
Abstract
Objectives:
There is a well-established association between alcohol use, misuse, intoxication and self-harm, the latter of which is associated with suicide. This study aimed to better understand the association between proximity to alcohol outlets and the likelihood of young people presenting to hospital following self-harm.
Methods:
This was a nationwide retrospective geospatial study using data from the New Zealand Integrated Data Infrastructure using population-level data for 10–29-year-olds for the 2018 and 2017 calendar years. Presentations to hospital following self-harm were identified using the national minimum data set. Proximity to alcohol outlets was defined in road network distance (in kilometres) and ascertained using Integrated Data Infrastructure geospatial data. Alternative measures of proximity were employed in sensitivity analyses. Complete-case two-level random intercept logistic regression models were used to estimate the relationship between alcohol outlet proximity and hospital presentation for self-harm. Adjusted models included sex, age, ethnicity, area-level deprivation, urbanicity and distance to nearest medical facility. Analyses were also stratified by urbanicity.
Results:
Of the 1,285,368 individuals (mean [standard deviation] age 20.0 [5.9] years), 7944 (0.6%) were admitted to hospital for self-harm. Overall, the odds of presenting to hospital for self-harm significantly decreased as the distance from the nearest alcohol outlet increased, including in adjusted models (adjusted odds ratio 0.980; 95% confidence interval = [0.969–0.992]); the association was robust to changes in the measure of alcohol proximity. The effect direction was consistent across all categorisations of urbanicity, but only statistically significant in large urban areas and rural areas.
Conclusions:
The findings of this study show a clear association between young people’s access to alcohol outlets and presentation to hospital for self-harm and may provide a mandate for government policies and universal interventions to reduce young people’s access to alcohol outlets. Further research regarding causative mechanisms is needed.
Background
Self-harm includes all intentional acts of self-poisoning or self-injury regardless of motivation or degree of intention to die (Hawton et al., 2003b). Globally, the rate of self-harm may be as high as 400 per 100,000, and is much more common than suicide, which is estimated to affect around 15 per 100,000 (WHO, 2014) people. Self-harm is a heterogeneous condition, associated with an increased risk of suicide (Carroll et al., 2014; Liu et al., 2020).
Self-harm increases rapidly from early adolescence and peaks around age 14 to 16 (Gillies et al., 2018; Plener et al., 2015; Voss et al., 2019). In Aotearoa/New Zealand (NZ), young people represent one-quarter of those hospitalised due to self-harm (Conner et al., 2003) and intervening early with this age group is an important prevention activity. More young people than ever are presenting to hospital with self-harm since the onset of the COVID-19 pandemic (Sara et al., 2023), although rates were already increasing (Fleming et al., 2022; Gillies et al., 2018; Griffin et al., 2018b), particularly among young women. While mental health difficulties make a large contribution to the risk of self-harm (Hawton et al., 2013; Witt et al., 2019), multiple interacting factors that accumulate over the lifetime have been shown to be associated with self-harm (Beautrais, 2000; Fliege et al., 2009; Mars et al., 2014a; Serafini et al., 2015). In NZ, as in other countries where Indigenous peoples are affected by the ongoing impacts of colonisation, there are disproportionately higher rates of self-harm among Māori, the Indigenous people of NZ (Crengle et al., 2013; Ministry of Health, 2018; Theodore et al., 2022)
There is a well-established link between alcohol use, misuse, intoxication, and suicide (Crossin et al., 2022) and self-harm (Borges et al., 2017; Cherpitel et al., 2004; Haw et al., 2005; Melson and O’Connor, 2019; Rossow and Norström, 2014). A longitudinal study of a database of sentinel surveillance of self-harm in England showed that the role of alcohol use in self-harm appears to have increased over the last few decades (Ness et al., 2015). In this study, for young adults who presented to hospital with self-harm between 2000 and 2007, 50% of the self-harm acts involved alcohol and 30% of young adults presenting with self-harm were assessed as misusing alcohol. Two related studies of self-harm hospital presentations in Ireland between 2012 and 2013 showed alcohol was present in 43% of presentations (Griffin et al., 2018a) and that alcohol involvement was associated with an increased number of hospital presentations over time (Griffin et al., 2020). The relationship is bidirectional, for example, in the Avon Longitudinal Study of Parents and Children (ALSPAC), a birth cohort of children born in 1991–1992, self-harm reported at the age of 16 was associated with the rate of harmful alcohol use at 18 years (Mars et al., 2014b).
