
Abstract
Objective:
There is growing awareness of the range of psychosocial, lifestyle, and sociodemographic factors related to self-harm, however this research is often limited by using cross-sectional or convenience samples. And while we generally assume that young adults who self-harm experience poorer long-term outcomes, longitudinal research is needed. This paper builds on prior research using a large, representative, longitudinal sample.
Methods:
5765 Australian women completed 5 surveys (age 18–23 to 31–36). Six-month self-harm was measured by self-report. We had two aims: firstly to predict future self-harm, separately for women with and without prior self-harm. Secondly, to identify outcomes 3 and 6 years following self-harm.
Results:
Six-month self-harm prevalence was 2.5%. Predictors among women without recent self-harm included depression, dieting behaviours, number of male sexual partners, and abuse. Among women with recent or current self-harm, predictors were number of dieting behaviours, tiredness of life, and stress. Women who self-harmed reported poorer outcomes, namely greater difficulties in relationships at 3- and 6-year follow-up.
Conclusions:
Longitudinal risk factors for self-harm differed depending on prior self-harm status, and included depression, dieting behaviours, tiredness of life and stress. These factors may serve as warning signs for new or continued self-harm. This study offers new insight into long-term outcomes up to six years after self-harm, particularly with relationships.
Self-harm in young adulthood is relatively common: 6-month prevalence is around 1–2% (Young et al., 2006). The most common forms of self-harm are cutting or scratching the skin, and overdoses (Young et al., 2006). There is growing awareness of a diverse range of psychosocial, lifestyle and sociodemographic factors that are related to self-harm. However, this research faces several limitations. These factors are often referred to as ‘risk factors’ for self-harm, yet at this stage, little is known about the causal pathway. A number of findings are drawn from cross-sectional studies, from which it is not possible to assess causality or to ascertain accurate timelines (Wilcox et al., 2012). Prior research frequently uses convenience samples of university students (e.g. Goldstein et al., 2009; Whitlock et al., 2006). The mental health profiles of these samples may be atypical compared to community samples, potentially reporting lower (Goldstein et al., 2009) or higher (Stallman, 2010) levels of mental health difficulties compared with the general population. Another common limitation is using a narrow set of factors (e.g. a focus on alcohol-related factors: Ogle and Clements, 2008). In these instances, it is difficult to compare the relative effect of variables studied, or to have confidence that the effects found are not due to unmeasured related factors (for further discussion, see Wilcox et al., 2012).
Thus, we need longitudinal research in large community samples incorporating a broad range of psychosocial factors. For example, Fergusson et al. (2000) investigated risk factors for self-harm in a large, longitudinal community sample aged 15–21 years. They noted the importance of early relationships, mental health problems such as depression, and exposure to stressful life events. More recently, Wilcox et al. (2012) followed a college sample annually for 4 years and identified several key predictors for self-harm, including maternal depression, non-heterosexual orientation, affective dysregulation and depression. They noted that there is still a considerable need for research in large longitudinal community samples to assist in understanding the risk and protective factors for self-harm, which can then direct prevention and intervention efforts.
While we generally assume that young adults who self-harm experience poorer long-term outcomes, we need longitudinal research to confirm this supposition using empirical data (Whitlock et al., 2006). The present study adopts a different focus to the existing limited body of research that is predominantly concentrated on continued mental health difficulties (e.g. Fergusson et al., 2005), or younger populations (Mars et al., 2014; Moran et al., 2012). Instead, we more broadly consider factors which putatively are indicators of success in life: employment, relationships, physical and mental health and life satisfaction.
