
Abstract
‘Depression is a common, recurrent disorder. The New Zealand Mental Health Survey conducted between 2003 and 2004 found that 16%% of adults had experienced major depressive disorder some time in their life and 5.7%% in the past 12 months [1,2]. The highest lifetime prevalence rates were found in the group aged 45–64 years (18.4%%) and lowest among those aged >=65 (9.8%%). The median age of onset was 32 years and, although most experienced an episode of depression before age 50 years, one-quarter will have a first episode after this. Women had higher lifetime prevalence rates then men: 20.3%% versus 11.4%% [1]. Twelve month depressive disorder prevalence for Pacific people in New Zealand was the lowest and, after adjustment for socioeconomic factors, was significantly lower (3.5%%) than prevalences for both Māori and Others (5.7%% and 5.8%%, respectively) [3].
Evidence-based treatment for major depressive disorder includes both pharmacological and psychological interventions. Recommended treatment for mild depression typically involves supportive clinical care alongside problem-solving skills development and supportive counselling [4–6]. Antidepressants and psychological treatments (cognitive behavioural therapy and interpersonal therapy) are equally effective in moderate depression, but antidepressants are most effective in severe depression with adjunctive psychological therapy for refractory symptoms [4,6]. Depression has a high rate of relapse and so continuation of an effective treatment is recommended for at least 6 months and ideally 1 year after an episode [5,6].
Selective serotonin re-uptake inhibitor (SSRI) antidepressants are recommended as first-line medicines for moderate depression primarily because of their lower adverse effect burden and toxicity in overdose compared to the older agents, such as tricyclic antidepressants (TCAs) and non-selective monoamine oxidase inhibitor (MAOI) antidepressants [4–6]. TCA agents tend to be used as a second line or in melancholic and severe depression, and MAOI agents for atypical depression [5,6]. Venlafaxine, a newer antidepressant, is also recommended as a second line or in melancholic and severe depression [6], but its use in New Zealand is restricted by the government pharmaceutical funding agency to treatment-refractory depression only [7].
Traditional efficacy data from clinical trials supports comparability between antidepressants for the majority of patients with depression. There is debate, however, about the effect of gender and age in clinical response to SSRI and TCA agents. Gender differences in treatment response have not been found consistently, but some studies suggest that men respond better to noradrenergic antidepressants such as nortriptyline and women to serotonergic agents such as fluoxetine [8,9]. Age has also been suggested to be involved in antidepressant response, with adolescents and young adults (aged <25 years old) responding better to serotonergic rather than noradrenergic antidepressants [8,10–12].
A review of antidepressant use in New Zealand from 1993 to 1997 consistently found a significant increase in the antidepressant market primarily for SSRI prescriptions, while prescribing of the older drugs remained constant [13]. This increase occurred nationwide, but regionally there was variation in antidepressant dispensing
levels (after adjustment for population size), with the highest rate being 2.3-fold the rate in the lowest area each year for 1993-1997 [14]. Initially there was also regional variation in the type of antidepressants prescribed, but by 1997 the regions had converged in terms of the ratio of older: newer antidepressant dispensing as prescribing of newer antidepressants increased [14].
Little more is known about the use of antidepressants at a national level in New Zealand despite the increased public awareness, educational campaigns and expenditure on pharmaceutical treatment for depression. Therefore the aim of the present paper was to explore community antidepressant dispensing trends in New Zealand over a 3 year period (2004-2007), and in particular with a focus on trends by age, gender, ethnicity, region and type of antidepressant.
Methods
These data were extracted from the data warehouse (held by the New Zealand Health Information Service) of all subsidized claims for antidepressants dispensed on prescription at all pharmacies in New Zealand between the period 1 July 2004 and 30 June 2007. The Pharmaceutical Management Agency of New Zealand (PHARMAC) is responsible for the management of the New Zealand Pharmaceutical Schedule of >2000 government-subsidized community medicines. In addition, PHARMAC is responsible for promoting the optimal use of medicines; for managing subsidies of some medicines and products for public hospitals; and for managing ‘exceptional circumstance’ schemes, which provide funding for medicines to patients with rare conditions. The delivery of PHARMAC's service is governed by a number of laws, Government guidelines and by Medicines New Zealand [15].
The antidepressants funded for community use on the pharmaceutical schedule in New Zealand during this 3 year period included three SSRI agents (fluoxetine, paroxetine and citalopram), 10 TCA and related agents (amitriptyline, nortriptyline, trimipramine, imipramine, clomipramine, dothiepin, doxepin, maprotiline, mianserin and desipra-mine), two non-selective MAOI agents (phenelzine and tranylcypramine), one reversible monoamine oxidase-A inhibitor antidepressant (moclobemide) and one serotonin and noradrenaline re-uptake inhibitor (SNRI) antidepressant (venlafaxine). Most were fully subsidized, but some had specialist prescribing restrictions or required prescription endorsements, including desipramine, mianserin, maprotiline, moclobemide, paroxetine and venlafaxine during the review period.