It is often assumed that individual intervention is the key to addressing self-harm, in this case addressing alcohol use and self-harm (Boden et al., 2022; Hobbs et al., 2020). However, there is limited evidence regarding the safety and efficacy of individual interventions, particularly in young people (Hawton et al., 2003a; Witt et al., 2021a, 2021b). Young people often experience difficulty accessing services through which they can receive these interventions; more so if they are Māori (Hobbs et al., 2019; Peiris-John et al., 2020; Theodore et al., 2022) and these services may not meet their needs. Furthermore, individual treatment does not take into account social or structural determinants (e.g. social security, access to housing, regulation and policy, colonisation, discrimination) that underpin these issues. In addition to individual interventions, whole of population approaches are needed to address alcohol use and self-harm (Barrett et al., 2018; Hawton et al., 2016; Rouen et al., 2019; Steeg et al., 2020).
Recent reviews have demonstrated that whole of population approaches to alcohol control may confer benefits, particularly for men, young people and Indigenous populations (Kõlves et al., 2020). In line with Rose’s paradox, because alcohol use is relatively common in the population, interventions to reduce alcohol use at the population level are likely to have greater impact on rates of self-harm (including across the socioeconomic gradient) than interventions targeting a smaller number of individuals at a higher level of risk (Rajput et al., 2019; Rose, 1992). Furthermore, addressing a major social and structural health determinant such as alcohol use is likely to have benefits beyond self-harm and suicide prevention. For example, alcohol use is associated with many social harms and poor health outcomes such as increased risk for cancer (Rumgay et al., 2021). It is also estimated to contribute to an increased risk of mortality (around 800 deaths per year and the leading cause of death in 15–49-year-olds) and to cost society approximately NZ$7.85 billion per year (Connor et al., 2015; Nana, 2018).
In NZ, particular groups bear a disproportionate burden of the negative environmental consequences resulting from industrial, governmental and commercial operations or policies (Mennis et al., 2016). The distribution of and access to alcohol outlets is not equitable; alcohol outlets are more often located within more deprived areas of NZ (Cameron et al., 2016; Hay et al., 2009; Hobbs et al., 2020; Pearce et al., 2008a), and proximity to alcohol outlets is associated with increased hazardous drinking and criminal behaviour (Day et al., 2012; Hobbs et al., 2020). International literature supports this finding, suggesting that inequities in environmental factors may be associated with increased risks of substance misuse, thus contributing to observed health disparities in rates of substance use disorders (Mennis et al., 2016). Therefore, there are increased risks of alcohol-related harm among populations who are already disproportionately negatively affected by a range of issues associated with where they live and what is available in their neighbourhood, including alcohol.
Persistent inequities in health outcomes, morbidity and mortality also exist between urban and rural regions of NZ (Edmondston and Maskill, 1989; Marek et al., 2020). Research dating back as far as the 1980s has shown spatial variations in health outcomes for small towns in NZ, for example having higher mortality than larger urban areas (Edmondston and Maskill, 1989; Fraser, 2006; Ministry of Health, 2007; Pearce et al., 2008b). A more recent NZ study showed that an increase in licenced clubs was significantly associated with violence in areas with smaller populations but not in areas with larger populations (Cameron et al., 2016). While studies have typically failed to address the full spectrum of urbanicity by opting for a dichotomy of urban–rural, more recent studies have highlighted nuanced findings showing higher adverse health outcomes in minor urban areas compared with main urban or rural areas across nearly all outcomes (Marek et al., 2020). It is therefore also plausible that the strength of any association that may exist between proximity to alcohol outlets and self-harm might be moderated by the degree of rurality or urbanicity in an area (Marek et al., 2020). There has been relatively little research and mixed findings about the impact of rurality or urbanicity on self-harm in NZ (Beautrais, 2018; Whigham et al., 2016). Most studies of self-harm in NZ are now out of date and have been conducted in specific settings, such as hospitals and outpatient settings (Fortune, 2006; Fortune et al., 2007; Hatcher et al., 2009), with particular groups such as farmers (Beautrais, 2018), elderly (Cheung et al., 2017) or school students (Fleming et al., 2022), or with particular ethnicities such as Pacific (Tiatia-Seath et al., 2017), rather than across settings.
Epidemiological analyses inform what interventions can be delivered at scale, and are likely to effectively reduce the adverse impact of the social and structural determinants of health (Satcher and Higginbotham, 2008; Solar and Irwin, 2010). Considering the limitations of previous evidence, the aim of this study was to understand the association between the distribution of, and access to alcohol outlets, and presentations to hospital following self-harm among young people nationwide and how this association differs by level of urbanicity.
