
Abstract
Objective:
A national network of expert centers for bipolar disorders was set up in France to provide support, mainly for psychiatrists, who need help for managing bipolar disorder patients. The aims of this article are to present the main characteristics of the patients referred to an expert center in order to highlight the major disturbances affecting these patients and to understand the most significant difficulties encountered by practitioners dealing with bipolar disorder patients.
Methods:
Patients were evaluated by trained psychiatrists and psychologists, with standardized and systematic assessment using interviews and self-report questionnaires.
Results:
All patients (n = 839) met Diagnostic and Statistical Manual of Mental Disorders–Fourth Edition criteria for bipolar disorder I (48.4%), bipolar disorder II (38.1%) or bipolar disorder–not otherwise specified (13.5%). Mean illness duration was 17 years (±11.3), with 41.9% of patients having a history of suicide attempts. Lifetime comorbidities were 43.8% for anxiety disorders and 32.8% for substance abuse. At the point of inclusion, most patients (76.2%) were not in an acute phase, being considered to have a syndromal remission, but which still required referral to a tertiary system of care. Among these patients, 37.5% had mild to moderate residual depressive symptoms (Montgomery and Asberg Depression Rating Scale ranging from 7 to 19) despite 39% receiving an antidepressant. However, 47.8% were considered to be poorly adherent to medication; 55% showed evidence of sleep disturbances, with half being overweight; 68.1% of patients showed poor functioning (Functioning Assessment Short Test ⩾ 12) with this being linked to residual depressive symptoms, sleep disturbances and increased body mass index.
Conclusions:
It appears that bipolar disorder patients referred to an expert center in most cases do not suffer from a severe or resistant illness but they rather have residual symptoms, including subtle but chronic perturbations that have a major impact on levels of functioning. The longitudinal follow-up of these patients will enable a better understanding of the evolution of such residual symptoms.
Introduction
A national network of expert centers for bipolar disorders (BDs) (FondaMental Advanced Centres of Expertise for Bipolar Disorders; FACE-BD) was set up in France to provide support for psychiatrists who need help for managing BD patients. In some cases, patients can also be referred by general practitioners (GPs), when BD is suspected, allowing their orientation to a specialized care system (Henry et al., 2011). The goals are to provide advice about potential treatment targets that is based on an accurate evaluation and which enhances concordance between evidence-based medicine guidelines and clinical practice, thereby promoting a personalized medicine approach. The network represents a tertiary system of care open to all BD sub-types allowing a large spectrum of patients to be included. Traditionally, specialized services of care are usually considered for severe and/or complex or resistant presentations meaning that research based on such severe BD presentations will not be representative of the population of BD patients.
However, several elements can influence access to specialized care. First, guidelines have become more complex, meaning that clinicians may become more prone to referrals to a specialized care system. Moreover, even if guidelines exist for prophylactic treatment that are built on evidence-based medicine, we lack information on very long-term management of BD patients, given the frequent complexity of presenting cases.
Second, patients have access to medical information from a wide array of sources, including consumer medicines information, media reports and Internet web sites. It is hoped that improved ‘medicine health information’ will help with patient compliance, reduce adverse events and result in better health outcomes. In turn, this may also change exigency levels of BD patients and their willingness to utilize specialized care.
Finally, there is now evidence that the manifestations of BD are not restricted to recurrent episodes of (hypo)mania or depression, but that there is also a more subtle chronic course than initially conceptualized (Leboyer et al., 2012). In most cases, the inter-episodic periods are characterized by residual symptoms (Judd et al., 2003), subtle cognitive impairment (Martínez-Arán et al., 2004), increased impulsivity (Etain et al., 2013; Swann et al., 2009) and emotional hyper reactivity (Henry et al., 2008; Boudebesse et al., 2013), as well as sleep and circadian rhythm abnormalities (Harvey et al., 2005). All these disturbances seem to be strongly linked to long-term prognosis and significantly impact on functioning (Soreca et al., 2009). Specialized care can be perceived as a system that can help achieve functional recovery by offering solutions for these chronic course elements (Henry and Etain, 2010).
