
Abstract
Objective:
Several epidemiological studies have evaluated the associations between dietary magnesium (Mg) and calcium (Ca) intake and the risk of depression. However, the results of these studies remain controversial. Thus, we performed a meta-analysis to explore these associations and to investigate the possible dose–response relationship between dietary Mg intake and risk of depression.
Methods:
MEDLINE, Web of Science, Embase, Cochrane CENTRAL, CINAHL database, Chinese National Knowledge Infrastructure, Wan fang databases and Databases of Chinese Scientific and Technical Periodicals were searched for eligible publications up to September 2016. Pooled relative risks with 95% confidence intervals were calculated using random-effects model. Publication bias was estimated using Egger’s test and the funnel plot. Dose–response relationship was assessed by restricted cubic spline functions.
Results:
A total of 17 epidemiological studies from 12 articles were included in the present meta-analysis. Among these studies, 11 studies evaluated the association between dietary Mg intake and risk of depression and 6 studies evaluated the association between dietary Ca intake and risk of depression. When comparing the highest with the lowest intake, the pooled relative risks of depression were 0.81 (95% confidence interval = [0.70, 0.92]) for Mg and 0.66 (95% confidence interval = [0.42, 1.02]) for Ca. Dietary Mg intake was significantly associated with a reduced risk of depression among studies conducted in Asia (relative risk = 0.57; 95% confidence interval = [0.44, 0.74]) and in studies adjusting for energy intake (relative risk = 0.73; 95% confidence interval = [0.58, 0.92]). For dose–response analysis, evidence of a nonlinear relationship was found between dietary Mg intake and risk of depression, and the largest risk reductions were observed for 320 mg/day.
Conclusion:
This meta-analysis indicated that moderate Mg intake may be inversely associated with the risk of depression, which still needs to be confirmed by larger prospective cohort studies.
Introduction
Depression is a common and disabling mental disorder. According to reports of the World Health Organization, an estimated 350 million people of all ages suffer from depression (www.who.int/mediacentre/factsheets/fs369/en/). It is predicted to be the world’s second leading cause of disease burden by 2030 (Mathers and Loncar, 2006). At present, there are adequate treatment options for depression, but several gaps in the mental health treatment exist globally (Fernandez et al., 2007; Kohn et al., 2004; Malhi et al., 2015; NICE, 2009). Thus, it is necessary to investigate effective preventive methods for depression.
Some lifestyle behaviors have been found to be among the risk factors of depression, such as sedentary behavior, short or long sleep duration and long-term stress (Slavich and Irwin, 2014; Zhai et al., 2015a, 2015b). Various dietary and nutritional factors have been reported to decrease the risk of depression, including coffee, fish, fruit and vegetables, nuts and Mediterranean or Norwegian diet etc. (Li et al., 2016; Liu et al., 2016; Quirk et al., 2013; Roca et al., 2016; Wang et al., 2016) As crucial components in foods, vitamin B12, vitamin D, folate and Omega-3 fatty acid may be significantly associated with depression (Anglin et al., 2013; Grosso et al., 2014; Petridou et al., 2015; Sarris et al., 2016). With regard to macroelements, Mg is a natural Ca antagonist and a voltage-dependant blocker of the N-methyl-
However, the results of these studies are controversial. Dietary Mg and Ca intake were found to be significantly associated with a decreased risk of depression in some studies (Jacka et al., 2012; Miki et al., 2015; Tarleton and Littenberg, 2015; Yary et al., 2013), while Yary, Sharkey, Jacka and Derom found no associations between dietary Mg and Ca intake and risk of depression (Derom et al., 2012; Jacka et al., 2009; Sharkey, 2003; Yary et al., 2016). Therefore, we conducted a dose–response meta-analysis to assess the associations between dietary intake of Mg and Ca and the risk of depression.
Method
We followed the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guideline in this meta-analysis (Moher et al., 2010).
Search strategy
MEDLINE, Web of Science, Embase, Cochrane CENTRAL, Cumulative Index to Nursing and Allied Health Literature (CINAHL) database, Chinese National Knowledge Infrastructure (CNKI), Wan fang databases and Databases of Chinese Scientific and Technical Periodicals (VIP) were searched systematically up to September 2016, using the following search terms ‘magnesium’, ‘calcium’, ‘adjunct’, ‘supplement’, ‘dietary’ and ‘depression’, ‘depressive disorder’, ‘depressive symptoms’ and ‘mood’ without restrictions. The search strategy in MEDLINE is ‘((((depression) OR depressive disorder) OR depressive symptoms) OR mood) AND (((((magnesium) OR calcium) OR adjunct) OR supplement) OR dietary)’. Furthermore, the reference lists of retrieved articles were reviewed for undetected relevant studies.
