
Abstract
Prospective studies have shown that in clinical populations, 5.4% died by suicide [1], and the excess mortality by suicide in mentally ill persons was estimated at 5–9.8-fold the number expected in the general population. Many studies have considered characteristics associated with suicide among psychiatric patients. A review by Appleby found that the following characteristics were common among patients who suicide: particular diagnoses (depression and psychosis), social circumstances (isolation, unemployment) and demographic characteristics (male sex, young age) [2]. The Wessex case–control study of 234 recently discharged psychiatric patients who committed suicide found the following risk factors: living alone, suicidal ideation precipitating admission, hopelessness, relationship difficulties, loss of job, inpatient deliberate self-harm (DSH), unplanned discharge and discontinuity of care from a significant professional [3]. The findings among the various studies, however, were inconsistent. Other studies showed that suicide subjects and controls could not be distinguished on the majority of patient- or treatment-based characteristics [4], [5].
It should be noted that the aforementioned studies are Western, and generalizability to Asian populations is still not well explored. Few studies have been conducted in Asian populations, especially Singapore. A total of 82.2% of published cases studying specifically the psychiatric diagnosis of people who died by suicide came from Europe (especially the UK and Scandinavian countries) and North America, and only 1.3% originated from Asian countries such as India and Taiwan [6]. This constitutes a strong bias towards European countries and hence any recommendation derived from these data to an Asian country may not be valid.
One Hong Kong study investigated suicide in Chinese patients after discharge from inpatient psychiatric treatment, and showed that suicide was associated with unemployment, past suicide attempts, maternal mental illness, suicidal ideation or attempt before the last admission [7]. The authors concluded that these Chinese psychiatric patients share some common risk factors for suicide identified in Western studies but there were several differences: predominance of schizophrenia in the suicide subjects; lower prevalence of substance abuse and comorbidity; low proportion of people living alone; increased clinical contact before death but less expression of suicidal intent, in these Chinese patients. A psychological autopsy study investigating Chinese suicide subjects in East Taiwan showed that risk factors for suicide include loss events, suicidal behaviour in first-degree relatives, ICD-10 major depressive episodes, emotionally unstable personality disorder and substance dependence [8]. The present study used a matched case–control design to test the hypothesis that there are clinical and treatment-based characteristics that can predict risk of suicide in psychiatric patients in Singapore.
Method
Study design
A matched case–control study design was used to estimate the strength of association between risk of suicide among psychiatric patients and various patient-specific (e.g. sociodemographic and clinical characteristics) and treatment-specific variables (e.g. continuity and duration of care, side-effects from treatment etc.). To ascertain if certain risk factors (such as unemployment) were characteristic of suicide subjects and not merely a characteristic of patients with mental illness, controls were used. In addition, matching for age, sex, principal diagnosis and calendar time of treatment was done.
Setting
All subjects in the present study were selected from the Institute of Mental Health (IMH), Singapore. IMH is a 2425-bed acute tertiary psychiatric hospital with satellite clinics in various parts of Singapore that serves the entire country (population 4 million). It receives referrals from the primary care physicians, general hospitals, and self-referrals, as well as inpatient treatment under the Mental Disorders and Treatment Act.
Selection of suicide subjects and controls
With permission of the Coroner, all the death reports with verdict of suicide from year 2003 to 2004 were obtained, and matched with the computerized register of IMH. Hence 138 cases of ex-IMH patients who killed themselves during 2003–2004 were obtained. Unfortunately we were unable to locate the medical records of 15 of the patients, and the medical records of only 123 suicide subjects were available,
For each suicide subject, one surviving control subject was identified with the same sex, age, principal diagnosis (DSM-IV), and calendar time of treatment. Matching for time of treatment was as follows: the control must have received outpatient or inpatient consultation in IMH 6 months before the index date (i.e. suicide date of the corresponding case.) This was done to ensure that both suicide subjects and controls received treatment around the 2002–2004 period, because over time the hospital may have changed in terms of treatment options, policies etc. All control subjects must not have died by suicide by the index date, and this was ascertained in two ways: first by checking the medical records if there were further consultations after the index date; and second, by checking with the Coroner if the control subject had received a verdict of suicide up to the index date.
Data collection
Information was collected from (i) inpatient psychiatric records at IMH; (ii) outpatient psychiatric records at IMH and the satellite clinics; and (iii) ancillary records from the medical social worker, clinical psychologists and community psychiatric nurses. Information on each control was collected up to the index date. Data were divided into three groups: sociodemographic, clinical and treatment-based variables (Table 1).
