
Abstract
During the past 10 years major changes have occurred in the use of antidepressants in Australia [1]. However, information as to how these drugs are used in some areas of practice, particularly concerning differences between general practitioners (GPs) and specialists, and the types of depression doctors believe that they are treating, is limited. Several secondary data sources are analysed in this paper to extend our understanding of these issues.
We first seek to establish the proportion of antidepressant prescriptions that were written by psychiatrists and GPs and how this proportion changes over time for a newly listed antidepressant drug. Also examined are differences in the prescribed daily doses (PDDs) between GPs and psychiatrists, the proportion of antidepressant prescriptions initiated by GPs, and the types of depression GPs believe that they are treating.
Materials and method
Prescription dispensing data
These were obtained from Health Insurance Commission (HIC) claim records of prescriptions subsidized under the Pharmaceutical Benefits Scheme (PBS) or its equivalent for entitled veterans, the Repatriation Pharmaceutical Benefits Scheme (RPBS). All citizens are covered by one or both of these subsidization schemes and the data collected represent over 88% of all antidepressant prescriptions dispensed through community pharmacies in Australia [2].
Within these data it is possible to determine the major speciality of the prescribing doctor by an algorithm based on their medical service claims. The percentage of antidepressant prescriptions written by doctors, assigned either a GP or a psychiatrist speciality code in the calendar year 2000, was determined.
To illustrate the evolution of prescription patterns after the introduction of a new antidepressant to the market, we also examined the proportion of GPs who prescribed paroxetine in the first six months of its PBS listing. The change in this proportion was followed over time and compared with that of an established drug in the same class (fluoxetine in the year 2000, having been on the PBS since 1991).
Approvals to prescribe database
To prescribe PBS items that have the highest level of restriction (‘authority required’ items) doctors must obtain prior approval from the HIC before prescribing. Certain additional pieces of information, not held within the standard HIC claims data, are collected as part of this approval process and one of these is the PDD as stated by the doctor. This is a unique set of information as it represents near total community use of these drugs and covers not only GPs but also specialists, who are not included in the standard market research surveys that examine dosage issues [3].
Until the end of 1998 all new antidepressants were initially listed on the PBS as authority restricted items for ‘the treatment of major depressive disorders’. Although these antidepressants no longer require such prior authorization, the restriction for subsidized supply to major depressive disorders still remains. The tricyclic antidepressants (TCAs) have always been listed on the PBS with no restriction on the indications for which they may be used, so were not available for this form of analysis.
As it is only possible to collect the data on PDD when a drug is an ‘authority required’ PBS listing, two to three month periods were selected from within a time when the respective antidepressant was covered by this level of restriction on the PBS. We analysed the daily dose prescribed by GPs and psychiatrists for the following antidepressants (and time periods): moclobemide, fluoxetine, paroxetine, sertraline (February to March 1995); nefazodone (May to July 1997) and venlafaxine (August to October 1996). The time periods were selected depending on when the drugs became available and listed with an authority restriction which allowed dosage data to be collected.
The World Health Organization (WHO) defined daily dose (DDD) is used to examine dosing differences between GPs and psychiatrists [4]. The DDD is based on the assumed average daily dose of the drug when used for its main indication by adults and is the WHO approved unit for drug use studies. It is important to note that the DDD is a nominal value that is used as a standardizing unit to allow comparison within and between countries [5]. Two sample tests of proportion measured at the 5% significance level were conducted using the STATA statistical package [6].
Prescriber surveys
The GP Statistics and Classification Unit of the Family Medicine Research Centre (FMRC) conducts a continuous national survey of service provision in general practice [7]. Rolling recruitment ensures that the GP recording weeks are distributed evenly over the year and that there is constant change in participants. Depending on the period for analysis, the sample size varies but approximates 1000 randomly selected, active, recognized GPs per year. Each GP participant records information for 100 consecutive patient encounters on structured paper forms, including up to four diagnoses/problems and drugs prescribed. Information on prescribing by specialists is not included in these GP surveys. From this survey, we analysed the mean and median daily dose of antidepressants prescribed by general practitioners for depressive disorders in the three-year period April 1998 to March 2001.
