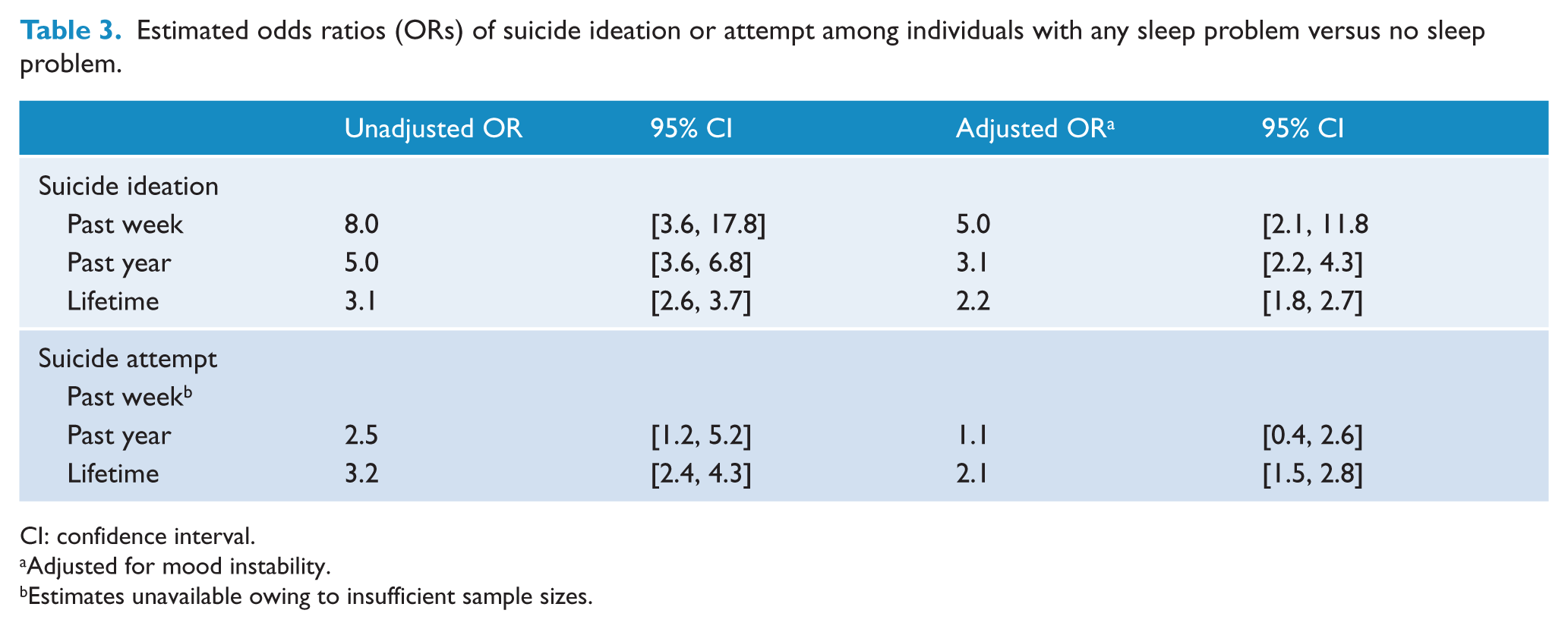
CI: confidence interval.
Adjusted for mood instability.
Estimates unavailable owing to insufficient sample sizes.
Discussion
The lifetime prevalence of MI in this study was approximately 14.7%. A previous study using the same data (Marwaha et al., 2014) observed a prevalence of 13.9%. This discrepancy is the result of differing methods of analysis; the prevalence estimate from the present study has been weighted, while the estimate made previously was unweighted. Weights are applied in order to account for non-response and to produce results that are more representative of the target population. Owing to the complex survey design, individuals have unequal selection probabilities and weights are applied to address potential resulting bias. Given that our analyses included weights, it is likely that our estimate is more representative of the true population prevalence of MI.
We observed that MI was significantly and positively associated with having sleep problems among females, but not males. This is an important finding because sleep problems have been associated with a range of negative health consequences including decreased quality of life (Ohayon et al., 2013), cardiovascular outcomes (Cappuccio et al., 2011), inflammation (Motivala and Irwin, 2007), diabetes (Gottlieb et al., 2005) and early mortality (Ferrie et al., 2007).
Importantly, we observed that the association with having a sleep problem appeared to be strongest when MI was present, especially if also diagnosed with a psychiatric condition. This may suggest that sleep disturbance is more strongly associated with the presence of MI than a psychiatric condition. However, these findings are limited owing to the cross-sectional data and because the measure of psychiatric condition includes all individuals who have ever been diagnosed with a mental illness and may not have symptoms of the condition at present.
