
Abstract
Objectives:
Cannabis use is prevalent among people with first episode psychosis and the epidemiology of its use in early psychosis is unclear. We performed a meta-analysis of observational studies to determine; (1) the interval between age at initiation of cannabis use and age at onset of first episode psychosis, (2) the prevalence of cannabis use at time of first episode psychosis, and (3) the odds of continuing cannabis following treatment for first episode psychosis.
Data sources:
Search of electronic databases MEDLINE, EMBASE, PsycINFO, Web of Science and CINAHL for English-language papers using search terms (psychosis OR schizophrenia) AND (cannabis OR marijuana) IN (title OR keyword OR abstract), current to October 2014.
Study selection:
Studies were included if they reported on prevalence of current cannabis use in first episode psychosis cohorts. A total of 37 samples were included for meta-analysis.
Data extraction:
Rates of cannabis use in each sample were extracted to determine prevalence estimates. The age at initiation of regular cannabis and age at onset of psychosis were used to determine the length of cannabis use preceding psychosis. Prevalence estimates at first episode psychosis and various time points of follow-up following first episode psychosis were analysed to determine odds ratio of continuing cannabis use. Data synthesis was performed using random-effects meta-analyses.
Results:
The pooled estimate for the interval between initiation of regular cannabis use and age at onset of psychosis was 6.3 years (10 samples, standardised mean difference = 1.56, 95% confidence interval = [1.40, 1.72]). The estimated prevalence of cannabis use at first episode psychosis was 33.7% (35 samples, 95% confidence interval = [31%, 39%]). Odds of continued cannabis use between 6 months and 10 years following first episode psychosis was 0.56 (19 samples, 95% confidence interval = [0.40, 0.79]).
Introduction
Cannabis use is prevalent among people with first episode psychosis (Baeza et al., 2009; Gonzalez-Pinto et al., 2011; Grech et al., 2005) and schizophrenia (Koskinen et al., 2010; Maremmani et al., 2004; Martinez-Arevalo et al., 1994; Negrete et al., 1986); however, the reasons for this association are unclear. Cannabis use is a risk factor for later psychosis, an association that is dose-dependent (Davis et al., 2013; Zammit et al., 2002), and is strengthened by initiation at a younger age (Arseneault et al., 2002) and use of high-potency cannabis preparations (Di Forti et al., 2014). Cannabis use is also associated with earlier age of psychosis onset (Large et al., 2011), and longitudinal studies suggest that continued cannabis use is associated with a poorer prognosis (Clausen et al., 2014; Faber et al., 2012; Grech et al., 2005). These observations imply that regardless of a potential aetiological association, cannabis use is a predictor of increased illness severity and may contribute substantially to disability associated with psychosis.
While there is substantial evidence from longitudinal cohort studies for a causal link between cannabis use and psychosis, such an association might be insufficient to account for the high prevalence of cannabis use by people with psychosis. It has been suggested that cannabis use may be a form of self-medication for negative and affective symptoms or for the side effects of anti-psychotic medications (Goswami et al., 2004). However, the relationship between cannabis use and psychosis is likely to be complex (Di Forti et al., 2007; Hall and Degenhardt, 2008; Radhakrishnan et al., 2014), potentially involving shared genetic factors (Power et al., 2014) and common psychological vulnerabilities (Burns, 2013). A shared predisposition to psychosis and cannabis use may explain the disappointing results of substance use interventions in this population (Bonsack et al., 2011; Hjorthoj et al., 2013; Smeerdijk et al., 2012).
The naturalistic methodology of studies reporting cannabis prevalence in psychotic illness is inherently prone to being confounded by socioeconomic, geographical and epidemiological differences in reported populations. Moreover, similar evidence reported for tobacco smoking has been shown to be liable to citation and reporting bias (Chapman et al., 2009). While there are a large number of studies reporting the epidemiology of cannabis use in psychosis, as yet there is no reported meta-analysis of these studies. A meta-analysis of relevant literature could clarify the temporal course of cannabis use in first episode psychosis by providing a quantitative synthesis of existing evidence and provide a means of examining factors that contribute to heterogeneity. In turn, this would inform ongoing debate regarding the role of cannabis in early psychosis, assist service planning and provide an epidemiological benchmark for future research.
Our aim was to estimate the following:
Length of time between age at initiation of cannabis use and the onset of psychosis (analysis of initiation);
Proportion of people with first episode psychosis who use cannabis at time of initial treatment (analysis of prevalence);
Longitudinal prevalence of cannabis use in cohorts of people followed up after first episode psychosis (analysis of continuation).
Methods
The methods are based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (Moher et al., 2009). The study was designed to be methodologically comparable to an earlier study of the course of tobacco use in first episode psychosis (Myles et al., 2012).
Searches
Systematic searches were conducted of English-language publications indexed in MEDLINE, EMBASE, CINAHL, PsycINFO and ISI Web of Science (Figure 1). The search terminology (psychosis OR schizophrenia) AND (cannabis OR marijuana) IN (title OR keyword OR abstract) was used. Preliminary searches found that cannabis use data reported in the body of some publications were not specified in title or abstract, and thus, our search strategy was kept deliberately broad. Therefore, all papers appearing to report on cannabis or substance use in first episode psychosis were examined in full text. The reference lists of included studies were hand-searched. Publications from non-peer-reviewed sources were not considered. We did not include ‘substance abuse’ as a search term because the vast majority of studies using this term in the title did not report detailed data on cannabis use and the few that did were identified in the searches we conducted by the keyword or abstract.
