
Abstract
Objective:
The aim of the current study was to examine the rates of violence prior to and 3 years following treatment initiation, and predictors of post-treatment violence in Chinese young people presenting with first-episode psychosis (FEP).
Method:
Seven hundred patients aged 15–25 years consecutively enrolled in a territory-wide early intervention program for FEP in Hong Kong from July 2001 to August 2003 were studied. Socio-demographic, pre-treatment, baseline and 3-year follow-up variables were collected via systematic medical file review. Violent behavior was defined as physical aggression towards people and was further categorized at two levels of severity.
Results:
After onset of psychosis, 6.7% (n = 47) patients exhibited violence before treatment. During 3-year treatment period, 9.4% (n = 66) committed violent behavior and 4.3% (n = 30) perpetrated serious violence. Two-fifths (40.4%) of patients who displayed pre-treatment violent behavior engaged in further act of violence after service contact. Multivariate regression analysis showed that previous violence, male gender and lower educational attainment were significantly associated with an increased risk of violence during 3-year follow-up. Comorbid substance, male gender, lower educational level and past history of violence were found to independently predict occurrence of serious violence after commencement of treatment for FEP.
Conclusions:
In a large representative cohort of Chinese young FEP patients, the rates of violent behavior before and after treatment were relatively lower than that reported in the literature. Risk factors for violence identified by the current study were comparable to the findings of previous research conducted in western populations. Close monitoring of patients with history of violence and specific treatments targeting at minimizing substance abuse may facilitate early identification and intervention of high-risk cases to reduce violence risk in the early course of illness.
Introduction
Psychotic disorders including schizophrenia are associated with an elevated risk of violence (Douglas et al., 2009; Fazel et al., 2009). Emerging evidence indicates that a first-episode psychosis (FEP) may represent a particularly high-risk period for the occurrence of violence (Nielssen and Large, 2010; Winsper et al., 2013a) including homicide (Nielssen and Large, 2010) when compared to other stages of the illness. Previous research on FEP showed that the prevalence of violence prior to service contact ranged between 10.5% and 43.5% (Coid et al., 2013; Crebbin et al., 2008; Foley et al., 2005; Harris et al., 2010; Johnstone et al., 1986; Milton et al., 2001; Payne et al., 2005; Verma et al., 2005; Volavka et al., 1997). A recent meta-analysis revealed that 34.5% of FEP patients perpetrated violent behavior before or upon presentation to psychiatric services (Large and Nielssen, 2011). Another meta-analytic review also confirmed high rates of violence in first-episode populations, with 28% and 31% of the patients committing violent acts before and after treatment initiation, respectively (Winsper et al., 2013a). Accumulating data suggest that violence in FEP is frequently, although not consistently, found to be related to a past history of violence, comorbid substance abuse, male gender, lower educational attainment and hostility (Large and Nielssen, 2011). Mixed results were noted regarding the relationships of violence with the duration of untreated psychosis (DUP) and positive symptoms, with some reports demonstrating that these variables were linked to violence (Coid et al., 2013; Verma et al., 2005; Volavka et al., 1997; Winsper et al., 2013b) but not others.
It should be noted that despite its profound clinical implications, particularly in the early course of psychotic illness, relatively few studies have been conducted to examine the rate and risk factors of violence in FEP. It is also worth noting that there was a marked discrepancy in violence rates among those few first-episode reports. This may, in fact, be partly attributable to methodological variations across studies. First, violence was defined variably among previous studies. Some investigators restricted the definition of violent behavior to physical aggression toward people (Coid et al., 2013; Milton et al., 2001; Verma et al., 2005; Volavka et al., 1997; Winsper et al., 2013b), while others adopted a broader construct in operationalizing violence which also included aggression against self, property or animals, or verbal threats without using a weapon (Crebbin et al., 2008; Dean et al., 2007; Foley et al., 2005; Harris et al., 2010; Humphreys et al., 1992; Payne et al., 2005; Spidel et al., 2010; Steinert et al., 1999). Second, various methods of violence assessment have been employed by different studies with some using medical record review (Bhugra et al., 2000; Crebbin et al., 2008; Foley et al., 2005; Payne et al., 2005; Steinert et al., 1999), while others relied mainly on self-report questionnaires (Spidel et al., 2010; Verma et al., 2005), informant reports (Volavka et al., 1997) or administering structured instruments to ascertain the occurrence of violent incidents (Coid et al., 2013; Dean et al., 2007; Harris et al., 2010; Milton et al., 2001; Winsper et al., 2013b). Third, time intervals for assessing pretreatment violence varied considerably among studies, ranging from 1 week preceding service contact (Foley et al., 2005) to a period extending before illness onset (Verma et al., 2005; Volavka et al., 1997). Fourth, substance-induced psychosis has been included in some studies (Crebbin et al., 2008; Foley et al., 2005; Harris et al., 2010) and may thus confound the results on violence rate. Conversely, several studies only recruited patients with schizophrenia (Bhugra et al., 2000; Humphreys et al., 1992; Johnstone et al., 1986; Steinert et al., 1999; Volavka et al., 1997). As an initial diagnosis of FEP is relatively unstable with subsequent diagnostic change commonly occurring in the first few years after illness onset (Chang et al., 2009), it is thus suggested that studying a sample with a broader spectrum of psychotic disorders would provide a more accurate estimation of the prevalence of violence and its associated factors.