Inclusion criteria
The inclusion criteria are as follows: (1) an observational study (cohort, case-control, cross-sectional); (2) the exposure of interest was the dietary intake of Mg or Ca; (3) the outcome of interest was depression (depression was determined by self-report based on doctor’s assessment, regular use of antidepressant drugs or depression rating scales); (4) relative risks (RRs) or odds ratio with 95% confidence intervals (CIs) were provided; (5) the study was conducted within the general population (postpartum depression, depression in pregnancy, diabetes, hypertension and other related diseases population excluded); and (6) for dose–response analysis, the studies had to report RRs with 95% CIs for at least three quantitative categories of dietary Mg or Ca intake. Besides, the number of cases and participants or person-years for each category of dietary Mg or Ca intake must be provided (or data available to calculate them).
The most recent studies were chosen if data from the same population were duplicated in more than one study. Two investigators (B.R.L. and W.J.W.) searched articles and reviewed all retrieved studies independently. If the two investigators disagreed about the eligibility of an article, it was solved through discussion with a third investigator (D.F.Z. or J.L.).
Data extraction
Data extracted from each study are as follows: publication year, first author’s name, country where the study was performed, sex, age, follow-up years, study design, sample size, number of cases, dietary Mg or Ca intake assessment, depression assessment methods, multivariate-adjusted RRs and 95% CIs for each dietary Mg or Ca intake category, covariates adjusted for in the multivariable analysis.
Statistical analysis
Pooled measurement was calculated as the inverse variance-weighted mean of the logarithm of study-specific RRs to assess the associations between dietary Mg and Ca intake and risk of depression. I2 of Higgins and Thompson was used to assess heterogeneity among studies (Higgins and Thompson, 2002). The DerSimonian and Laird random-effects model (REM) was selected as the pooling method (Higgins et al., 2003). Univariate and multivariate meta-regression analyses by sex, study design, sample size, dietary intake assessment and adjustment for energy intake (yes or no) and body mass index (BMI) (yes or no) were conducted to explore potential sources of heterogeneity, and p values from meta-regression were calculated with a permutation test of 1000 to control the spurious findings (Higgins and Thompson, 2004). The leave-one-out sensitivity analysis (Patsopoulos et al., 2008) was carried out to evaluate the key studies that have substantial impacts on the between-study heterogeneity. To assess whether the results could have been affected distinctly by a single study, an influence analysis was carried out with one study removed at a time (Tobias, 1999). Publication bias was assessed with visual inspection of the funnel plot (Higgins et al., 2011) and Egger test (Egger et al., 1997).
For dose–response analysis, a two-stage random-effects dose–response meta-analysis was performed (Orsini et al., 2012). The median or mean level of dietary Mg intake for each category was assigned to the corresponding RR. When the median or mean dietary Mg intake for per category was not reported in the study, the midpoint of the upper and lower boundaries in each category was used as the average level. For the open-ended upper interval, the value arbitrarily assigned was 20% higher than the low end of the interval (Berlin et al., 1993). In the first stage, a restricted cubic spline model with three knots at the 10th, 50th and 90th percentiles of the levels of dietary Mg intake was estimated using generalized least-square regression (Harrell et al., 1988), taking into account the correlation within each set of published RRs (Orsini et al., 2006). Then the restricted maximum likelihood method in a multivariate random-effects meta-analysis was used to combine the study-specific estimates (Jackson et al., 2010). All statistical analyses were performed with STATA version 12.0 (Stata Corp, College Station, TX, USA). All reported probabilities (p values) were two-sided with p < 0.05 considered statistically significant.
Results
Literature search and study characteristics
Initially, 70,519 articles from MEDLINE, 28,877 from Web of Science, 29,341 from Embase, 3938 from Cochrane CENTRAL, 2513 from CINAHL database, 7154 from Wan fang databases, 7173 from VIP and 1796 from CNKI were identified. One additional article was also found from reference lists. After reviewing the titles and abstracts, 197 articles about associations of dietary Mg or Ca intake with risk of depression were identified. After reviewing the 197 full-text articles, 185 articles were further excluded for various reasons. Overall, 12 articles with 17 studies met the inclusion criteria and were included in the meta-analysis (Aparicio et al., 2013; Bae and Kim, 2012; Derom et al., 2012; Jacka et al., 2009, 2012; Kim et al., 2015; Miki et al., 2015; Oishi et al., 2009; Sharkey, 2003; Tarleton and Littenberg, 2015; Yary et al., 2013, 2016). The flowchart for study inclusion is shown in Figure 1.