One of the challenges in the literature is the wide variation in how self-harm is defined and measured. It is not within the scope of this article to discuss this issue in detail (see Kapur et al., 2013). This paper adopts a broad definition of self-harm, which includes any behaviour where a person intentionally self-inflicts harm with immediate physical consequences (Morgan, 1979). Our definition incorporates self-harm with suicidal intent and non-suicidal self-harm. While the self-harm literature is increasingly moving towards a separation of suicidal and non-suicidal self-injury, as outlined in the Diagnostic and Statistical Manual of Mental Disorders–Fifth Edition (DSM-5) (American Psychiatric Association, 2013), a number of researchers continue to raise concerns that it is not possible to make clear categories. Suicidal intent is often ambivalent, and non-suicidal self-injury is a strong risk factor for suicide attempt (Brunner et al., 2014). Thus, the classification of intent is complex and requires further research (Kapur et al., 2013). Our measurement approach is self-reported and self-defined; prior work indicates that participants are able to accurately identify self-harm in concordance with a widely accepted self-harm definition (Stanford and Jones, 2010).
This paper has two aims. First, we aim to identify the factors that predict self-harm. We hypothesised that psychosocial, lifestyle and sociodemographic factors measured in Survey 2 would predict self-harm in Survey 3, and that these factors would differ depending on self-harm status at Survey 2. We include a broad range of risk and protective factors that have been investigated in prior research, within those available in the dataset. Second, we aim to assess the effect of self-harm on subsequent outcomes. We hypothesised that self-harm reported in Survey 3 would predict financial, relationship, physical and mental health outcomes and life satisfaction reported in Surveys 4 and 5. We set out to describe these relationships longitudinally – it is not possible to attribute causation since we do not have data prior to early adulthood.
Method
Participants
Data were collected as part of the Australian Longitudinal Study on Women’s Health (ALSWH), conducted by the University of Newcastle and the University of Queensland. Participants were selected in 1996 from the Medicare database, which contains contact details of all Australian citizens and permanent residents. Sampling was random among women born between 1973 and 1978, with oversampling of rural and remote areas at twice the rate of women in urban areas. Participants in the 1973–1978 cohort completed a mailed survey in 1996, 2000, 2003, 2006 and 2009 (see Lee et al., 2005 for further details pertaining to recruitment and retention). Participants provided informed consent, with approval from the University of Newcastle Human Research Ethics Committee.
Measures
All measures are from the ALSWH surveys; questionnaires are available online (www.alswh.org.au). Items or scales that have been developed by the ALSWH are noted as such, and details pertaining to data origin and validation are also available online.
Self-harm
Self-harm was measured at Survey 3 (age 25–30) by the question ‘In the past 6 months have you EVER deliberately hurt yourself or done anything that you know might have harmed or even killed you?’ with response options ‘Yes’ and ‘No’. The item was modified from Beck and colleagues’ (1974) Suicide Intent Scale.
Antecedent factors
Antecedent factors were taken from Survey 2 in 2000 (age 22–27). Age, country of birth and age left school were obtained from Survey 1 in 1996 (age 18–23). Hereafter, antecedent factors are primarily referred to as measured in Survey 2 in 2000, for simplicity. Measures were chosen on the basis of prior self-harm research, utilising the variables included in the ALSWH.
Psychosocial factors
Depression was measured using the 10-item Center for Epidemiologic Studies Depression Scale (CES-D), Short Version (Andresen et al., 1994). The 10-item CES-D is not diagnostic, but asks respondents to report depressive symptoms experienced in the past week. Shortened versions have been found to have good internal consistency (Andresen et al., 1994) and without undue loss of specificity or sensitivity compared with the 20-item version (Shrout and Yager, 1989). Number of dieting behaviours denotes the number of methods used to control weight or shape reported in the last 12 months, from a list of 9 items, such as ‘How often have you gone on a diet to lose weight during the last year?’ based on a scale by French et al. (1995). Dissatisfaction with weight or shape in the last month is based on the sum of two items asking level of dissatisfaction in the past month (ALSWH). The six-item Life Orientation Test–Revised measures optimism and shows evidence of good internal consistency and test–retest reliability, and modest convergent and discriminant validity (Scheier et al., 1994). Life events were measured using a modified version of Norbeck’s (1984) Life Events Questionnaire, which demonstrates good test–retest reliability and validity. Results are reported as a proportion of the possible events. Lifetime physical, emotional and sexual abuse were measured using items adapted from the Australian Bureau of Statistics (ABS, 1996) by ALSWH and assessed lifetime abuse from any person. In addition, two items measured recent physical and emotional abuse, drawn from Hwalek and Sengstock (1986). ‘Tiredness of life’ was measured by a question that asked have you been ‘feeling that life isn’t worth living’ in the past week. Stress was represented by a mean score based on participants’ reports of stress in the last 12 months in 10 areas of life, such as own health and living arrangements (ALSWH). The stress scale displays good internal reliability and validity (Bell and Lee, 2003). Sexual history was measured by participants’ reported number of male and female sexual partners. Greater than 30 partners was truncated to 30, for the purpose of analysis (0.7% of valid responses). Participants were asked to select which option most closely described their sexual orientation (dichotomised: heterosexual, other).