Thus far, the majority of first-episode studies focused on examining violence occurring before or at the time of presentation to psychiatric service. Very few studies have been conducted to investigate the rate and predictors of violent behavior in FEP patients after treatment initiation (Crebbin et al., 2008; Milton et al., 2001; Spidel et al., 2010; Steinert et al., 1999; Winsper et al., 2013b), with most having follow-up duration of less than 2 years (Crebbin et al., 2008; Spidel et al., 2010; Winsper et al., 2013b). Hence, it is suggested that more longitudinal research should be carried out to clarify the risk profiles of violence occurring following the commencement of treatment for FEP (Winsper et al., 2013a). Alternatively, among those few studies that investigated violence in first-episode samples, most, if not all, were conducted in Western populations. As socio-cultural and health-care system contextual factors may have impact on the risk of violence in FEP, whether these findings could be generalized to different ethno-cultural backgrounds have not been fully explored.
To this end, we report a 3-year follow-up study in a large representative cohort of Chinese young people presenting with FEP to a comprehensive early intervention program in Hong Kong with an aim to (1) examine the prevalence of violent behavior prior to and 3 years following service enrollment and (2) to identify pretreatment and early illness predictors of post-treatment violent behavior over a 3-year follow-up period.
Materials and methods
Participants and setting
The initial sample comprised 839 patients who were consecutively enrolled in the Early Assessment Service for Young people with psychosis (EASY) program from July 2001 to August 2003. Since 2001, this publicly funded specialized program has been providing early assessment and phase-specific intervention to all individuals aged 15–25 years experiencing their FEP in Hong Kong (Tang et al., 2010). The program consists of five treatment teams covering the whole territory of Hong Kong with a population of approximately 7 million and over 95% of the population being Han Chinese. The service adopts a case–management approach and assertively follows up patients for the first 3 years after their initial episode (including follow-up in a transitional step-down clinic in year 3). Standardized clinical assessments evaluating the onset and development of psychosis, symptom profiles, risk behaviors and psychosocial functioning are performed on each patient. Multidisciplinary case reviews are held regularly for close monitoring of each patient’s clinical progress and treatment outcome. Patients are discharged to generic psychiatric services at the end of the program.
In this study, we excluded patients who had mental retardation, psychotic disorders due to general medical condition or substance-induced psychosis. Individuals with more than 1 month of psychiatric treatment before presentation to the program were not recruited. Patients with incomplete or missing medical files were also excluded. Of the initial cohort, 700 participants fulfilled the inclusion criteria and were retained as the study sample. This study was part of a large-scale historical-control study evaluating the effectiveness of the EASY program (Chen et al., 2011). The findings on gender differences, prediction of remission and recovery, relationship between DUP and treatment outcome and risk factors of suicidal behavior in 700 first-episode patients who received treatment in the EASY program have been reported elsewhere (Chang et al., 2011, 2012a, 2012b, 2015). The study was approved by the local research and ethics committees.
Assessments and procedure
Participants’ baseline and follow-up variables were obtained via systematic record review. For each participant, outpatient and inpatient medical records and computerized clinical information from medical database were retrieved. Trained research assistants acquired the data from medical files according to a protocol designed specifically for data collection in this study. Standardized data entry forms were used to systematically extract intake, treatment and follow-up variables from consecutive medical files. Weekly consensus meetings were held throughout the period of data collection to ensure strict adherence to protocol and to resolve ambiguity in clinical information during the data acquisition process. Only the data that could be reliably extracted from records were targeted for retrieval and analysis. Validity and inter-reliability for major variables including DUP and outcome measures were evaluated using intraclass correlation coefficient (ICC). Validity compared ratings between an experienced psychiatrist and research staff (ranging from 0.78 to 1.00). Interrater reliability compared ratings between research staff (ranging from 0.70 to 1.00). Both validity and interrater reliability exercises yielded satisfactory levels of concordance.
Socio-demographic data included gender, age at service entry, educational level and occupational status. Pretreatment illness characteristics included past history of suicide attempt and substance abuse and previous violence committed during DUP. Baseline clinical characteristics included age and mode of onset of first psychotic episode and DUP which was defined as the time interval between the onset of positive psychotic symptoms and first contact with a psychiatric service. Acute onset was defined as the development of a psychotic episode from the first noticeable behavioral change occurring within 1 month. Following the method used by previous research (Conus et al., 2007), severity of positive and negative symptoms at entry was assessed using Clinical Global Impression–Severity of Illness Scale (CGI-S; Guy, 1976). Functioning at intake was measured by Social and Occupational Functioning Assessment Scale (SOFAS; Goldman et al., 1992). Data on service utilization including hospitalization status at the first month of treatment and length of stay in the service were obtained. Diagnostic assignment of individual participant was based on a longitudinal approach taking into consideration the fact that diagnostic change may take place over time (Chang et al., 2009). In the EASY program, diagnosis of each case was derived from consensus results of interdisciplinary conference utilizing multiple sources of information, and regular diagnostic reviews were undertaken to incorporate additional clinical information emerging along the course of illness. In this study, the final 3-year clinical diagnosis based on International Classification of Diseases-10 (ICD-10) criteria (World Health Organization, 1992) was thus ascertained as the participant’s research diagnosis. Comorbid substance abuse during follow-up was also recorded.
The status and nature of post-treatment violent behavior, which was documented and regularly updated in standardized EASY clinical assessment forms by treating clinicians and case managers using multiple sources of information including patient interviews, informant reports and police records, were examined via systematic medical file review. Violent behavior was defined as ‘an act involving use of physical force which is intended to hurt or injure another person’ (Serper, 2011) and was further categorized into two levels of severity based on MacArthur Violence Risk Assessment Study (Steadman et al., 1998). Serious violence referred to an assault resulting in injury or involving the use of a weapon, threat with a weapon or sexual assault. Other violence referred to an assault without injury or weapon use. In this study, aggression against self or property or verbal threats without an accompanying weapon was not considered violent behavior.