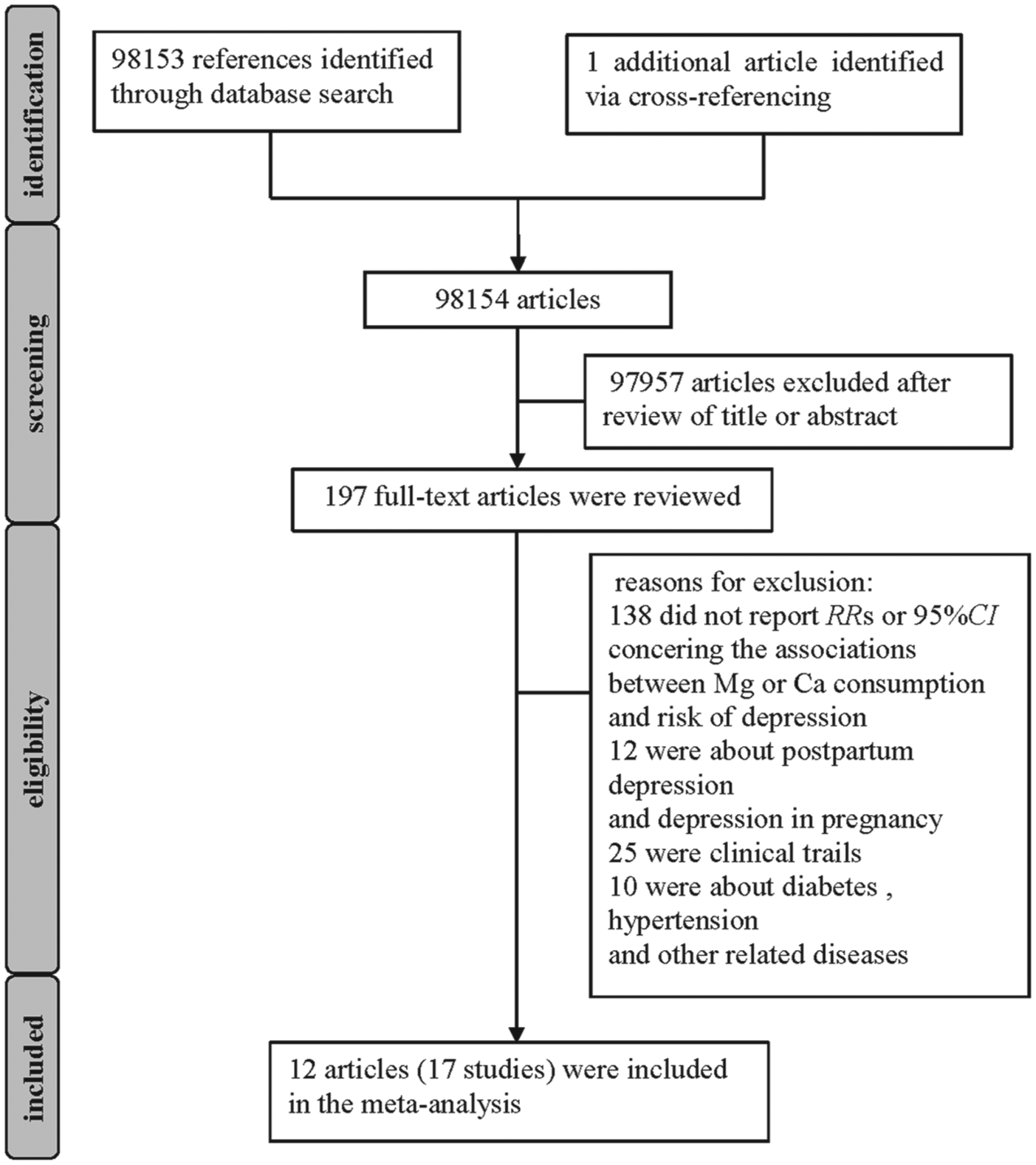
Flow diagram of literature search (relative risk [RR]).
Among the 17 studies published between 2003 and 2016, 11 studies evaluated the association between dietary Mg intake and risk of depression (Aparicio et al., 2013; Bae and Kim, 2012; Derom et al., 2012; Jacka et al., 2009, 2012; Kim et al., 2015; Miki et al., 2015; Sharkey, 2003; Tarleton and Littenberg, 2015; Yary et al., 2013, 2016), and 6 studies evaluated the association between dietary Ca intake and risk of depression (Bae and Kim, 2012; Kim et al., 2015; Miki et al., 2015; Oishi et al., 2009; Sharkey, 2003). The major adjusted confounding factors included age, sex, race, education, marital status, BMI, smoking, alcohol use and energy intake. The baseline characteristics of included studies are shown in Table 1.
Characteristics of the studies included on intake of Mg and Ca and risk of depression.