Anonymized individual dispensing records were supplied for the study, with demographic data including age, gender, prioritized ethnicity derived from the individual's National Health Index and the District Health Board (DHB) region of New Zealand that the dispensing claim originated from. Use of the unique patient identifier, which was supplied in an anonymized form, allowed identification of the population of individuals who had been dispensed an antidepressant prescription at any time in the 3 year follow-up period. Most medications dispensed on a prescription in New Zealand during the study period were supplied for 3 months (90 days), but most antidepressants were commonly dispensed on a monthly basis unless 3 month supply was specifically requested. For the purposes of the present study the prioritized ethnicity data were further aggregated into three categories: Māori, Pacific People and New Zealand European and All others combined (NZEO).
Calculating the prevalence of antidepressant dispensing
We calculated the prevalence of antidepressant prescribing for each of the five main antidepressant types funded on the pharmaceutical schedule (SSRI, TCA, MAOI, venlafaxine, moclobemide) in 2004–2005, 2005–2006 and 2006–2007 separately for male and female subjects among the ages 15–24, 25–44, 45–64 and ≥65. In the present study we used the number of prescriptions rather than the number of individuals as our numerator, because we were interested in the overall amount of antidepressants dispensed. The total of all antidepressant prescriptions claimed for each age group was used as the denominator and ethnicity-specific analyses were not conducted due to the small size of cells for some age/gender combinations within ethnic groups.
Calculating antidepressant dispensing rates
To calculate rates of antidepressant dispensing for different age, gender and/or ethnic groups, a dataset consisting of the population receiving antidepressants was required. Therefore, we extracted the first occurrence of an antidepressant prescription dispensed for an individual in each financial year (2004–2005, 2005–2006 and 2006–2007), irrespective of the type of antidepressant dispensed. Prescribing rates per 100 000 were age standardized to the NZEO population according to the 2006 Census population [16]. We calculated prescribing rates for the population aged 15–24, 25–44, 45–64 and 65++, by gender and ethnicity and DHB. In addition, incidence rate ratios were calculated, with NZEO as the reference population.
Results
Prevalence of antidepressant dispensing
The 12 month prevalence of antidepressant dispensing among the total population aged 15–100 years increased from 7.36%% in 2004–2005 to 8.21%% in 2005–2006 and to 9.39%% in 2006–2007 (analysis not shown). The pattern of prescribing by drug type is reported in Table 1 and shows that among the total population SSRIs were the most commonly dispensed drug, accounting for approximately 53%% of all prescriptions per annum. There was a slight reduction in the dispensing of TCAs, from 42.77%% (42.69–42.85%%) in 2004–2005 to 40.46%% (40.39–40.52%%) in 2006–2007, in addition to a marginal reduction in dispensing of moclo-bemide, from 1.61%% (1.59–1.63%%) in 2004–2005 to 1.23%% (1.22– 1.24%%) in 2006–2007. These reductions were associated with a twofold statistically significant increase in the prevalence of venlafaxine dispensing over time, from 2.43%% (2.40-2.45%%) in 2004-2005 to 5.94%% (5.91-5.97%%) in 2006-2007. Table 1 also reports the prevalence of dispensing by antidepressant type for each gender and demonstrates that female subjects account for approximately two-thirds of all prescriptions dispensed, irrespective of the agent dispensed or time.
Pattern of antidepressant prescriptions dispensed: 2004–2007
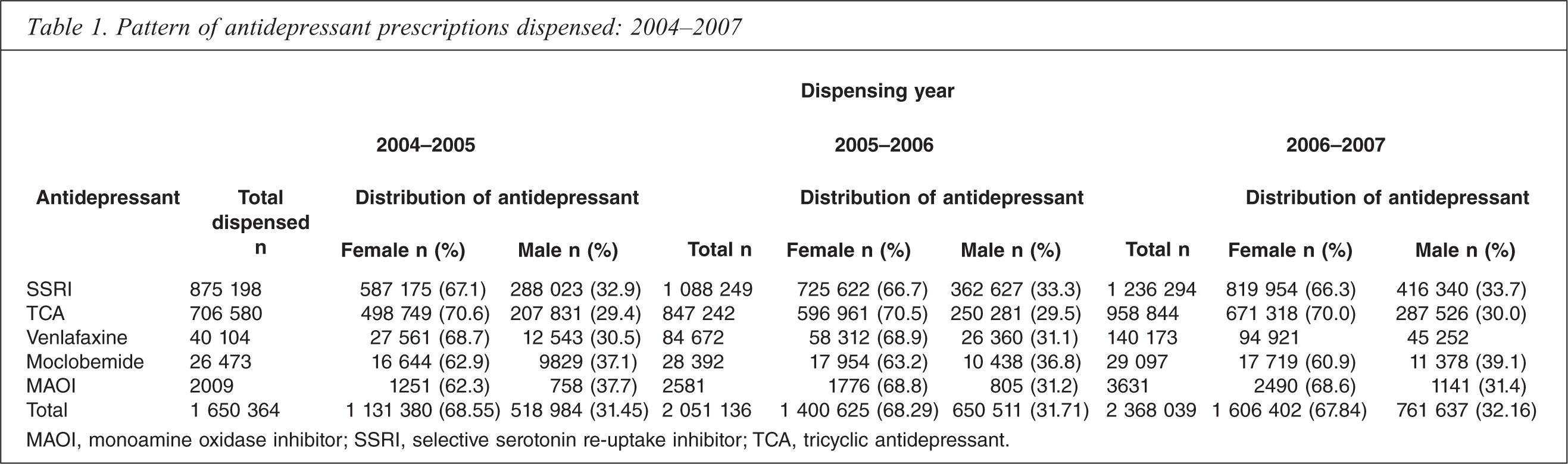
MAOI, monoamine oxidase inhibitor; SSRI, selective serotonin re-uptake inhibitor; TCA, tricyclic antidepressant.