Data collection
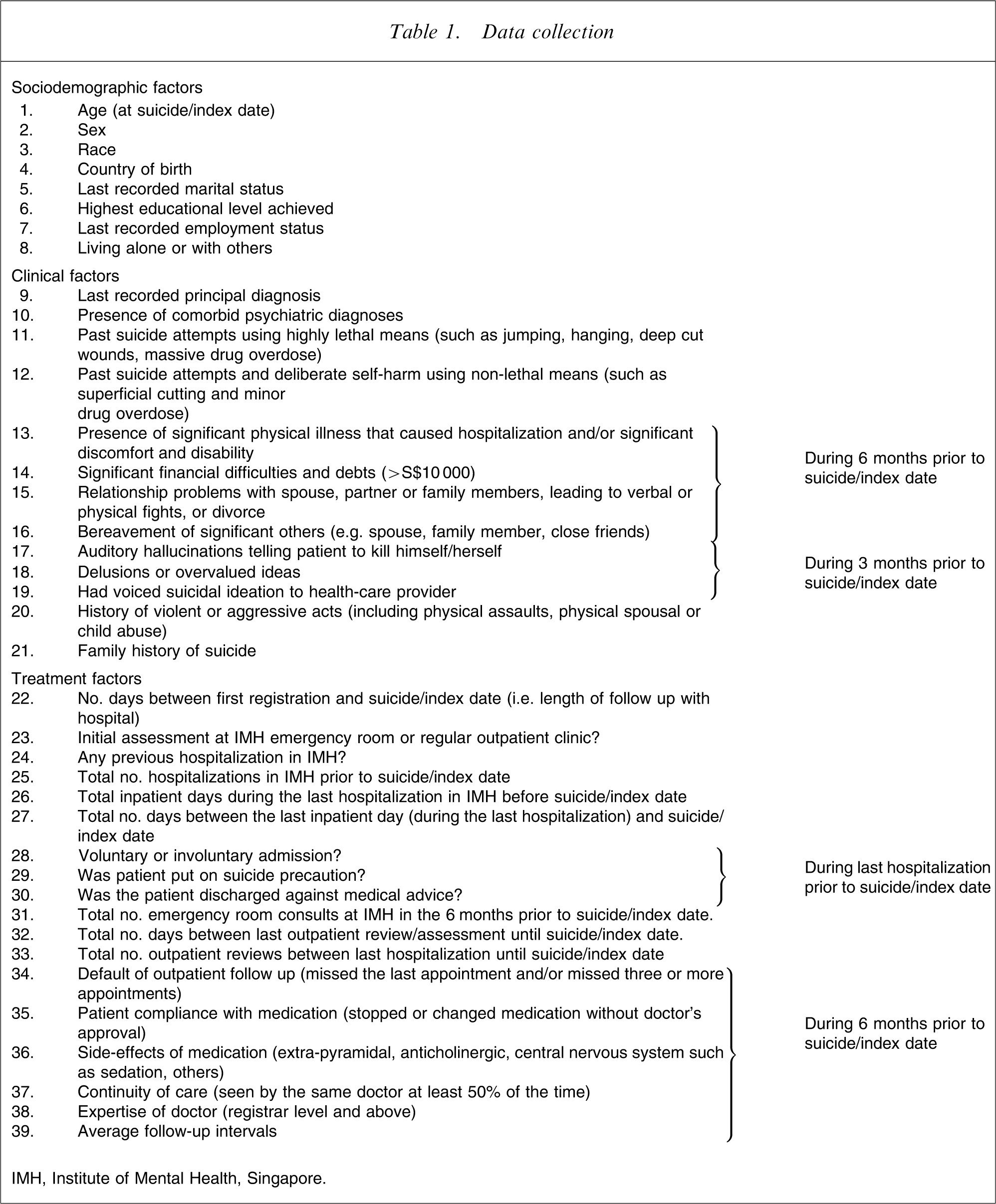
IMH, Institute of Mental Health, Singapore.
Statistical analysis
All analyses were performed using SPSS 14.0 (SPSS, Chicago, IL, USA). Descriptive statistics for quantitative variables will be presented as mean±SD and qualitative variables as n (%). The predictors for suicide were determined using conditional logistic regression taking into account the matching by sex, age, principal diagnosis, and time of treatment. Suicide subjects and controls were compared in a pairwise fashion using McNemar's test for dichotomous variables and Wilcoxon signed-rank test for continuous variables. When comparison was made between factors among the suicide subjects, χ2 test was used for categorical variables and Mann–Whitney U-test for continuous variables. Due to the multi-colinearity of the independent variables, a stepwise conditional logistic regression was performed to determine the most significant predictors, and the relative risks (RRs) and 95% confidence intervals were determined. Statistical significance was set at p < 0.05. Subgroup analyses were done to investigate differences between subjects who suicided within 30 days of discharge and those who suicided after that.
Results
Sociodemographics
Table 2 shows the relative risks of sociodemographic variables found to influence suicide in psychiatric patients. The male: female ratio was 1.2:1. The mean age at suicide was 43 years. 75% of suicide subjects were ≤52 years of age. Being divorced resulted in an increase in suicide risk.
Sociodemographic factors (conditional logistic regression)
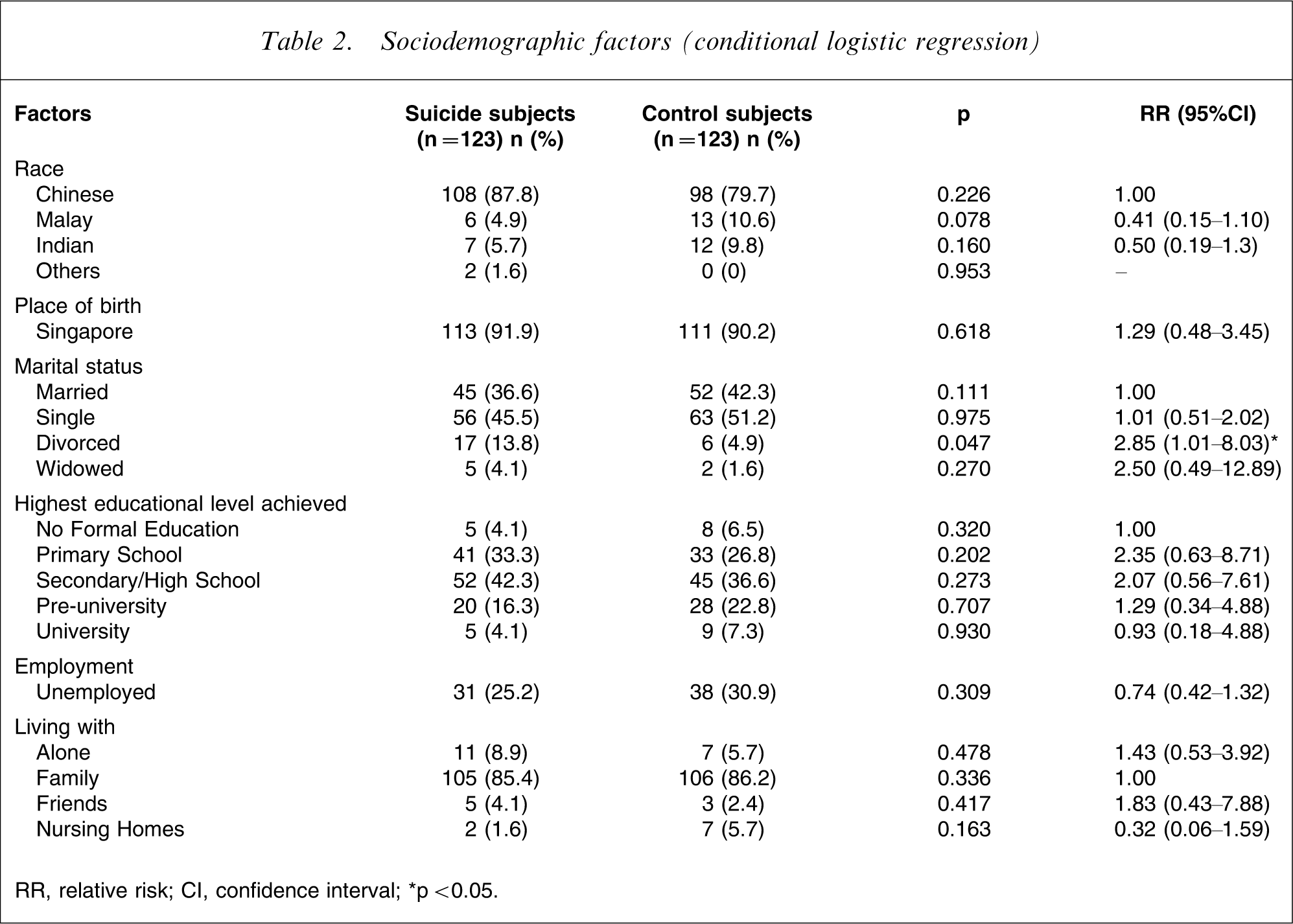
RR, relative risk; CI, confidence interval.
