
Abstract
Objective:
To analyse the average treatment duration with antidepressants that are reimbursed for concession card holders under the Pharmaceutical Benefits Scheme in Australia.
Method:
This pharmacoepidemiological study was based on a representative 10% sample of patients receiving Pharmaceutical Benefits Scheme prescriptions. Antidepressants redeemed by concession card holders in the period from 2010 to 2013 were analysed. A 5-year baseline period was used to exclude prevalent users from incident users. Estimation of treatment duration was based on the epidemiological equation: prevalence/incidence = average duration. The mean value for prevalence and incidence over the studied period was used in the equation.
Results:
The number of prevalent and incident users increased from 90,475 to 103,305 and from 25,006 to 26,289, respectively. The epidemiological average treatment duration in the period was about 4 years. When considered by age-bands, average treatment duration was 2 years in patients under 24 years, 3 years in patients 35 to 44 years and up to 5 years in the 55 to 64 year age group. Of new users of antidepressants reimbursed under the Pharmaceutical Benefits Scheme, 86% received their first prescription from general practitioners, 4.3% from psychiatrists and 9.7% from other physicians.
Conclusion:
While recommendations have underlined the importance of giving antidepressants for a sufficient period of time, the results from this study show that it is as important to remind general practitioners to review patients on antidepressant treatment regularly, and try to cease drug treatment when timely.
Introduction
Depression, measured by disability-adjusted life years, was the fourth leading cause of global burden of diseases in 2001, but is anticipated to rise to number two by 2020 (Murthy et al., 2001). This prediction is supported by a report from the Organisation for Economic Co-operation and Development (OECD) showing that the use of antidepressants has increased considerably from 2000 to 2011 in most countries (OECD, 2013). In Australia, the consumption of antidepressants was 89 defined daily doses/1000 inhabitants/day in 2011, almost double that of those dispensed in 2000. Among OECD countries, only Iceland used more antidepressants per capita than Australia (OECD, 2013; Stephenson et al., 2013).
Antidepressants are not recommended routinely to patients with subthreshold depressive symptoms or mild depression as the risk-benefit ratio is poor. Instead a stepped-care model for treatment of depression is recommended, both in adults and in children and adolescents (Anderson et al., 2010; Attwood et al., 2005). According to these recommendations, detection, recognition and an assessment of the risk profile should be followed by psychosocial interventions, increased physical activity and cognitive behavioural therapy. In adults, drug treatment should be considered if the patient has a past history of moderate to severe depression or if the depression persists for a long period despite other interventions. In moderate or severe depression, a combination of high-intensity cognitive behavioural therapy or psychological intervention and antidepressant medication are recommended. In children and adolescents, referral to specialised services should be considered if drug treatment seems to be needed.
The Australian Bettering the Evaluation and Care of Health (BEACH) study (Britt et al., 2011, 2012, 2013, 2014) found that depression was the most commonly treated clinical problem in general practice, representing 5.1–5.6% of treated problems in the years 2010–2013. Clinical treatment was provided in about 40% of contacts registered as depression, and pharmacological treatment was provided for half of these contacts (49.1–53.0%). Depression was also the most frequent problem referred to allied health service (10.6–12.0% of such referrals).
Antidepressants are mainly prescribed by general practitioners (GPs) (Kjosavik et al., 2009, 2011; McManus et al., 2003). In Australia, GPs prescribed about 70% of antidepressants for depression, 16% for other psychological problems and 10% for musculoskeletal problems, neurological problems, premenstrual or menopausal problems (Henderson et al., 2010). A Canadian study has shown that tricyclic antidepressants now appear to be recommended most often for non-psychiatric reasons (Patten et al., 2007). The prescribing practices may differ among GPs, psychiatrists and other physicians due to differences in patient populations and diagnoses. Yet, an international review found there were few differences in symptoms and demographic profiles between patients with major depression in primary and secondary care (Kennedy, 2013).