Lifestyle factors
Participants reported frequency of binge drinking, as defined as more than five standard drinks of alcohol on one occasion (modified from the Australian Institute of Health and Welfare and National Heart Foundation, 1990). Smoking was calculated based on reported cigarettes smoked, reported in units of 20 cigarettes per week. Pattern of drug use summarised participants’ detailed reports of illicit drugs in the following two patterns: exclusive use of cannabis and use of multiple drugs (may or may not include cannabis use), within the last 12 months and more than 12 months ago. Items were derived from the National Drug Strategy (1996; see Turner et al., 2003 for further details of scale construction). Exercise status was recorded as five categories ranging from nil/sedentary to high, based on total number of minutes exercising per week (Armstrong et al., 2000).
Sociodemographic factors
Sociodemographic factors included age, age left school, country of birth (dichotomised), highest education level completed, and current living arrangement (ALSWH; ABS, 1996). Rurality was assessed using the Accessibility/Remoteness Index of Australia Plus (ARIA+) based on the participant’s address in 2000 (Department of Health and Aged Care [GISCA], 2001).
Outcomes
Outcomes were measured at Survey 4 (age 28–33) and at Survey 5 (age 31–36).
Financial
Financial stress was measured by the question ‘How do you manage on the income you have available?’ dichotomised into ‘difficulty managing’ and ‘managing ok’. Level of employment was represented by three categories: Not employed, less than 25 hours and 25 hours or more per week. Women who reported that they would like to do more hours of paid work than they currently do were considered underemployed (modified from ABS, 1996).
Relational
Marital status was represented by four categories: Married, Never married, De facto (opposite sex and same sex combined) and Separated/Divorced/Widowed (Modified from ABS, 1996). Number of children was numeric.
General and mental health
The Short-Form General Health Survey (SF-36) comprises 36 items measuring health-related quality-of-life (Ware and Sherbourne, 1992). The scale comprises four Physical Health scales and four Mental Health scales (see Table 1); each scale produces a numeric score 0–100). The SF-36 demonstrates excellent test–retest and internal reliability, and content and predictive validity (Ware et al., 1993, 1994). Life satisfaction measures general satisfaction with seven areas such as work and friendships; the scale is numeric with scores ranging from 1 to 5 (ALSWH).
Risk factors (Survey 2, age 22–27) predicting self-harm (Survey 3, age 25–30), separately for women who self-harmed at Survey 2 and women who did not self-harm at Survey 2: Unadjusted and adjusted.