Methods
Study design, participants and settings
This was a nationwide retrospective geospatial study using data from the Integrated Data Infrastructure (IDI), a large repository containing linked administrative and survey data curated by Stats NZ – Tatauranga Aotearoa (Stats NZ) for the purposes of research for the public good (Milne et al., 2019), and geospatial data on proximity to alcohol outlets (see the section ‘Alcohol outlet proximity’ below). Data within the IDI are linked by Stats NZ using an established linking methodology (Statistics New Zealand, 2014). This method uses a unique identifier for each individual determined from information including first name, last name, sex and date of birth.
The study population was the NZ estimated resident population (ERP) of 10–29-year-olds for the 2018 calendar year. The 2017 and 2018 calendar years were chosen to align with the timing of the collection of geospatial data on location of alcohol outlets. This population was determined using an established IDI-based method for identifying the NZ ERP and constructs a population that is within 2% of the official NZ ERP (Gibb et al., 2016). Individuals were included in the IDI-ERP when there was evidence they had activity within key government services such as health, education and tax (Marek et al., 2021). This population was restricted to individuals alive and living in NZ, as on 31 December 2018.
Self-harm
Self-harm was identified using hospitalisation data (the national minimum data set [NMDS]), a national collection of all publicly funded hospital admissions in NZ hospitals (Bowden et al., 2020). Hospitalisation is inclusive of all those admitted to hospital including day patients (over 3 hours but not overnight) as well as emergency department visits of greater than 3 hours. Self-harm was indicated if an individual presented to hospital at least once in the 2017 and 2018 calendar year with an ICD-10-AM diagnosis Intentional Self-Harm code (X60-X84 or Y870), which include self-inflicted poisoning and injury via various methods.
Alcohol outlet proximity
Distribution and access to alcohol outlets was operationalised as proximity to alcohol outlets and ascertained by linking the residential address of each individual as on 31 December 2018, determined using data from the IDI address notification table, to geospatial alcohol outlet information. Data were linked at the 2018 meshblock level, a small area unit reflecting neighbourhoods of approximately 60–120 residents (Statistics New Zealand, 2019). This included both on- and off-licence premises; on-licence includes, for example, pubs, restaurants, cafes, bars, entertainment venues and allows for the sale and consumption of alcohol on the premises; off-licence includes, for example, bottle shops and supermarkets and allows for the sale or supply of alcohol for consumption off the premises. The primary measure of alcohol outlet proximity used was the road distance (in kilometres [km]) from the centre of the population-weighted neighbourhood that the individual resides to the nearest alcohol outlet. Alternative measures employed in sensitivity analyses included: median distance (km) on the road to nearest five alcohol outlets; driving time (in minutes) to nearest outlet, median driving time (in minutes) to nearest five outlets, distance (km) to nearest on-licence alcohol outlet and distance (km) to nearest off-licence alcohol outlet.
Sociodemographic measures
Sex (male/female), age (10–14, 15–19, 20–24, 25–29 years) and ethnicity were drawn from the IDI personal details table. Within the IDI, data on sex uses the current statistical standard that typically asks individuals whether they are male or female, without the terms gender or sex used in the question. In 2021, Stats NZ released a revised standard for sex and for gender identity to address issues including limited inclusiveness of intersex and transgender populations. However, for this study, we were restricted to existing administrative data for 2018 (female/male). Ethnicity measurement employed the total concept approach, which means that individuals can identify with more than one ethnic group. The NZ Standard Classification 2005 V2.0.0 of major ethnic groups was used: European, Māori, Pacific peoples (Pasifika), Asian and Middle Eastern, Latin American, African (MELAA), Other. Due to small numbers in the Other group, European and Other were combined into a composite group, European/Other (EO).
The level of socioeconomic deprivation, defined by the NZ Deprivation Index 2018 (NZDep2018; Atkinson et al., 2019), and the urbanicity of residence were both established based on 2018 meshblock of residence. NZDep2018 establishes a deprivation score assigned to each meshblock. These scores were then collapsed into quintiles, 1 (least deprived) to 5 (most deprived). Urbanicity was defined by the Urban Rural Indicator 2018 (Statistics New Zealand, 2019, 2020) that was collapsed into five categories representing: major urban areas (populations of 100,000 or more); large urban areas (30,000–99,999); medium urban areas (10,000–29,999); small urban areas and rural areas (< 1,000). These time varying measures (age, NZDep2018, and urbanicity) were determined as at 31 December 2018.
Distance to nearest medical facility
Because the outcome of interest was hospital presentation for self-harm, we wanted to account for the potential impact that distance to a medical facility might have on the analyses. Distance to the nearest medical facility was sourced from the IDI sample, which included 79 medical facilities (including large hospitals, small and community-based hospitals and mental health inpatient units). We geocoded all relevant medical facilities and, for the IDI sample, calculated the distance from the participants population-weighted centroid of the 2018 meshblock to the nearest facility.