To better understand the role of these specialized care services, there is a need to better know the nature of BD patients referred to them. The aim of this report is to assess the global characteristics of the BD patients referred to expert centers, in turn indicating the main difficulties that practitioners face in the management of BD patients.
Method
Design of FACE-BD
The methods are presented briefly below and have been described in more detail elsewhere (Henry et al., 2011). The network of expert centers dedicated to BD is an innovative health care system in France. Until now, mental health care in France has been based essentially on catchment areas. Because of the complexity of diagnosis and care of BD disorders, this network was created to provide support to clinicians for the management of BD patients and, in parallel, to generate clinically relevant research.
Site selection
Sites must be affiliated to an academic center that is actively involved in BD care and research, and have the motivation to integrate into the network. Currently, there are nine expert centers in France. Members of the clinical teams from each center have joint monthly meetings to ensure inter-rater reliability, to receive or provide training in new therapeutic interventions, to develop research protocols and to maintain the levels of expertise required in this tertiary care system that is associated with specialized care and research.
Participant enrollment
Patients are referred by a GP or psychiatrist (mainly a psychiatrist), who subsequently receives a detailed evaluation report that outlines potential therapeutic interventions. Although patients are re-assessed and followed at the expert center, routine care and treatment is still managed by the referring physician.
There are no exclusion criteria for referral, and all patients who appear to meet the diagnostic criteria for any BD sub-type (I, II or not otherwise specified [NOS]) can be assessed. Patients are only outpatients and are not referred to us in emergency. The assessment protocol was approved by the relevant ethical review board and requires only a letter of information for patients (CPP-Ile de France IX, 18 January 2010). A web-based application, e-bipolar© was developed to collate data for clinical monitoring and research purposes. Access to the system is carefully regulated and approval was obtained from the body overseeing the safety of computerized databases (CNIL) (DR-2011-069).
Assessments
In this study, we have focused on the general characteristics of the referred BD presentations allowing the assessment of their current state to better clarify why patients are referred to us. The Structured Clinical Interview for the Diagnostic and Statistical Manual of Mental Disorders–Fourth Edition (DSM-IV) Axis I Disorders (SCID) was used to confirm BD diagnosis, as well as to evaluate the course of the disease (First, 1996). SCID was also used to identify comorbid psychiatric disorders. Current mood state was assessed using the Montgomery and Asberg Depression Rating Scale (MADRS) (Montgomery and Asberg, 1979) and the Young Mania Rating Scale (Young et al., 1978).
In the first part of the study, we have included all patients referred to us and meeting a BD diagnosis. In the second part, we keep only the patients who are not in an acute episode, being normothymic or with sub-syndromal symptoms.
Current psychotropic treatments were recorded and adherence to treatment is checked using the French version of the Medication Adherence Rating Scale (MARS) (Misdrahi et al., 2004). MARS is a 10-yes/no item questionnaire, which includes reverse items, being a self-reporting multidimensional instrument along three dimensions that were determined by two previous principal component factor analyses and has been utilized in previous studies. The three dimensions are ‘medication adherence behavior’ (items 1–4), ‘attitude toward medication’ (items 5–8) and ‘negative side effects and attitudes to psychotropic medication’ (item 9 and 10). The total score and the three sub-scores are obtained by summing the items. A low score is correlated with a low likelihood of medication adherence and a total score ⩾ 8 is associated with a higher likelihood of medication adherence.
Global social functioning was evaluated using the Global Assessment of Functioning scale (GAF) and the Functioning Assessment Short Test (FAST) (Rosa et al., 2007). The FAST is an interview developed to evaluate disability in BD patients and includes items on autonomy, work, cognitive functioning, financial issues and interpersonal relationships. This scale provides a total score of functioning and also six specific domain sub-scores.
Sleep disturbance was assessed with the Pittsburgh Sleep Quality Index (PSQI) (Buysse et al., 1989), which is a 19-item self-completed questionnaire requiring the participant to describe patterns of sleep, such as typical bedtime and wake time, sleep latency and actual sleep time. The patient is also asked about sleeping habits and quality. The French version of this questionnaire has been validated by Blais et al. (1997).