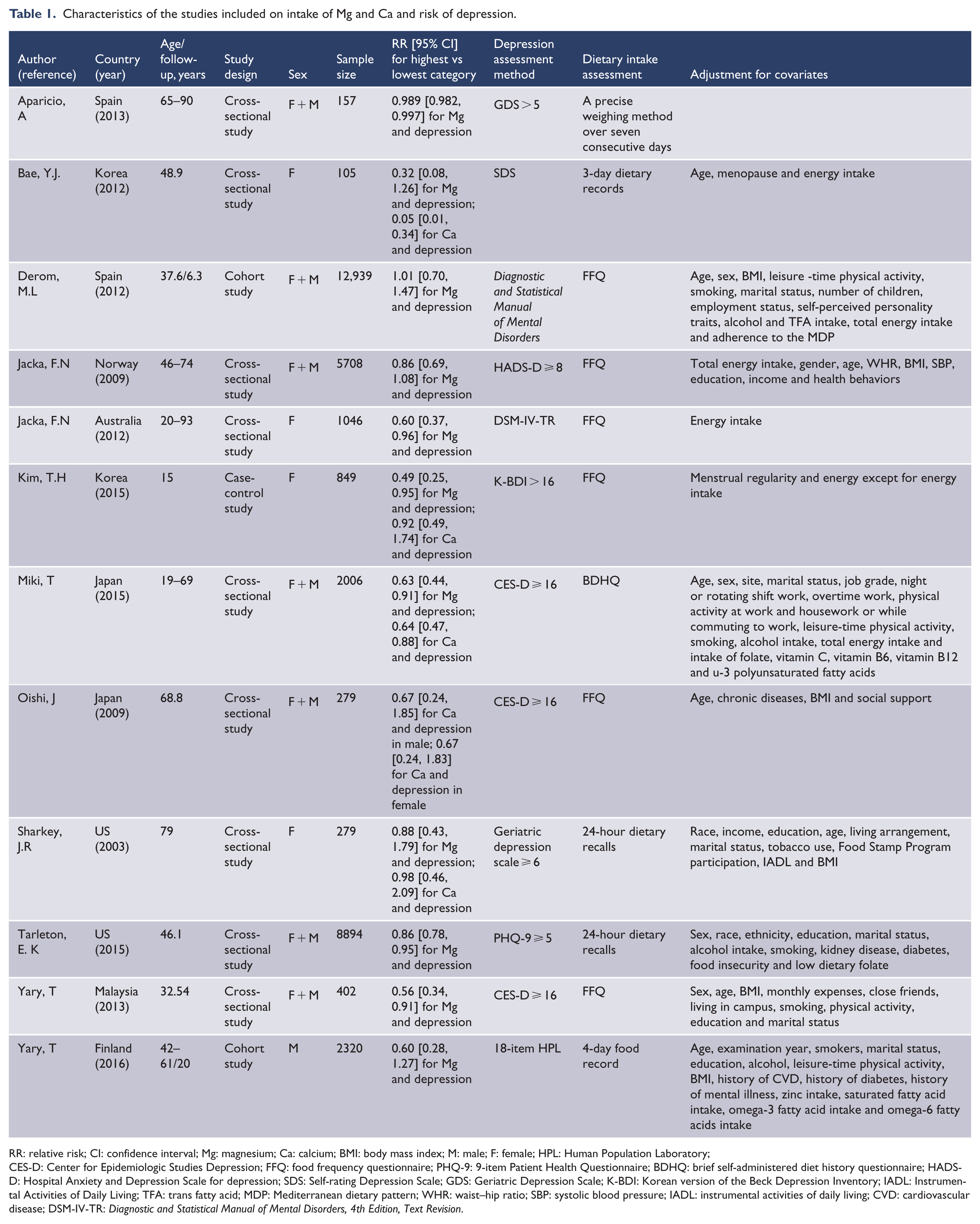
RR: relative risk; CI: confidence interval; Mg: magnesium; Ca: calcium; BMI: body mass index; M: male; F: female; HPL: Human Population Laboratory;
CES-D: Center for Epidemiologic Studies Depression; FFQ: food frequency questionnaire; PHQ-9: 9-item Patient Health Questionnaire; BDHQ: brief self-administered diet history questionnaire; HADS-D: Hospital Anxiety and Depression Scale for depression; SDS: Self-rating Depression Scale; GDS: Geriatric Depression Scale; K-BDI: Korean version of the Beck Depression Inventory; IADL: Instrumental Activities of Daily Living; TFA: trans fatty acid; MDP: Mediterranean dietary pattern; WHR: waist–hip ratio; SBP: systolic blood pressure; IADL: instrumental activities of daily living; CVD: cardiovascular disease; DSM-IV-TR: Diagnostic and Statistical Manual of Mental Disorders, 4th Edition, Text Revision.
Quantitative synthesis
Dietary Mg intake and risk of depression
Among the 11 studies, 4 studies were carried out in Asia (Bae and Kim, 2012; Kim et al., 2015; Miki et al., 2015; Yary et al., 2013), 4 in Europe (Aparicio et al., 2013; Derom et al., 2012; Jacka et al., 2009; Yary et al., 2016), 2 in America (Sharkey, 2003; Tarleton and Littenberg, 2015) and 1 in Oceania (Jacka et al., 2012). As for study design, there were eight cross-sectional studies (Aparicio et al., 2013; Bae and Kim, 2012; Jacka et al., 2009, 2012; Miki et al., 2015; Sharkey, 2003; Tarleton and Littenberg, 2015; Yary et al., 2013), two cohort studies (Derom et al., 2012; Yary et al., 2016) and one case-control study (Kim et al., 2015). One study (Kim et al., 2015) was conducted in adolescents and the others in adults. Six studies revealed a significant association between dietary Mg intake and the risk of depression, while the other five studies found no association. The pooled RR of depression for the highest vs the lowest intake of Mg was 0.81 (95% CI = [0.70, 0.92]; I2 = 69.6%; REM; p for heterogeneity <0.001; Figure 2). The results remained significant (RR = 0.83; 95% CI = [0.72, 0.94]) for studies conducted in adults, after excluding the single study conducted in adolescents.