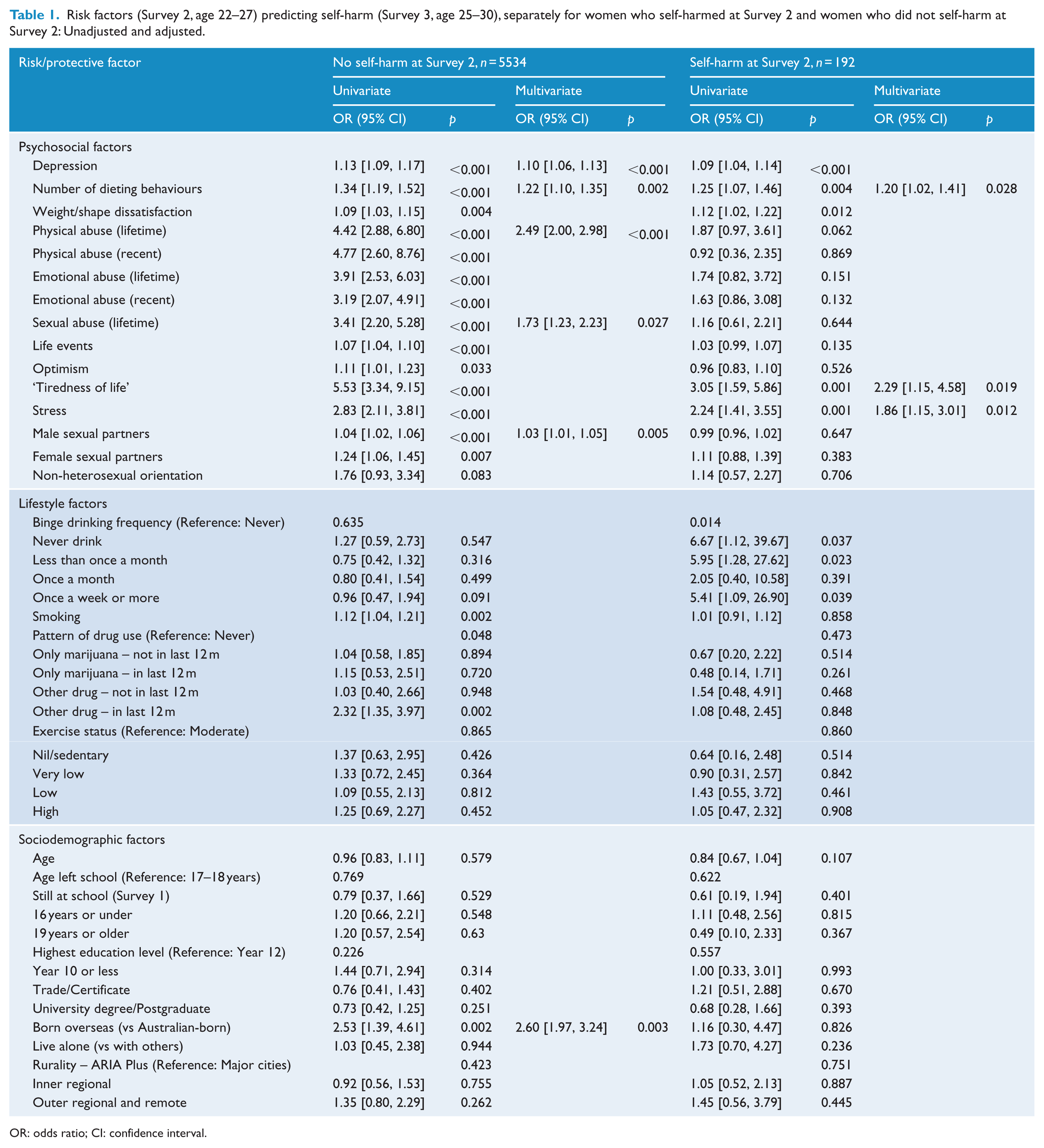
OR: odds ratio; CI: confidence interval.
Analysis
To fulfil the first aim regarding antecedent factors, unconditional logistic regression was used to determine risk and protective factors (as measured at Surveys 1 and 2) that predict self-harm 3 years later (at Survey 3), in two separate analyses based on self-harm status at Survey 2. These results were reported as odds ratios (ORs) with 95% confidence intervals (CIs). This set of antecedent factors was reduced using multiple logistic regression; ORs were reported. To fulfil the second aim regarding outcomes, univariate regression was used to determine outcomes (as measured at Surveys 4 and 5) for self-harm (at Survey 3), reported as ORs. Insight into which outcomes were independently associated with self-harm was obtained using multiple logistic regression with backward elimination, reported as ORs. To achieve this, the outcomes were entered as predictor variables for the dependent variable self-harm. For univariate analyses, missing values were not imputed – results are reported for the available cases, due to very low rates of missing values per variable. For multivariable analyses, despite the low rate of missing values per variable, the total proportion of cases would be quite high (69.6%) as this accumulates across all dependent and independent variables. We used multiple imputation to fit individual logistic models with five multiply imputed datasets. We used linear regression for ordinal/numeric variables and binary logistic regression for dichotomous outcomes. Statistically significant independent subsets of predictive and outcome variables were identified via backward elimination, sequentially removing the variable with the highest significance until all variables were statistically significant at the 0.05 level. Analyses were performed using SPSS.