The standard information in the survey relates to the specific encounter only. In addition, for subsamples over particular time periods, GPs (or patients through their GPs) are questioned briefly about specific aspects of patient health or health care delivery, not limited to the specific encounter. These are recorded on a section of the form – the Supplementary Analysis of Nominated Data (SAND) [8].
Two SAND surveys conducted with questions nominated by the authors through the Drug Utilization Sub-Committee provide additional information for this paper. In the first (8333 encounters from 309 GPs, collected between 13/7/1999 and 27/3/2000) we sought to determine the proportion of encounters in general practice, irrespective of the problem being managed, that involved patients whom the doctors considered were depressed. Additionally, for patients seen in general practice who were taking antidepressants, we examined the proportion for whom the therapy had been initiated by general practitioners.
In the second SAND survey (5624 encounters from 196 GPs, collected between 16/1/01 and 26/3/01), we examined the type of depression GPs believed that they were treating, given the following categories: major depression; adjustment disorder with depressed mood; chronic mild depression; alcohol/drug induced depression; depression associated with anxiety or anxiety disorder (e.g. generalized anxiety, panic, phobia, obsessive–compulsive). The DSM-IV criteria for major depression [9] were provided in this survey, however, the other diagnoses were given as descriptive terms only with no definitional guidelines. No equivalent data exist for psychiatric practice.
Combinations of these datasets have been used previously in drug utilization studies, and descriptions of the methodology and representativeness of the FMRC surveys have been published [1, 7, 8].
Results
Speciality of prescriber
Proportion of prescriptions by speciality of prescriber
The percentage of antidepressant prescriptions written by doctors assigned either a GP or a psychiatrist speciality code, based on HIC data for all prescriptions dispensed under the PBS/RPBS in the calendar year 2000, are presented in Table 1. These data indicate that 62% to 90% of the various antidepressant classes are prescribed by GPs. On average, GPs prescribed 86% of antidepressants and psychiatrists 10%.
PBS/RPBS antidepressant scripts in year 2000 by speciality of doctor prescribing, sorted in decreasing percentage use by general practitioners (GPs)
The proportion that these subsidized prescriptions represented of overall community use was also estimated for each antidepressant by using 1998 data, the most recent year for which community dispensing information are available [2]. These data are also detailed in Table 1. The lower percentages for the TCAs and the older monoamine oxidase inhibitors (MAOIs) reflect a dispensed price that is below the general PBS copayment, resulting in a less complete capture of data on the PBS than for newer antidepressants, such as the selective serotonin reuptake inhibitors (SSRIs), all of which have a dispensed price above the general copayment ($21.90 as at September 2001).
Change in relative proportions by speciality over time
To examine the movement from specialist prescribing into general practice for a new antidepressant, the proportion of GPs and psychiatrists who prescribed paroxetine in the first six months of its PBS listing, followed by the change in this proportion over time, was compared with that of an established drug in the same class (year 2000 data for fluoxetine – first listed on the PBS in 1991). Details are presented in Figure 1.