Finally, we observed that having any sleep problem was significantly and positively association with suicidal ideation and attempt for all measured time periods. This finding is consistent with prior research, which shows evidence that sleep problems such as insomnia, nightmares, and other sleep disorders increase the risk of suicidal ideation and behaviour (Bernert et al., 2015; Pigeon et al., 2012). Adjusting for MI diminished the strength of association, particularly for past week and past year suicidal ideation; the unadjusted odds of suicidal ideation during the past week were approximately eight-fold higher in those with sleep problems versus those without, and still nearly five-fold after adjusting for MI.
Identifying modifiable risk factors associated with the development and maintenance of multiple different pathologies is relevant for guiding clinical interventions and preventing and diminishing morbidity and mortality. Sleep disturbance may be a modifiable and transdiagnostic risk factor for psychiatric morbidity (Harvey, 2008; Harvey et al., 2011). Individuals reporting MI may be showing prodromal or subsyndromal symptoms. Effectively treating early symptoms of illness is critical for prevention or improving disease course. Preliminary evidence shows that maintaining sleep reduces MI (Bowen et al., 2013). Therapies that address transdiagnostic factors such as sleep therapies may be effective, particularly given that psychiatric illnesses are often complex, multifactorial and commonly comorbid. Although these cross-sectional data cannot reveal causality, the results also suggest that addressing current sleep problems may be particularly valuable for ameliorating immediate suicidal thoughts or behaviours. Future research should aim to investigate the link between MI and development of psychiatric disorders and the potential role of sleep-related therapies.
Limitations
We recognize a few limitations to this study. First, the measure of MI in the survey relies on a single, subjective question about the frequency of mood changes. While there is no clear and consistently used definition of MI, existing definitions typically involve aspects of lability, intensity and proportionality to social situations in addition to frequency of mood changes (Marwaha et al., 2014). The question in this survey only involves one of several aspects of MI, and it is based on the SCID-II, which is founded in the Diagnostic and Statistical Manual of Mental Disorders–Fourth Edition (DSM-IV) (American Psychiatric Association, 2000) diagnosis of borderline personality disorder. Although the question has been thoroughly validated in borderline personality disorder, the phenomenological meaning of a positive answer is less clear in other groups. Additionally, the cross-sectional nature of the study provides no indication of temporality of the association. Both MI and sleep problems were self-report and not assessed prospectively. Sleep problems may represent a symptom of MI, but poor sleep quality appears to also produce or exacerbate MI (Bowen et al., 2013). In bipolar disorder, the association appears to be bidirectional (Talbot et al., 2012). While the results of this study represent a cautious estimate of MI, it is useful for generating future hypotheses and guiding possibly meaningful future research avenues.
Finally, the role of medication in the relation between sleep and MI warrants more systematic investigation. In this study, accounting for the use of sedating and non-sedating medication in the analysis did not appear to alter the estimate of association. However, many psychotropic medications such as antidepressants and antipsychotics have sometimes profound effects on sleep (e.g. Winokur et al., 2001, for review). It is possible that our classifications of medications were too broad, thereby limiting the ability to disentangle the association. We were unable to narrow the classes owing to insufficient power. Narrowing the classes to include only medications with more specific sleep effects may improve control. Additionally, many other medicines commonly prescribed to treat psychiatric symptoms such as antiepileptics were not assessed in this survey. It is likely that the influence of medication on the association between sleep disturbance and MI is underestimated in our findings.
Conclusion
Sleep problems are very common in the general population and in those with MI. Suicidal ideation and behaviour are higher in those with current sleep problems, even in the absence of MI. Given the apparently strong association between MI and sleep problems in the community, future work should examine this association more rigorously. Improved measures of MI including high frequency prospective mood monitoring (e.g. True Colours; www.truecolours.nhs.uk) have been developed. Future studies using objective, prospective designs may be worthwhile in elucidating the temporality between MI and sleep changes. Future research should also aim to systematically examine smaller classes of psychotropic medications in order to elucidate the effect of psychotropic medications. Finally, sleep problems are a potentially salient therapeutic target for reducing morbidity and mortality in the general population, particularly for those with MI. Treatments that target risk and maintenance factors that transcend diagnostic boundaries, such as therapies that target sleep disturbance, may be particularly valuable for preventing and addressing complications related to MI, such as suicide.
Footnotes
Acknowledgements
We acknowledge the UK Data Archive and the National Centre for Social Research for the data collection and sharing of the Adult Psychiatric Morbidity Survey, 2007.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Miss McDonald has no funding source to declare. Dr Saunders is supported by a Wellcome Trust Strategic Award (CONBRIO: Collaborative Network for Bipolar Research to Improve Outcomes).