Guidelines for treatment of major depression recommend maintaining antidepressant drug use for 6 to 12 months after remission of the first episode, and for 1 to 5 years for patients who have relapsed (Hegarty et al., 2009; Lam et al., 2009; Timonen and Liukkonen, 2008). Despite the recommendations, studies have shown that the treatment with antidepressants in primary care has been discontinued early in a high proportion among new users (Burton et al., 2012, 2015; Milea et al., 2010; Serna et al., 2010). On the other hand, the risk of re-initiation of antidepressants in patients with short treatment duration has been shown to be lower than in patients with a first-time treatment duration of more than 6 months, perhaps due to over-prescribing of antidepressants to patients without a real need for such a treatment (Verdoux et al., 2011). Increased use of antidepressants may result from elongation of treatment episodes as recommended by guidelines (Reid et al., 2014), but may also be a result of too lengthy a treatment if the physician does not cease the treatment when recommended (Johnson et al., 2012). Studies about treatment duration have typically focussed on treatment in new user populations (Burton et al., 2012, 2015; Serna et al., 2010), but knowledge about overall antidepressant treatment duration is scarce.
Aims of the study
The aims of this study were to analyse the distribution of initial prescribing of antidepressants reimbursed for concession card holders under the Pharmaceutical Benefits Scheme among GPs, Psychiatrists and Other Physicians, determine the proportion of incident and prevalent users and to assess the average treatment duration for the use of these drugs.
Material and methods
Data source
The study is based on information about prescription of antidepressants issued to a sample of 10% of the patients receiving medicines listed on the Pharmaceutical Benefits Scheme (PBS) between 1 January 2005 and 31 December 2013. The data cover all reimbursed prescriptions of antidepressants redeemed in Australia, but lack information about drugs that cost less than the co-payment level (fully paid for by the patients) and drugs that are not PBS listed (most are). In addition, the material lacks information about drugs used by patients in hospitals.
Only prescriptions redeemed by concession card holders (about 90% of the prescriptions in the material) were included in the study, as these patients are eligible for reimbursement for all subsidised PBS medicines, and the database has a complete record of the prescriptions redeemed by these patients.
The study used the following variables; an unique personal identifying code for patients and prescribers, patients’ gender, year of birth and eventual year of death, prescriber’s specialty, dispensed items generic name, Anatomical Therapeutical Chemical (ATC) code and date for redeemed prescriptions (de-identified data).
Methods
The drugs were divided by class into; Tricyclic Antidepressants (TCA) (amitriptyline, clomipramine, dothiepin, doxepin, imipramine and nortriptyline), Selective Serotonin Reuptake Inhibitors (SSRI) (citalopram, escitalopram, fluoxetine, fluvoxamine, paroxetine and sertraline), Serotonin Noradrenaline Reuptake Inhibitors (SNRI) (desvenlafaxine, duloxetine and venlafaxine) and others (Others) (mianserin, mirtazapine, moclobemide, reboxetine tranylcypromine and phenelzine).
The study period was from 2010 to 2013. Data from 2005 to 2009 were used to exclude prevalent users in the analysis of incident users. The prescribers were grouped by specialty into three groups; GPs, Psychiatrists and Other physicians. When information about the prescriber’s specialty was missing on some prescriptions in the material, the physician’s specialty code from other prescriptions was used, if known.
Estimation of treatment duration was based on the epidemiological equation: prevalence/incidence = mean duration (Freeman and Hutchison, 1980). This relationship is valid for a steady state. Then the prevalence and incidence figures for a short period of time are enough to calculate the average treatment duration even when the latter is considerably longer than the observation period. Since the figures for prevalence and incidence in this study slightly changed over time, the mean value over the studied period from 2010 to 2013 was used in the equation.
Statistical analysis
Excluded from the material were as follows: (a) records lacking information about patient’s age (n = 4004) or gender (n = 3), (b) records lacking information about physician’s identity (n = 193), (c) records on prescriptions redeemed after patients death (n = 1734), and (d) records on bupropion (n = 6412) as it is used mainly for treatment of nicotine addiction. The analysis was performed using descriptive statistical methods. Stata software version 11.0 (Stata Corp., College Station, was TX, USA) were used.
Ethics and approvals
The study was approved by the Department of Human Services External Request Evaluation Committee (EREC) and conducted in accordance with the agreement between the Department of Human Services and the University of South Australia.
Results
The 1,154,796 prescriptions redeemed by 193,588 patients in the period from 2010 to 2013 were issued by 50,230 physicians, of whom 68.5% were classified as GPs, 5.0% as psychiatrist and 30.0% as other specialties. (As specialty can change over time, some doctors were classified in different groups during the study period. Consequently, the sum is greater than 100).
