
Abstract
Clinicians and researchers have long observed that women express and experience schizophrenia differently from men. An earlier age at onset of schizophrenia in male subjects, described by Kraepelin in 1909 and Bleuler in 1911 [1], has been one of the most stable findings in this area of study [2]. It has been reported in various reviews as robust across cultures, for different definitions of onset including age at first onset of symptoms, age at first diagnosis, and age at first hospitalization, and for different definitions of illness [3–5], although it has not been found in all studies [6–10]. Some studies have also reported a bimodal distribution of age at onset in women, with the second peak occurring in mid-life [11]; Castle and Murray report a third peak for women in old age [12]. Marital status and family history of schizophrenia may confound the relationship between sex and age at onset [1], [13]. Other differences have also been observed including differences in symptom expression – with men more likely to manifest negative symptoms [14] and women more likely to have affective symptoms [15], [16], better premorbid functioning in women [15], and a milder course of illness and lower levels of disability in women [17], [18]. Different patterns of service utilization have been described, with women more likely to seek treatment but spending fewer days in hospital and being less likely to be rehospitalized or involuntarily committed [18], although one study has suggested that these differences are site specific rather than gender specific [19].
While there is an extensive literature on the differences in schizophrenia between women and men, few studies have had the capacity to assess whether their findings extend to other psychotic disorders. A comprehensive review of the published literature found that, where data are available, there is more concordance than discordance across the psychoses with respect to differences between women and men [20], although differences appear to be more pronounced in schizophrenia [15]. Australian data also point to similarities across diagnostic groups: Preston etal. found that men had poorer premorbid functioning compared to women irrespective of diagnosis (schizophrenia and schizophreniform disorder compared to any other psychotic disorder) in a first-episode sample [21].
The aims of the present study were to use a large representative sample of persons with psychoses to (i) document differences between women and men in their expression and experience of schizophrenia, and (ii) investigate the stability of these differences across diagnostic groups. In this paper we distinguish biologically determined sex differences from culturally and socially mediated gender differences [22], [23].
Method
The data for the present study come from the Australian National Survey of Low Prevalence (Psychotic) Disorders, an epidemiological study conducted across catchment areas in four Australian States. Details of the study methodology are provided elsewhere [24]. In brief, in phase 1 of the study, individuals were screened for psychosis in a census month in 1997 at inpatient and outpatient services, in general medical and private psychiatric practices and in marginalized settings within the study catchments (with a total catchment population aged 18–64 of 1 084 978). In addition, registers were used to identify persons in contact with inpatient and outpatient services within 3 years of the census but not in the census month. In phase 2, 1126 individuals were randomly selected, stratified by recruitment source, from those screen-positive for psychosis, and interviewed in depth. Those whose diagnosis of psychosis was confirmed are the subjects reported here.
Diagnoses were determined using the Diagnostic Interview for Psychosis (DIP), a semi-structured clinical interview, for use by trained and experienced mental health professionals [25]. Where applicable, DIP uses questions and probes from the World Health Organisation Schedules for Clinical Assessment in Neuropsychiatry to elicit the items of the 90-item Operational Criteria for Psychosis (OPCRIT) checklist [26]. An allied computerized algorithm generates diagnoses according to various diagnostic criteria. ICD-10 criteria were used in the present study. Interrater agreement for DIP-generated ICD-10 diagnoses was good [25].
χ2 tests for categorical data and t-tests for continuous data were performed using SPSS 11.0.0 (SPSS, Chicago, Illionois, USA). The distribution of age at onset was assessed using the two-sample Kolmogorov–Smirnov test of equality of distribution and quantile–quantile plots in Intercooled Stata 7.0 (Stata Corp, College Station, Texas, USA); the former test has been applied in studies of seasonality of birth in schizophrenia [27], and for assessing sexual dimorphism in anthropological research [28]. Significance levels were set at p < 0.05. Because this was a descriptive study, Bonferroni corrections were not applied.