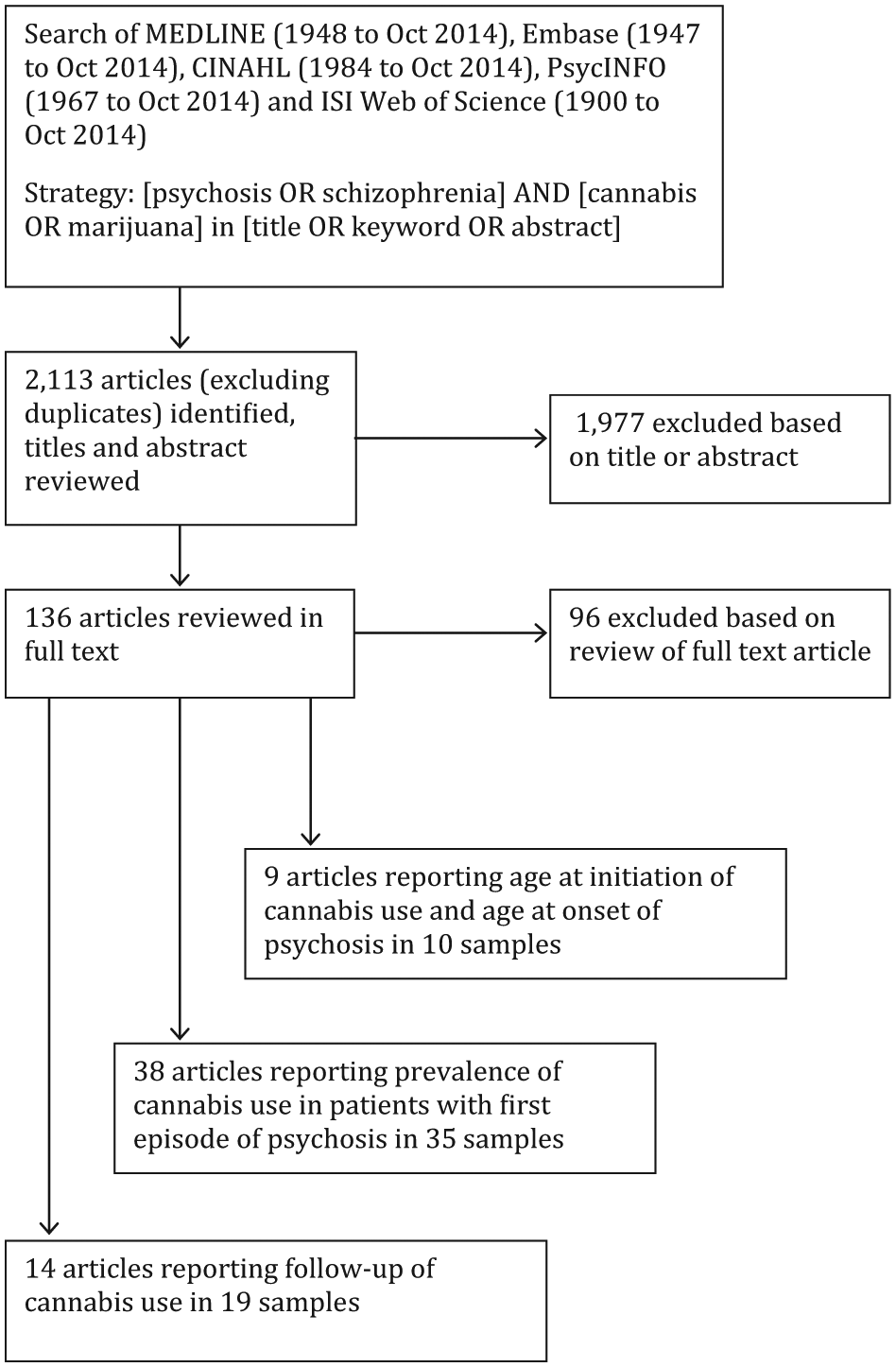
Flow chart of search strategy and results.
Inclusion and exclusion criteria
Samples were included if they
Reported on cohorts of subjects assessed at first episode of psychosis that was defined to include first episode schizophrenia, schizoaffective disorder, other schizophrenia-spectrum disorder, affective psychosis or psychosis not otherwise specified AND
Reported on the use of inhaled organic cannabis AND
Could be included in the meta-analysis of (a) cannabis initiation, (b) prevalence or (c) continuation if they reported (a) The mean age and standard deviation (SD) at onset of psychosis and at initiation of cannabis use, or other effect size data for this interval OR (b) Prevalence of cannabis use OR (c) Longitudinal data regarding proportions of subjects with initial and later use.
Samples were excluded if they reported on
Subjects who were not assessed at first episode of psychosis (to avoid recall bias in the meta-analysis of prevalence and continuation);
Subjects suffering from drug-induced or organic psychoses;
Subjects recruited by consenting to a clinical trial;
Subjects recruited as part of a randomised controlled intervention trial; these samples were excluded from the analysis of continuation;
Studied synthetic or oral cannabis;
Subjects or cohorts that were reported on in another more recent or larger publication.
Definitions of cannabis use and first episode psychosis
The definitions of current cannabis use were those used in the primary research. Of the 35 samples, 30 used cannabis use disorder as defined by Diagnostic and Statistical Manual of Mental Disorders (DSM) or International Classification of Diseases (ICD) criteria as the threshold for inclusion in the cannabis-using group. In samples where other clinical measures of cannabis use were reported, we considered regular monthly use as the minimum threshold for inclusion as a current user. Samples reporting subjects with intermittent or sporadic use that did not meet criteria for a cannabis use disorder, previous use more than a year prior to the first episode of psychosis or lifetime cannabis use, were excluded from analysis. Some studies reported urine toxicology to validate self-reported cannabis use status; however, this was not used as a measure in this meta-analysis as it may incorrectly classify active cannabis users as non-users due to delay between cannabis consumption and time of testing (Large et al., 2012).