Statistical analysis
The primary analysis of this study focused on identifying pretreatment and early illness variables that predicted the occurrence of violent behavior during a 3-year follow-up in the EASY program. First, a series of logistic regression analyses was conducted with violence (i.e. participants with vs without violent behavior) during a 3-year treatment period as the dependent variable, demographic, pretreatment and baseline illness variables as candidate predictors and length of time in the service (which varied with individual participant) as a covariate. Second, those variables that showed p value < 0.10 in the preceding regression analyses were then entered into a multivariate logistic regression model with length of time in the service as a covariate to identify independent predictors of occurrence of violent behavior over 3 years based on Wald statistics (odds ratios with 95% confidence levels were computed). To assess potential attrition bias, baseline differences between completer and noncompleter groups were evaluated using chi-square test and independent t-test as appropriate. DUP was log-transformed due to its skewed distribution. The level of statistical significance was set at p < 0.05.
Results
Characteristics of the sample
A total of 700 participants were included in the study and 51.4% (n = 360) were male. The mean age of the sample at intake was 21.2 years (standard deviation [SD] = 3.4 years), and the average educational level was 10.9 years (SD = 2.3). The median DUP of the sample was 91 days (mean = 239.8 days, SD = 373.4 days). Schizophrenia was the most common diagnosis which accounted for 65.9% (n = 461) of the sample. For other diagnostic entities, 11.9% of the cohort had affective psychosis (bipolar affective disorder with psychotic features n = 54, depression with psychotic features n = 29), 3.9% had schizoaffective disorder (n = 27), 12.4% had acute and transient psychotic disorders (n = 87) and 6.6% had unspecified nonorganic psychosis (n = 46). Attrition analyses revealed no significant differences between 3-year follow-up completers (n = 539, 77%) and noncompleters on socio-demographics, DUP and other baseline characteristics, with the exception of diagnosis. Participants who completed follow-up were more likely to have schizophrenia-spectrum disorder (schizophrenia and schizoaffective disorder) when compared with those who were disengaged from service (χ2 = 18.9, p < 0.001).
Prevalence of violent behavior
A total of 47 patients (6.7%) had committed violent behavior prior to entry to the EASY program. A total of 66 patients (9.4%) exhibited violent behavior during the 3-year follow-up and 4.3% of the cohort (n = 30) perpetrated serious violence (Table 1). Of the 47 patients who had a history of pretreatment violence, 40.4% (n = 19) engaged in further violent act during the 3-year treatment period. In total, 87 violent acts were identified among 66 patients who displayed violence after service entry. Most patients had committed violent behavior on one occasion (n = 53, 80.3%), nine (13.6%) had two violent acts and four (6.1%) had three or more violent incidents.
Prevalence of violent behaviors in patients with first-episode psychosis.
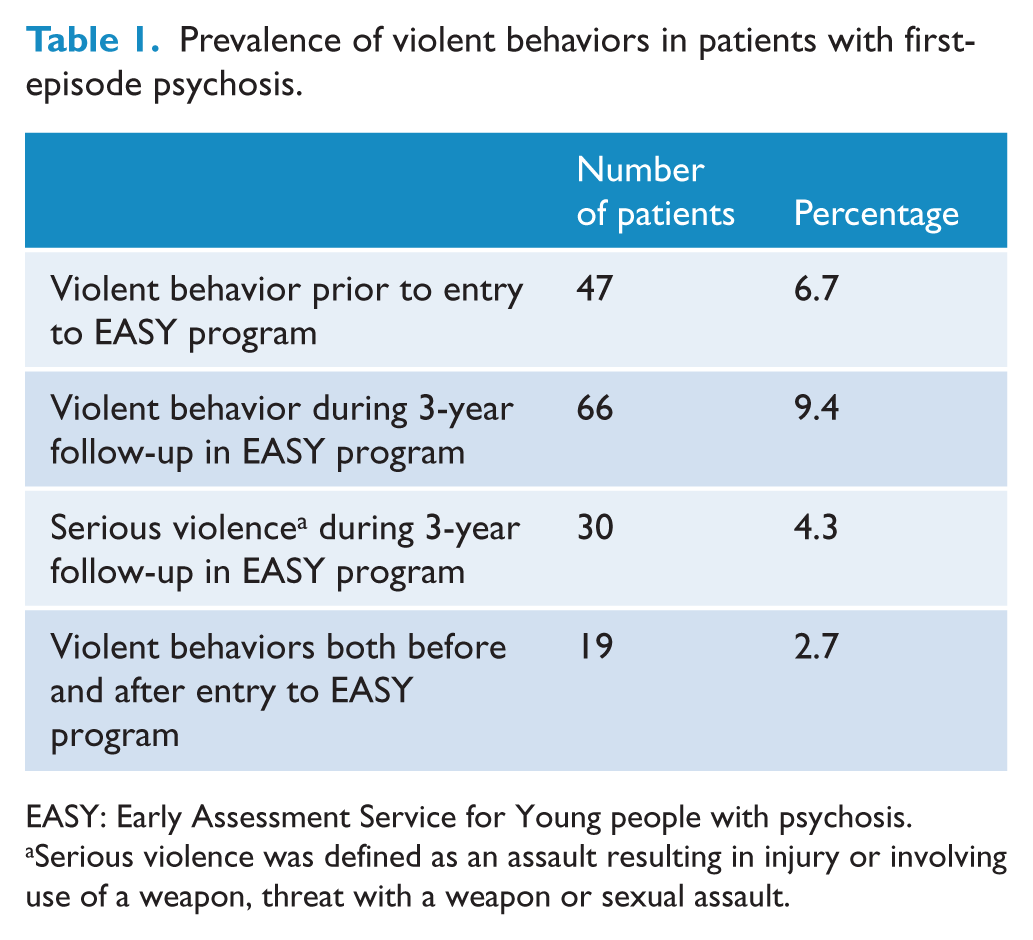
EASY: Early Assessment Service for Young people with psychosis.