The number of prevalent users in the material increased from 90,475 in 2010 to 103,305 in 2013 (Table 1). In the same period, the number on new users, defined as patients who had not redeemed any PBS-registered antidepressant drug in the preceding 5 years, increased from 25,006 in 2010 to 26,289 in 2013 (Table 1).
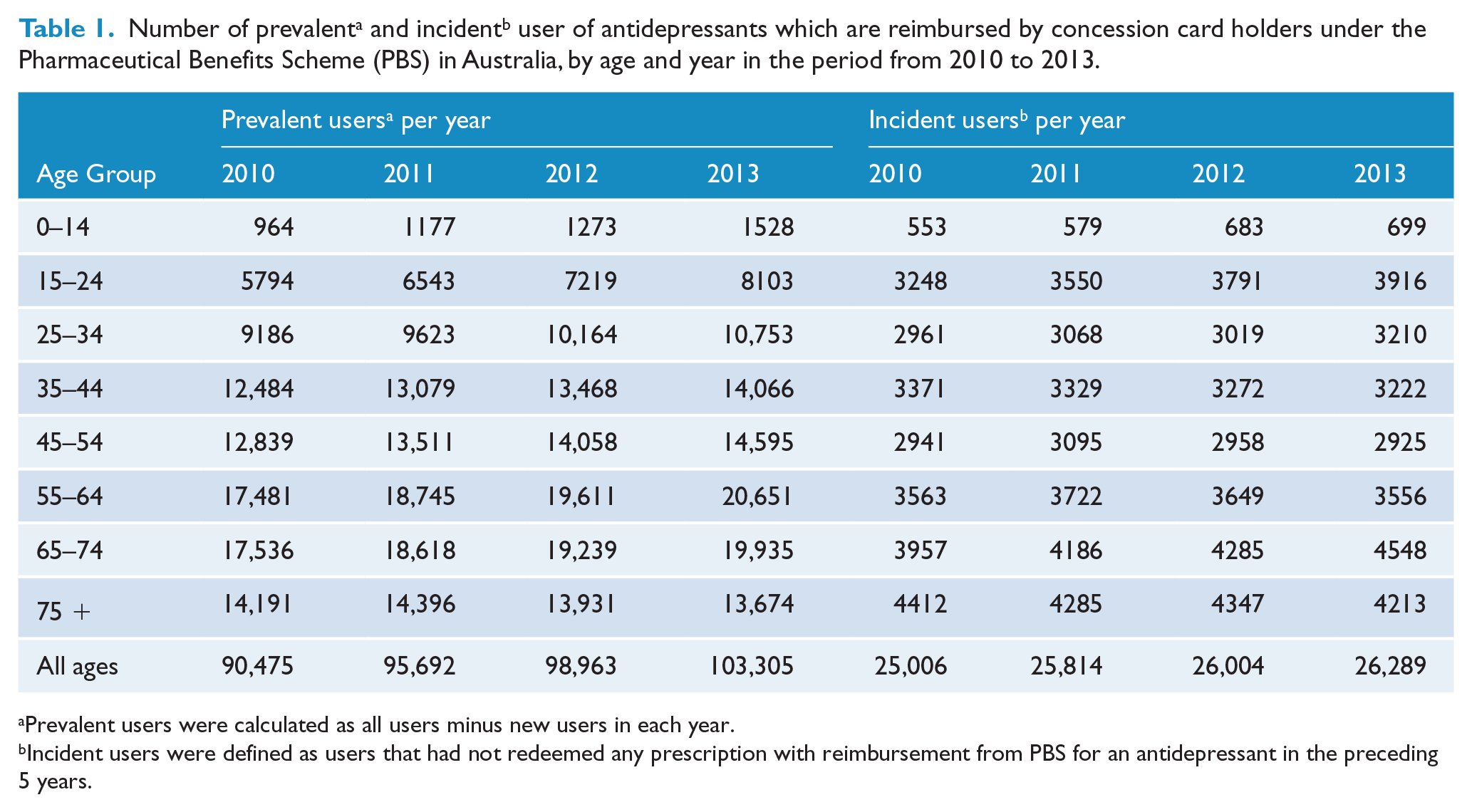
Prevalent users were calculated as all users minus new users in each year.
Incident users were defined as users that had not redeemed any prescription with reimbursement from PBS for an antidepressant in the preceding 5 years.