∗p < 0.05.
Diagnosis and psychiatric comorbidity
Table 3 shows the relative risks of clinical variables found to influence suicide in psychiatric patients. The most common principal diagnoses were schizophrenia (n = 57, 46.3%) and major depressive disorder (n = 33, 26.8%). The other diagnoses were bipolar disorder (n = 8, 6.5%; the last episode of two were depressed, and the other six were manic), adjustment disorder (n = 5, 4.1%), delusional disorder (n = 5, 4.1%), schizoaffective disorder (n = 3, 2.4%), brief psychotic disorder (n = 2, 1.6%) and obsessive–compulsive disorder (n = 2, 1.6%). The remaining eight suicide subjects had substance-induced psychotic disorder, anxiety disorder (not specified), conduct disorder, mental retardation, opioid and benzodiazepine dependence, alcohol dependence, personality disorder (not otherwise specified) and no mental illness. The controls were well matched for sex, age (mean ages for suicide and control subjects were 43.0 years and 43.1 years, respectively) and diagnosis. There was greater psychiatric comorbidity in suicide than control subjects. For suicide subjects the most common comorbidity was depression: 12 (9.8%) compared to three (2.4%) control subjects. It was found that nine out of the 12 suicide subjects with comorbid depression had schizophrenia as their principal diagnosis.
Clinical factors (conditional logistic regression)
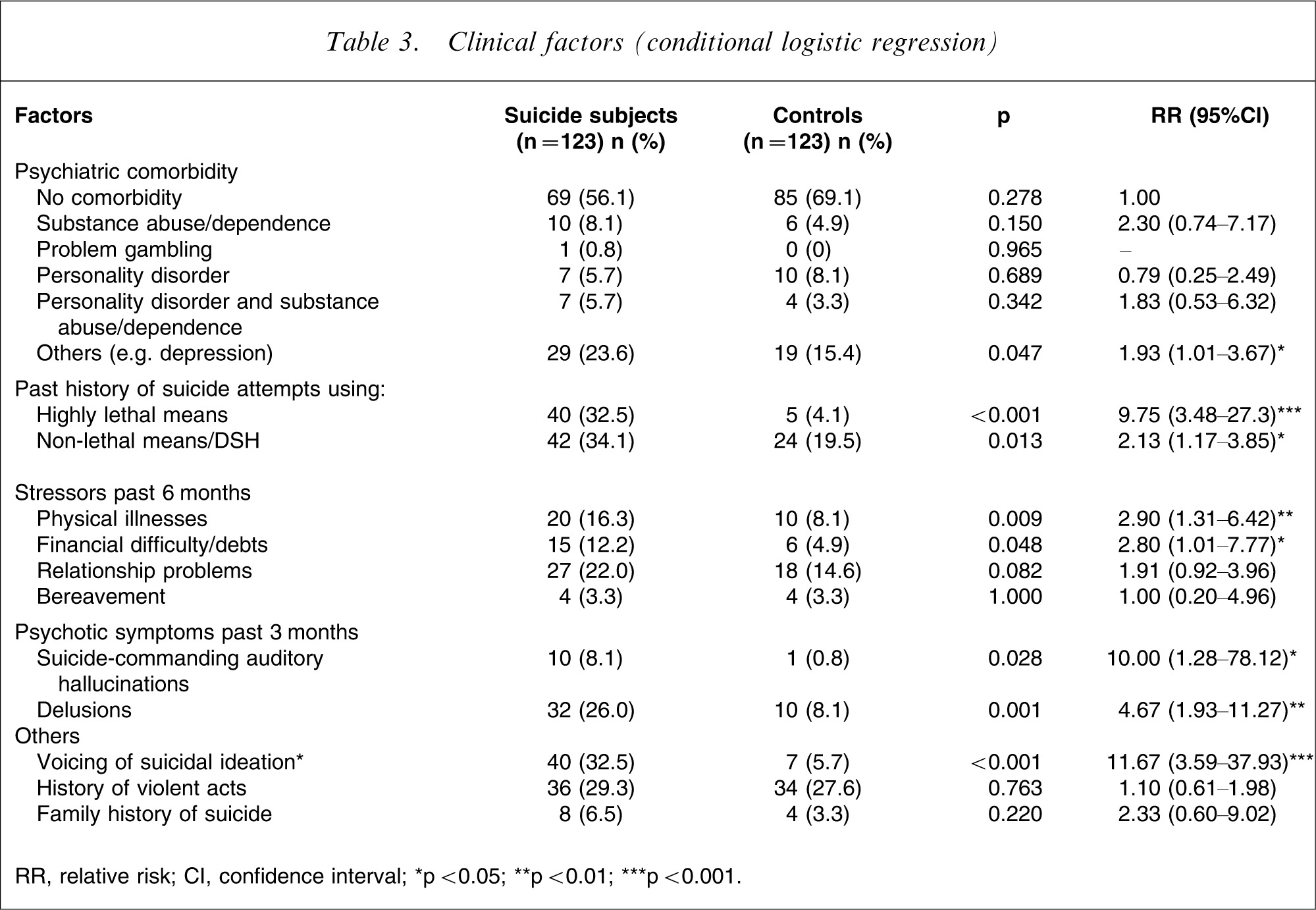
RR, relative risk; CI, confidence interval.