Forest plot of the relative risks (RRs) with corresponding 95% CIs of studies on dietary magnesium (Mg) intake and risk of depression. The size of gray box is positively proportional to the weight assigned to each study, which is inversely proportional to the standard error of the OR, and horizontal lines represent the 95% CI.
Subgroup analyses by continent and adjustment for BMI and energy intake were conducted. The results revealed that there was a statistically significant association between dietary Mg intake and risk of depression for studies carried out in Asia (RR = 0.57; 95% CI = [0.44, 0.74]), but the association was not statistically significant in Europe (RR = 0.98; 95% CI = [0.93, 1.03]). The pooled RRs were 0.83 (95% CI = [0.69, 0.99]) for studies adjusting for BMI and 0.80 (95% CI = [0.67, 0.95]) for those without adjustment for BMI. The pooled RRs were 0.73 (95% CI = [0.58, 0.92]) for studies adjusting for energy intake and 0.88 (95% CI = [0.76, 1.02]) for those without adjustment for energy intake. The pooled RR for women was 0.60 (95% CI = [0.43, 0.83]; I2 = 0.0%; p for heterogeneity = 0.520).
For dose–response analysis, data from five articles (Bae and Kim, 2012; Derom et al., 2012; Kim et al., 2015; Tarleton and Littenberg, 2015; Yary et al., 2016) including six studies were used. A nonlinear relationship between dietary Mg intake and depression was found (p for nonlinearity = 0.0038; Figure 3). The RRs with 95% CIs of depression were 0.93 (95% CI = [0.88, 0.98]), 0.86 (95% CI = [0.77, 0.97]), 0.87 (95% CI = [0.78, 0.98]), 0.93 (95% CI = [0.81, 1.06]) and 1.03 (95% CI = [0.86, 1.24]) for 138, 320, 361, 465 and 581 mg/day of dietary Mg intake, respectively.
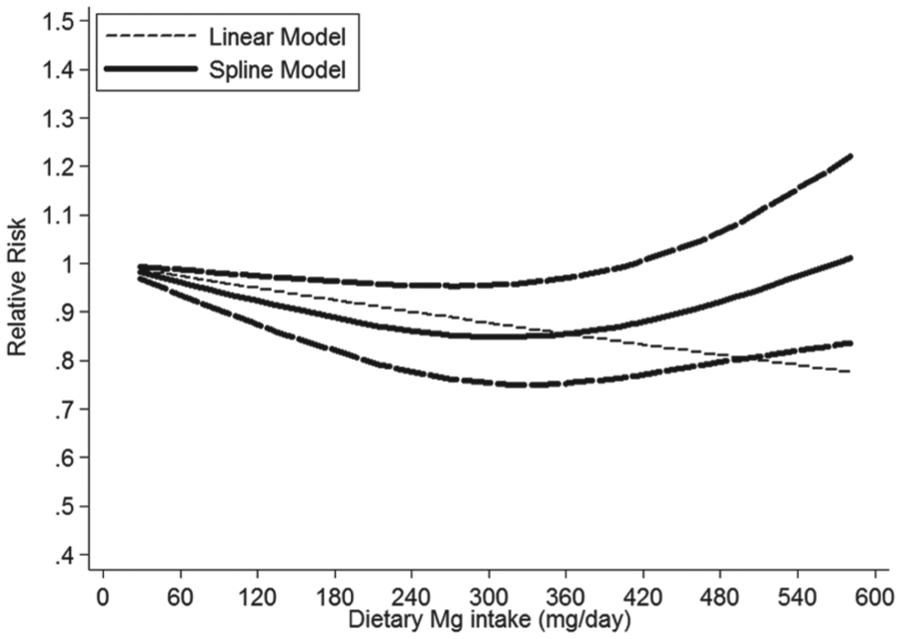
Dose–response relationship between dietary magnesium (Mg) intake and risk of depression.
Dietary Ca intake and risk of depression
Among the six studies, five studies were carried out in Asia (Bae and Kim, 2012; Kim et al., 2015; Miki et al., 2015; Oishi et al., 2009) and one in America (Sharkey, 2003). There were five cross-sectional studies (Bae and Kim, 2012; Miki et al., 2015; Oishi et al., 2009; Sharkey, 2003) and one case-control study (Kim et al., 2015). Three studies revealed a significant association between dietary Ca intake and the risk of depression, whereas the others reported no significant association. The pooled RR of depression for the highest vs the lowest dietary intake of Ca was 0.66 (95% CI = [0.42, 1.02]; I2 = 51.6%; p for heterogeneity = 0.066; Figure 4).