First, episode psychosis was defined according to the primary research. Studies generally defined first episode psychosis as the period between the onset of positive symptoms and the end of a course of anti-psychotic treatment (Norman and Malla, 2001). We did not restrict our inclusion criteria to specific eventual diagnoses (e.g. schizophrenia, brief psychotic episode, bipolar affective disorder) as cases are typically undifferentiated at baseline and stratification at baseline is less likely to be relevant at a clinical or population level. Studies examining drug-induced or organic psychosis were not considered for inclusion, given they represent a different clinical entity to primary psychotic illnesses.
Data extraction
H.M. and N.M. independently extracted the data into an electronic spread-sheet, and disagreements were resolved by a joint examination of the papers. The following data were extracted:
Mean age and SD of age at regular cannabis use and age at onset of psychosis (analysis of initiation);
Proportion of cannabis users and sample size at admission for first episode of psychosis (analysis of prevalence);
Proportion of cannabis users at intervals of follow-up after initiation of treatment and the sample size at each interval of follow-up (analysis of continuation).
There were no disagreements in 10 data points extracted for the meta-analysis of initiation; there were eight disagreements in 35 prevalence data points and one disagreement in 19 continuation data points.
The following methodological characteristics were recorded:
The proportion of males in each sample;
The year in which the samples were collected;
The mean age of each sample;
The geographical region in which the sample was drawn;
Time point at follow-up (converted to months).
Meta-analysis
Meta-analytically estimated standardised mean difference (SMD), logit event rates and odds ratios were computed using Comprehensive Meta-Analysis Version 2 (Biostat, Englewood, NJ). Between-study heterogeneity was assessed using the I2 statistic, and between-group heterogeneity was assessed using the Q-value statistic. A random-effects meta-analysis was chosen for all analyses because of assumed differences between studies in patient groups and methods.
Publication bias
Potential publication bias was assessed using Egger’s test (Egger et al., 1997). Duval and Tweedie’s (2000) trim and fill method was used to examine the possible effect of hypothetically missing samples on the pooled estimate of effect.
Sub-group analysis and meta-regression