Serious violence was defined as an assault resulting in injury or involving use of a weapon, threat with a weapon or sexual assault.
Predictors of violent behavior
As shown in Table 2, the occurrence of any violent behavior during the 3-year treatment period was significantly associated with male gender, lower educational attainment, unemployment at entry, history of suicide attempt, violence and substance abuse prior to service enrollment, involuntary admission at presentation, poorer baseline functioning and comorbid substance abuse during follow-up. Multivariate logistic regression analysis revealed that male gender, lower educational level and pretreatment violence independently predicted violent behavior (Table 3). Table 4 summarizes the differences between patients with and without serious violence in terms of demographics, pretreatment characteristics and baseline clinical variables. Patients who exhibited post-treatment serious violence were more likely to be male, to have fewer years of education, history of suicide attempt, violence and substance abuse before treatment and comorbid substance abuse during follow-up. Multivariate regression analysis showed that male gender, lower educational attainment, previous violence and comorbid substance abuse predicted the occurrence of serious violence (Table 5).
Demographics, pretreatment and clinical predictors of violent behavior in patients with first-episode psychosis.
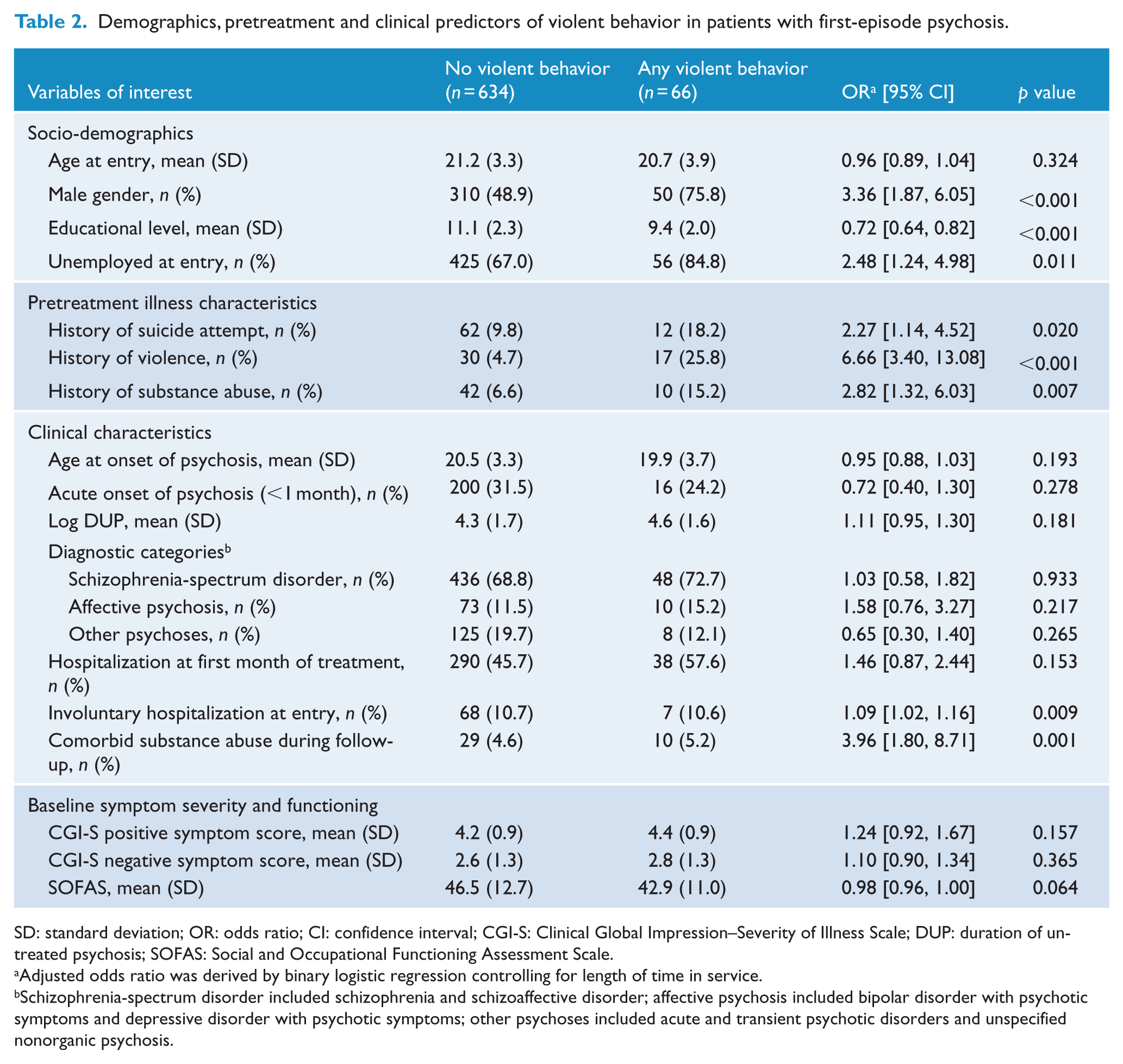
SD: standard deviation; OR: odds ratio; CI: confidence interval; CGI-S: Clinical Global Impression–Severity of Illness Scale; DUP: duration of untreated psychosis; SOFAS: Social and Occupational Functioning Assessment Scale.