Procedure
Data were extracted using SAS 8.3 and analysed using Stata MP version 16.1. Stats NZ confidentiality requirements were adhered to including randomly rounding all count data to base three and suppressing any counts less than six. Analyses and reporting of data were informed by the Reporting of Studies Conducted using Observational Routinely collected health Data (RECORD; Benchimol et al., 2015).
Statistical analyses
The sociodemographic characteristics of the study population and observed distances to alcohol outlets were presented descriptively, stratified by self-harm status. Complete-case two-level random intercept logistic regression models with individuals nested within District Health Boards (geographic health administration catchments in NZ as in 2018) were used to estimate the relationship between alcohol outlet proximity and hospital presentation for self-harm. Adjusted models included sex, age, ethnicity, NZDep2018, urbanicity and distance to nearest medical facility as covariates. Analyses stratified by urbanicity were also conducted. Two-tailed tests were at the 5% level defined significance.
Sensitivity analyses were conducted to estimate the relationship between self-harm and the alternative measures of alcohol outlet proximity described in the section ‘Alcohol outlet proximity’.
Ethics
This study was approved by the University of Otago Human Research Ethics Committee (reference: HD17/004) and was reviewed as a ‘Minimal Risk Health Research – Audit and Audit related studies’ proposal. Stats NZ approved access to the IDI. Informed consent from participants was not deemed necessary according to national legislation, i.e. the Statistics Act (1975).
Results