Between-study heterogeneity might be associated with sample characteristics and the time and place of the study. Meta-regression or sub-group analysis was used to examine between-study heterogeneity in effect size associated with the following:
Proportion of patients in each study who were male, because men are generally more likely to use cannabis than women;
Mean age of patients in each sample because younger subjects are more likely to use cannabis than older patients;
Geographical region of the study, because prevalence and initiation of cannabis use vary between regions;
Year in which data for each study were collected, because prevalence of cannabis use may have declined or increased over time.
Results
Searches
The number of samples included in each meta-analysis is outlined in Figure 1, and descriptions of each study are outlined in the Supplementary Appendix. Samples specific to each analysis included the following:
A total of 10 data samples reported in nine papers with a total sample size of 796 subjects (mean per sample = 88.4, SD = 33.4) were included in the analysis of initiation.
A total of 35 samples reported in 38 papers with a total sample size of 6321 subjects (mean per sample = 180.6, SD = 137.7) were included in the analysis of prevalence.
A total of 19 samples reported in 14 papers with a total sample size of 3645 subjects (mean per sample = 191.8, SD = 106.5) were included in the analysis of continuation.
Meta-analysis
Analysis of initiation
Meta-analysis of initiation found that regular cannabis use begins at 6.3 years before age at onset of psychosis (SMD = 1.56, 95% confidence interval [CI] = [1.40, 1.72]; see Figure 2). Heterogeneity was moderate and statistically significant (Q = 17.85, df(Q) = 9, p = 0.04, I2 = 49.6) (see Table 1).
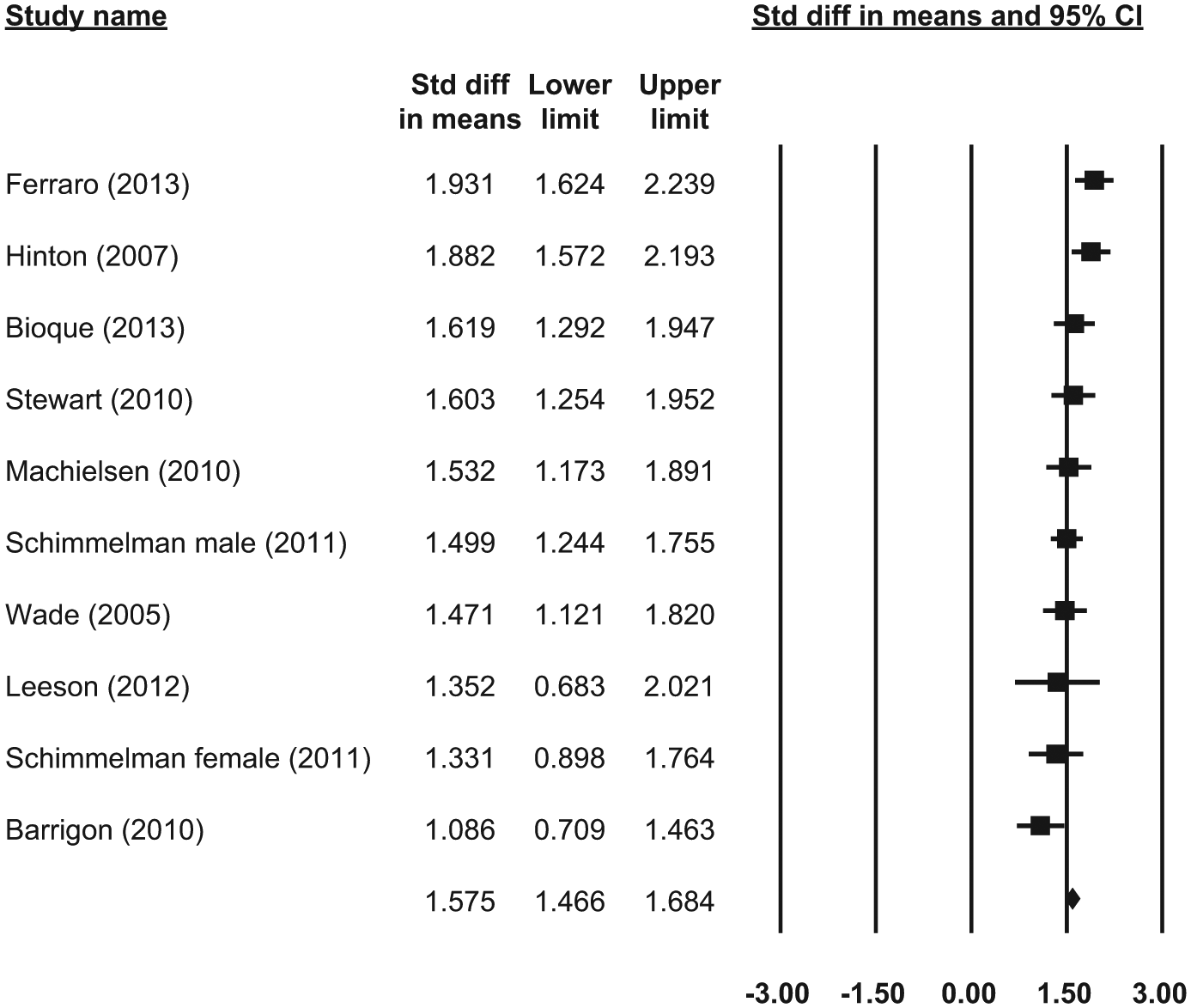
Forrest plot of meta-analysis of initiation.
Meta-analysis of initiation.
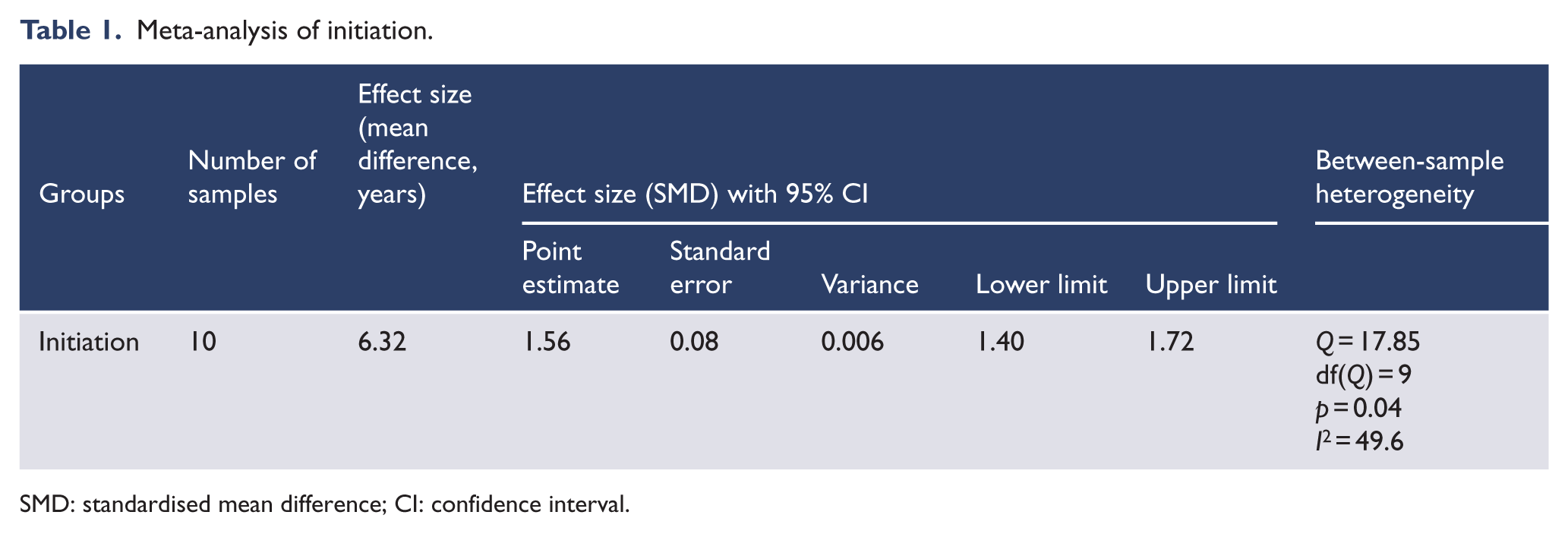
SMD: standardised mean difference; CI: confidence interval.
There was little evidence of publication bias. Egger’s test did not demonstrate any evidence of bias (intercept = −2.48, standard error [SE] = 2.09, p = 0.27). Trim and fill analysis identified three samples that may have biased the results to a smaller estimate. The exclusion of these studies increased the SMD from 1.56 to 1.65 with wider CIs (95% CI = [1.48, 1.82]) equating to an increased interval of 9 months.
Analysis of prevalence
Meta-analysis of prevalence indicated 33.7% (95% CI = [29%, 38%]) of subjects used cannabis at the time of first episode psychosis (see Figure 3). There was a high degree of between-study heterogeneity (Q = 430.4, df(Q) = 34, p < 0.001, I2 = 92.1; see Table 2).