Results
Sample overview
Of those invited to the survey, 42% responded and 14,247 completed the first survey in 1996 at age 18–23. Our analysis includes the follow-up Surveys 2–5 conducted in 2000 (n = 9688), 2003 (n = 7790), 2006 (n = 6940) and finishing in 2009 at age 31–36 (n = 5790). We analysed data collected from 5765 women who completed all five surveys and answered the self-harm question at Survey 3. Based on comparison with 1996 census data, the initial sample was considered broadly representative of the Australian population of women in this age group, although there was some overrepresentation of women with tertiary education and underrepresentation of some groups of immigrant women (Brown et al., 1999). Retention rates varied between 61% and 69% for each of Surveys 2–5, which is comparable to other surveys in this age group, given the mobility and changing nature of this demographic (Lee et al., 2005). The main reason for non-response was that researchers were unable to contact the participant, accounting for 21–28% of attrition for Surveys 2–5 (Lee et al., 2005). A review of the impact of attrition found that although consistent responders reported better general health and mental health compared with intermittent responders, attrition did not appear to bias the relationships between study variables (Powers and Loxton, 2010). The risk of bias due to missing responses was quite low given low rates of missing data; the highest was 3% (see Tables 1 and 2).
Self-harm (Survey 3, age 25–30) predicting outcomes 3 and 6 years later (Survey 4, age 28–33 and Survey 5, age 31–36): Unadjusted and adjusted.
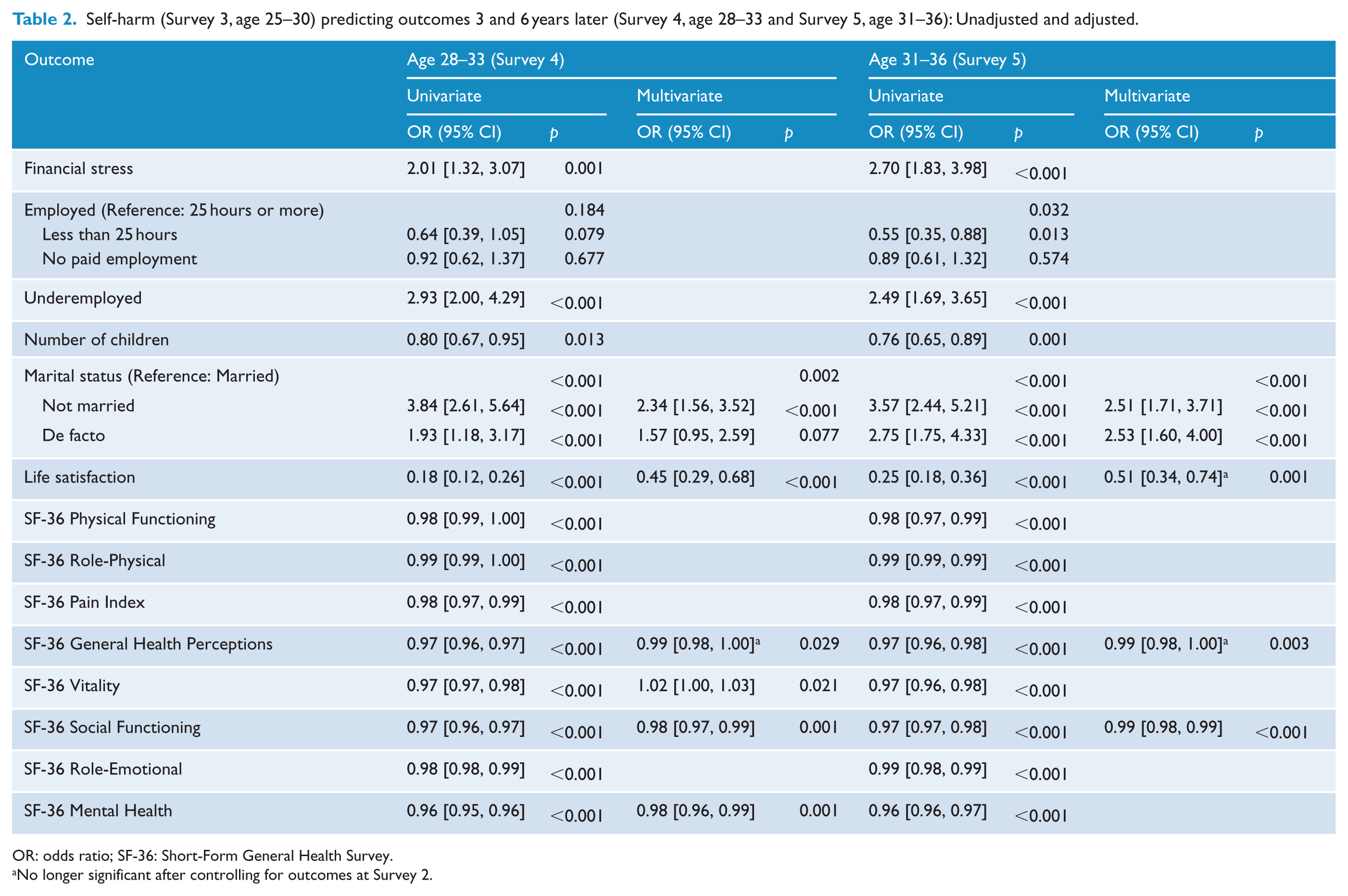
OR: odds ratio; SF-36: Short-Form General Health Survey.
No longer significant after controlling for outcomes at Survey 2.
Self-harm prevalence and continuation
Self-harm in the last 6 months was reported by 192 (2.5%) young women in Survey 3 (age 25–30) and was slightly lower in future waves (1.7% at Survey 4 and 2.0% at Survey 5). Women who reported self-harming at Survey 3 were more likely to report self-harm in later surveys compared with women who did not report self-harm in Survey 3 (Survey 4: 27.3% vs 1.1%; Survey 5: 24.6% vs 1.4%). Self-harm rates did not vary according to participants’ age (see multivariate analysis, Table 1).