The 2017/2018 ERP of 10–29-year-olds contained 1,285,368 individuals (mean [SD] age 20.0 [5.9] years) of whom 7,944 (0.6%) presented to hospital for self-harm (mean [SD] age 20.6 [4.1] years). Table 1 displays the sociodemographic characteristics of the participant population, stratified by self-harm status. Compared to those who did not present to hospital for self-harm, those who did were more likely to be female (70.4% vs 48.3%), aged 15–19 and 20–24 years (40.1% vs 23.1% and 35.5% vs 24.2%, respectively), and be EO (78.3% vs 65.9%) or Māori (33.9% vs 23.2%) ethnicity. They were also more likely to live in areas of high deprivation (28.8% vs 24.3%). Differences in urbanicity of residence and distance to nearest medical facility were marginal.
Sociodemographic characteristics of the participant population (N = 1,285,368), by self-harm status.
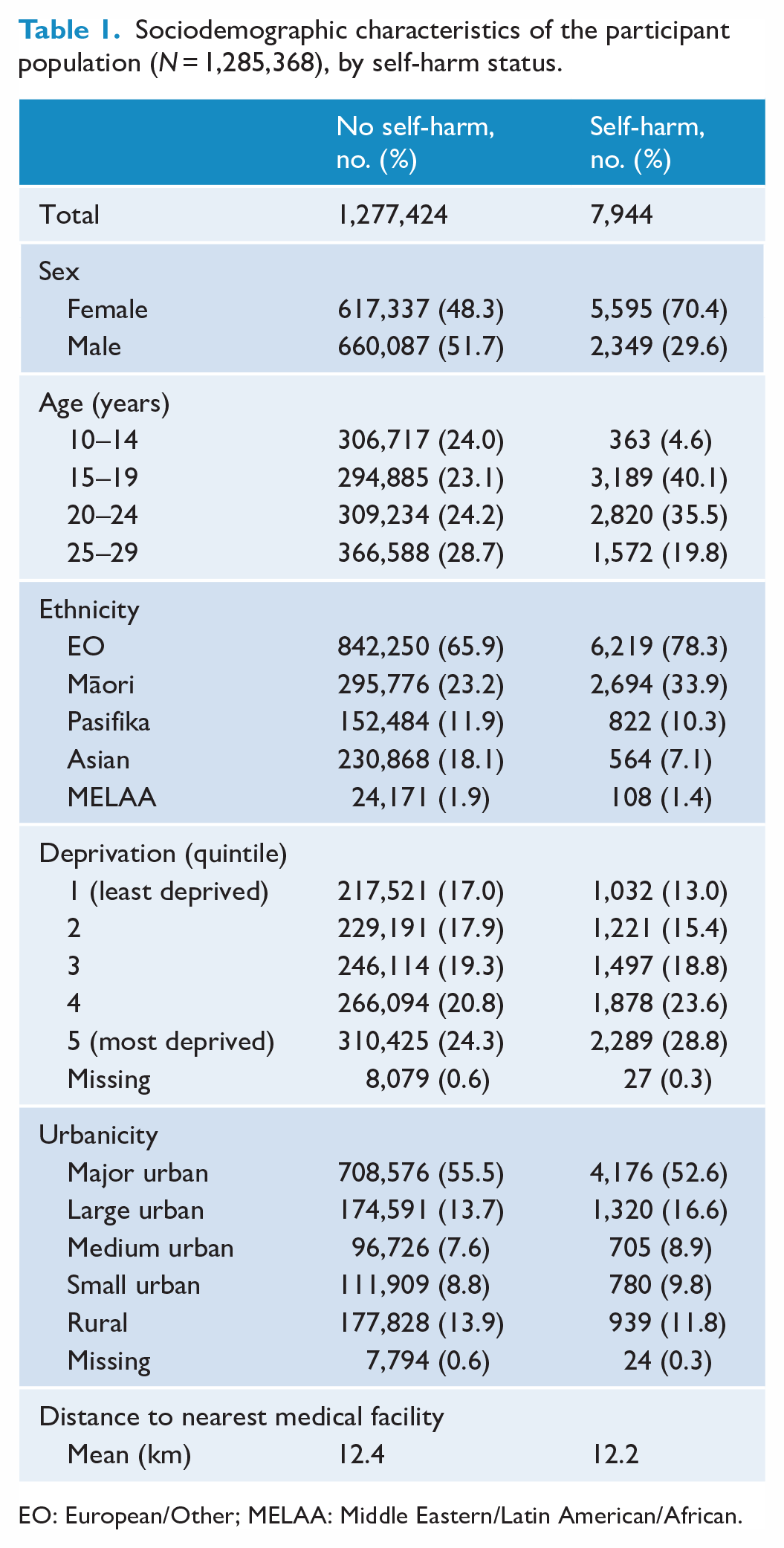
EO: European/Other; MELAA: Middle Eastern/Latin American/African.
Observed differences in distance to nearest alcohol outlets stratified by self-harm status are presented in Table 2. The mean distance to the nearest alcohol outlet was lower for those who had engaged self-harm (1.28 km) compared to those who did not self-harm (1.46 km). Observed distances to the nearest alcohol outlet by level of urbanicity were all lower for those who had presented to hospital for self-harm; however, those differences were greatest for those living in large urban areas, medium urban areas and rural areas.
Distance (in km) to nearest alcohol outlet, overall and by urbanicity of residence, stratified by self-harm status.
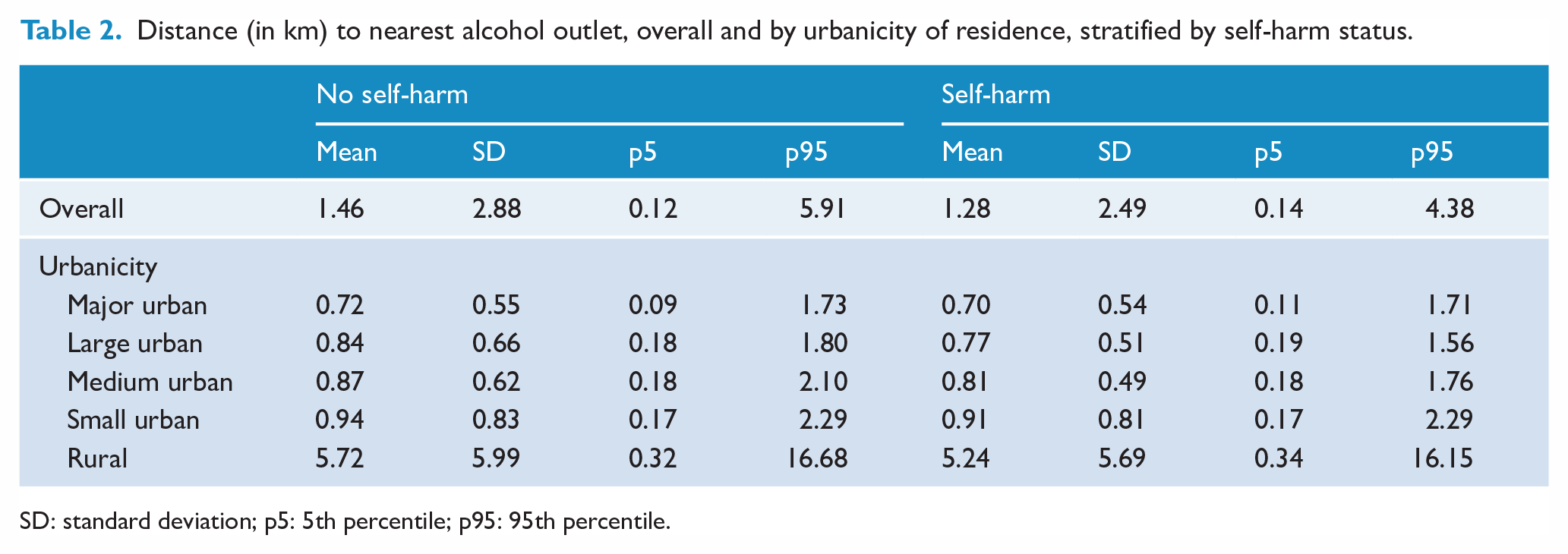
SD: standard deviation; p5: 5th percentile; p95: 95th percentile.