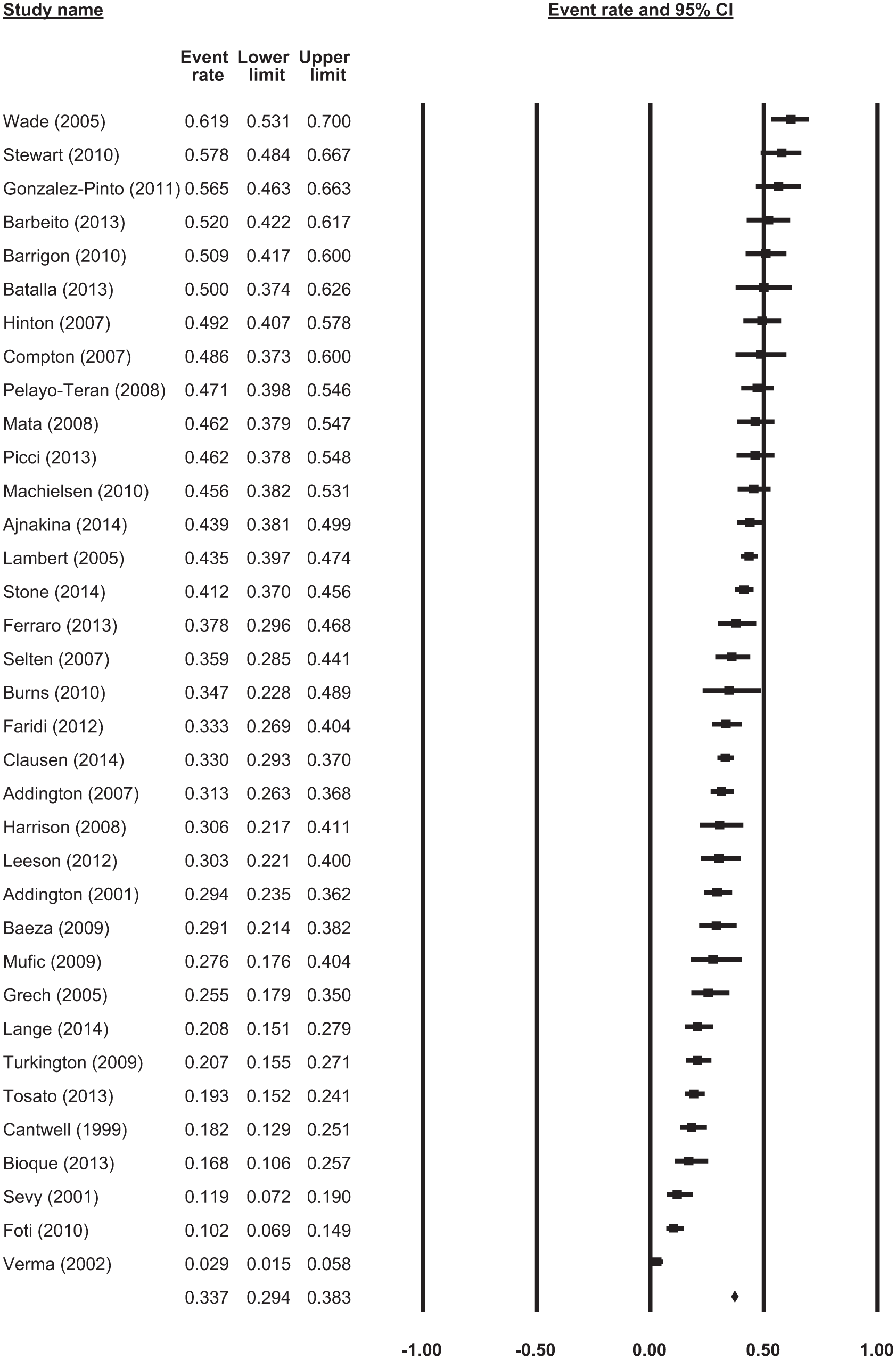
Forrest plot of meta-analysis of prevalence.
Sub-group analysis for meta-analysis of prevalence.
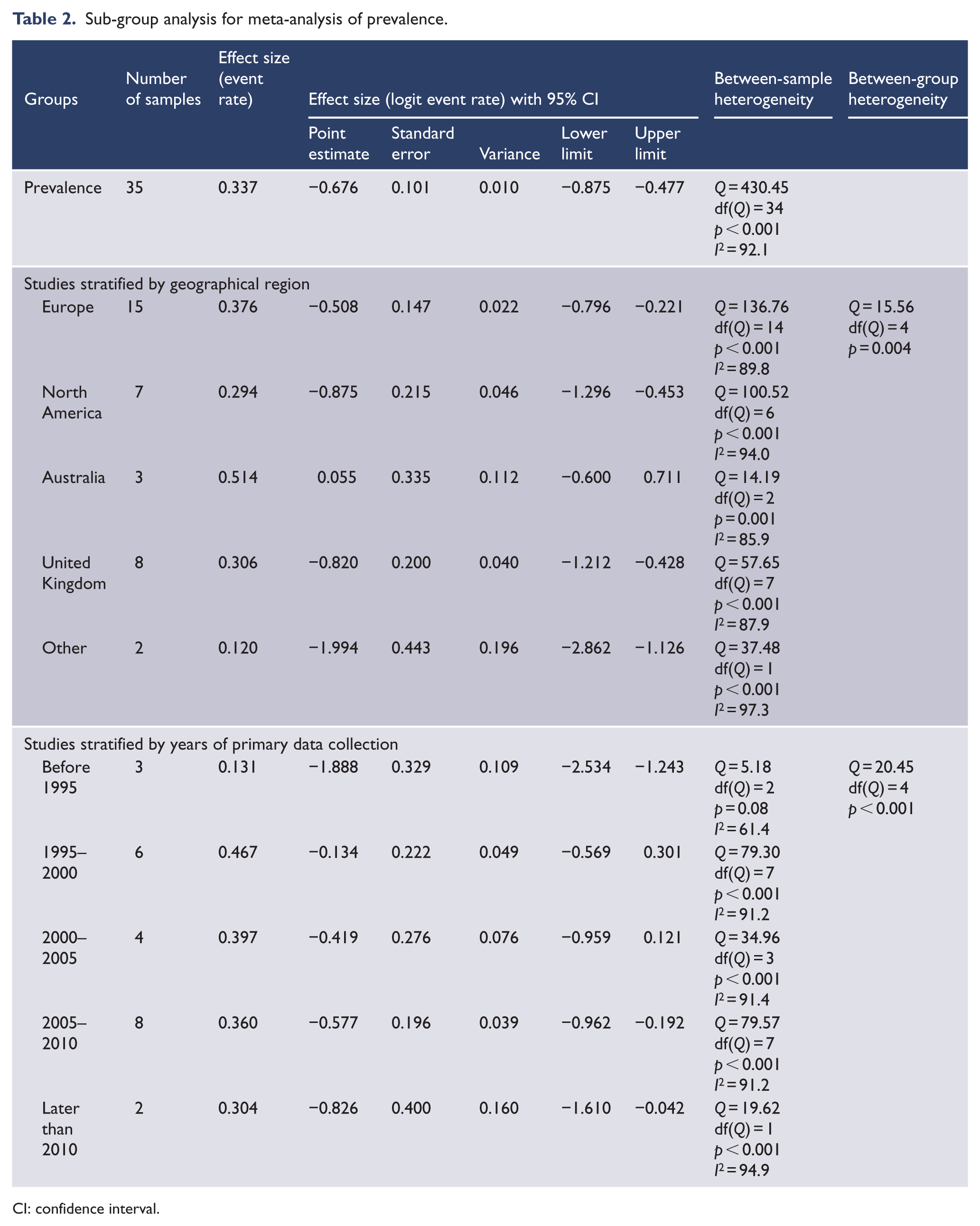
CI: confidence interval.
Sub-group analyses demonstrated a significant difference in prevalence according to geographical region and year of primary data collection. The highest rate of cannabis use was recorded in Australia, followed by Europe, the United Kingdom and North America (see Table 2). The year of data collection, stratified as 5-year increments, demonstrated comparatively low rates in the years prior to 1995, peak rates in 1995–2000, followed by a steady decline in 2000–2005, 2005–2010 and after 2010 (see Table 2). Meta-regression