Antecedents of self-harm
As expected, it was possible to predict self-harm at Survey 3 (age 25–30) using a range of factors measured at Survey 2 (age 22–27), analysed separately for women who reported self-harm at Survey 2 and women who did not report self-harm at Survey 2 (see Table 1). First, we consider the predictors for self-harm among women who did not report self-harm at Survey 2, which was the majority of the sample (n = 5534). Across all categories of antecedent factors, many factors predicted self-harm at Survey 3 when considered in isolation, but were represented by a smaller set of factors in the reduced model which considers predictors simultaneously. For example, while the strongest predictor of self-harm univariately was ‘tiredness of life’ (OR: 5.53; 95% CI: [3.34, 9.15]), this was no longer statistically significant after controlling for other factors such as depression, abuse, and stress. Independent predictors of self-harm centred around lifetime physical and sexual abuse, higher depressive symptoms, number of dieting behaviours, number of male sexual partners, and being born overseas.
Next, we consider self-harm predictors among the smaller subset of women who reported self-harm at Survey 2 (n = 192). The statistical power available in this subset is lower than for the prior self-harmers due to a combination of smaller total number and reduced prevalence of self-harm at Survey 3. Despite this, we were able to identify a number of univariate predictors of self-harm including several statistically independent predictors. Notable univariate predictors were ‘tiredness of life’ (OR: 2.29, 95% CI: [1.15, 4.58]), stress and number of dieting behaviours. These three predictors remain statistically significant in the multivariate model, indicating that they provide statistically independent discrimination between women who self-harm at Survey 3 and those who do not.