Figure 1 shows considerable differences in the dispensing patterns for different age groups, in which the dispensing of SSRIs decreases while dispensing of TCAs increases with increasing age of the individual. Among women aged 15-24 for example, SSRIs accounted for >70%% of the prescriptions, compared to approximately 20%% of TCAs, although this trend changes with age, such that TCAs become the dominant agent for the population aged 3≥65 years. Throughout the period, TCAs accounted for 55%% of all dispensed agents in women aged 3≥65, compared to 42%% of SSRIs. Dispensing patterns among men aged 15-24 are consistent with those observed for women, but the older male population the dispensing of TCAs and SSRIs converges, with each agent accounting for approximately 48%% of antide-pressants prescribed.
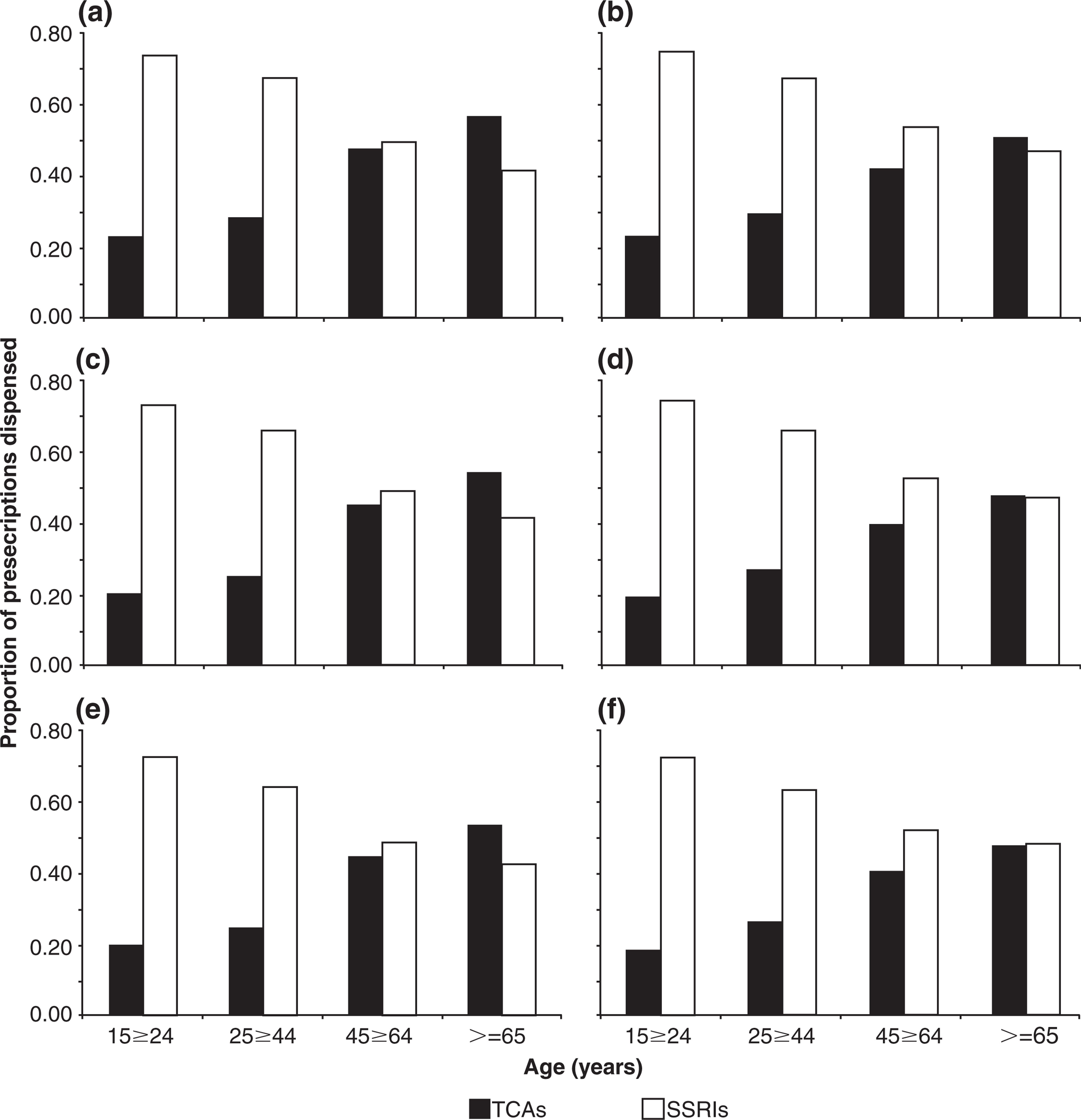
Antidepressant prescribing patterns by age and gender between 2004 and 2007. (a,c,e) Female; (b,d,f) male. (a,b) 2004-2005; (c,d) 2005-2006; (e,f) 2006-2007. (□) Tricyclic antidepressants; (□) selective serotonin re-uptake inhibitors.