∗p < 0.05; ∗∗p < 0.01; ∗∗∗p < 0.001.
History of attempted suicide
Significantly more suicide subjects compared to controls previously attempted suicide using highly lethal methods such as hanging and jumping, as well as using less lethal means such as self-cutting.
Comorbid physical illness
Significantly more suicide subjects compared to controls were suffering from physical illnesses that caused significant suffering and disability. These physically ill suicide subjects were older than the general sample: the mean age was 52.9 years (range = 40–74 years). More of these suicide subjects (50%) were diagnosed with depression than schizophrenia (30%).
Ten (50%) of these physically ill suicide subjects had been given a definite medical diagnosis: these include cerebrovascular accident, benign prostatic hypertrophy, lower limb fractures, liver impairment, migraine, osteoarthritis of the knees, myasthenia gravis, neuroleptic malignant syndrome, nasopharyngeal carcinoma and urinary tract infection. The other 10 suicide subjects were not given definite diagnoses but instead were recorded as complaining of distressing pain or weakness (either generalized or specific to the lower limbs).
Financial difficulties
Significantly more suicide subjects had financial difficulties compared to controls (12.2% vs 4.9%). Most of these suicide subjects were aged 30–55 years, the mean age being 43.9 years, and there were noticeably more men (73.3%) than women (26.7%) when compared with suicide subjects without financial problems. Six (40%) of these suicide subjects suffered from depression and four (26.7%) had schizophrenia; 80% of them were working.
Psychotic symptoms
Psychotic symptoms in the form of suicide-commanding auditory hallucination and delusions were associated with significantly increased risk of suicide. Of the 32 suicide subjects with delusions (26.0%), there were 20 suicide subjects with schizophrenia (62.5%), five with depression (15.6%), and three with delusional disorder (9.4%). Most of these delusions were persecutory in nature (75.1%), with the rest having delusions of reference, grandiosity and somatic delusions. Suicide-commanding auditory hallucinations were uncommon: only 10 suicide subjects (8.1%) versus one control (0.8%). Of these 10 suicide subjects, half (50%) were diagnosed with schizophrenia; 18.8% of suicide subjects had both delusions and suicide-commanding auditory hallucinations.
Suicidal ideation
Significantly more suicide subjects expressed suicidal ideation to mental health-care workers compared to controls. Further analysis showed that suicide subjects with schizophrenia (17.5% of suicide subjects with schizophrenia) were less likely than suicide subjects with depression (48.5% of suicide subjects with depression) to express suicidal ideation.
Course of illness
Table 4 shows the relative risks of treatment-related variables found to influence suicide in psychiatric patients. Being seen in the emergency room at first presentation (instead of being seen in a regular outpatient clinic) was associated with significantly increased risk of suicide. More suicide subjects died by suicide in the initial period of the illness. Hence by the end of the first year of first presentation at the hospital, 29 suicide subjects (23.6%) would have died by suicide. Another 14 suicide subjects (11.4%) would have died at year 2, and another 10 suicide subjects (8.1%) at year 3. In the subsequent years, the number would range from one (0.8%) to seven (5.7%) per year, until year 35.