Results
A diagnosis of a psychotic disorder was confirmed at interview in 1090 of the 1126 eligible subjects. According to ICD-10 criteria, 54.4% of these had a diagnosis of schizophrenia, 10.9% had a schizoaffective disorder, 19.3% had an affective psychosis, and the remainder (15.4%) had another psychotic disorder, primarily paranoid psychosis or a non-organic psychosis. Women made up 40.6% of the total sample but were differentially distributed within the four diagnostic groups, comprising 33.6% of the schizophrenia group, 47.1% of the schizoaffective group, 53.8% of the affective psychoses group and 44.6% of the other psychoses group. To test for sampling biases, the interviewed sample was compared with the larger census month screen-positive sample. The percentage of men was the same and the ratio of men to women within the various recruitment sources was similar for both samples. Moreover, when the screening data responses of those selected for interview were compared to responses of those not interviewed, there were no significant differences between samples in the percentage of positive responses for each screening item.
Current and premorbid characteristics
Women within each of the diagnostic groups were a little older than men at interview (by 2–5 years) and had been ill for approximately 2–3 years longer (Table 1). Across the groups, women were significantly more likely to be in long-term relationships and to have children. Women in all diagnostic categories were more likely to have had better premorbid social functioning (the difference was significant for schizoaffective disorder and affective psychoses) and, apart from those with schizophrenia, better premorbid work functioning. Women were more likely than men to be engaged in meaningful although not necessarily paid employment in the 12 months prior to interview (significantly so for the affective and other psychoses groups), and less likely to be on a pension (significant for schizoaffective disorder and affective psychoses).
Sample characteristics by sex and diagnostic group
∗Significant differences between men and women within a diagnostic group (p < 0.05).
Age at onset
Women were a little older than men at onset of illness (except for affective psychoses where the mean age was the same) but not significantly so (Figure 1). While more women than men were in the 40+ age category at onset (significant for schizophrenia and schizoaffective disorder), differences in the age at onset distribution were not significant when analysed using the Kolmogorov–Smirnov statistic.
Age at onset by sex and disorder.
In the schizophrenia group the mean age at onset was 25 for women compared to 23 for men, a difference that was not statistically significant. Age at onset was similarly distributed for both sexes with a single peak in the late teens–early 20s. However, women were more likely than men to be aged ≥40 (p = 0.001), with quantile–quantile plots also indicating some elevation in onset rates for women compared to men after the age of 40. To test for potential confounders, age at onset was modelled using analysis of variance with sex, marital status and family history as independent variables; marital status and family history were highly significant (p = 0.00 for both), with no effect for sex, and no significant two-way or three-way interactions.
Because the use of prevalence data may have confounded age-at-onset findings, analyses were repeated using only those individuals whose onset of psychosis was within 3 years of the census and who therefore would have been captured as incident cases either at census or through case finding using administrative health records up to 3 years prior to census (total n = 170). None of these analyses were significant. In addition, to ensure that reliance on retrospective, self-reported survey data had not introduced a bias, a separate analysis was undertaken using prospectively collected, electronic psychiatric case register data for the 173 Western Australian participants who had been in contact with inpatient and outpatient mental health services. The psychiatric case register, established in 1966, is described in detail elsewhere [29]. Age at onset was operationalized as age at first contact with mental health services. Quantile–quantile plots indicated a very high degree of consistency between both survey and register data sources in the reporting of age at onset.
Mode of onset and course of illness
Across all diagnostic groups, women were more likely than men to report a psychosocial stressor prior to onset (significant for all groups except the other psychoses). The mode of onset was similar for women and men, with two out of three experiencing gradual or insidious onset over a period of ≥6 months. However, women were more likely than men to have single or multiple episodes, with some recovery in between episodes, and less likely to experience a chronic course of illness (significant for schizophrenia; Table 2).
Onset and course of illness by sex and diagnostic group
∗Significant differences between men and women within a diagnostic group (p < 0.05).
Symptom profiles
Lifetime and current symptom profiles for women and men are presented in Figure 2. There was variability with respect to the pattern of difference between men and women across variables within a diagnosis, and across diagnostic groupings, with few significant differences. In schizophrenia specifically, women were significantly less likely than men to report having hallucinations, delusions or poor concentration currently (p = 0.02, p = 0.03, p = 0.05, respectively) and more likely to report at least one serious episode of dysphoria over a lifetime (p = 0.01). Within all groups, women were less likely than men to experience negative symptoms; this was significant for the affective and the other psychoses (data not shown).
Symptom profile (current; lifetime) by sex and disorder. †Lifetime profile: significant differences between men and women within a diagnostic group (p < 0.05); ‡current profile: significant differences between men and women within a diagnostic group (p < 0.05).