Proportion of Pharmaceutical Benefits Scheme (PBS)/Repatriation Pharmaceutical Benefits Scheme prescriptions written by general practitioners (GPs) and psychiatrists in the first 6 months of PBS listing for paroxetine (as an example of a new selective serotonin re-uptake inhibitor [SSRI]) and by year from 1995 to 1998 and for fluoxetine in 2000 (as an established SSRI, first introduced on the PBS in 1991). □, psychiatrists; ▪, GPs.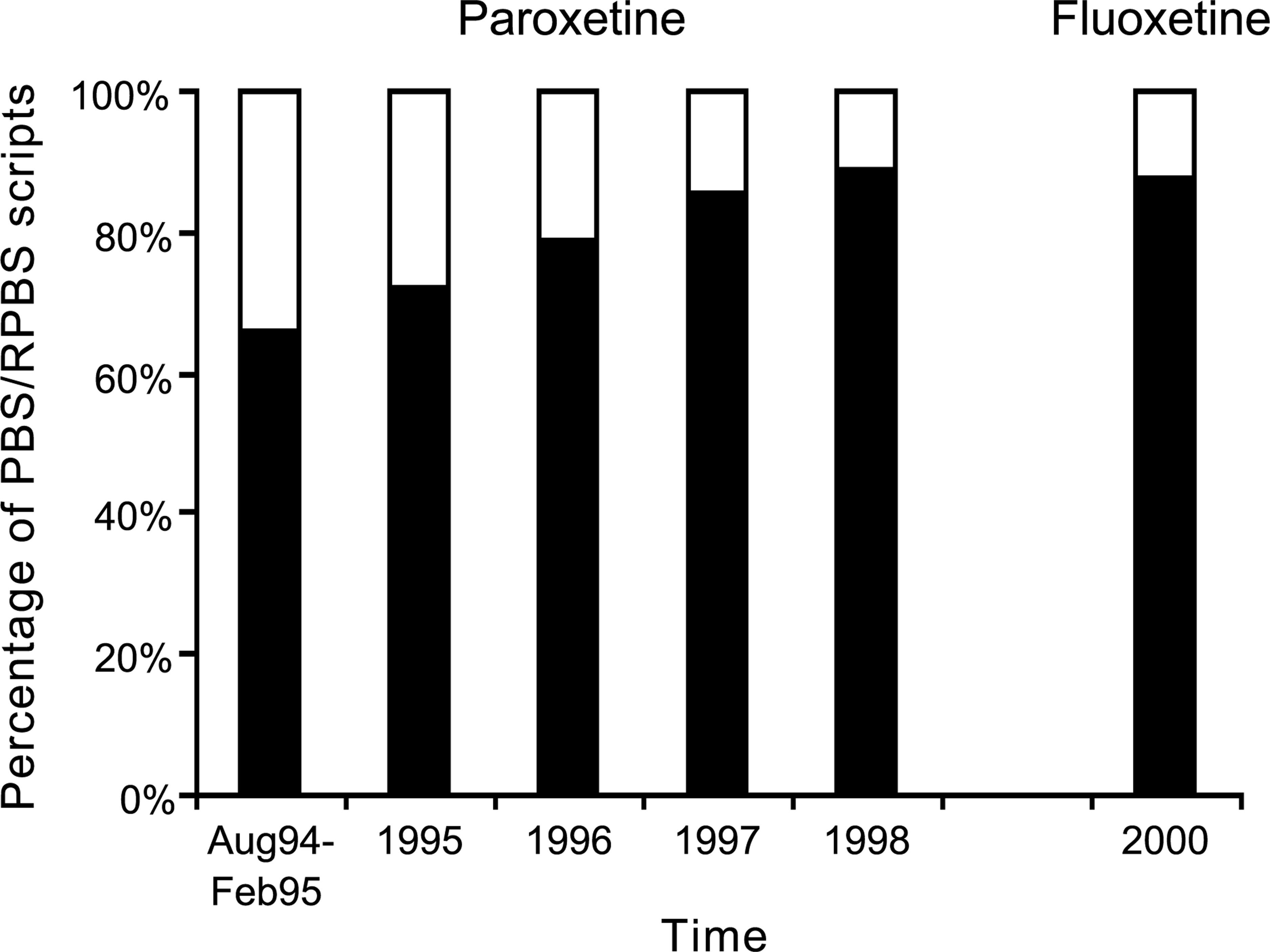
In the first six months of PBS listing (August 1994 to February 1995) 33 628 prescriptions dispensed for paroxetine were written by GPs, representing 64.6% of all the PBS prescriptions for this drug. Psychiatrists were responsible for writing 17 587 paroxetine prescriptions (33.8%) in this period. With longer time on the market, the proportion of paroxetine prescriptions written by GPs increased, with 235 161 (68.5%) in 1995 through to 881 516 (86.2%) in 1998. Conversely, the proportion written by psychiatrists declined from one-third of prescriptions in the first 6 months of PBS listing to around 11% (109 682 scripts) in 1998.
These proportions around 4 years after listing were similar to that ultimately achieved by fluoxetine, an established drug in the class. In the year 2000, 10 years after its market release, the relative proportions for fluoxetine were 84.3% (654 557 scripts) written by GPs and 12% (93 358 scripts) written by psychiatrists.