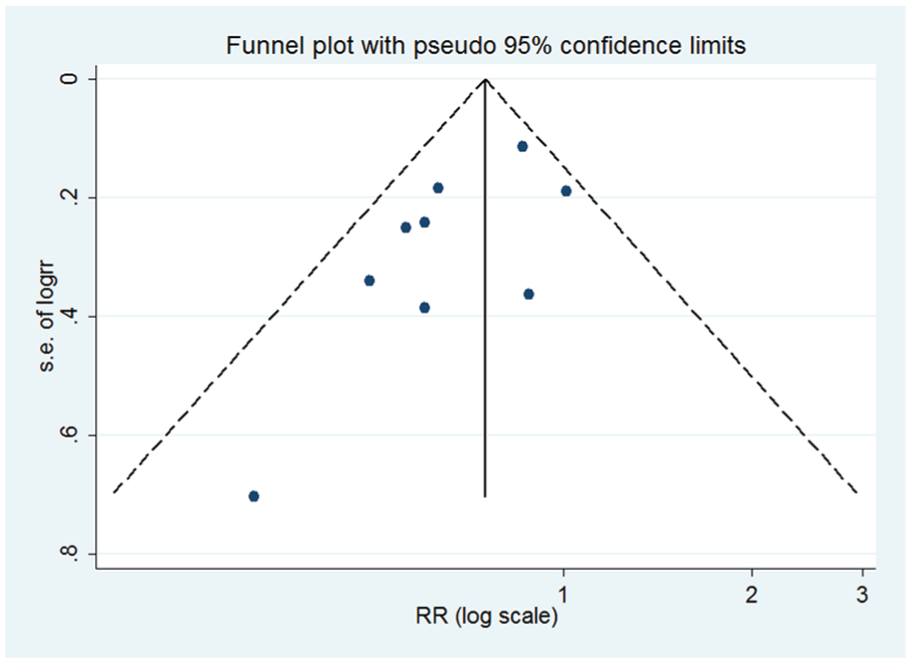
Funnel plot with pseudo 95% confidence limits for the analysis of dietary magnesium (Mg) intake and risk of depression after removing two studies which have a strong effect on heterogeneity (RR, relative risk).
Meta-regression and sensitivity analysis
Moderate heterogeneity was found in the analyses of dietary Mg (I2 = 69.6%; p for heterogeneity < 0.001) and Ca intake (I2 = 51.6%; p for heterogeneity = 0.066) and risk of depression. In the analysis of dietary Mg intake and depression, p values of univariate meta-regression analysis with the covariates of sex, study design, sample size, dietary intake assessment, adjustment for BMI and energy intake were 0.11, 0.92, 0.63, 0.12, 0.94 and 0.33, respectively, and p values from multivariate meta-regression were 0.08, 0.69, 0.36, 0.11, 0.28 and 0.62, respectively. A joint test for all six covariates gave a p value of 0.09, indicating no evidence for their interactions. In the analysis of dietary Ca, p values of univariate meta-regression analysis with the covariates of study design, dietary intake assessment, adjustment for BMI and energy intake were 0.54, 0.21, 0.67 and 0.50, respectively, and the p values from multivariate meta-regression were 0.24, 0.60, 0.93 and 0.26, respectively. The p value for the joint test for all four covariates was 0.43.
In the leave-one-out analysis of dietary Mg intake and risk of depression, two studies (Aparicio et al., 2013; Tarleton and Littenberg, 2015) were found to contribute to the moderate heterogeneity. After further excluding these two studies, the heterogeneity decreased (I2 = 24.1%, p = 0.229) and the result remained significant (RR = 0.72; 95% CI = [0.60, 0.86]). In the analysis of dietary Ca intake and risk of depression, one study (Bae and Kim, 2012) was found to contribute to the moderate heterogeneity. After further excluding this single study, the heterogeneity decreased (I2 = 0.0%, p = 0.791), and an inverse association was found between dietary Ca intake and risk of depression (RR = 0.71; 95% CI = [0.56, 0.91]).
Influence analysis and publication bias
Influence analysis showed that no individual study had an excessive influence on the above-mentioned pooled RRs. The funnel plot and Egger test showed no evidence of significant publication bias in the analysis between dietary Ca intake and risk of depression (p = 0.508), but publication bias was found in the analysis between dietary Mg intake and risk of depression. However, no significant publication bias was found (p = 0.06; Figure 5) after removing two studies (Aparicio et al., 2013; Tarleton and Littenberg, 2015), which had strong effect on heterogeneity.