Treatment factors (conditional logistic regression)
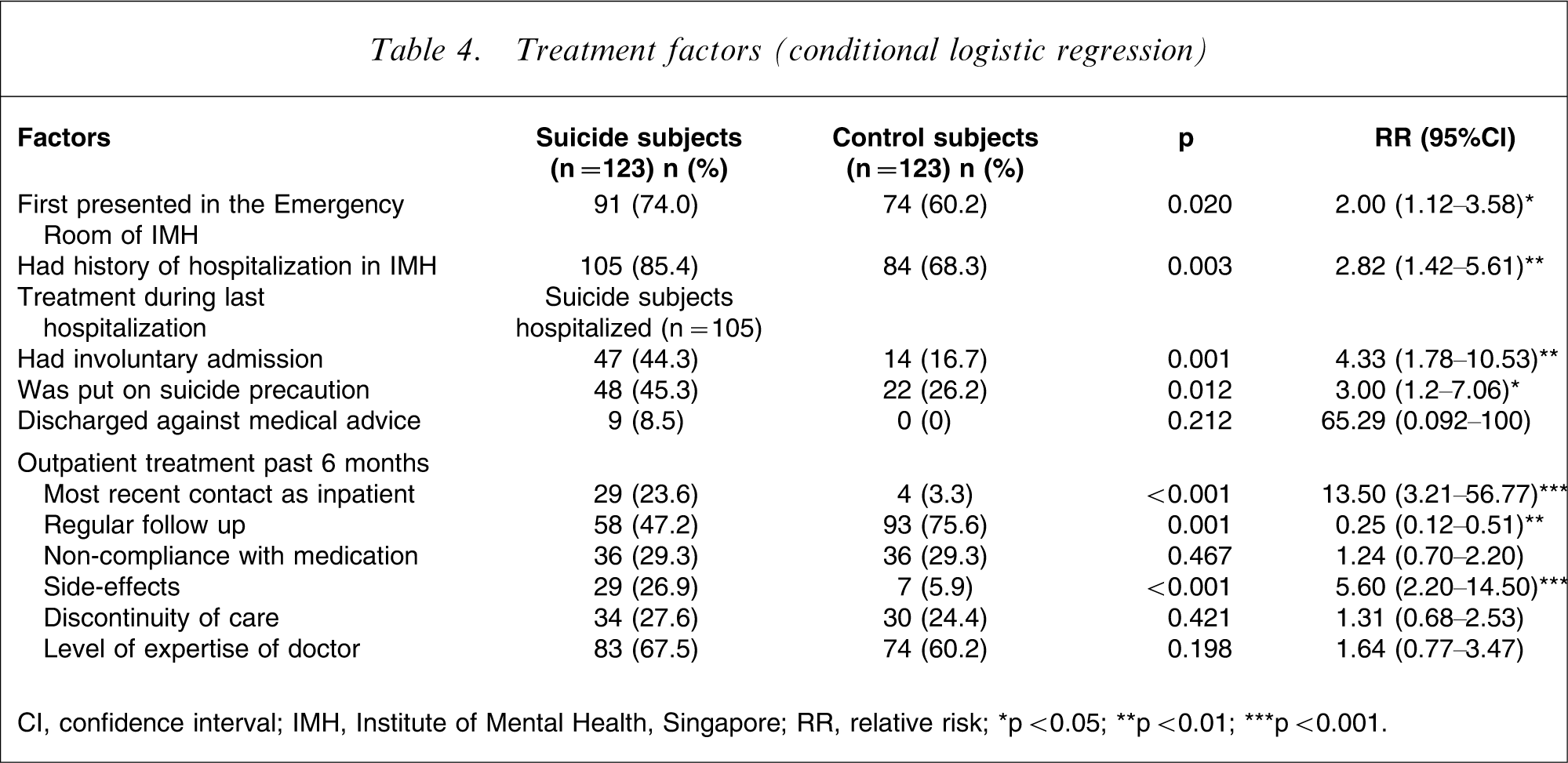
CI, confidence interval; IMH, Institute of Mental Health, Singapore; RR, relative risk.
∗p < 0.05; ∗∗p < 0.01; ∗∗∗p < 0.001.
Treatment during last hospitalization
Significantly more suicide subjects had previous hospitalization at IMH compared to controls. Both suicide subjects and controls had a similar number of psychiatric hospitalizations (approx. four) and similar length of stay during the last admission (average of 18 days). Significantly more suicide subjects were involuntarily admitted to hospital and placed on suicide precaution during the last hospitalization.
Utilization of psychiatric emergency room
Suicide subjects had an average of 0.8 visits to the emergency room of IMH during the last 6 months before suicide (with more suicide subjects having multiple visits). Controls had an average of 0.2 visits.
Outpatient follow up and compliance
Significantly more suicide subjects defaulted outpatient treatment compared to controls. Significantly more suicide subjects developed side-effects to medication compared to controls. Most of the side-effects were extrapyramidal side-effects such as drug-induced parkinsonism and acute dystonia. With regards to continuity of care, both suicide subjects and controls were equally likely to be seen by the same doctor at least 50% of the time in the past 6 months. Both were also equally likely to be seen by doctors who were registrars or above. Suicide subjects were more likely to be seen more frequently in the outpatient clinic, with more being seen weekly (2.4%), once every 2 weeks (10.6%), and once every 3–4 weeks (44.7%), compared to controls.
Stepwise conditional logistic regression
Stepwise conditional logistic regression was performed on the variables, and in the final model three independent factors best predicted suicide: history of attempted suicide using highly lethal methods (adjusted RR = 28); having a physical illness (adjusted RR = 8); and having delusions (adjusted RR = 8; Table 5).
Independent factors associated with suicide†
CI, confidence interval; RR, relative risk.
†Stepwise conditional logistic regression.
∗p < 0.05; ∗∗p < 0.01; ∗∗∗p < 0.001.
Post-discharge suicide
Figure 1 illustrates the proportion of survival within 2 years of discharge. Significantly more suicide subjects had their last contact with a mental health-care worker as an inpatient (i.e. they were not reviewed in the outpatient clinic or the emergency room after discharge). There was clustering of suicides during the period soon after discharge. Of the 105 suicide subjects who had previous admissions to the hospital, 16 suicide subjects (15.1%) had died by suicide within 1 week after discharge, 22 suicide subjects (20.8%) within 2 weeks, and by 4 weeks 28 (26.4%) were dead. By 1 year after discharge, 67 (63.2%) had died. The mode was 7 days after discharge from hospital, when five suicide subjects (4.1%) had died.