Figure 1 displays the adjusted odds ratios (aOR) of self-harm status (and associated 95% confidence intervals [CIs]) on distance (in km) to nearest alcohol outlet. After adjustment for sociodemographic factors and distance to nearest medical facility, the odds of presenting to hospital for self-harm significantly reduced the further the individual lived from the nearest alcohol outlet (aOR 0.980; 95% CI = [0.969 – 0.992]; see Table 3 in the Appendix for details). Similarly, analyses stratified by urbanicity indicated associations of the same direction exist across all urban/rural categorisations; however, effect sizes differed substantially (from aOR 0.996; 95% CI = [0.937 – 1.058] for major urban areas to aOR 0.872; 95% CI = [0.785 – 0.969] for large urban areas). Moreover, only the aORs for large urban and rural areas were found to be statistically significant (see Tables 4–8 in the Appendix for details).
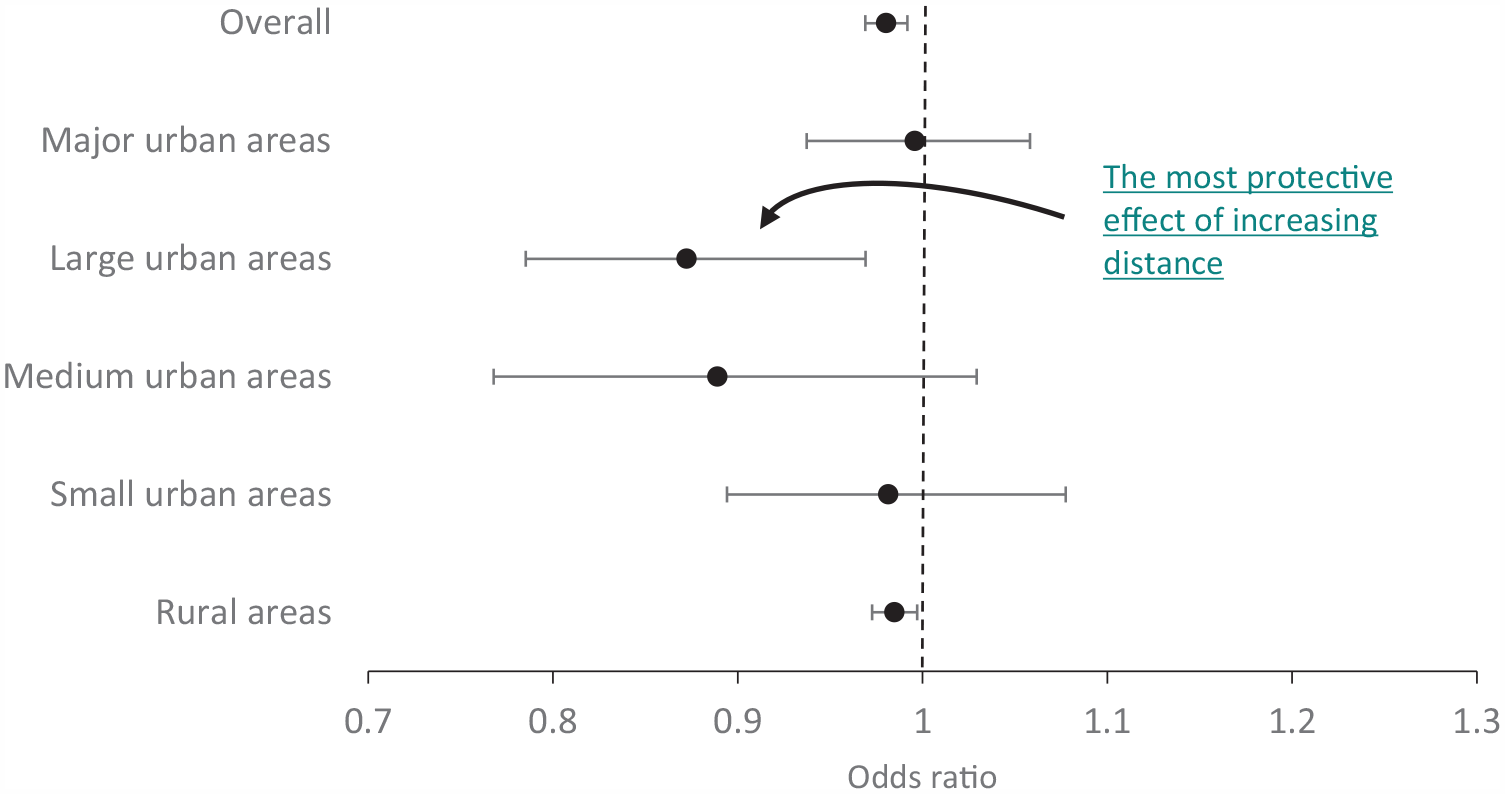
Adjusted odds ratios for the relationship between increasing distance (in km) to the nearest alcohol outlet and odds of hospitalisation for self-harm, overall and stratified by urbanicity.