Doses prescribed by specialists and GPs
In Table 2, the proportions of psychiatrists and GPs who were prescribing a daily dose that was greater than the WHO DDD are compared.
Health Insurance Commission approvals for antidepressants PDDs above the World Health Organization DDD by GPs and psychiatrists during selected intervals within the period that these drugs were ‘authority required’ Pharmaceutical Benefits Scheme listings – moclobemide, fluoxetine, paroxetine, sertraline (February and March 1995); nefazodone (May to July 1997) and venlafaxine (August to October 1996)
Psychiatrists prescribed doses higher than the DDD significantly more often than GPs for all the antidepressants examined. Furthermore, moclobemide was also used in doses higher than the DDD by a significantly greater proportion of both GPs and psychiatrists than any of the three SSRIs – fluoxetine, paroxetine or sertraline (p < 0.0001).
General practice surveys
When used for depressive disorders, TCAs had a PDD consistently lower than the WHO DDD. The PDDs and DDDs for the tricyclic antidepressants most commonly prescribed in the FMRC general practice survey (April 1998–March 2001) were dothiepin (mean, 82.2 mg; median, 75 mg; DDD, 150 mg), amitriptyline (mean, 65 mg; median, 50 mg; DDD, 75 mg), and doxepin (mean, 60.6 mg; median, 50 mg; DDD, 150 mg). These were calculated from the actual doses recorded by participating GPs at individual patient encounters.
The PDDs for the most commonly prescribed SSRIs were much closer to the DDD: sertraline (mean, 72.4 mg; median, 50 mg; DDD, 50 mg), paroxetine (mean, 23 mg; median, 20 mg; DDD, 20 mg), and citalopram (mean, 23.5 mg; median, 20 mg; DDD, 20 mg). Other new antidepressants had a PDD broadly in line with the DDD: nefazodone (mean, 370.6 mg; median, 300 mg; DDD, 400 mg), venlafaxine (mean, 121.6 mg; median, 75 mg; DDD, 100 mg), with the exception being a much higher PDD for moclobemide (mean, 523.6 mg; median, 600 mg; DDD, 300 mg).
Based on a sample of 8333 encounters from 309 GPs in the first SAND survey during 1999–2000, it was estimated that 14.4% (95%CI: 13.1%, 15.7%) of all encounters in general practice, irrespective of the problem being managed, involved a patient whom the doctor considered was depressed. Depression thus appears commonly as a comorbid condition among patients seen in general practice. Additionally, of the 703 antidepressants prescribed in encounters where a depressive disorder was treated, 73% had been initiated by a GP.
The focus of the second SAND survey (5624 encounters from 196 GPs) was on the type of depression that the doctors believed they were treating in the patient encounters where depression was being managed. As stated by the treating doctors, the most common types of depression seen in general practice were, in descending order: ‘chronic mild depression’ (151 encounters, 22.1%); ‘depression with anxiety disorder’ (148 encounters, 21.7%); ‘adjustment disorder with depressed mood’ (139 encounters, 20.4%) and ‘major depression’ (125 encounters, 18.3%).
The most infrequent type of depression was ‘alcohol/drug induced depression’, which as a single form of depression was recorded in 15 encounters only (2.2%). Unlike other types of depression, most of the respondents with alcohol/drug induced depression were male (20/28).
In the majority of cases (87%), the GP only recorded one type of depression. The most common combination was anxious depression with chronic mild depression (5.1% of those managed for depression).
Discussion
Interesting changes have occurred with the use of antidepressants in the past decade, with many new therapeutic options becoming available to prescribers both in specialized psychiatric practice and in primary care. Although most antidepressant prescriptions dispensed under the PBS/RPBS in 2000 were written by GPs (86%), there was a higher than average proportion written by psychiatrists for nefazodone or venlafaxine. Some older drugs such as mianserin and the nonselective MAOI antidepressants, perhaps seen as more difficult drugs to use appropriately (or reserved for special situations), also had a higher proportion prescribed by psychiatrists.