Survival within 2 years of discharge.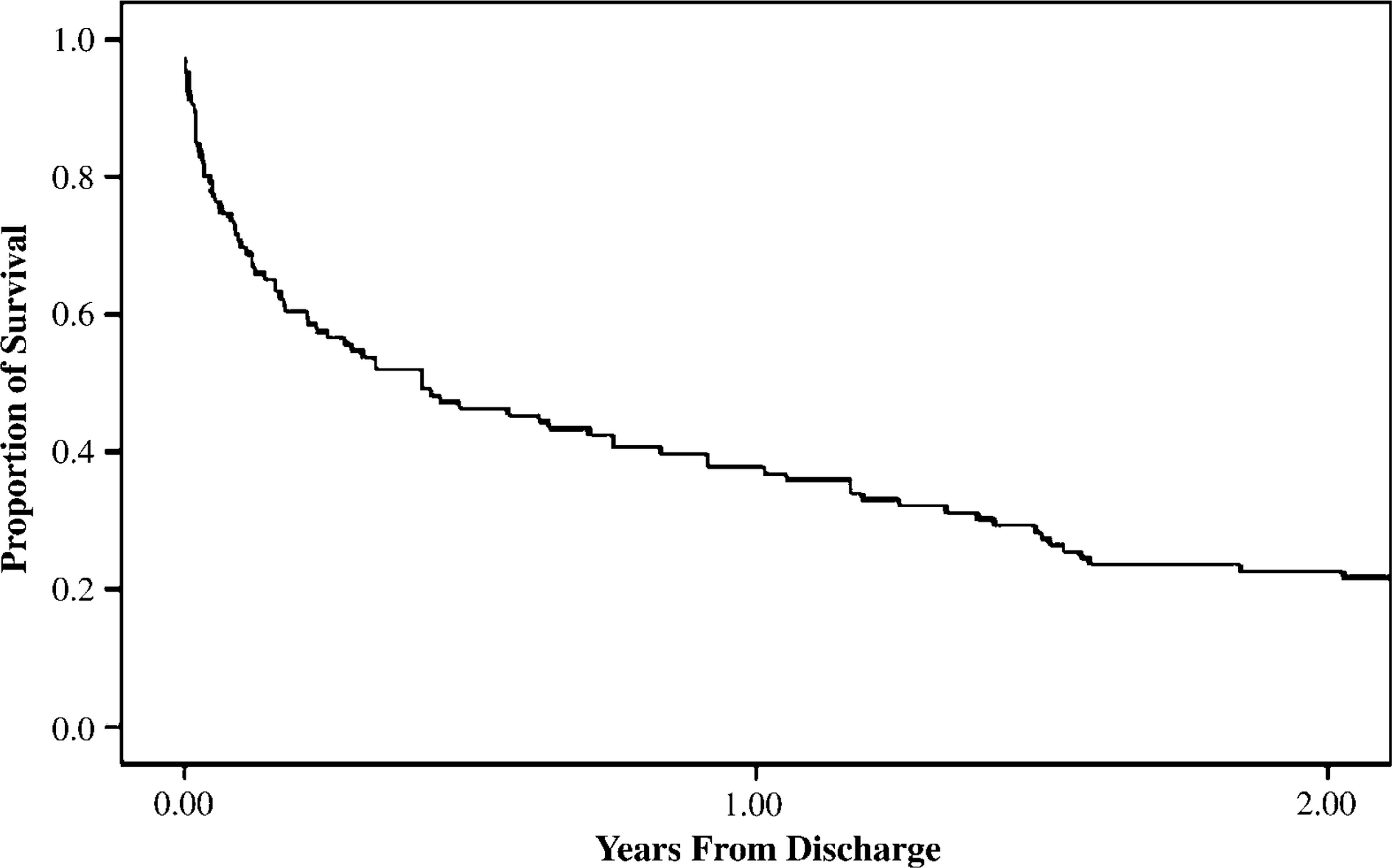
Suicide after outpatient consult
Figure 2 illustrates the proportion of survival within 1 year after an outpatient consult, which again showed the clustering of suicides after a psychiatric consult in the outpatient setting. Of the 94 suicide subjects who received outpatient treatment before suicide, seven (5.7%) died by suicide the very next day. Twenty-six (27.7%) were dead within 1 week, 42 (44.7%) were dead within 2 weeks, 39 (58.5%) were dead within 4 weeks, and within 1 year 70 (91.5%) were dead. The highest frequency (mode) was day 1 after outpatient review. Of those who died within 14 days after outpatient consult, 65% of suicide subjects had schizophrenia and 12.5% had depression as principal diagnoses, whereas of those who died after 14 days, 38.9% had schizophrenia and 35.2% had depression.
Survival within 1 year after outpatient review.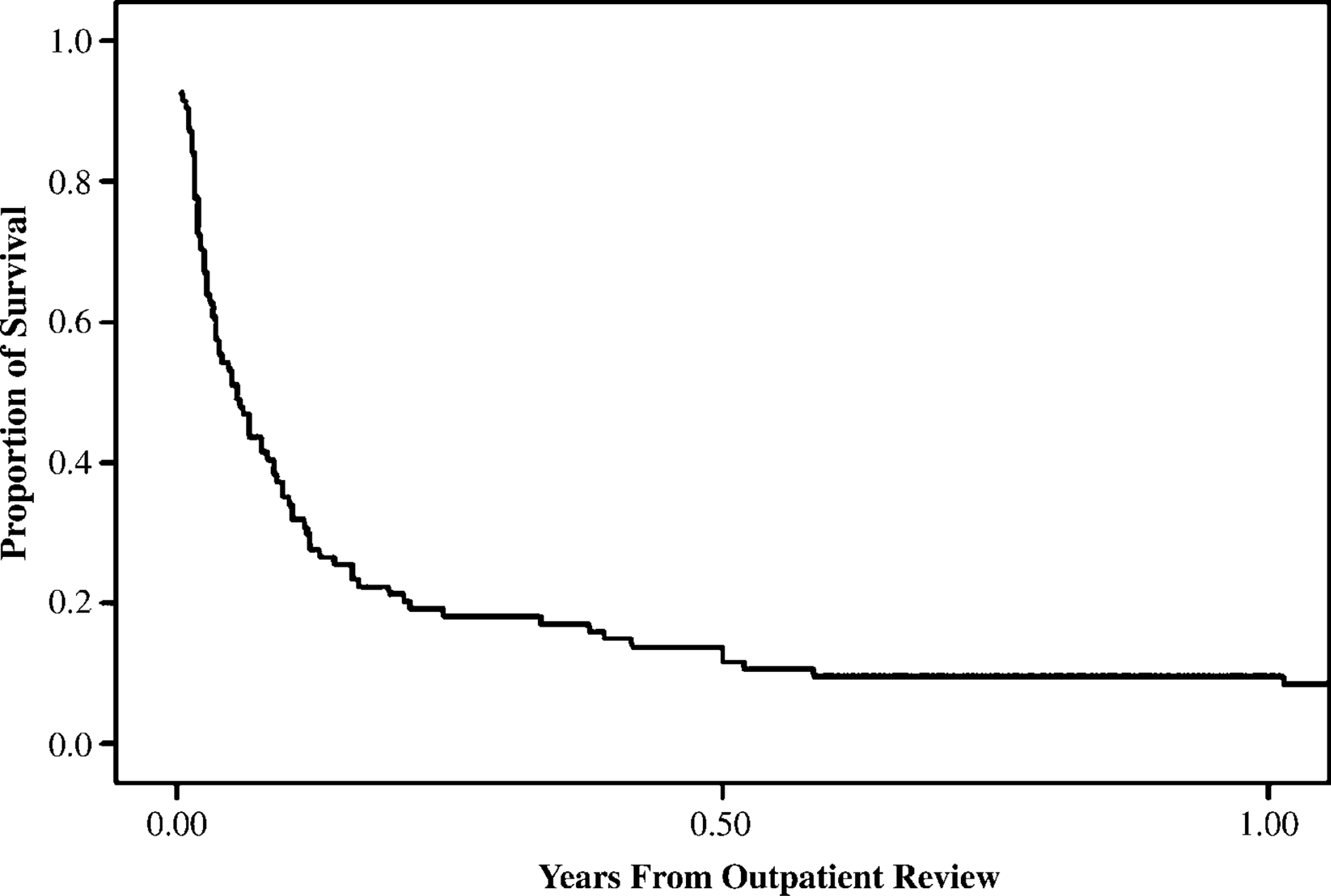
Suicide within 30 days of discharge
Compared to suicide subjects who suicided >30 days after discharge, early suicide was significantly more likely to involve relationship problems, and expression of suicidal ideation. These suicide subjects had more frequent hospitalizations (mean: early suicide = approx. 6, late suicide = 3.5), more frequent visits to the IMH emergency room and were more likely to default outpatient reviews.