The epidemiological mean treatment duration in the period was 3.8 years (Figure 1(A)). However, approximately 10% of the incident users redeemed only one prescription. When limited to patients that redeemed more than one prescription, the average treatment duration was 4.1 years (Figure 1(B)) (2010–2012 data used).
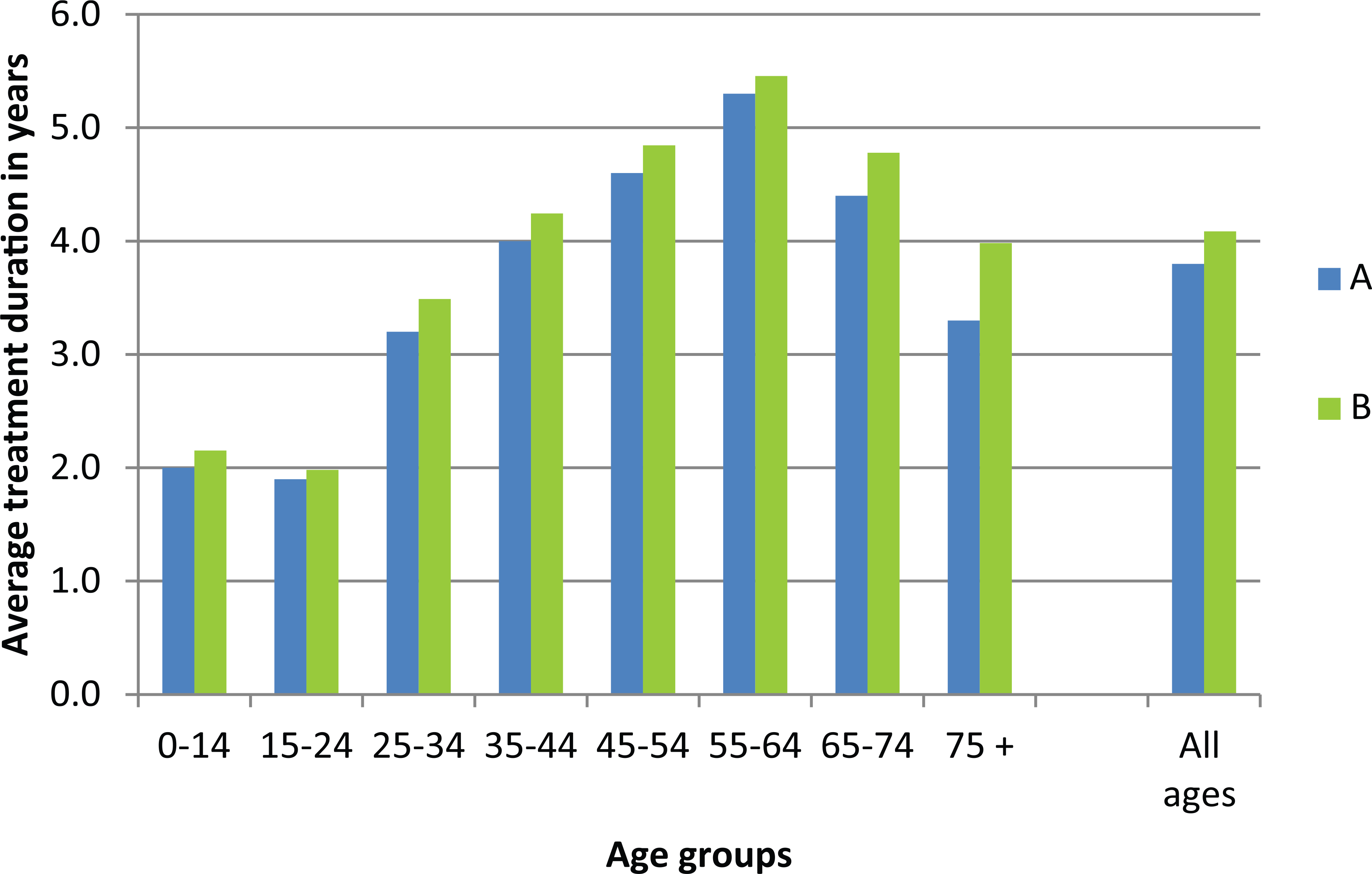
Average treatment duration1 based on the mean figures for prevalence and incidence in the period from 2010 to 2013. (A) 2010–2013, patients who redeemed at least one prescription and (B) 2010–2012, patients who redeemed more than one prescription.