Service utilization
Patterns of service utilization in the year prior to interview by women and men within the diagnostic groups were also variable (Table 3). Women were generally a little less likely to have had any inpatient admissions but, once admitted, had a similar number of admissions. In schizophrenia and affective psychoses, the number of weeks in hospital in the previous year was similar for men and women, but women with schizoaffective disorder had spent more weeks in hospital compared to men, and women with other psychoses had spent significantly fewer weeks in hospital. Women were more likely to visit a general practitioner (significant for schizophrenia and the other psychoses) and had significantly more visits (except for schizoaffective disorder).
Service utilization (in past year) by sex and diagnostic group
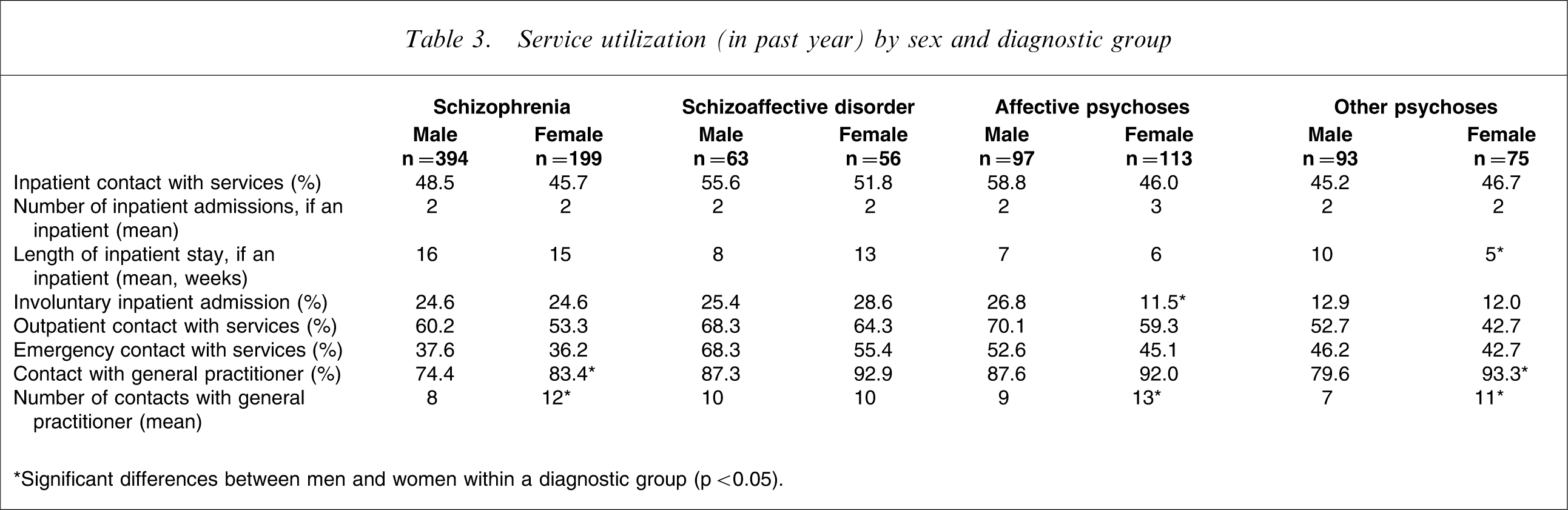
∗Significant differences between men and women within a diagnostic group (p < 0.05).
Disability
Within diagnostic groupings, women reported better functioning and less disability than men, whether assessed using a global measure such as the Social and Occupational Functioning Assessment Scale [30] (where the difference was significant for affective psychoses and other psychoses) or on the basis of specific items such as self-care (significant for schizophrenia), socializing (significant for affective psychoses and other psychoses), and various aspects of their relationships with family and friends (Table 4). Compared to men, more women in all groups reported satisfaction with their level of independence (significant for other psychoses) and, other than those with schizophrenia, were more likely to be satisfied with their life as a whole.