did not demonstrate a significant interaction between proportions of men (33 samples, point estimate = 2.27, SE = 1.40, p = 0.10) or mean age of subjects (25 samples, point estimate = −0.04, SE = 0.03, p = 0.13) and effect size.
There was some evidence of publication bias. Egger’s test demonstrated a statistical trend towards reporting a higher rate of cannabis use (intercept = −2.98, SE = 1.64, p = 0.079). Trim and fill analysis identified five samples that might have been biased to a higher rate of cannabis use. The exclusion of these studies increased the point estimate from 33.7% to 38.0% (95% CI = [33.0%, 43.3%]).
Analysis of continuation
Meta-analysis of continuation demonstrated that at between 2 months and 10 years of follow-up after first episode of psychosis, the odds ratio of continued cannabis use was 0.56 (95% CI = [0.40, 0.79]) (see Figure 4). Heterogeneity was high (Q = 114.06, df(Q) = 18, p < 0.001, I2 = 84.2). Heterogeneity was not significantly accounted for by time point (in months) at follow-up in each sample (see Table 3). Meta-regression demonstrated that studies with a higher proportion of users at base line tended to have a greater reduction use at follow up (point estimate = −3.49, SE = 0.73, p < 0.001).
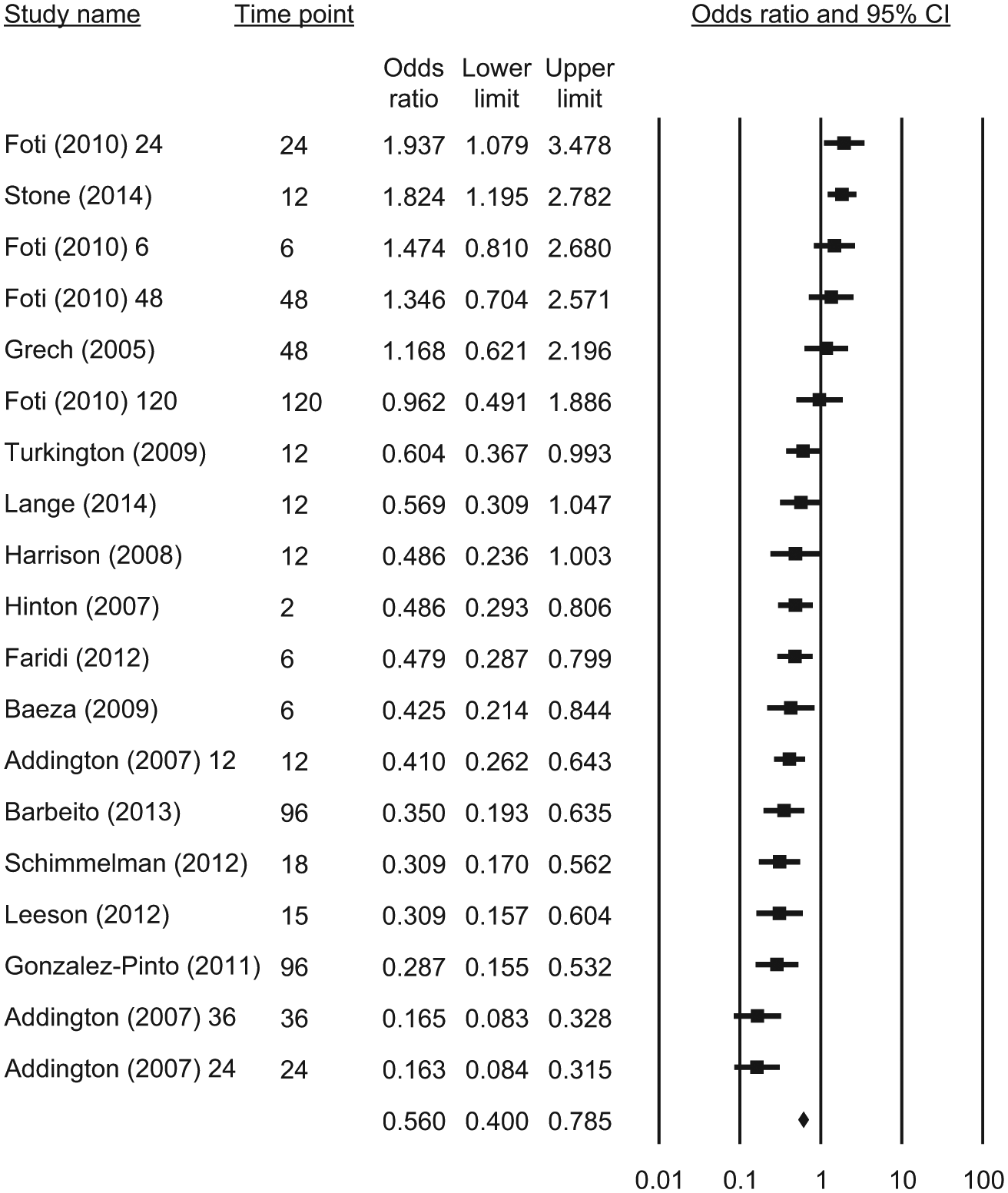
Forrest plot of meta-analysis of continuation.
Sub-group analysis for meta-analysis of continuation.
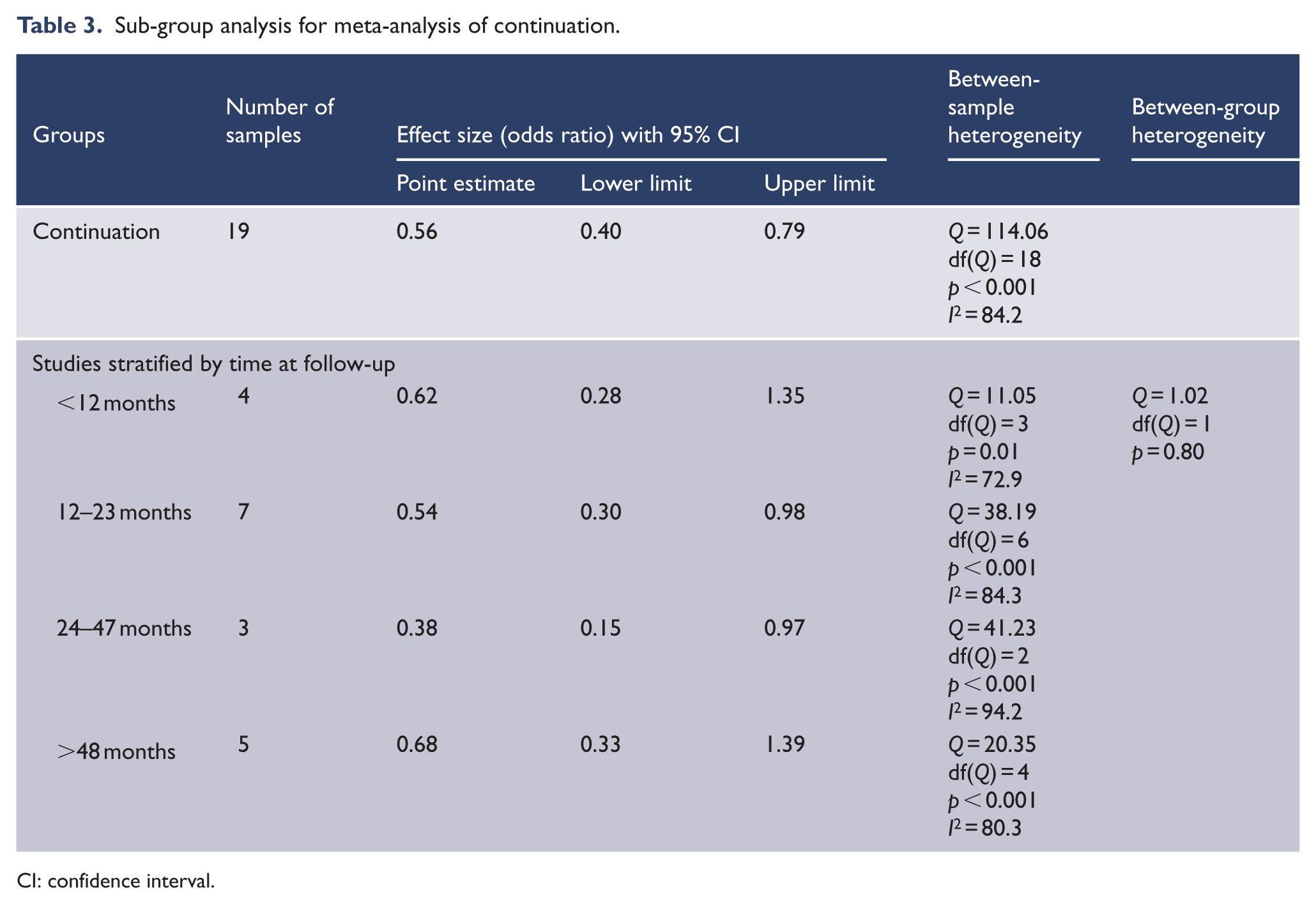
CI: confidence interval.