The same package of evaluations has been adopted by all centers, and the full assessment is performed by members of a specialized multidisciplinary team: a nurse, a clinical psychologist, a neuro-psychologist and a psychiatrist.
Statistical methods
Socio-demographic characteristics and the principal clinical feature of the disease and comorbidities for the first 839 BD patients included in the cohort are presented. Measures of means and dispersion (standard deviation, SD) were used for continuous data and frequency distribution for categorical variables.
Since a high proportion of patients are referred to us in a non-acute episode (n = 588), we present disease characteristics and comorbidities of this sub-sample and we have explored the links between these characteristics and functioning. To evaluate the association between functioning and various factors (clinical characteristics and comorbidities), we performed a multivariate linear regression analysis. SAS software (release 9.1; SAS Statistical Institute, Cary, NC) was used for the statistical analyses.
Results
Demographic characteristics
The sample included 839 BD patients. The mean age of the participants was 41.6 (±12.9) years and 57.7% were female (see Table 1). Approximately half of the patients (50.9%) were married, with one-third (34.4%) being single.
Demographic and illness characteristics of the entire cohort.
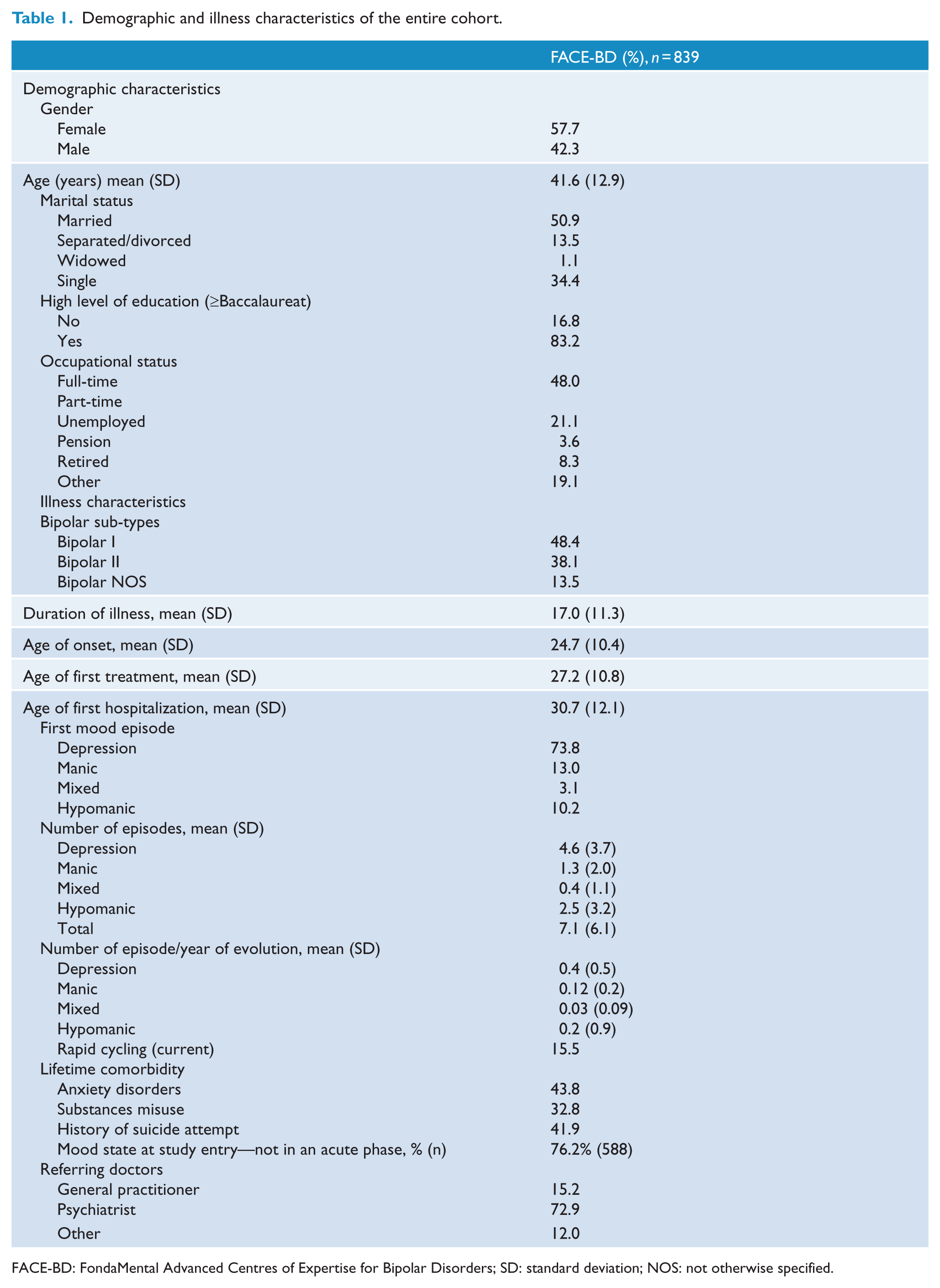
FACE-BD: FondaMental Advanced Centres of Expertise for Bipolar Disorders; SD: standard deviation; NOS: not otherwise specified.
A large proportion of the patients (83%) had a high school diploma. Unemployment was prevalent, with 21.1% of the patients unemployed (double the French national unemployment rate).
Clinical features and treatment
In our sample, 48.4% of patients met criteria for BD I disorder, 38.1% BD II and the remaining patients were classified as BD NOS. The mean age at onset was 24.7 (±10.4) years: the age at first pharmacological treatment, irrespective of the pharmaceutical class, was 27.2 (±10.8) years, and the mean age at first hospitalization was 30.7 (±12.1) years.