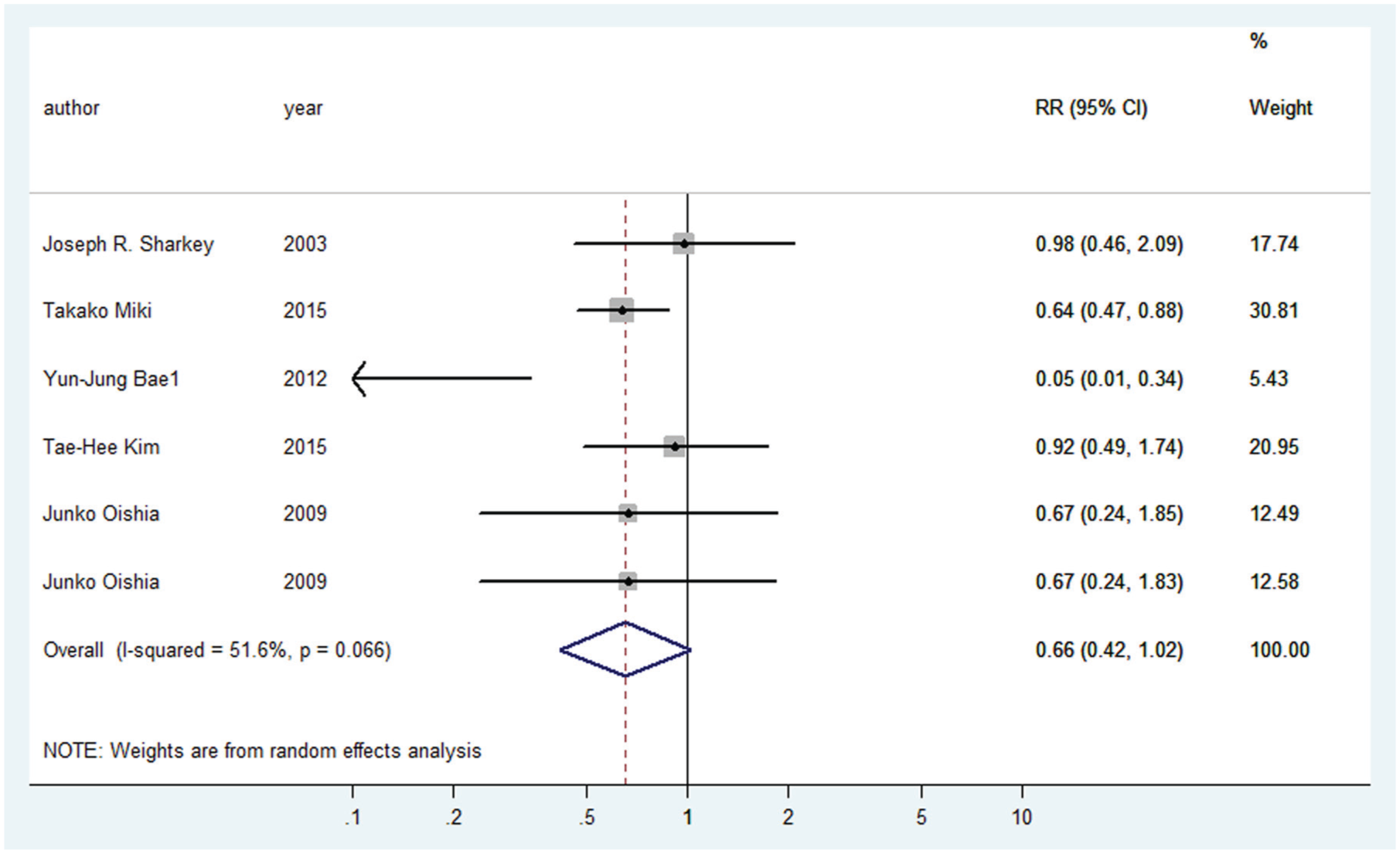
Forest plot of the relative risks (RRs) with corresponding 95% CIs of studies on dietary calcium (Ca) intake and risk of depression. The size of gray box is positively proportional to the weight assigned to each study, which is inversely proportional to the standard error of the OR, and horizontal lines represent the 95% CI.
Discussion
To our knowledge, this is the first meta-analysis to quantitatively evaluate the associations of dietary Mg and Ca intake with risk of depression. This meta-analysis included 17 studies from 12 articles. The results were indicative of a significant inverse association between moderate Mg intake and the risk of depression, but no significant association between dietary Ca intake and risk of depression. Dietary Mg intake was also significantly associated with a reduced risk of depression among studies conducted in Asia and studies adjusting for energy intake. The pooled results of studies conducted in Asia showed the strongest association may be due to that the majority of included studies were conducted in Asia. Energy intake might be a confounding factor in the analysis of dietary Mg intake with depression (Miki et al., 2015), so the association revealed strongest in studies adjusting for energy intake. A nonlinear relationship was also found between dietary Mg intake and risk of depression. The association became significant when the dietary Mg intake was above 76 mg/day and below 360 mg/day, and the largest risk reductions were observed for 320 mg/day. As a matter of fact, 320 mg/day is approximate to recommended intake level in China (Cheng Yiyong, 2014).