Adjusted odds ratio was derived by binary logistic regression controlling for length of time in service.
Schizophrenia-spectrum disorder included schizophrenia and schizoaffective disorder; affective psychosis included bipolar disorder with psychotic symptoms and depressive disorder with psychotic symptoms; other psychoses included acute and transient psychotic disorders and unspecified nonorganic psychosis.
Multivariate logistic regression analysis for predictors of violent behavior in patients with first-episode psychosis.
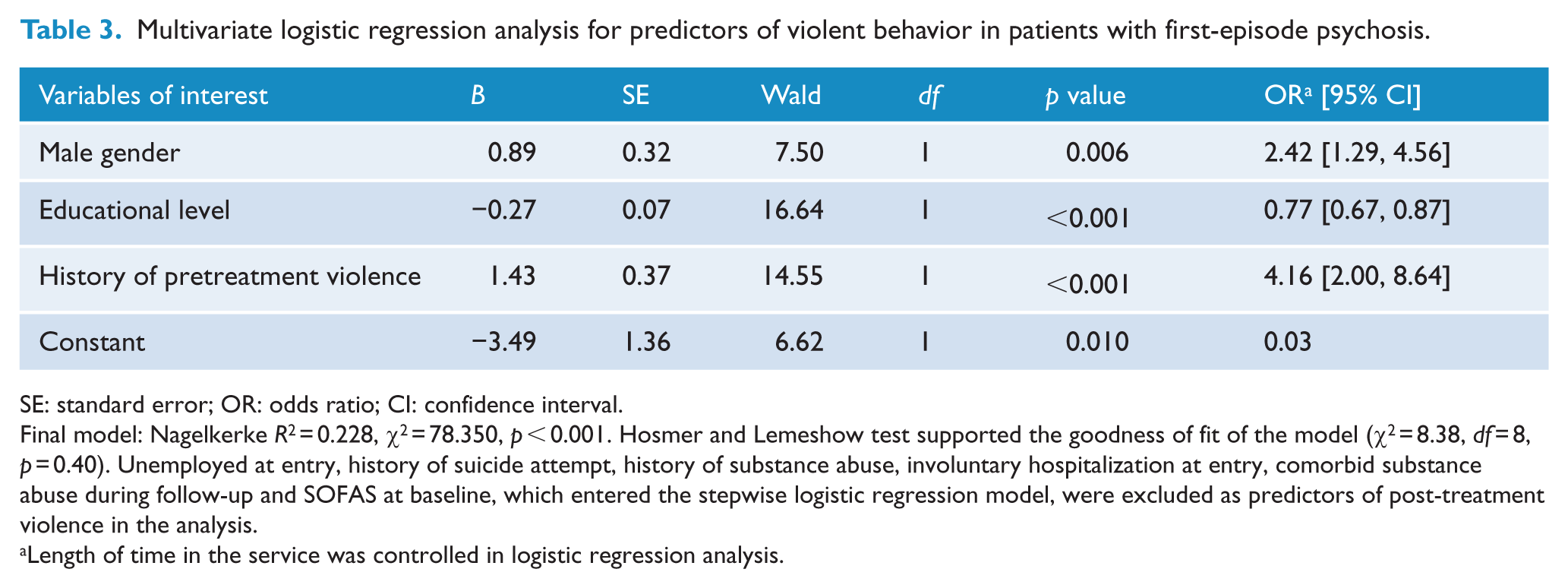
SE: standard error; OR: odds ratio; CI: confidence interval.
Final model: Nagelkerke R2 = 0.228, χ2 = 78.350, p < 0.001. Hosmer and Lemeshow test supported the goodness of fit of the model (χ2 = 8.38, df = 8, p = 0.40). Unemployed at entry, history of suicide attempt, history of substance abuse, involuntary hospitalization at entry, comorbid substance abuse during follow-up and SOFAS at baseline, which entered the stepwise logistic regression model, were excluded as predictors of post-treatment violence in the analysis.
Length of time in the service was controlled in logistic regression analysis.
Demographics, pretreatment and clinical predictors of serious violence in patients with first-episode psychosis.