Antidepressant dispensing rates
Ethnicity-specific trends in rates of antidepressant dispensing by age and gender are shown in Figure 2, which demonstrates increasing antidepressant use with age irrespective of gender or ethnicity. Figure 2 also demonstrates that the dispensing rates among the NZEO population were significantly higher than for Māori or Pacific populations for each age group, regardless of gender or time. Table 2 reports relative risks in antidepressant dispensing rates for the period 2004-2007, and shows that the rates among the NZEO population are significantly higher than those reported for the Māori and Pacific populations. For example, the rate of antidepressants dispensed to the NZEO population was double that for Māori in both genders aged 15-24 and the older female population (>=65). For the population aged 25-44, the dispensing rate for the NZEO population is 45%% higher (95%% confidence interval (95%%CI) = 42–47%%) than Māori rates for women and 59%% higher (95%%CI = 56-63%%) among NZEO male subjects, while the rate among the population aged 45-64 years is 59%% higher (95%%CI = 56-62%%) and 72%% higher (95%%CI = 67-77%%) among women and men, respectively. Differences in antidepressant dispensing rates are also significantly higher between the NZEO and Pacific population. Dispensing rates in women are between 2.73-fold (95%%CI = 2.62-2.83) and 4.80-fold (95%%CI = 4.48-5.13) greater for NZEO than for Pacific peoples, while among male subjects the dispensing rates are between 2.13-fold (95%%CI = 1.98-2.30) and 4.27-fold (95%%CI = 3.86-4.73) higher in the NZEO population.
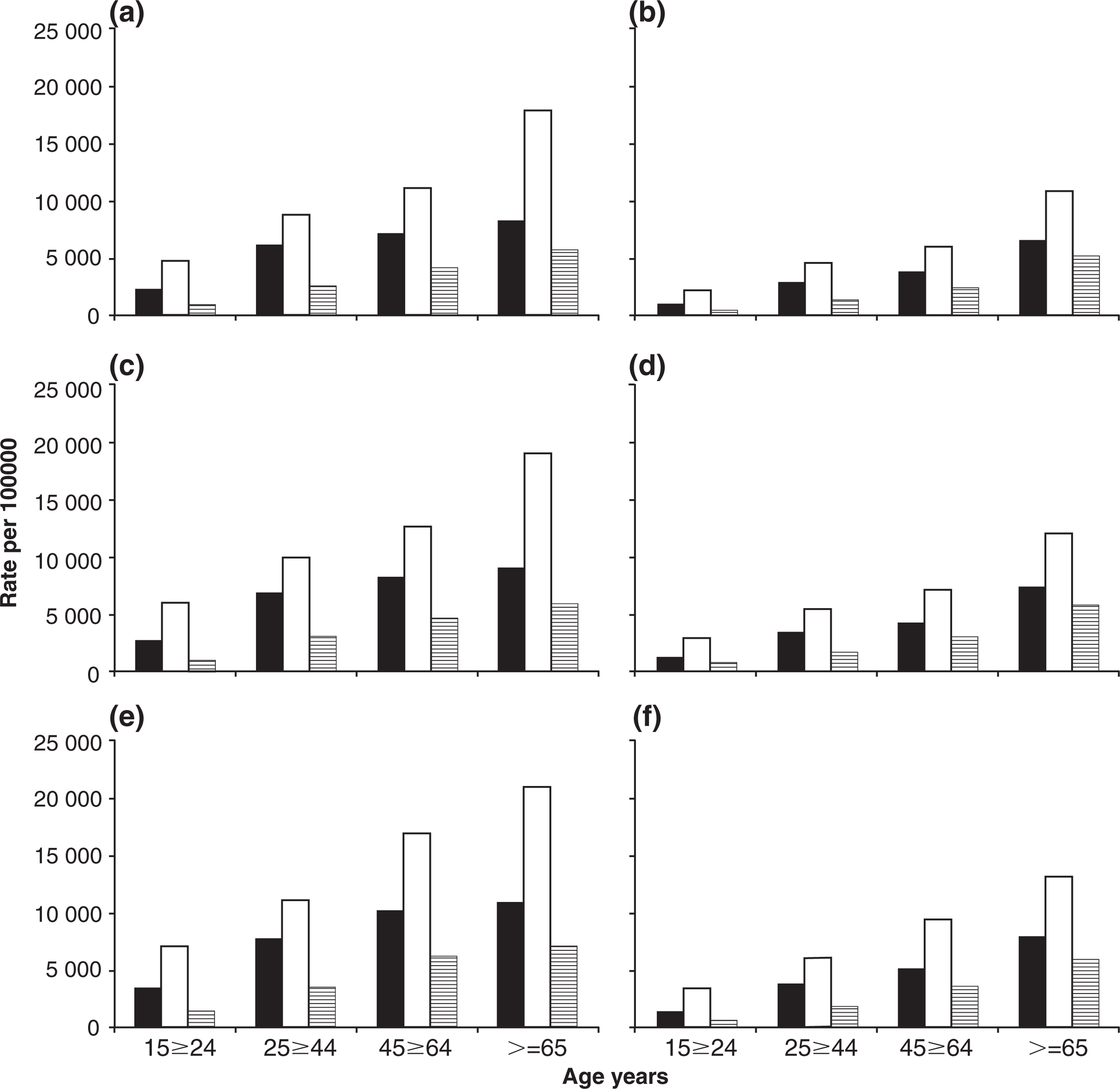
Antidepressant prescribing rates (per 100 000) by ethnicity, age and gender: (a,b) 2004-2005, (c,d) 2005-2006 and (e,f) 2006-2007. (a,c,e) Female; (b,d,f) male. (□) Māori; (□) New Zealand European/Other; □ Pacific.