The polarity of the first episode was a major depressive episode in most cases (73.8%) and the first manifestation of the disorder was manic or hypomanic states for only 23.2% of the patients. The predominant polarity of all episodes was depressive, with means of 4.6 (±3.7) depressive episodes, 1.3 (±2.0) manic episodes and 2.5 (±3.2) hypomanic episodes.
For lifetime comorbidities, the rates of anxiety disorders was 43.8% and substance abuse 32.8%; 41.9% of the patients had a history of suicide attempts; 15.5% of the patients fulfilled criteria of rapid cycling. The mean number of medication received was 2.4 (±1.3) (Table 2), with 42% of patients receiving an antidepressant. The most frequently prescribed class of mood stabilizers was anticonvulsants (57.5%) followed by atypical antipsychotics (APA) (32.4%) and lithium (31.5%).
Pharmacological treatment (based on 610 patients).

FACE-BD: FondaMental Advanced Centres of Expertise for Bipolar Disorders; APA: atypical antipsychotics; SD: standard deviation.
Most patients (76.2%) were not in an acute phase when referred to us. The clinical characteristics in this sub-sample are presented in Table 3. Although the patients were supposed to be in syndromal remission, most of them had residual symptoms. In particular, 59.7% of patients had at least one depressive symptom, and the scores at the MADRS ranged from 7 to 19 in 37.5% of patients due to mild to moderate depressive symptoms, despite 39% being in receipt of an antidepressant. Manic symptoms were less prevalent than depressive symptoms: 32.1% of patients had one or more manic symptom, although 94.6% of the patients had a YOUNG score below or equal to 8. Almost half of these patients (47.8%) were considered to be non-adherent to medication (MARS score below 8). These patients also showed moderate to serious impairment of global functioning as assessed using the GAF scale (5.4% had a score < 51 and 48.4% a score < 70). Using the FAST, a more specific tool to assess BD patient functioning, we obtained a mean total score of 17.6 (SD = 12.9) corresponding to 68.1% of patient with an impaired functioning (FAST total score ⩾ 12).
Characteristics of the sample considered in a syndromal remission phase (n = 588).