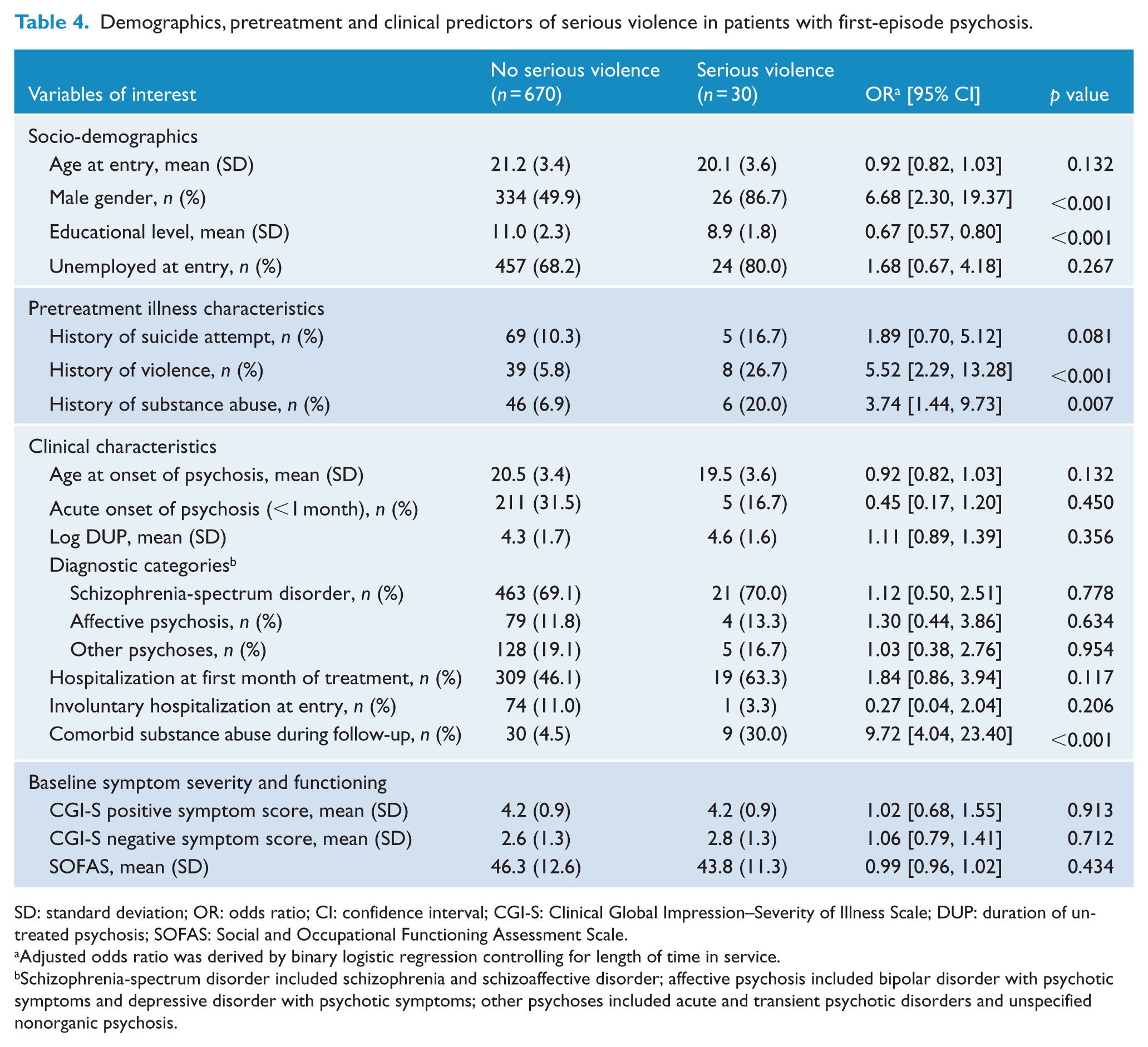
SD: standard deviation; OR: odds ratio; CI: confidence interval; CGI-S: Clinical Global Impression–Severity of Illness Scale; DUP: duration of untreated psychosis; SOFAS: Social and Occupational Functioning Assessment Scale.
Adjusted odds ratio was derived by binary logistic regression controlling for length of time in service.
Schizophrenia-spectrum disorder included schizophrenia and schizoaffective disorder; affective psychosis included bipolar disorder with psychotic symptoms and depressive disorder with psychotic symptoms; other psychoses included acute and transient psychotic disorders and unspecified nonorganic psychosis.
Multivariate logistic regression analysis for predictors of serious violence in patients with first-episode psychosis.
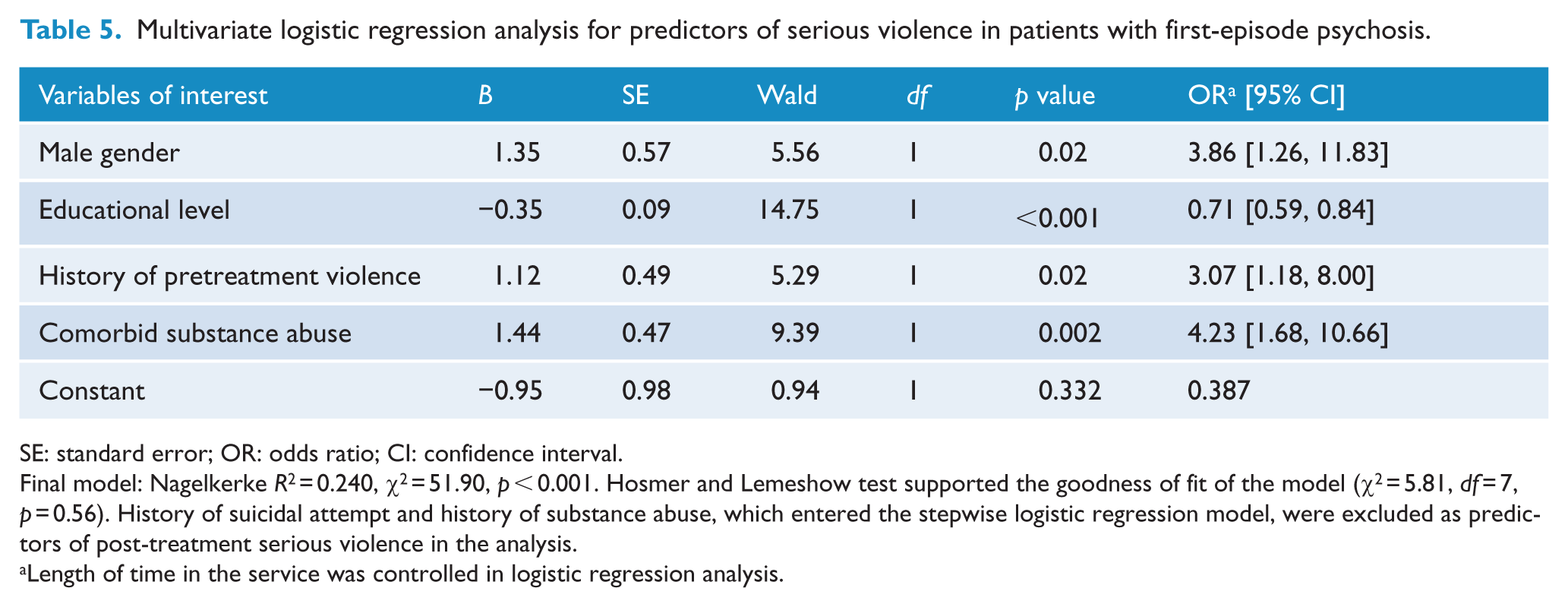
SE: standard error; OR: odds ratio; CI: confidence interval.