During the early period following listing for subsidy of a new antidepressant (using here the example of paroxetine) a higher proportion of scripts was written by psychiatrists. Paroxetine reached the GP/psychiatrist split seen with an established drug in the same therapeutic class (fluoxetine) around 4 years after its introduction. This may have been due to the initial marketing of these agents being targeted at specialist psychiatrists. The greater proportion of psychiatrist prescriptions for newly marketed antidepressants may also at least partially explain the lower GP prescription rates for nefazodone and venlafaxine in the 2000 data.
Another factor in this gradual uptake by GPs was the restricted nature of the initial PBS listing with an ‘authority required’ for ‘the treatment of major depressive disorders where other therapy is inappropriate’. The application of such a prior approval mechanism was common to the initial listing of most of the new antidepressants. Even when the authority was removed, the PBS listing remained restricted to major depressive disorders, although there is likely to be less effect on prescribing from restricted listing without the administrative requirement to obtain prior approval. The older tricyclic antidepressants have been general PBS listings with no specific prescribing restrictions.
The PBS/RPBS claims data show that most prescriptions are written by GPs, but do not distinguish who prescribes the initial and continuing prescription. However, the SAND survey showed that the majority of antidepressant prescriptions written for depression in general practice were initiated by a GP. This probably reflects the perceived safety of the SSRIs and the fact that SSRIs are now the most commonly prescribed antidepressants, with members of this class on the market for more than decade.
Psychiatrists prescribed higher doses than GPs for all the antidepressants examined, no doubt reflecting the more refractory or severely depressed case-mix seen in specialist practice. Earlier work had also shown that psychiatrists were more likely to use combinations of antidepressants than GPs [10].
In general practice, the PDDs were lower than the defined daily dose (DDD) for the TCAs, but close to the DDD for the SSRIs and other newer antidepressants. The widespread use in general practice of less than therapeutic doses for TCAs in treatment of depression has been previously documented, and probably reflects concerns about adverse effects from a therapeutic dose for TCAs, the need to take as many as six tablets to achieve that dose, as well as the greater likelihood of TCAs being prescribed for patients who are not depressed – (for example in pain management, sleep disturbance, anxiety and back complaints [1]). In contrast, it is simple to prescribe a therapeutic dose of an SSRI which is usually achieved with one or two tablets.
Moclobemide was used in doses higher than the DDD by a significantly large proportion of all prescribers (both GPs and psychiatrists) than any of the three SSRIs examined. This suggests that the designated DDD of 300 mg for this antidepressant is too low to use as an indicator in Australia.
Depressed people represent a high percentage of patients seen by GPs. Although earlier surveys [7] estimated that around 3.5% of encounters in general practice involved management of depression as a specific problem on that occasion, encounter-based data does not equate to numbers of patients. When the diagnosis of depression is considered for all patients seen by the GP, not just those whose depression is managed at the specific encounter, the rate per encounter was more than four times higher (at 14.4 per 100 encounters). The burden of depression as both a specific problem to manage and its occurrence as a comorbid condition is thus considerable in general practice.
The most prominent type of depression that GPs considered they were treating was ‘chronic mild depression’ followed by ‘depression with anxiety disorder’.
The GP survey clearly implies that antidepressants are frequently utilized for the management of ‘chronic mild depression’. For only one in five encounters managed for depression did the GP choose the category ‘major depression’. Major depression may be mild and is often chronic, which may have caused some confusion. It is not certain how GPs interpreted the DSM-IV terminology used. However, the survey data suggest prescribing is often inconsistent with the PBS listing for the ‘major depressive disorders’. It is not possible to determine from these data whether this is inappropriate clinical practice.
As the listing is based on clinical trial data provided in premarketing applications by the manufacturing companies that apply to major depression defined rigorously by DSM-IV criteria, this raises issues about the costeffectiveness of prescribing of antidepressants in practice.
Conclusions
General practitioners are the major providers of treatment for depression in Australia. When writing prescriptions for tricyclic antidepressants GPs use lower than recommended doses for major depression, however, most management in primary care is not for conditions regarded by the GP as major depression. A significant number of prescriptions for the newer antidepressants may not accord with the PBS restrictions for use.
Footnotes
Acknowledgements
We thank Josephine Farrugia of the Health Insurance Commission for information on PBS authority approvals and Stephanie Knox from the Family Medicine Research Centre for providing data relating to the SAND prescriber surveys.