SD: standard deviation; MADRS: Montgomery and Asberg Depression Rating Scale; GAF: Global Assessment of Functioning scale; MARS: Medication Adherence Rating Scale; PSQI: Pittsburgh Sleep Quality Index; FAST: Functioning Assessment Short Test.
Half of these patients also had sleeping disturbances (55.1% had an abnormal PSQI score) and 48.4% were overweight or obese, with a body mass index (BMI) > 25.
We used multivariate linear regression to assess the consequences of these clinical characteristics on the functioning, as assessed with FAST (Table 4). The main factors impacting functioning are residual depressive symptoms (MADRS total score, p < 0.0001), sleep disturbances (PSQI total score, p = 0.005) and BMI (p < 0.0003). Considering the FAST sub-scores, corrected for multiple testing (p < 0.01), depressive symptoms assessed with the MADRS had an impact on all sub-scores (autonomy, work, cognitive functioning, financial issues, leisure and interpersonal relationships) (p < 0.0001); non-adherence had an negative impact on autonomy (p < 0.0065); poor sleep had an impact on leisure (p = 0.0049) and interpersonal relationships (p < 0.003); a high BMI had a bad impact on all the sub-scores except on work.
Factors associated with functioning using the FAST in patients considered in a syndromal remission phase (n = 588).
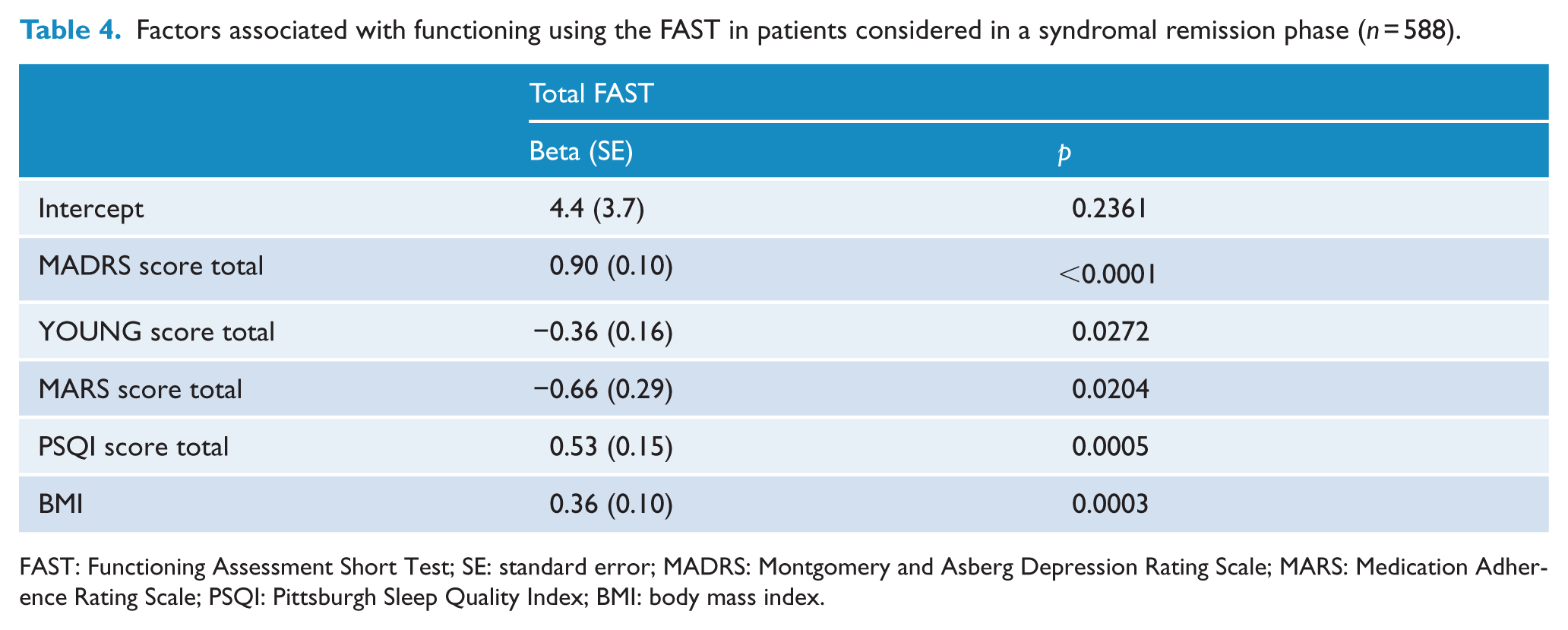
FAST: Functioning Assessment Short Test; SE: standard error; MADRS: Montgomery and Asberg Depression Rating Scale; MARS: Medication Adherence Rating Scale; PSQI: Pittsburgh Sleep Quality Index; BMI: body mass index.