Final model: Nagelkerke R2 = 0.240, χ2 = 51.90, p < 0.001. Hosmer and Lemeshow test supported the goodness of fit of the model (χ2 = 5.81, df = 7, p = 0.56). History of suicidal attempt and history of substance abuse, which entered the stepwise logistic regression model, were excluded as predictors of post-treatment serious violence in the analysis.
Length of time in the service was controlled in logistic regression analysis.
Discussion
Our results indicated that 6.7% of FEP patients had committed violence before treatment. During a 3-year follow-up, 9.4% of our cohort exhibited violent act and 4.3% perpetrated serious violence. The violence rates of our FEP cohort are thus comparatively lower than that reported in the literature. It should be noted that it may be difficult to directly compare our results with previous findings due to substantial methodological heterogeneity across studies. Alternatively, there are several possible explanations for our relatively low prevalence of violent behavior. First, we defined violence narrowly to indicate physical aggression toward people, whereas many studies have incorporated a wider range of aggressive behavior including those with a milder degree of severity in coding violence and may thus generate higher occurrence of violent incidents. Second, comorbid substance abuse, which was consistently shown to be a key risk factor of violence in psychosis (Douglas et al., 2009; Witt et al., 2013), was much less frequently observed in our cohort (5.6%) when compared to those first-episode populations in Western countries and may, therefore, partly contribute to our low prevalence estimates on violence. This also echoes the findings of a previous local population-based study which revealed low prevalence of substance abuse in Hong Kong (male: 5%, female: 1.8%; Lau et al., 2005). Third, the relatively low violence rate in our sample is in parallel with and may, in fact, reflect the lower rate of violent crimes in Hong Kong as compared to many other jurisdictions (Broadhurst et al., 2007). Of note, thus far, only five studies have been conducted that examined post-treatment violence in FEP with its prevalence ranging between 12% and 42.7% (Crebbin et al., 2008; Milton et al., 2001; Spidel et al., 2010; Steinert et al., 1999; Winsper et al., 2013b). One study assessed violence only in patients who had readmissions during follow-up (Steinert et al., 1999), thereby introducing bias by excluding patients who had milder illness without requiring inpatient treatment. It may also raise the likelihood of detecting violent incidents which may have precipitated hospitalization and hence may generate an inflated estimate of the violence rate. In fact, our finding on post-treatment violence rate is largely consistent with two other FEP studies (with violence rates of 12% and 13.7%, respectively; Crebbin et al., 2008; Winsper et al., 2013b). Our rate of serious violence is also comparable to that reported by the only FEP study which further classified post-treatment violence according to the severity of aggression (serious violence: 4.8%; Milton et al., 2001).
Our findings that previous violence, male gender and lower educational attainment predicted violent behavior at follow-up concur with recent reviews on risk factors for violence in schizophrenia (Bo et al., 2011) and several FEP studies that examined post-treatment violence (Milton et al., 2001; Steinert et al., 1999). In particular, our results that 40% of patients with pretreatment violence continued to exhibit violent behavior during a 3-year treatment period further highlight the clinical importance of intensive monitoring with regular systematic risk assessment of patients with a past history of violence to facilitate early identification of high-risk cases and prompt intervention for violence prevention. Notably, comorbid substance abuse, alongside the aforementioned risk factors for post-treatment violence, was found to predict serious violence during follow-up. This was in keeping with the literature showing a significant relationship between substance abuse comorbidity and heightened violence risk in patients with psychotic disorders (Douglas et al., 2009; Witt et al., 2013). Moreover, our findings suggest that concurrent substance abuse may confer an increased risk of committing serious violent behavior in FEP patients. It should be acknowledged that this observed association may be mediated by other putative risk factors of violence including personality traits and social adversity that are also linked to increased likelihood of substance abuse (Fazel et al., 2009) but were not measured in this study. In addition, alcohol and drug abuse might have differential effects on violence risk in FEP. Although a meta-analysis examining the risk factors for violence among patients at various stages of psychotic illness found that both alcohol and drug abuse were associated with an increased violence risk (Witt et al., 2013), the results were relatively less consistent in first-episode populations. Some FEP studies revealed that drug but not alcohol abuse was associated with violence (Dean et al., 2007; Foley et al., 2005; Harris et al., 2010) while others suggested otherwise (Steinert et al., 1999; Volavka et al., 1997), and a recent meta-analytic review of FEP patients showed that drug but not alcohol abuse predicted violent behavior (Large and Nielssen, 2011). As we evaluated comorbid substance abuse using a composite measure without further categorizing into alcohol and drug misuse, their potential differential relationships with violence could not be examined in this study. Notwithstanding this, our results underscore the clinical significance of incorporating specific treatment strategies targeting at minimizing substance abuse, which is a potentially modifiable risk factor, into early intervention service to lower the risk of violence in FEP patients.