We also investigated whether there were any geographical inequalities in antidepressant dispensing. Figure 3 shows the age standardized rates by DHB for 2006-2007, by ethnicity and gender. Among NZEO male subjects (Figure 3a), the Waitemata, Counties Manukau, Mid-Central, Capital and Coast, and Southland DHBs dispensed significantly fewer antidepressants than the national NZEO male rate, while 10 of the 21 DHBs dispensed significantly more antidepressants than the national rate. Figure 3(c) shows a considerably stable distribution for Māori male subjects by DHB, in which the Counties Manukau DHB was the only region to be significantly different to the national rate for Māori. Furthermore, at 3269.8 per 100 000 the antidepressant dispensing rate in Counties Manukau was 6%% lower than the national rate for Māori (4438.8 per 100 000). The dispensing trends for Pacific male subjects is shown in Figure 3(e), in which the rates in Northland and Auckland were significantly higher and the rates in the Counties Manu-kau and Mid-Central DHBs were significantly lower than the national rate for Pacific male subjects.
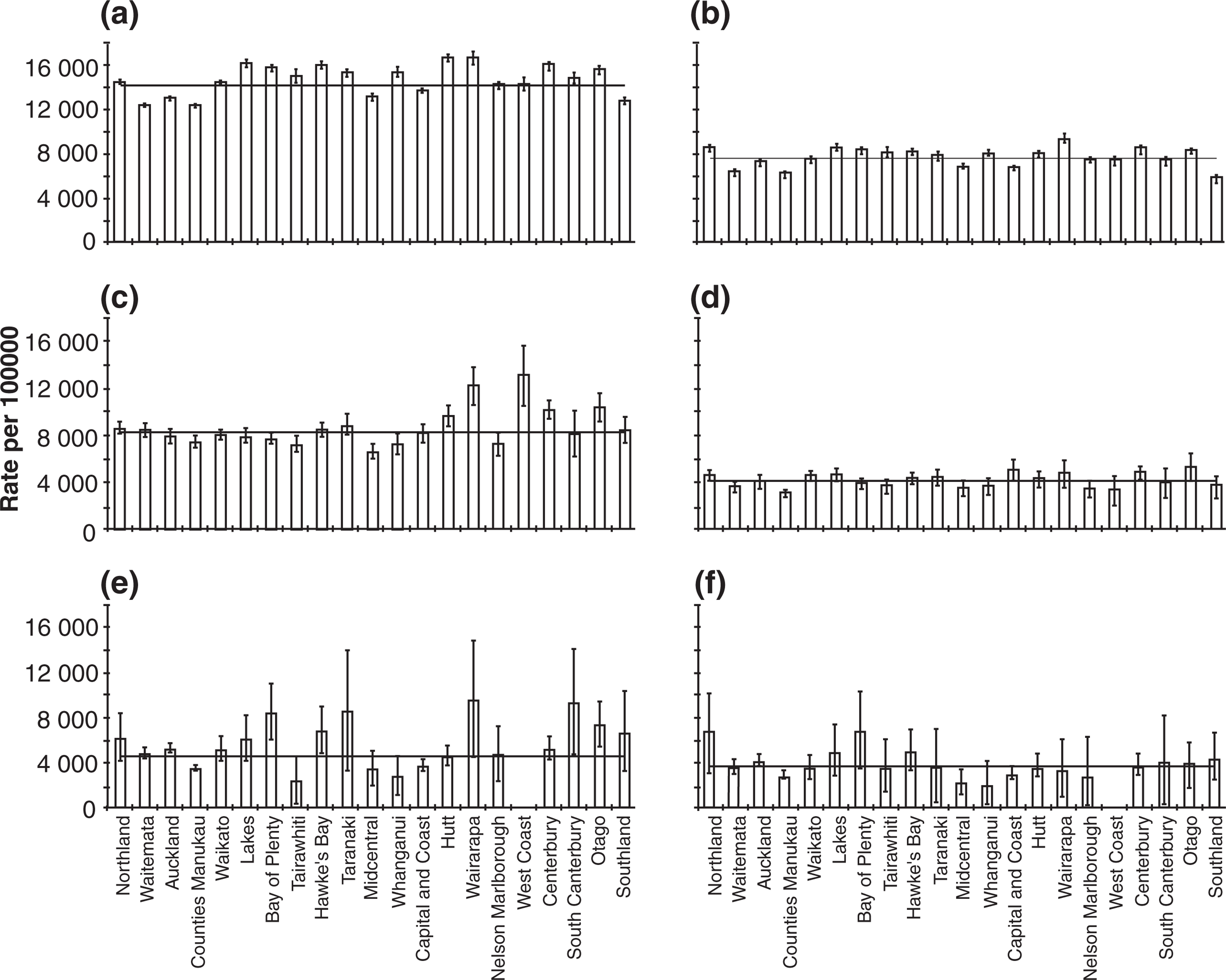
Age standardized rates of antidepressant dispensing by ethnicity, age and gender, 2006–2007. (a,c,e) Female; (b,d,f) male. (a,b) New Zealand European/Other; (c,d) Māori; (e,f) Pacific. ––, national rate for each ethnicity.