Egger’s test did not demonstrate evidence of publication bias (intercept = −5.13, SE = 3.65, p = 0.18). Trim and fill analysis identified one sample that might have been biased to lower odds of cannabis use. The exclusion of this study increased the point estimate from 0.56 to 0.65 (95% CI = [0.45, 0.91]).
Discussion
The principal findings of this meta-analysis are that cannabis use is initiated around 6 years before the onset of psychosis, approximately a third of people who present with first episode psychosis have clinically significant cannabis use and cannabis use at follow-up declines by approximately 50%, over time. The finding demonstrating a decline in cannabis use after first episode psychosis is consistent with lower median rates of cannabis use disorders in long-term patients when compared to people with first episode psychosis demonstrated in a previous data synthesis of cross-sectional studies of cannabis use in people with schizophrenia (Koskinen et al., 2010).
We also found that the prevalence of cannabis use varies according to region with Australia having rates approaching double that of the United Kingdom and North America. The Australian findings should, however, be interpreted with caution given all samples were collected from a single first episode psychosis centre that may not be representative of Australia as a whole. Similarly, heterogeneity in prevalence estimates within other geographical regions indicates that the burden of cannabis use at a local level varies considerably, and while representing a significant clinical issue for some mental health services, this may not be true for other services within broad geographical regions. Of note, rates of cannabis use also differed significantly depending on the period in which studies were performed with a lower prevalence before 1995, peak prevalence in 1995–2000 and a modest decline in prevalence thereafter. These temporal and geographical variations in cannabis use might reflect changing patterns of substance cost and availability in the wider community, societal attitudes to cannabis use and population awareness of the potential harms of cannabis.
The results of this meta-analysis when compared to a previous meta-analysis of tobacco use in early psychosis that employed similar methods (Myles et al., 2012) provide insight into epidemiological differences between the two commonly smoked addictive, psychoactive substances. Regular tobacco use predated the onset of psychosis by a similar period to cannabis use of more than 5 years. In contrast, almost two-thirds of patients with first episode psychosis smoke tobacco and there was no evidence for a decline in smoking rates during follow-up (Myles et al., 2012). Hence, although cannabis and tobacco use are likely to be initiated at a similar interval prior to the onset of psychosis, there are almost twice as many tobacco smokers as cannabis smokers among first episode samples, and it appears that cannabis users are more likely to cease use than are tobacco smokers.
The long interval between the onset of regular cannabis use and psychosis onset has two notable implications. First, it casts further doubt on the popular belief that cannabis is initiated as a form of self-medication for the positive symptoms of psychosis (Hall, 2000), because the interval of 5 years is several times longer than average duration of untreated psychosis (Large et al., 2008), a duration which is not significantly longer among cannabis users compared to non-users (Burns, 2012). However, this does not exclude the possibility that cannabis use is initiated in response to other less specific anxiety or affective symptoms that might predate psychosis (Schaub et al., 2008) or as a consequence of shared genetic, psychological or social vulnerabilities. The evidence for these hypotheses can currently only be based on epidemiological evidence and requires further clarification. Intervention during this period, however, might delay the onset of psychosis and could plausibly reduce the burden of symptoms in those who subsequently transition to psychosis.
The proportion of current cannabis users with first episode psychosis should be of interest to service planners, emphasising that treatment of substance use in early psychosis should be given particular priority. Substance use treatment should play an integral role in first episode psychosis programmes, given that early cessation of cannabis use is associated with benefit in terms of positive symptoms, mood and social function compared to later cessation (Mullin et al., 2012). While our finding of significant rates of cannabis use cessation at follow-up is encouraging, the explanation for this observation is unclear. Plausibly, those people who do cease use early may recognise the adverse contribution of cannabis to their symptoms or may respond to usual clinical care. The high quit rate observed in this analysis is at odds with the generally disappointing rates of cessation reported in interventional studies (Hjorthoj et al., 2009). However, it is possible that the high quit rate achieved during and after first episode psychosis paradoxically contributes to the apparent lack of effectiveness of formal interventions designed to effect cessation. If people who can achieve abstinence do so early in the course of their disease without formal intervention, the remaining subset of users might be more dependent, less motivated or otherwise less able to quit. Investigations of factors that predict cessation might help to inform clinical strategies to further reduce long-term cannabis use in this population.
The limitations to this meta-analysis should be acknowledged. First, we conducted a meta-analysis of available studies and not a global survey of cannabis use in first episode psychosis. We also found that there was significant heterogeneity in rates of cannabis between geographical regions and over different time periods. Hence, the estimate of prevalence reported here may not be generalisable to all patient groups or treatment settings; rather, it should be recognised that cannabis use by people with psychosis is likely to be impacted by complex social and geographical factors. Second, the analysis of longitudinal use of cannabis, while able to determine trends of cannabis use over time, was unable to determine the proportional transition of users to non-users and vice versa. It is plausible that a proportion of subjects initiate use following first episode of psychosis, which is offset by a large proportion of those who cease use. Cannabis use is likely to be relapsing and remitting, and the extent of the problem of genuinely new users of cannabis after the diagnosis of psychosis and the proportion of lifelong quitters remain unclear.
Conclusion
This analysis indicates cannabis use predates and is prevalent in early psychosis with significant rates of cessation at follow-up. Risk factors underlying the prevalence of cannabis in early psychosis warrant ongoing investigation, particularly in the current climate of liberalisation of cannabis control and greater societal acceptance of use. Regardless, the practical problem remains: how do we target and develop effective strategies to reduce cannabis use among people considered at high risk of psychosis and how do we effect cessation in those cannabis users who have transitioned to psychotic illness?
Footnotes
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not for profit sectors.