Comprehensive sensitivity analyses exploring alternative measures of distance (and time) to alcohol outlets revealed only marginal differences from the primary results above (see Tables 9–13 in the Appendix for details). This included analysis of median distance (in km) to nearest five outlets, driving time (in minutes) to nearest outlet, median driving time (in minutes) to nearest five outlets, distance (in km) to nearest off-licence outlet, and distance (in km) to the nearest on-licence outlet.
Discussion
Key findings
Using nationwide NZ population-level data for young people aged 10 to 29, we explored the association between residential proximity to alcohol outlets and presentation to hospital due to self-harm. We aimed to inform universal interventions to limit access to, and use of alcohol to prevent self-harm at a population level. Analyses revealed an association between distance to nearest alcohol outlet and self-harm hospital presentation, indicating the odds of a self-harm hospital presentation significantly decreased as the distance from the nearest alcohol outlet increased. This effect persisted after controlling for sex, age, ethnicity, deprivation, urbanicity of residence and distance to the nearest medical facility. Sensitivity analyses revealed that this finding was robust to changes in the measure of alcohol proximity and was evident for both on-licence and off-licence alcohol outlets. In stratified analyses, the effect direction was consistent across all urbanicity categorisations, but was only statistically significant in large urban areas with populations of 30,000–99,999 and in rural areas with population < 1,000.
Findings in relation to other studies
Our study builds on the existing literature that highlights the link between adverse outcomes and social harm and proximity to alcohol outlets (Boden et al., 2022; Hobbs et al., 2020; Zhang et al., 2015). Our findings, which are situated within a public health framework, highlight an association between a key systemic environmental factor, proximity to an alcohol outlet and hospital presentations for self-harm, adding to the range of adverse outcomes that have already been associated with proximity to alcohol outlets. There is a well-established link between alcohol use and self-harm (Borges et al., 2017; Cherpitel et al., 2004; Haw et al., 2005; Melson and O’Connor, 2019; Rossow and Norström, 2014), but this is the first study to show an association between proximity to alcohol outlets and hospital presentation for self-harm. Our findings, along with theory, and some emerging evidence that greater accessibility to alcohol results in greater consumption (Auchincloss et al., 2022; Young et al., 2013), leading to greater alcohol-related harm including self-harm, indicate that proximity to an alcohol outlet represents a modifiable risk factor. The body of evidence, including our study, highlights the need for urgent action in the form of universal public health interventions to reduce access to alcohol outlets, for example, via licencing regulation (Boden et al., 2022). There are good examples of modest reductions in alcohol outlet density being associated with reduction in violent crime (Zhang et al., 2015). A recent systematic review indicates that a universal public approach can be successful in reducing self-harm and suicide (Kõlves et al., 2020).
There are important and novel nuances to our findings. In analyses accounting for the full spectrum of urbanicity, as opposed to just urban or rural categorisation as is often carried out in previous research, the significant association between distance to nearest alcohol outlet and self-harm hospital presentation only held in large urban and rural areas. Interestingly, effect sizes were comparatively larger for the large and medium urban areas and small for the rural areas. The small effect size found for rural areas is perhaps understandable in the context of the already large distances that those residing in rural areas need to travel to access goods and services. In this study, the average distance was ~6 km in rural areas, so an extra 1 km is an extra ~15% distance, whereas the average distance for all urban areas was < 1 km, so an extra 1 km is more than double the distance to travel. Nevertheless, this variation seen across the full spectrum of urbanicity classification echoes similar findings, albeit about health generally (Edmondston and Maskill, 1989; Marek et al., 2020).