Since sub-syndromal depressive symptoms had a major impact on functioning, we looked at the profile of patients considered truly in a normothymic phase with a MADRS <7. This sub-group also had poor functioning in 43.9%, with a score at the FAST ⩾ 12. Such poor functioning was associated with residual symptoms even when they are very low (MADRS total score, p = 0.002, adherence to treatment, MARS, p = 0.03, and the BMI, p = 0.01).
Discussion
We report a description of the first 839 BD patients included in the FACE-BD cohort, including socio-demographic characteristics and the principal clinical features of the disease, as well as comorbidities and current state. It appears that 76% of patients referred to an expert center were not in an acute episode. Our data highlight the main features presented, giving clarity to the reasons motivating a consultation in an expert center.
The main demographic and clinical characteristics of the FACE-BD patients were comparable to those of other cohorts or data from the literature. For example, the mean age, the slight preponderance of women and the recorded educational level are very close to those of the Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD) study (Kogan et al., 2004). Most of our patients reported depression as their first mood episode, with presentations of comorbid anxiety disorders and a history of suicide attempts being very common (respectively 43.8% and 41.9%) (Kogan et al., 2004; Popovic et al., 2013).
The age at onset, 24.7 years in our cohort, is consistent with previous studies in Europe but higher than in the United States (Etain et al., 2012). Several explanations for this difference have been suggested (Bellivier et al., 2011), including cultural factors, clinical differences, genetic mechanisms (Lange and McInnis, 2002), differences in the approaches to treatment (Da Silva Magalhães et al., 2009; Reichart and Nolen, 2004) or differences in access to specialized mental health care (Carlson, 2011).
A high proportion of patients in our cohort met the criteria for BD II (38%) and BD NOS (13.5%). This may be due in part to the fact that a substantial proportion of patients (42.4%) included in the FACE-BD cohort were referred by private psychiatrists often in charge of less severe patients.
Another particular feature of FACE-BD cohort is the high proportion of patients who are considered in syndromal remission (defined as ‘not currently in an acute episode’ using the DSM-IV criteria) (76.2%). It appears that approximately 40% of these patients had residual depressive symptoms, in spite of 39% receiving an antidepressant. Previous studies have shown that BD patients have sub-syndromal and minor depressive symptoms nearly three times more frequent than full episodes (Judd and Akiskal, 2003; Judd et al., 2002, 2003) and that sub-threshold depressive symptoms are good markers of rapid and frequent relapse and/or recurrence of a clinically depressive episode (De Dios et al., 2012; Judd et al., 2008). Regarding the great impact on functioning of these depressive symptoms, further studies are needed to better characterize them and to understand their poor response to antidepressant. The next step is to characterize them with a dimensional approach, which seems more appropriate to capture the heterogeneity of mild symptoms (article in preparation).
We also found that patients had sleep disturbances, were overweight and showed only partial adherence to treatment. Other studies have found that symptoms of insomnia and circadian rhythm disturbances are frequent in remitted patients with BD (Milhiet et al., 2011). A more systematic assessment of sleep and circadian rhythms in patients with BD may help to define appropriate personalized treatment. Light-therapy (Sit et al., 2007) and specific psycho-social interventions, such as Interpersonal and Social Rhythms Therapy (Frank et al., 2005), could be preferentially proposed to patients with such disturbances.