Outcomes following self-harm
Women who reported self-harm at Survey 3 (age 25–30) reported poorer outcomes at the 3-year follow-up, the majority of which persisted to the 6-year follow-up (Table 2). Many outcomes were related to self-harm in the univariate analysis that did not remain significant after controlling for all other outcomes, suggesting a complex pattern of correlations between outcomes that are not statistically independent. Thus, the reduced model offers clarity in interpreting the results, and highlights the need for broad variable sets because any one measure may not provide adequate representation of the broader constructs which are impacted by self-harm. Women who self-harmed were less likely to be married and were more likely to report that physical and emotional problems impacted on their social activities. Another notable outcome that was evident at both follow-ups was lower life satisfaction among women who self-harmed (Survey 4 – OR: 0.45; 95% CI: [0.29, 0.68]). To alleviate the concern that these outcomes preceded self-harm, we re-ran the final model controlling for these outcomes at Survey 2. Most factors remained significant (see Table 2), particularly the relational outcomes that persisted in the 6-year follow-up. Women who reported self-harming reported poorer general health at both follow-ups; however, this finding was no longer significant after controlling for outcomes at Survey 2, and life satisfaction at Survey 5 also lost significance.
Discussion
In our large, representative sample of Australian women aged 25–30, 2.5% reported engaging in self-harm in the last 6 months. This is comparable to rates reported in other community samples (Young et al., 2006). Any estimate of self-harm rates relies on self-report, and it is possible that the true occurrence of self-harm is higher (Fergusson et al., 2000). This may be due to social desirability bias, or poor memory recall (Armiento et al., 2014). These prevalence rates fit the general picture of self-harm across the lifespan from adolescence through to adulthood: the average onset of self-harm is age 12–14 (Jacobson and Gould, 2007), and most adolescent self-harm resolves spontaneously during or after the teenage years (Moran et al., 2012). Yet, for a proportion of those who self-harm during adolescence, self-harm continues into adulthood (Mars et al., 2014), particularly for females (Nkansah-Amankra, 2013). Indeed, there may be new cases of self-harm in early adulthood; in a college sample, Whitlock et al. (2006) found that 38.6% reported initiating self-harm at age 17–24.
Understanding the predictive factors for self-harm can inform prevention strategies in the community. Clinicians and health professionals can benefit from an increased awareness of the predictive factors which may serve as warning flags for current or future self-harm. Self-harm at age 25–30 was predicted by a number of factors measured 3 years earlier, including psychosocial factors (depression, dieting behaviours, ‘tiredness of life’ and stress) and abuse (physical and sexual). The link between these factors and self-harm has been well established in prior research (e.g. Wichstrøm and Hegna, 2003; Whitlock et al., 2006). While causality cannot be inferred, their antecedence and the large, representative nature of this sample strengthen these findings. We also note that although depression is identified as a significant predictor of self-harm, the magnitude of the relationship is modest compared with other predictive factors, as consistently found in prior research (Dupéré et al., 2009; Wichstrøm and Hegna, 2003). A notable predictive factor among women who did not report self-harm at Survey 2 was lifetime physical abuse: young women who disclosed physical abuse were over twice as likely to report self-harm. Our large community sample, broad range of factors and longitudinal design add clarity to the mixed findings surrounding physical abuse in prior self-harm research, which has primarily used cross-sectional designs (e.g. significant findings: Hahm et al., 2010; non-significant findings: Gratz et al., 2002; Whitlock et al., 2006). Sexual abuse was also predictive of self-harm, as found in prior work (Gratz et al., 2002; Hahm et al., 2010; Whitlock et al., 2006). Therefore, professionals in medical, mental health and forensic settings should consider screening for self-harm when a woman discloses abuse, even when there are no signs of self-harm evident. Other factors that may serve as warning flags for future self-harm among women who are not currently self-harming are depression, engaging in multiple dieting behaviours and a high number of male sexual partners.