Discussion
This is one of the first case–control studies to investigate risk factors and mental health care of a Southeast Asian psychiatric population who committed suicide, involving those who had and had not received inpatient treatment. The few previous studies on Asian populations involved only suicide subjects who had been admitted to hospital for psychiatric treatment. The present study shows that the risk factors in Singaporean patients do not differ much from those in Western societies.
Mental illness and psychiatric comorbidity as a risk factor
A suicidologist investigated all suicides in Singapore from 2000 to 2004, and found that up to 70% of adults (20–60 years of age) had mental illness. Depression was most common, occurring in 28.2% of the sample, followed by schizophrenia (14.4%). Furthermore, it was found that almost all subjects with schizophrenia and major depression had previous contact with mental health professionals (Chia BH: unpublished data, 2006). The significance of these figures is that those working in the mental health field are in a unique position to identify these high-risk persons, treat them and hopefully prevent suicide.
Comorbidity makes suicidal acts more likely, and the two most frequent comorbid disorders linked to suicide are depression and substance abuse or dependence. Beautrais et al. calculated that the odds ratio for suicidal behaviours escalated from 17.4 for those with one disorder to 89.7 for those with two or more DSM-III-R mental disorder diagnoses [9]. In the present study it was also found that comorbid psychiatric disorders further increased suicidal risk, and these were mostly suicide subjects who had schizophrenia with comorbid depression. A Taiwanese study found that a comorbid depressive syndrome in residual schizophrenia increased the risk of completed suicide [10]. The Finnish National Suicide Prevention Project was undertaken to examine the clinical characteristics of suicide victims with schizophrenia in Finland [11]. The study showed that two-thirds of individuals with schizophrenia who died from suicide were positive for a depressive syndrome. The acknowledgement that one is suffering from a severe mental illness with a disabling course often leads to depression, despair and sometimes suicidal behaviour.
Perhaps due to Singapore's strict anti-drug laws, comorbid substance dependence or abuse was less prevalent in the present Singaporean sample, but it appeared to be a common comorbidity in other countries. Toxicology data for completed suicides in other countries generally indicate that between 40% and 60% were legally intoxicated at the time of death [12]. Substance abuse has a disinhibiting effect on protective mechanisms against self-harm, or acts as a depressant that worsens already disturbed emotional evaluation of stressful situations.
High lethality of past suicide attempts as a risk factor
A history of parasuicide is a risk factor in most studies. Such self-harm acts occurred in around 50% of psychiatric patients who died from suicide [13], [14]. In addition, Flood and Seagar found that the last admissions of suicides were twice as likely to have followed a parasuicide [15]. The Wessex study found that a history of DSH increased the risk of suicide fourfold [3], and another study in Hong Kong showed that past suicidal attempts increased risk of suicide by 3.4-fold [7]. The present study demonstrated similar findings: a history of DSH or suicide attempt using non-lethal method doubled the risk of suicide. More significant were suicide subjects who previously attempted suicide using lethal means, such as jumping and hanging, with a 28-fold increase in risk of suicide in the present study. Obviously, those who are ready to make a dangerous attempt of high medical lethality will be at particular risk in any subsequent suicide attempts. Yim et al. found that patients who had used a violent method in the last suicide attempt had a 4.5-fold increase in suicide risk [7]. Because of the high prevalence of prior attempts among the mentally ill patients who eventually die by suicide, we may hope to prevent many suicides if we can focus on suicide attempters and their underlying psychiatric and social conditions, and monitor these patients closely after discharge.
Physical illness as a risk factor
Harris and Barraclough outlined a list of medical conditions that were associated with increased suicidal risk: chronic renal failure, HIV or AIDS, and head and neck cancer [16]. These diseases are generally chronic, debilitating, painful, deteriorating, embarrassing, stigmatizing and predisposing to dependency. In the present study the presence of physical illness predisposed to suicide. It is important to note, however, that most patients with acute or chronic physical diseases do not kill themselves. For those who do, certain risk factors such as pre-existing mental illness, poor social support and limited finances play an important role. Instead of focusing only on the psychological aspects during consultations, mental health-care providers need to be more aware of how physical illnesses are affecting their psychiatric patients. In the present study many of these symptoms were ill-defined and without formal medical diagnosis, but were nonetheless persistent, distressing and disabling to the patient. This also highlights the need for physicians working with the chronically physically ill (such as those in hospices) to be able to effectively assess suicidal risk.