This highlights the importance of understanding local context and factors that might modify the association between proximity to alcohol outlets and alcohol-related harm, particularly when considering what intervention(s) is required. A recent review examining the relationship between urban living and suicide, self-harm and suicidal thinking suggested a range of urban environmental features that should be considered, such as aspects of the built environment, ethnic diversity, SES, social fragmentation, crime (Satherley et al., 2022). Other factors to consider include the type of education, employment and industry available, access to healthcare, infrastructure, access to lifestyle and leisure activities, housing quality, particularly in areas that are not close to a major urban area, all of which influence the type of population that is retained in or moves to smaller urban and rural areas (Marek et al., 2020). Stigma associated with seeking help for mental health difficulties will have an impact on the risk of self-harm (Stewart et al., 2015). Differences in populations across and within different areas in terms of gender and age, poverty and unemployment or underemployment, factors associated with the risk of self-harm as highlighted in the findings of this paper, are important to consider (Edmondston and Maskill, 1989; Geulayov et al., 2022). Of note are our findings with regard to age, which are in line with evidence about the onset and magnitude of the prevalence of self-harm in young people (Gillies et al., 2018) and highlight the need for attention for those aged 15 to 24.
Strengths and limitations
This study used national population-level data (the IDI) that enabled a large sample, including identification of almost 8,000 individuals who presented to hospital for self-harm. This large sample enabled analysis stratified by urbanicity. Moreover, IDI data include linked temporal residence information, which in turn permits linking of alcohol outlet proximity data. In addition, the IDI contains sociodemographic information such as ethnicity that draws on multiple data sources that are of higher quality than would otherwise be possible via stand-alone administrative data sets. While we controlled for a range of factors, there may still be residual confounding, for example, we did not control for familial factors such as parental education, mental illness or alcohol use or numbers living in household nor other aspects of the environment that might be important. We were unable to control for mental health difficulties as it is difficult to get population-level data about this, but we do know that, for example, personality disorder and mood disorders are important modifiable risk factors for self-harm in young people (Witt et al., 2019). From a public health perspective, social and structural determinants are key, and proximity to alcohol outlet clusters with other pernicious environmental exposures like gambling outlets and, therefore, our exposure variable likely captures other aspects of the environment, which we have shown to be related to mental health outcomes, including self-harm, in young people (Hobbs et al., 2023).
This analysis is based on hospital presentation data, and this is the visible but smaller part of a much larger problem, with less than one in eight episodes of self-harm resulting in presentation to hospital (Hawton et al., 2002, 2012), and events of less than 3 hours not included in the definition of a hospital presentation. We did not have police or ambulance call-out data for self-harm, nor community-level data regarding self-harm and how this relates to proximity to alcohol outlets. Finally, given the legal age for drinking alcohol in New Zealand is 18 and over, further research is needed to understand the association between proximity to alcohol outlets and self-harm presentation in the 15- to 19-year-old group, who despite being underage may still be accessing alcohol or may be impacted by the harms associated with the adults around them drinking (Huckle and Romeo, 2022; Rossow and Moan, 2012).
Conclusion
Closer proximity to alcohol outlets was associated with an increased risk of hospital presentation for self-harm. This effect remained after controlling for sex, age, ethnicity and deprivation and remained in sensitivity analyses of different proximity metrics. Previous research has shown the potential for universal public health and policy initiatives to impact on alcohol related harm, highlighting alcohol outlet density as a modifiable risk factor (Fone et al., 2016; Zhang et al., 2015), which may provide a mandate for government policies and universal interventions to reduce young people’s access to alcohol outlets. Research is now needed to provide causal evidence of an association.
Supplemental Material
sj-docx-1-anp-10.1177_00048674231203909 – Supplemental material for Proximity of alcohol outlets and presentation to hospital by young people after self-harm: A retrospective geospatial study using the integrated data infrastructure
Supplemental material, sj-docx-1-anp-10.1177_00048674231203909 for Proximity of alcohol outlets and presentation to hospital by young people after self-harm: A retrospective geospatial study using the integrated data infrastructure by Sarah E Hetrick, Matthew Hobbs, Sarah Fortune, Lukas Marek, Jesse Wiki, Joseph M Boden, Reremoana Theodore, Troy Ruhe, Jesse J Kokaua, Hiran Thabrew, Barry Milne and Nicholas Bowden in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
We would like to thank Statistics New Zealand for access to the Integrated Data Infrastructure data and to the Statistics New Zealand Data Lab staff for their thorough checking of our results.
Disclaimer
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by A Better Start – National Science Challenge, New Zealand Ministry for Business, Innovation and Employment (grant no. UOAX1511) and A Better Start/Cure Kids 2021 research grant [Reference: Bowden 2021MRP-006].
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.