Of new users of antidepressants among concessional card holders, 86% received their first prescription from GPs, 4.3% from psychiatrists and 9.7% from other physicians (Figure 2).
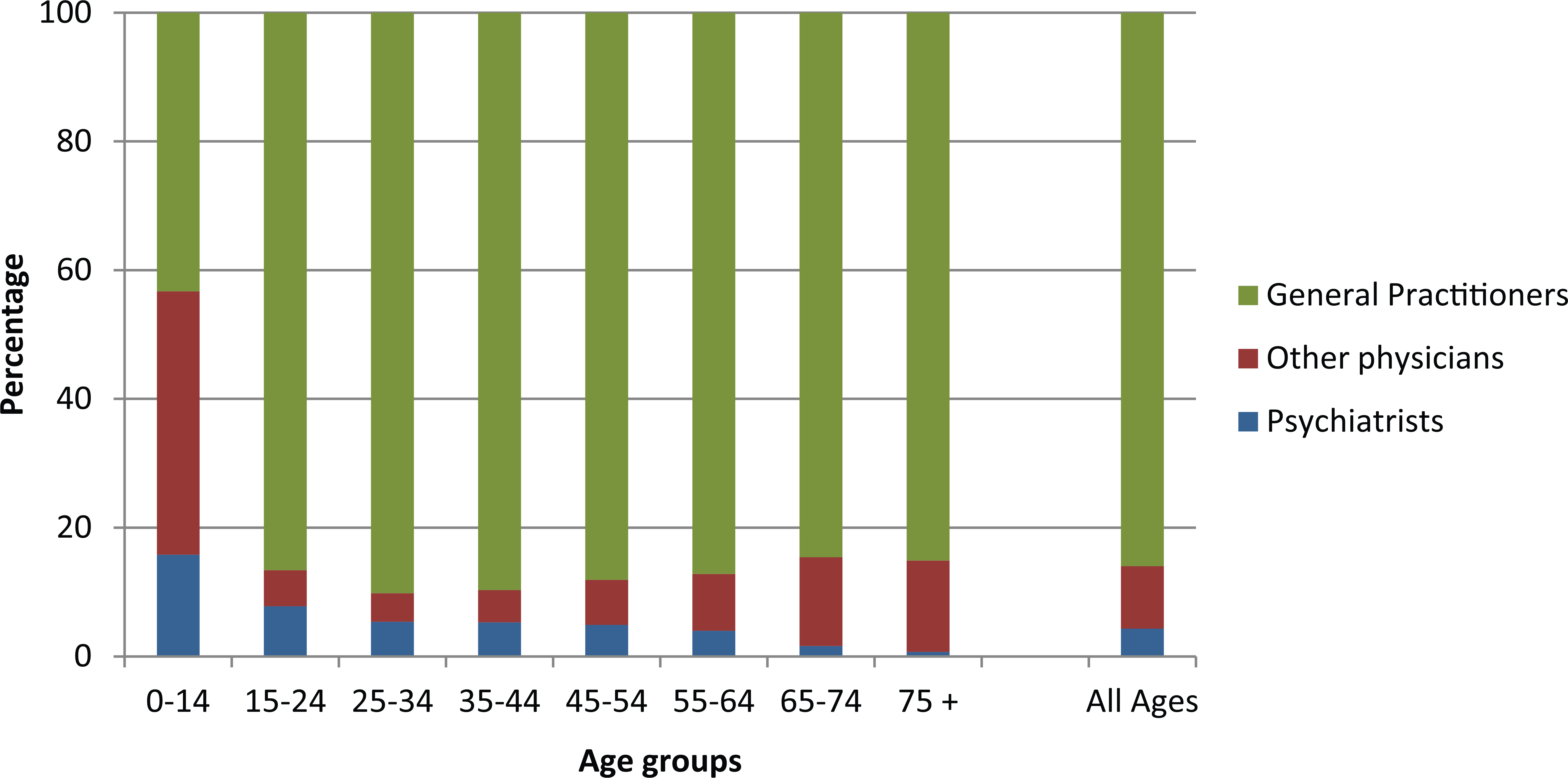
The distribution of prescribers of the first prescription of antidepressants to concession card holders during the period from 2010–2013 among GPs, Psychiatrists and Other Physicians, by patients’ age group and in total.