Disability and satisfaction with life (in past year) by sex and diagnostic group
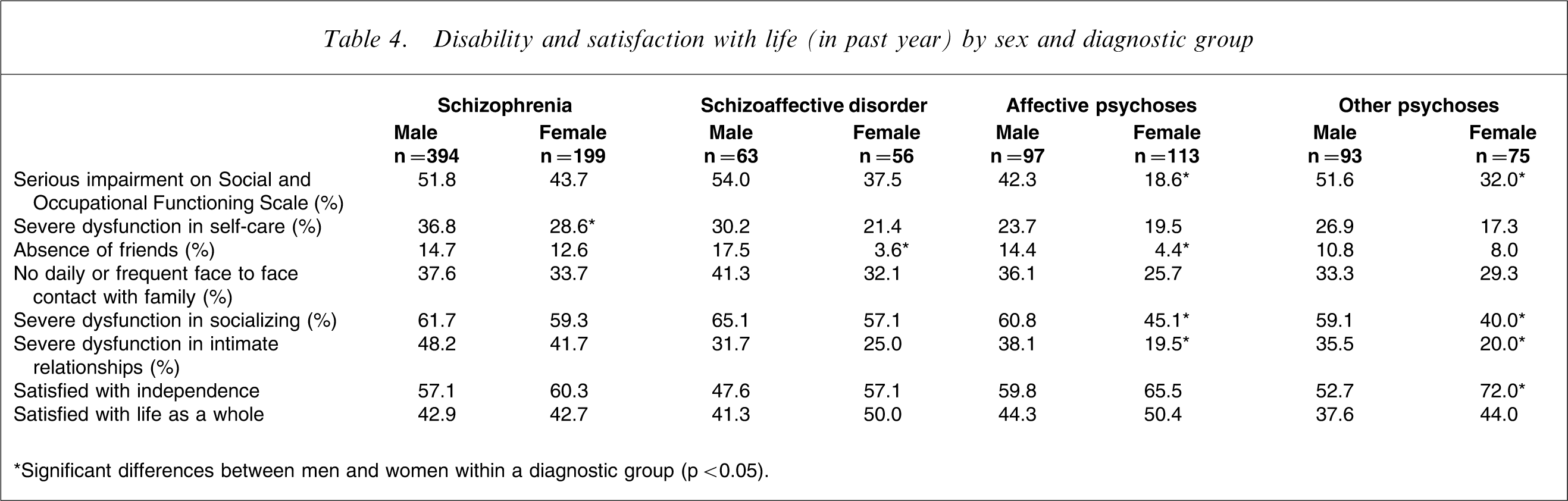
∗Significant differences between men and women within a diagnostic group (p < 0.05).
Women with schizophrenia compared to women with other psychotic disorders
Differences between women across the four diagnostic groups were much larger than differences between women and men within diagnostic groups. Significant differences were recorded for many of the variables assessing social and occupational functioning, with women with schizophrenia more likely than those in the other diagnostic groups to be single, to be childless (only significant at p < 0.1), to have poor premorbid functioning, to be currently unemployed, to be in receipt of disability benefits and to be suffering from a range of impairments. Moreover, there were significant group differences for each of the symptoms reported in Figure 2, with women with schizophrenia less likely to report dysphoria, loss of pleasure, suicidal ideation, irritable or elevated mood, or poor concentration, either currently or over a lifetime, and more likely to report having experienced hallucinations currently and over a lifetime as well as to be currently experiencing delusions and passivity phenomena. Women with schizoaffective disorder were most likely to report subjective thought disorder (current and lifetime) and a lifetime–ever experience of delusions and passivity phenomena. In terms of service utilization, women with schizophrenia stood out mainly with respect to the mean number of weeks they had spent in hospital (15 weeks, compared to 13 weeks in schizoaffective disorder, 6 weeks for affective psychoses and 5 weeks for the other psychoses).
Discussion
Within all diagnostic groupings, we found differences in how women express and experience psychotic illness compared to men. The distinction was most marked in areas involving social engagement with others. Women were more likely to be in long-term relationships, to have children, to have friends and to maintain regular contact with family. When specific aspects of functioning and disability were compared, we found that women were more likely than men to report better premorbid functioning, a more benign course of illness, lower levels of disability, better socialization and integration into the community, and greater satisfaction with their level of independence and life as a whole, regardless of diagnosis; although not all of these comparisons reached significance. No consistent pattern of difference emerged when comparing symptoms and service utilization in women and men. It appears that better functioning in women may be independent of symptom expression and service needs, an observation that has been reported previously [9]. While patterns of difference between women and men found in the other diagnostic groupings held true for schizophrenia, the gap between women and men with schizophrenia tended to be smaller and, across a wide range of variables, women with schizophrenia were much more severely affected than women with any other form of psychotic disorder.