Regional trends for NZEO female subjects are shown in Figure 3(b), which indicates a similar pattern to the NZEO male dispensing trends. Antidepressant dispensing rates were significantly higher than the national NZEO female rate in the Lakes, Bay of Plenty, Hawke's Bay, Whanganui, Hutt, Wairarapa, Canterbury and Otago DHBs. Consistent with the trend for NZEO male subjects, the rates in Waitemata, Counties Manukau, Mid-Central, Capital and Coast, and Southland, in addition to Auckland, were significantly less the national rate. Figure 3(d) compares the national rate with the DHBs for Māori female subjects, where the antidepressant dispensing rates in Hutt, Wairarapa, West Coast, Canterbury and Otago were significantly higher than the national rate. Figure 3(f) shows that dispensing rates were significantly higher than the national rate for Pacific female subjects in the Auckland, Bay of Plenty, South Canterbury and Otago DHBs, while Counties Manu-kau and the Capital and Coast DHBs dispensed significantly fewer antidepressants than the national rate.
Discussion
The present study investigated trends in antidepressant dispensing in the community. The present findings of a 30.2%% increase in antidepressant prescriptions between 2004 and 2007 and a 2%% increase in the 12 month prevalence of antidepressant dispensing during the study is consistent with previous local and international studies. For example, the proportion of the population in Ontario, Canada dispensed antidepressants grew by 35%% between 1990 and 1995 [17], while among 100 general practices in the UK, antidepressant prescriptions increased by more than 30%% in 1993–1995, particularly for SSRIs [18]. A more recent study of 139 general practices in East London (UK) found that antidepressant prescriptions doubled between 1996 and 2002, in which an increase in SSRI prescriptions coincided with a decrease in anxiolytics and hypnotics [19, 20]. Research from Australia reported an increase in antidepressant use from 12.4 defined daily doses (DDD) per 1000 population per day in 1990 to 35.7 DDDs 1000 population−1 day−1 in 1998 [21]. Between 1990 and 1998 the use of SSRIs increased significantly, but was met with a 25%% reduction in the use of TCAs.
Roberts and Norris found that expenditure in antidepressant dispensing grew from NZD$26.4 m to NZD$60 m between 1993 and 1996 in New Zealand [13]. In addition, dispensing of antidepressants rose from 473 202 to 1 350 319, although this growth is artificially inflated, resulting from the change to monthly dispensing in May 1996. Nevertheless, the authors reported a doubling in dispensing of new antidepressant agents (fluoxetine, moclobemide and paroxetine), from 20.9%% of dispensed antidepressants in 1993 to 44.8%% in 1997 [13]. Whereas the present study reported a steady use of SSRIs and TCAs between 2004 and 2007, Roberts and Norris reported a steady rise in SSRI prescriptions, and a consistently high use of TCAs in 1993–1997, suggesting that the community dispensing of SSRIs and TCAs has stabilized in recent times. Venlafaxine prescriptions were subsidized from January 2004, therefore the present finding that the prevalence of this agent doubled during the present study possibly reflects a change in prescribing practice by general practitioners (GPs) and psychiatrists. We found that the dispensing rate was considerably higher for women than for men and that antidepressant dispensing increased with age, irrespective of gender or ethnicity, which concurs with previous international research. Female subjects have a higher propensity to engage medical services and therefore one would expect the proportion of scripts to be higher than for male subjects. Of the 7432 patients recruited from 77 general practices in Auckland, New Zealand in a recent prevalence study of depression, 60%% were female [22]. Furthermore, a study from British Columbia in 1996– 2004 found that the prevalence of antidepressant use increased with age, with the prevalence among 54–64-year-olds greater than for patients aged 65–84 years from 1999 onward [23]. A Danish study found that 70.9%% of the 6593 patients followed between 1991 and 1993 were female, although subsequent research from Denmark has reported a reduction in the proportion of female antidepressant users from 72.3%% (1992) to 67.7%% (1997) [24]. Significant differences were found in the type of antidepressant dispensed by gender and age group in Sweden between 1991 and 1996: 54%% of men were dispensed TCAs and 46%% were dispensed SSRIs; for women, 65%% were dispensed TCAs and 35%% were dispensed SSRIs [25]. In Lombardy, Italy, 404 238 people were dispensed antidepressants in 2001, producing a prevalence rate of 2.85 (95%%CI = 2.84-2.87) per 100 male subjects and 5.92 (95%%CI = 5.90-5.94) per 100 female subjects. Moreover, in both genders, the prevalence of SSRI dispensing was higher than prevalence of TCA or other antidepressant dispensing at 53.8%% of men were dispensed SSRIs and 12.1%% were dispensed TCAs; for women 51.6%% were dispensed SSRIs and 12.6%% were dispensed TCAs [26].