The proportion issued by psychiatrists varied depending on patient age; psychiatrists issued the first prescription for antidepressants in 15.8% to patients younger than 15 years to less than 1.6% among patients older than 65 years. Other physicians issued the first prescription to 40.9% of patients younger than 15 years. Of these, paediatricians were responsible for 72% (not shown in figure).
The SSRIs were the most commonly used antidepressants, prescribed to 46.6% of the new users, while TCAs and SNRIs were issued to 25% and 17.3%, respectively (Table 2). GPs prescribed the highest proportion of the SNRIs (90%) while TCAs use was highest among Other Physicians (19%). Psychiatrists used other antidepressants relatively more often (17%), but these drugs were used to a limited extent, and had little impact on the total consumption.
The relative use of different antidepressants to new users with concession card in the period from 2010 to 2013, and the distribution of these among the different prescriber groups.
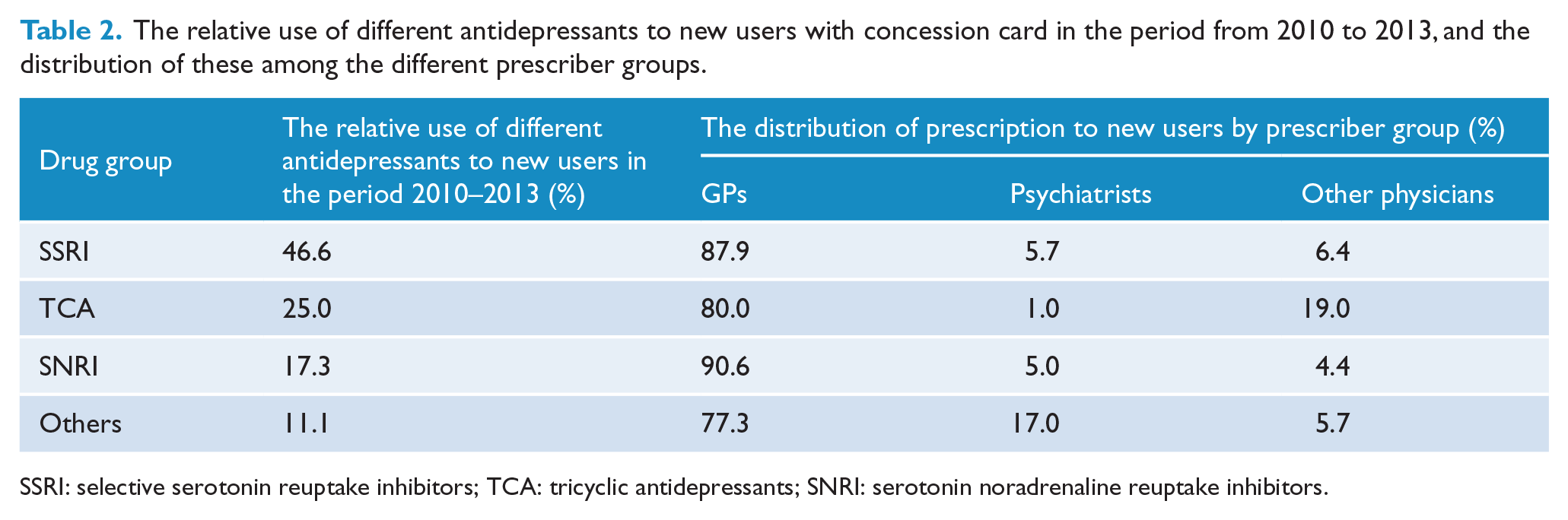
SSRI: selective serotonin reuptake inhibitors; TCA: tricyclic antidepressants; SNRI: serotonin noradrenaline reuptake inhibitors.
Discussion
Treatment of mental health problems in general, and particularly depression, involves much more than the use of drugs, including use of cognitive behavioural therapy, psychosocial interventions and increased physical activity. Drug treatment should be considered in more severe cases, and if the non-pharmacological treatment gives too little results.