Delusions and hallucinations as risk factors
Various studies have shown that psychotic disorders, mostly schizophrenia, are associated with increased risk of suicide. In particular, those with paranoid disorders and paranoid schizophrenia are highlighted as being at increased risk. Fenton et al. found that two positive symptoms (suspiciousness and delusions) were more severe among successful suicides [17]. The paranoid schizophrenia subtype was associated with an elevated risk and the deficit subtype was associated with a reduced risk of suicide. It may be that these patients with prominent negative symptoms are less aware or suffer less from the disabling effects of the disorder. Also, cognitive deficits may impair the mental processes needed to plan and execute a lethal suicide attempt. Heilä et al. found that suicides occurred throughout the course of schizophrenia, but both active illness and depressive symptoms were highly prevalent immediately before suicide [11]. The present study showed that significantly more suicide subjects who died had active psychotic symptoms before death, and they were mostly principally diagnosed with schizophrenia and delusional disorder. But note that only 8.8% of suicide subjects with schizophrenia had suicide-commanding hallucinations, similar to the 10% figure in the Heilä et al. study; this low number challenges the commonly held view that schizophrenia patients killed themselves because the voices told them to do so. Rather, a more plausible explanation is that these actively psychotic individuals killed themselves in order to escape from distressing psychotic symptoms or perceived persecution.
Communication of suicidal thought
The present study found that voicing of suicidal ideation predisposes to higher risk of suicide. One point of interest is that many of the present suicide subjects with schizophrenia failed to communicate their suicidal ideas to their doctors: only 17.5% did so. In contrast, almost half of all depressed suicide subjects expressed suicidal thoughts in the 3 months before suicide. This may be explained by the affective blunting and abnormal emotional expression in patients with schizophrenia, and in a busy outpatient clinic the depressive symptoms and suicidal ideation may be easily overlooked. Such a phenomenon might perhaps account for ‘sudden’ suicides of many patients with schizophrenia: it seemed to the clinicians that there were no ‘warning signs’ during the preceding weeks before the tragic event.
Non-compliance to treatment as a risk factor
The present study shows that significantly more suicide subjects (especially those with schizophrenia) complained of side-effects to medication, especially extra-pyramidal side-effects. Greater default of follow up in the outpatient clinic may predispose to relapses. Autopsies done on persons with previously diagnosed schizophrenia who died by suicide in Singapore from 2000 to 2004 showed that antipsychotics were detected in only 27% of the suicides (Chia BH: unpublished data, 2006). Second-generation antipsychotics, with their reduced propensity for side-effects, may be used for patients who stopped medicines on their own due to side-effects. In the longer term, clozapine has been shown to have a positive effect on suicide risk in schizophrenia patients as compared with patients treated with older neuroleptics. This decrease in suicidality in clozapine-treated patients is associated with improvement in depression and hopelessness [18].
Post-discharge clustering of suicide
The danger of suicide is substantial in the first month after discharge. The present results regarding post-discharge suicides concur with those of previous studies. Roy reported that 18% die within 1 week of entering outpatient care and 44% within 1 month [13]. Two studies from Hong Kong noted similar observations: Yim et al. demonstrated that 27.4% of psychiatric patients died within 1 month of discharge from psychiatric inpatient care [7], and Ho reported that of all the patients who suicided within 1 year of discharge, 30% died within 28 days [19]. But can we identify these patients who kill themselves very soon after discharge? The present study showed that they were more unwell, with more crises and suicidal ideation, yet poorly compliant to outpatient treatment. Kan et al. suggested a profile of an uncooperative patient with a past history of deliberate self-harm, who lived alone and who was exposed to work stresses after discharge [20].
Suicide after seeing doctor in the clinic
By arranging an early outpatient follow up after discharge, we are assuming that seeing a doctor will help reduce the risks of suicide, especially at the time just after the consultation. Unfortunately, judging from the data now presented, this may not be so, with a reasonable number of patients (5.7% in the present sample) killing themselves the very next day after a consult at the outpatient clinic. The Myers and Neal study yielded similar results: 36% of their sample killed themselves within 1 week of seeing a doctor, and 63% within 1 month [14]. A clinical audit of psychiatric patients who committed suicide in Australia showed that approximately half received care within 4 weeks of death [21].
Limitations
The present study had a number of limitations. First, the sample was restricted to IMH, a tertiary psychiatric hospital, and hence the patients referred to this hospital have more severe illness. Also IMH treats a large number of patients who have a diagnosis of schizophrenia, hence the overrepresentation of that diagnosis in this sample of suicides. Second, this is a retrospective study, and the reported psychopathology might not be as complete as in a prospective study. The quality of the information recorded varied among different doctors. Certain data were not frequently recorded, for example data concerning suicidal ideation were sometimes simply not written down. Third, the principal investigator (Thong) was not blinded to the data collection. Fourth, if we investigated only suicide subjects who were hospitalized, we would be selecting for the most severely ill patients. Hence we included suicide subjects who had no previous hospitalization, resulting in the difficulty of matching controls with suicide subjects for the specific year of treatment. Both suicide subjects and controls should have been treated at around the same time so that both samples may be comparable. Because matching using the date of last inpatient discharge could not be done for all suicide subjects, the next best way was to use a control subject who had been seen 6 months before the suicide date of the corresponding suicide subject. Because of this method of matching, the controls were biased with regards to certain variables such as default and time from last outpatient review until index date. Another problem was that when matching is done for many variables (i.e. over-matching), one is not be able to examine the importance of these matched variables (e.g. age and sex) as a risk factor for suicide. Last, despite the unavailability of the medical records of 15 suicide subjects, investigators believed that the misplacement of the records was random, and thus unlikely to constitute a systematic bias. In addition, the fairly small number of 15 suicide subjects was not likely to influence the present results.
Conclusion
The components of a suicide prevention strategy for psychiatric patients are suggested here. First, we have identified certain features of the mental state, social background, external stressors, suicidal career and course of illness that appear to be associated with increased risk. These risk factors allow us to identify and pay greater attention to this high-risk group of psychiatric patients. Second, services should increase in intensity of activity at high-risk periods such as the first few months following hospital discharge. As we move towards community psychiatric care, suicidal patients might be discharged home earlier than what was once conventional practice, perhaps at a time of incomplete recovery. Hence community care plans must emphasize recognition of suicidality, early intervention, and measures to improve compliance in high-risk patients