There are significant differences in the ethnicity distribution of subjects in the community who are dispensed antidepressants. In the 15–24 age group, for example, the rate of dispensing to the NZEO population was twice that of the rate for Māori and more than fourfold greater than the rate for Pacific peoples (Table 2). Research conducted at a general practice in South Auckland, New Zealand, estimated the prevalence rate of depression in primary care to be 13.8%%. Although the rate of depression among Māori patients was similar to that of non-Māori patients, the study found that Māori subjects were less likely to be treated with antidepressants [27]. The present finding that the antidepressants are dispensed for NZEO patients more than Māori and Pacific peoples is also broadly consistent with further evidence from Te Rau Hinengaro: the New Zealand Mental Health Survey, in which the 12 month prevalence for depressive disorder, adjusted for age and sex, was significantly lower for the Pacific people at 3.9%% (95%%CI = 2.7-5.1%%) than for Others (comparable to the NZEO category used in the present study) at 5.7%% (95%%CI = 5.1-6.4%%) and for Māori subjects at 6.0%% (95%%CI = 5.0-7.1%%). After adjusting for age, sex, educational qualifications and equivalized household income, the 12 month prevalence of depressive disorder remained lowest for Pacific people at 3.5%% (95%% CI = 2.4-4.6%%), followed by Māori subjects at 5.7%% (95%%CI = 4.7-6.6%%) while Others had the highest prevalence of 5.8%% (95%%CI = 5.2-6.5%%), respectively [3]. The present results, however, showed that antidepressant dispensing rates are significantly lower for Māori than for the NZEO population, across all age groups, and further research is required to identify possible explanations for these disparities. The ecological nature of the present study does not allow us to investigate cultural differences in the management and/or treatment of depression and related illnesses. Previous guidelines, however, for the management of depression in New Zealand provide detailed information regarding the assessment, treatment and management of depression in Māori and Pacific people [28].
Relative risks in antidepressant prescribing by gender and ethnicity (2004–2007)
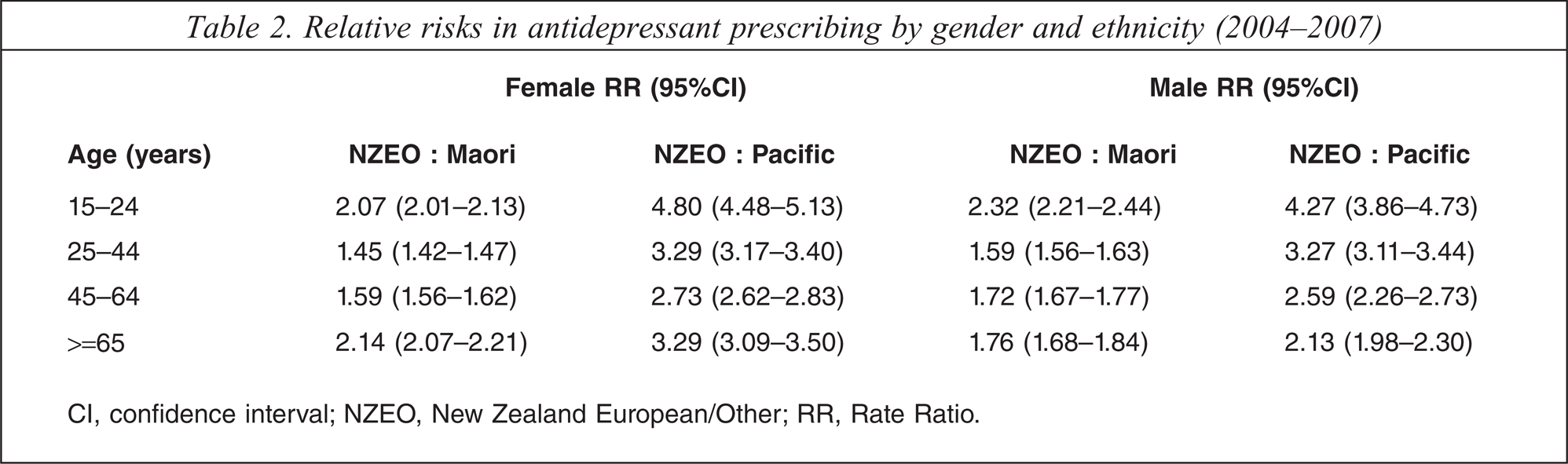
CI, conf dence interval; NZEO, New Zealand European/Other; RR, Rate Ratio.