Almost half of our patients were overweight or obese. Being overweight and obesity are both more prevalent in patients with BD than individuals with no psychiatric condition (adjusted odd ratio of 3.9) (Gurpegui et al., 2012). As a consequence, life expectancy is reduced by around 10 years, due in part to cardiovascular and metabolic disease (Roshanaei-Moghaddam and Katon, 2009). In addition to somatic complications, high BMI has a negative effect on functioning, including impairing quality of life (Kolotkin et al., 2008); it is also linked to a poorer response to classical mood stabilizers (Kemp et al., 2010).
Beyond direct adverse effects, all these elements impact the functioning of patients. In fact, our data highlight that depressive residual symptoms, sleep disturbances and a high BMI are associated with a poor functioning (Table 3).
All together, these data reveal that a high proportion of patients are referred to an expert center as a consequence of residual depressive symptoms, poor functioning, moderate adherence to treatment and sleep disturbances. The recruitment into the FACE-BD cohort seems not based on refractory or severe cases but on more subtle, but chronic disturbances.
The strengths of the FACE-BD study include its multisite patient sample, the uniformity of diagnostic and evaluation procedures and its broad spectrum of multidimensional assessments. The non-restrictive criteria for entering the cohort favor wide inclusion, limited only by the willingness of patients and recruitment capacity.
However, it is a cross-sectional study, giving an overview of the main disturbances evident in patients who are referred to an expert center during a remitted phase, and requires longitudinal follow-up data to better understand the evolution of such disabling features.
Large longitudinal cohorts of BD patients are essential for studying the progression of the disease, individual differences, relapse factors and treatment effectiveness. The establishment of specialized care and treatment based on guidelines should improve the management and consequently change the course of the disease (Bauer et al., 2009; Kessing et al., 2013). With this prospective cohort, we will be able to generate data about outcomes from the patients followed up within the network. Our data highlight the need to focus on subtle and chronic disturbances of the disease.
Specialized care is inherent to the progress of medicine and is particularly important for psychiatric diseases, as the nosology is changing: this is due to a better understanding of psychopathological mechanisms and should be further refined in the light of responses to treatments (Berk et al., 2013; Vieta, 2013). These data reinforce that mood instability and sub-syndromal symptoms rather than mood episodes might be the key feature of BD, reinforcing the idea that classical psychiatric diagnosis would benefit from being completed along a dimensional perspective.
Footnotes
Acknowledgements
This research received the support of the Foundation FondaMental. We would like to thank George Anderson, CRC Scotland & London, for English editing of this article. FACE-BD group: AP-HP, Hôpital H. Mondor—A. Chenevier, Pôle de Psychiatrie, Créteil: C. Boudebesse, A. Raust; AP-HP, GH Saint-Louis—Lariboisière—Fernand Widal, Pôle Neurosciences, Paris: M. Leroux, S. Sportiche; Hôpital C Perrens, Centre Expert Trouble Bipolaire, Service de psychiatrie adulte, Pôle 3-4-7, Bordeaux: S. Gard, K. M’Bailara; Département d’Urgence et Post Urgence Psychiatrique, CHRU Montpellier, Montpellier: E. Olié, F. Molière; Département de Psychiatrie, Hôpital Sainte Marguerite, Marseille: N. Viglianaise, L. Lescalier; Service de Psychiatrie et Psychologie Clinique, CHU de Nancy, Hôpitaux de Brabois, Vandoeuvre Les Nancy: O. Wajsbrot-Elgrabli, R. Cohen; Clinique Universitaire de Psychiatrie, CHU de Grenoble, Grenoble: M. Polosan, M.A. De Pourtales; Centre Hospitalier de Versailles, Service de Psychiatrie Adulte, Le Chesnay: N. Kayser, I. Grevin; Centre Hospitalier Princesse Grace, 98000 Monaco: J. Loftus, I. Médecin.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
Funding
This work was supported (in part) by the Investissements d’Avenir programs managed by the ANR under references ANR-11-IDEX-0004- and ANR-10-COHO-10-01.