Although prolonged DUP has been shown to be associated with violence occurring during the pretreatment period (Nielssen and Large, 2010), our finding of a lack of any relationship between DUP and post-treatment violence was, however, in accord with the results of most previous studies examining the risk factors of violence in FEP after treatment initiation (Crebbin et al., 2008; Milton et al., 2001; Spidel et al., 2010; Steinert et al., 1999). We also failed to find any significant difference between patients with and without violent behavior during follow-up with respect to positive symptom severity at entry. Our finding is thus contrary to some but not all (Appelbaum et al., 2000; Bo et al., 2011) studies which otherwise suggested that specific constellations of psychotic symptoms such as persecutory delusions (Coid et al., 2013; Swanson et al., 2006), threat or control-override symptoms (Link et al., 1998) or command hallucinations (McNiel et al., 2000) might increase violence risk. One possible explanation for our negative finding was that positive symptoms were rated by CGI-S based on medical record review which generated a global rating only and thus may not be sensitive enough to adequately capture the range of symptom severity and could not be able to identify any differential relationships of individual positive symptoms with violence. It might also be plausible that the effects of positive symptoms on violence could be better elucidated when temporal proximity between active psychosis and occurrence of violent incidents is taken into consideration. In fact, one recent FEP study revealed a strong relationship between serious violence and active delusions implying threat, with such association being mediated by angry affect (Coid et al., 2013). As the occurrence of violence in our FEP cohort was ascertained over a 3-year treatment period while symptom severity was evaluated at baseline, the dynamic nature of active psychotic symptoms and their proximal impacts on precipitating violence could not be adequately addressed in our study.
There are several limitations in the study. First, the study was based on medical file review which may be biased by varying degrees of documentation quality. As the EASY program adopts a case–management approach in which the same clinical team follows through the patients in the first 3 years of treatment, the quality of clinical documentation of the study sample was, therefore, relatively more homogeneous than other comparable retrospective record review using clinical data from generic psychiatric services. Besides, as clinical presentation and treatment progress of each participant enrolled in the program was thoroughly assessed and closely monitored, and all available sources of information were ascertained via multidisciplinary input, the possibility of missing relevant clinical and violence-related data for case notes documentation was minimized. Moreover, errors in data extraction might be further reduced via close scrutiny of data acquisition and rating processes by regular consensus meetings. Second, similar to previous research examining violence, our study was subject to underreporting of violent incidents, particularly those emerging during the pretreatment period as violent behavior following service contact would be more likely to be identified due to increased clinical monitoring (Winsper et al., 2013a). Additionally, as the literature indicates that family members were the most likely targets of violence perpetuated by patients with psychotic disorders (Steadman et al., 1998), the cultural inhibition of Chinese people on reporting violence occurring within the family (Chan et al., 2008) might, therefore, lead to an underestimation of the violence rate in our cohort. Third, we had no access to official criminal records for violent offenses and the violence rate might thus be underestimated. Moreover, certain individuals with untreated FEP who have committed very serious violence may be managed in forensic settings instead of entering the EASY program and could not be included in the study. Fourth, structured violence assessment instruments which were found to be more sensitive in ascertaining violent incidents (Winsper et al., 2013a) were not used in this study. Fifth, our study did not include measures for personality disorders and antisocial traits, childhood conduct problems and prior victimization which were found to be related to increased violence risk (Nolan et al., 1999; Spidel et al., 2010; Swanson et al., 2006).
In conclusion, our results show that in a large representative cohort of Chinese young people presenting with FEP to a territory-wide early intervention program in Hong Kong, violence was not an uncommon event occurring before and after service entry. Around 1 in 10 committed violent behavior in the initial 3 years of treatment. Previous violence, male gender and lower educational attainment were found to predict post-treatment violence, and comorbid substance abuse was specifically more related to serious violence. As accumulating evidence indicates a high violence rate during FEP with a lack of significant risk reduction following service contact (Winsper et al., 2013a), along with a recent debate regarding sustained efficacy and cost-effectiveness of early intervention for psychosis (Amos, 2012; McGorry and Mihalopoulos, 2013; Mihalopoulos et al., 2012; Raven, 2013), more intensive risk evaluation and psychosocial interventions should be incorporated into early intervention programs to further improve patients’ functional and clinical outcomes including minimization of violence risk. Owing to limited data on the risk factors for violence following treatment initiation for FEP, more longitudinal research adopting a prospective design should be conducted to examine both static and dynamic risk variables for post-treatment violence in first-episode samples. In addition, further investigation taking into consideration primary motivation for violence (Serper, 2011) and its temporal relationship with acute psychopathology (Coid et al., 2013; Douglas et al., 2009) is required to enhance prediction and hence risk management of future violent behavior in the early course of psychotic illness.
Footnotes
Acknowledgements
The authors would like to thank all coordinating clinicians and staff from the participating hospitals, clinics and medical records departments for their kind assistance.
Declaration of interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: E.Y.H.C. has participated in the paid advisory board for Otsuka, has received educational grant support from Janssen-Cilag and has received research funding from Astra-Zeneca, Janssen-Cilag, Eli Lilly, Sanofi-Aventis and Otsuka. The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This study was part of the historical case-controlled study of first-episode psychosis which was supported by a grant from the Health and Health Service Research Fund (03041041) of the Food and Health Bureau, the Government of the Hong Kong Special Administrative Region.