The data used in the present study were derived from claims for antidepressant prescriptions provided by community pharmacists. Therefore it was not possible to examine whether there were differences in treatment compliance by age, gender and/or ethnicity. Further information is required to investigate trends in alternative treatments for depression as a possible explanation for the differences in antidepressant dispensing rates reported in the present study.
Te Rau Hinengaro: the New Zealand Mental Health Survey examined ethnicity differences in access to mental health treatment, and found that service (health or other social service) utilization was highest among the Other population (41.1%%), followed by Māori subjects (32.5%%), and only 25.4%% of Pacific patients, although these differences were statistically insignificant when adjusted for age, sex and socioeconomic position [3]. Crampton et al. found that after adjusting for age, gender, deprivation, rural/urban localities and type of provider, average annual exposure to primary medical care was higher in the European ethnic group than in the Māori, Pacific, and Asian ethnic groups [29]. The trends in ethnicity-specific antidepressant dispensing and access to mental health services is consistent with trends reported for other health outcomes including mortality [30, 31] and morbidity [32–34].
The DHBs used in the present study were introduced in December 2000 and are not directly equivalent to the Area Health Boards or Regional Councils used in previous studies investigating antidepressant dispensing trends geographically [14,35]. Although there was considerable variation in the dispensing rates between DHBs, there were few DHBs that were significantly different to the ethnicity-specific rate of dispensing for New Zealand as a whole; and there were subtle differences in the dispensing trends by gender (Figure 3).
The trend for increased dispensing of antidepressants has led to some concern of ‘over-prescribing’ but, in light of the prevalence rates found in epidemiological studies such as the New Zealand Mental Health Survey, this suggests that more individuals in New Zealand are now accessing treatment. The largest single risk factor for suicide is depression and, in parallel with increasing anti-depressant dispensing, decreasing suicide rates and behaviours have been reported both in New Zealand and internationally [36–38]. In fact, as SSRI prescriptions for adolescents decreased in both USA and Netherlands after regulatory warnings were issued about possible association between suicide risk and antidepressants (2003-2004), correspondingly youth suicide rates increased [39]. With this treatment association in mind, the trend of increased dispensing of antidepressants found in the present study should continue to have a positive effect on suicide rates in New Zealand.
The rate of suicide among non-Māori subjects decreased significantly from 13.7 per 100 000 in 1996 to 11.0 per 100 000 in 2006. In contrast, Māori suicide rates fluctuated during this period, decreasing from 18.3 per 100 000 in 1996 to 17.2 per 100 000 in 2006. Thus, one may argue that any improvements in suicide resulting from the use of antidepressants will likely have a greater impact on the NZEO population, because they receive substantially more antidepressants than Māori subjects, despite depression prevalence rates being comparable.
The present cross-sectional study is based on data from a national register of antidepressants dispensed through community pharmacies and does not provide any information concerning the prescriptions written, or about patient adherence to antidepressant medication. Because these data were not linked to clinical information for the patients, we were unable to determine the extent to which antidepressant agents are used for other psychiatric disorders such as anxiety, nor were we able to analyse the data according to clinical outcomes. The present study reports trends in the antidepressant dispensing of agents that were subsidized by the Government, therefore newer antidepressants such as sertraline, reboxetine, and mirtazapine were excluded.
It is important to acknowledge that different agents may be prescribed in various strengths and/or durations for different patients. For example, more tablets/ capsules are required to reach a therapeutic dose of a TCA compared with an SSRI or SNRI. Secular trends in antidepressant use and adherence are important public health issues. A recent longitudinal study examining depression among Australian general practices found high rates of antidepressant prescribing by GPs. Furthermore, although depression is recognized as a chronic, recurrent illness, the GPs typically prescribed short courses of antidepressants [40]. We were not able to differentiate trends for older and newer antidepressant agents; this may mask a proportion of patients that continue a particular treatment plan (e.g. TCAs) for historical reasons and we acknowledge that analyses by age conducted in the present study may confound this association. Subsequent research will explore trends in the duration of antidepressant use according to the DDD [41], which will enable comparisons with international research on antidepressant utilization.
We were unable to adjust for socioeconomic position (SEP) in the present analyses due to lack of data. Many contemporary studies use composite deprivation indices (e.g. New Zealand Index of Deprivation 2006) as a proxy measure of an individual's SEP. The only geographical identifier in these data, however, was the DHB of the community pharmacist claiming a subsidy for dispensing. More refined geographical data such as the census area unit would facilitate better use of sociode-mographic measures such as deprivation that may be predictors of dispensing trends.
The present study has shown an increasing trend of antidepressant dispensing between 2004 and 2007, in conjunction with extensive variance in the prescription of antidepressants in the community by age, gender, and ethnicity with moderate variations by DHB. Further research is required to better understand the average duration and doses of antidepressant agents that patients are exposed to, the rate of patients switching from one agent to another, and trends in the dispensing of older and newer antidepressant agents.
Footnotes
Acknowledgements
DE wishes to thank the School of Population Health at the University of Auckland for financial support to purchase these data. Sue Crengle provided useful feedback on early drafts of this manuscript. Val Grey's assistance in formatting the figures in this paper is greatly appreciated.