This study shows that the average duration for treatment with antidepressants in the period from 2010 to 2013 was about 4 years, and seemed to increase slowly year by year as the prevalence increased more than the incidence. Consequently, the data are suggestive of overly long durations, some of which is likely to represent overuse of antidepressants in Australia. This may be due to drug treatment of patients who do not need such treatment, or too little awareness about terminating the drug use leading to unnecessary prolongation of the treatment. Some may also continue to prescribe such drugs at the behest of patients who just feel better taking them or are afraid of ceasing the treatment.
We have found few studies that have analysed treatment duration with antidepressants among prevalent patients in clinical practice. An American study showed that about 14% of Americans taking antidepressant medication have done so for 10 years or longer, and more than 60% had been treated for more than 2 years, with no significant difference between the genders (Pratt et al., 2011). A Scottish study covering around 1.2 million of the population, found average treatment duration of 5.5 years. The study also showed that reduced use is possible, as about 20% of patients who had used antidepressants for more than 2 years were successfully able to have the dose reduced or treatment discontinued after review (Johnson et al., 2012).
The number of patients in our study who redeemed only one prescription during the period from 2010–2012 was less than 10%. This is in line with American findings (Pratt et al., 2011), but less than in other studies (Burton et al., 2012, 2015; Kjosavik et al., 2011; Milea et al., 2010; Serna et al., 2010; Verdoux et al., 2011). It is well known that GPs prescribe the vast majority of antidepressants (Australian Institute of Health and Welfare, 2014; Kjosavik et al., 2009, 2011; McManus et al., 2003). This study also confirmed that GPs issued the first prescription to concessional card holders in 86% of the patients, while psychiatrists and paediatricians had a considerable impact on the use among patients younger than 15 years.
Guidelines on treatment duration with antidepressants are largely based on consensus and on experience from studies mostly undertaken in specialised health care settings (Hegarty et al., 2009; Piek et al., 2010). These have encouraged GPs to use antidepressant treatments for at least 6 months after remission of first episode of major depression, and to give long-term treatment to patients at high risk of relapse. However, a review of the literature on long-term treatment with antidepressants (El-Mallakh and Briscoe, 2012) found that the risk of recurrence did not fall with longer stabilisation prior to discontinuation of an antidepressant, and the relapse rate was highest in the first 6 months after cessation. The chance of getting depressed very soon after antidepressant discontinuation increased with more prolonged antidepressant exposure, raising the question of whether such relapses represent an antidepressant-withdrawal depression. While long-term use may be necessary in some patients, the criteria for patients at risk or patients in need for long-term treatment are ambiguous, and evidence and recommendations are lacking on the duration of maintenance treatment of such patients in general practice (Hegarty et al., 2009; Piek et al., 2010). Whenever prescription is renewed, physicians should consider whether further treatment is necessary, justified and in accordance with guidelines, and terminate the drug treatment when appropriate (Ambresin et al., 2015).
Strengths
The study is based on a large sample of more than 2 million patients, representative for all PBS-registered persons in Australia. The definition of incident drug use is strict, excluding patients receiving treatment during a 5-year baseline period. By excluding patients who redeemed only one prescription, the results are refined to patients who have accepted to continuing the treatment by an additional.
Limitations
The analysis is based only on prescriptions redeemed by concession card holders in a 10% sample of the PBS registered patients. Thus the incidence and prevalence figures do not include general beneficiaries due to the lack of complete capture of their data. In addition, information about drugs used in hospital is lacking.
There may be a slight over-estimate of incident patients when patients are transferred from general beneficiary to concessional status. This group would be considered new users when they redeemed their first prescription as concessional card holders even though they may have used such drugs earlier. This would also have the consequent effect of leading to an underestimation of the treatment duration.
The impact of GPs on the prescribing of drugs to new users may also be overestimated as the treatment may have been initiated or advised by a psychiatrist or another specialist although the first PBS-registered prescription was issued by a GP.
The study lacks clinical information and is based on the number of treated patients, not on the amount of redeemed or used drugs. Consequently, the quality of the given antidepressant treatment or the dosage have not been evaluated.
Conclusion
This epidemiological analysis shows that the average duration of treatment with antidepressants in Australia is about 4 years. Based on this finding, it seems important not only to recommend that GPs give antidepressants for a sufficient period of time, but also to remind them to revise the treatment regularly. Until the evidence is clarified, GPs should review patients on antidepressant treatment regularly, at least every 6 months, and try to cease drug treatment when appropriate.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Svein R. Kjosavik received postdoctoral fellowship from The Western Norway Regional Health Authority.