The exact biological mechanisms underlying dietary Mg and Ca intake and risk of depression are still not completely determined. There have been several possible explanations. First, Mg may play important roles in the regulation of the hypothalamic–pituitary–adrenal (HPA) system and contribute to lowering systemic inflammation (Almoznino-Sarafian et al., 2007). HPA system is confirmed to be the main stress response system (Sartori et al., 2012), and dysregulation of the HPA system can affect the levels of stress hormones, which is related to depressive symptoms (Reul and Holsboer, 2002). In addition, Mg is also a predominant intracellular cation and plays a role in a plenty of enzymatic reactions (Sanders et al., 1999; Touyz, 2004). Second, Ca activates tryptophan hydroxylase in the biosynthetic pathway causing serotonin synthesis (Knapp et al., 1975). Moreover, the calcium/calmodulin-dependent system may enhance the dopamine synthesis in the brain (Sutoo and Akiyama, 1997). Ca works as a signal in cells of the immune system as well (Rao and Hogan, 2009). Changes in the extracellular calcium concentration may influence the excitability of neuromuscular tissues involved in emotional regulation (Carman and Wyatt, 1979). Last, Mg is a natural Ca antagonist and a voltage-dependant blocker of the NMDA channel, and it also plays a role in the entrance of calcium into the neuron (Bresink et al., 1995; Iseri and French, 1984). Mg is likely to protect the neuron against cell death by regulating this entry (Sobolevskii and Khodorov, 2002; Wan, 2006). Dietary Mg intake may be associated with depression via protecting nervous system (Bourre, 2006).
Between-study heterogeneity is common in meta-analysis because of characteristics of the sample, diversity in population stratification, measurement of Mg and Ca intake, variation of the covariates etc. Moderate heterogeneity was found in this meta-analysis. Thus, univariate and multivariate meta-regression was conducted to explore the source of heterogeneity. But, it was failed to find the covariates of sex, study design, sample size, dietary intake assessment and adjustment for energy intake and BMI as the potential contributors to the between-study heterogeneity. A joint test for all covariates indicated no evidence for their interactions. In subgroup analyses by continent, the heterogeneity decreased to 0% for studies carried out in Asia, 0% in America and 5.8% in Europe. The continent may be one of the sources of heterogeneity. Depression symptoms have been assessed via self-report or questionnaires in the majority of the included studies. Clinical interview methods were used to assess depression symptoms in two included studies. Presumably, differences in depression assessment methods may have contributed to the heterogeneity. Furthermore, many different estimated methods of nutrient intake were reported, such as Nutrica software, Norwegian Food Composition table and so on, which may be an important determinant in the heterogeneity. The leave-one-out sensitivity analysis was also conducted to further explore the potential sources of heterogeneity. In the analysis between dietary Mg intake and risk of depression, the heterogeneity decreased after excluding two studies. And the results remained significant, because obesity is a risk factor of depression (Luppino et al., 2010), and thesetwo studies did not adjust for BMI and energy intake. It may give rise to that these two studies have a strong effect on heterogeneity. In the analysis of dietary Ca, the heterogeneity decreased after excluding one study. The accuracy of the results in this study may contribute to the heterogeneity due to the small sample size.
There are several strengths in present meta-analysis. First, this study included a large number of participants, allowing a much great possibility of reaching reasonable conclusions. Second, nearly all the RRs we extracted had adjusted for potential confounders, such as age, sex, BMI, alcohol intake and smoking, increasing the credibility of the results. Third, a significant association was also found between dietary Mg intake and risk of depression among studies adjusting for BMI and studies without adjustment for BMI, indicating the stability and accuracy of the results. Fourth, the dose–response analysis was conducted to evaluate the relationship between Mg intake and depression quantitatively. A moderate level of Mg intake was found, which is approximate to recommended intake level for general population in all Asia.
However, several limitations of the study should also be considered. First, potential confounders adjusted for in each study were different, and it may affect the results to some extent, and residual confounding should be of concern as well. Second, publication bias was found in the analysis of dietary Mg intake and risk of depression. But the bias was not evident after removing two studies that had a strong effect on heterogeneity, and the result remained significant. Third, the depression assessment methods were inconsistent in the included studies. Questionnaires or self-report were used to assess depression symptoms in the majority of the included studies, such as the Center for Epidemiological Studies Depression (CES-D) and Geriatric Depression Scale (GDS). Clinical interview methods were used in the minority of the included studies. The validity and reliability of different scales may affect the results. Furthermore, the cut-offs reported for depression differed a lot between the studies included. For example, the 9-item Patient Health Questionnaire (PHQ-9) score above 5 were reported as depression, but it just implied mild to moderate depressive symptoms when the score was between 5 and 10. The different cut-offs may influence the results as well. Fourth, in the subgroup analysis stratified by study design, an inverse association between Mg intake and depression risk was found in cohort studies, but it was not statistically significant. It may be due to the limited number of cohort studies. Thus, further prospective cohort studies are still needed to confirm these findings.
Conclusion
In conclusion, this meta-analysis of observational studies provides further evidence in support of a significant inverse association between dietary Mg intake and risk of depression, which still needs to be confirmed by larger prospective cohort studies.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.