While past self-harm research in community samples often focuses on risk factors for self-harm in the whole sample, a focused examination of risk factors in women with current or recent self-harm elicits findings that are useful for intervention. Among women who reported self-harm at Survey 2, the key predictors of future self-harm were number of dieting behaviours, tiredness of life and stress. These factors may be useful in clinical settings when working with identified self-harmers as indicators of future self-harm risk. ‘Tiredness of life’ has been associated with self-harm in prior research and has been considered a suicide-related cognitive construct that is earlier on a spectrum of suicidal behaviour (Aschan et al., 2013; Bebbington et al., 2010). Screening measures in medical and mental health settings should include ‘tiredness of life’ to flag the risk for self-harm behaviour. Higher stress scores were predictive of continued self-harm in this group. In treatment, women who engage in self-harm may need assistance with skills to cope with overwhelming emotions and a range of co-occurring psychosocial factors and life experiences (Chapman et al., 2006). Engaging in multiple dieting behaviours was the one predictor that was consistent across women with and without recent self-harm. This may reflect common cognitive pathways that underlie self-harm and disordered eating behaviours, such as reduced sense of self-worth, self-punishing behaviours or maladaptive coping strategies. This overlap can be conceptualised as a continuum of self-destructive behaviour (Holinger and Klemen, 1979). We also note the absence of some of the predictors for self-harm that are commonly cited in prior literature, such as depression and abuse.
These results concur broadly with nascent literature attempting to understand self-harm cessation and maintenance. Cessation has been linked with an improved ability to regulate emotion, developing positive coping behaviours, increased self-awareness and support from others (Whitlock et al., 2015). The predictors for continuing self-harm in this study may reflect deficits in these areas of skills, support and cognitive patterns.
This study offers new insight into the long-term outcomes up to 6 years after self-harm, offering insight for community and clinical settings. Women who self-harmed reported greater difficulties in relationships: they were less likely to be married and were more likely to report that physical and emotional problems limited their social activities. The association between self-harm and difficulty with relationships was observed as far ahead as 6 years. The lower life satisfaction may reflect objective differences in circumstances, or may indicate difficulties in processing negative events and experiences (such as working memory deficits; Fikke et al., 2011), or a combination of both. Women who have self-harmed may need assistance in building social support networks, developing and maintaining romantic relationships, and strategies to improve life satisfaction. These findings raise awareness of the long-term impact of self-harm, and the need for ongoing support. Clinically, these are important factors to consider in preparation for discharge, particularly in brief treatment settings that will not offer long-term support. Given that many who self-harm will not seek help, we also need strategies at the community level: for example, improving mental health literacy through schools, workplaces and advertising campaigns, to reduce the stigma surrounding self-harm and encouraging people to seek help. This needs to be supported by adequate funding to provide effective support through crisis-call lines and chat services, and web programs.
This study had several strengths. First, we used a large, representative community sample. Second, we used a broad range of factors and a longitudinal design spanning 13 years. Third, we conducted side-by-side analyses of predictive factors for self-harm separately depending on self-harm status. Fourth, we provide evidence to confirm that women who self-harm experience poorer long-term outcomes. This study also had some limitations which warrant discussion. First, although this paper included a broad range of antecedent factors for, and outcomes of, self-harm, we were limited to the variables included in the ALSWH project. Therefore, it was not possible to include other factors that have been previously studied in relation to self-harm, such as anxiety. Second, we were also not able to examine subtleties of self-harm status, such as first onset, suicidal ideation, severity, method or frequency. Third, the present study focuses specifically on a female sample; similar research is also needed in male samples, as risk factors and outcomes may differ (e.g. Gratz et al., 2002; Kposowa, 2000). Although we present data for a significant time period, it would be useful to conduct longitudinal research in community samples over longer time spans, as the antecedent factors for, and outcomes of, self-harm may change throughout the lifespan. Differences in the timeframe for reporting on variables may have reduced the clarity of our findings.
Despite increasing awareness of the presence of self-harm in general, self-harm often remains a hidden problem (Armiento et al., 2014). Predictive factors such as depression, dieting behaviours, tiredness of life and stress can act as warning flags for current or future self-harm. Women who self-harm need ongoing support with relationships and life satisfaction, even after ceasing self-harm.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.