Many of the differences we have found are consonant with the published literature. One main divergence is with respect to age at onset. Mean age at onset did not differ significantly between men and women, although there was a trend in the expected direction; also, the distribution of age at onset was similar for both men and women. Investigating this further for schizophrenia, we found that the absence of an age-at-onset effect could not be attributed to the use of self-reported data or to the use of a prevalence sample. Indeed, it may be that case finding in the present study, which included treated and untreated cases, persons in public and private treatment settings, and patients using both inpatient and outpatient services, resulted in a minimization of sampling bias. Several studies have not found sex differences in age at onset or have found that onset was earlier in women [7], [8], [10]. Jablensky and Cole, in a re-analysis of the World Health Organization (WHO) 10-country study data, propose that reported differences may be the result of confounding, particularly by marital status, which acts as a protective factor, delaying onset [1]. The present data support this: we found that both marital status and familiality confound the association between sex and age at onset.
It was not possible to determine the extent to which oestrogens may play a protective role in delaying onset or moderating the course of schizophrenia in women [11], [31]. Onset was only marginally later, and not significantly so, for women in any diagnostic group, although we noted less chronicity among women, and a greater proportion with onset at ≥40 years of age; these findings were significant in schizophrenia. In keeping with the findings of McGlashan and Bardenstein [15], we also found that women reported having experienced a psychosocial stressor just prior to illness onset significantly more frequently than men in all diagnostic groups except the other psychoses group. However, in the absence of more precise data on the nature of the relationship between the stressor and illness onset, we were not able to assess the implications of this finding for a diathesis-stress model of psychosis [32], including increased susceptibility for psychosis at key points in a woman's life cycle.
Limitations and advantages
A main limitation of the present study was that it is a secondary analysis of data that were not collected primarily to investigate differences between women and men. Although this has restricted the biological data available for analysis, the survey remains an excellent source of data on disability and psychosocial aspects of functioning. Furthermore, the present study had two considerable advantages over much of the previous research. First, the results are based on data from an epidemiologically drawn population of both treated and untreated cases of psychoses, including marginalized groups and those no longer in contact with treatment services, thereby minimizing sampling bias. Second, data were compiled across the range of psychotic disorders using the same ascertainment criteria and the same instruments and measures, with diagnoses derived on the basis of thorough diagnostic interviews and using an operationalized checklist. As a result, the comparisons across diagnoses presented here are among the most systematic and comprehensive in the literature.
Conclusion
WHO policy is to collect and analyse data disaggregated by sex in order to be able to assess the impact of gender differences on risks and outcomes in health [33], [34]. In psychosis, data on differences between women and men can also inform our understanding of the basis of these disorders and influence risk management and treatment [35]. It is likely that a number of models are needed to explain the differences we have observed. On the one hand, the strong pattern of greater social integration and functioning in women across diagnostic groups may well reflect culturally and socially determined gender differences. On the other hand, variability and attenuated findings with respect to symptom profiles beg the question of biological mechanisms with some degree of specificity, a question we could not answer with the data available to us. In particular, the role of oestradiol, a biological factor, and its interaction with gender, remains unclear.
Our findings illustrate the benefits of diagnostic precision when assessing sex- and gender-based differences. However, more hypothesis-driven investigations are needed to explore the interaction between sex and other confounding factors, including obstetric complications, childhood trauma, hormonal changes, and negative life events in order to better understand the mechanisms underlying the differences found and to tease out biological from socially determined differences in psychotic illness.
Footnotes
Acknowledgements
The present report is based on data collected in the Collaborative Study on Low-Prevalence (Psychotic) Disorders, an epidemiological and clinical investigation that was part of the National Survey of Mental Health and Well-being, Australia 1997–1998. Ethics approvals for the study were obtained from relevant institutional ethics committees. (Details available on request.) The study was funded by the Australian Commonwealth Department of Health and Aged Care (for fieldwork in Brisbane, Melbourne and Perth); and by the Australian Capital Territory Department of Health and Community Care, and the Psychiatric Epidemiology Research Centre, Australian National University (for fieldwork in Canberra). The Chief Investigators were Assen Jablensky (Project Director), Vaughan Carr, David Castle, Mandy Evans, Oye Gureje, Carol Harvey, Helen Herrman, Ailsa Korten, John McGrath and Vera Morgan. A complete list of the investigators is available. We acknowledge, with thanks, all the mental health professionals who assisted in the preparation and conduct of the survey and the many Australians with psychotic disorders who agreed to participate.