
Abstract
Objective:
The ego-syntonic nature of anorexia nervosa means that sufferers often deny their symptoms or experience them as positive or comforting. Positive beliefs about eating disorder symptoms may contribute to the development and/or maintenance of eating-disordered behaviour. To date, however, research in this field has been confined to women and anorexia nervosa. Given increasing scientific interest in muscle dysmorphia, a potential eating disorder with ego-syntonic qualities, there is a need to extend current research to include men and muscle dysmorphia. The present study examined whether positive beliefs about anorexia nervosa and muscle dysmorphia were associated with more marked eating disorder symptoms and explored sex differences in these associations.
Method:
Male and female university students (n = 492) read descriptions of a male or female character with clinically significant symptoms of anorexia nervosa or muscle dysmorphia. Participants subsequently answered questions about the characters and completed a measure of disordered eating. Knowledge, personal history and interpersonal familiarity with the conditions were assessed.
Results:
Results from two simultaneous multiple regressions showed that more positive beliefs about anorexia nervosa and muscle dysmorphia were uniquely associated with more eating disorder symptoms for both male and female participants. Effect sizes for these relationships were medium to large (partial eta-squared = 0.09–0.10). The relationships were not moderated by the sex of the participant, nor the sex of the character.
Conclusions:
Although preliminary, these findings suggest that, among young men and women, positive beliefs about anorexia nervosa and muscle dysmorphia may contribute to the development and maintenance of these conditions. Some symptoms of muscle dysmorphia may be perceived as ego-syntonic, providing another parallel with anorexia nervosa.
Anorexia nervosa is among the few mental illnesses that sufferers experience as ego-syntonic. Individuals with anorexia nervosa often deny that they have a problem and perceive their symptoms as positive or comforting, resulting in delayed treatment seeking, poor engagement with treatment and treatment refusal (Guarda, 2008; Mond et al., 2006). Evidence suggests that young peoples’ positive beliefs about the symptoms of anorexia nervosa, such as the belief that these symptoms are desirable or admirable, are associated with higher levels of eating disorder pathology (Mond et al., 2006). An implication of these findings is that positive beliefs about anorexia nervosa may contribute to the development and maintenance of the condition, providing a target for prevention and intervention programs aimed at curtailing the development of eating disorders.
However, a notable limitation of the extant literature on positive beliefs about anorexia nervosa is that it has been largely confined to women. Epidemiological studies suggest that men account for a substantial minority of eating disorder diagnoses, including up to 33% of diagnoses of anorexia and bulimia nervosa (Hudson et al., 2007) and 25% of early-onset eating disorder diagnoses (Madden et al., 2009). Further, among Australian men, the prevalence of eating disorder behaviours has increased during the past two decades (Hay et al., 2008) with some behaviours, namely extreme dieting and purging, increasing faster among Australian men than women (Mitchison et al., 2013). Despite these trends, no research to date has examined whether the link between positive beliefs about anorexia nervosa and eating disorder symptoms generalises from women to men. Previous research has shown that men are more critical and more stigmatising of individuals with anorexia nervosa than women (Griffiths et al., 2013), that the public associates eating disorders in men with reduced masculinity (Griffiths et al., in press; Räisänen and Hunt, 2014; Robinson et al., 2013), and that muscularity-oriented body and eating concerns, not thinness-oriented body and eating concerns, are associated with increased conformity to masculine norms among men (Griffiths et al., 2014). These perceptions may have the effect of reducing the desirability of the condition for men.
A second limitation of the extant literature on positive beliefs about anorexia nervosa and eating-disordered behaviour more generally is that is has not yet examined beliefs about ‘muscle dysmorphia’. Muscle dysmorphia, formerly named ‘reverse anorexia’ (Pope et al., 1993), is a psychological condition currently classified in the DSM-V as a subtype of body dysmorphic disorder in which sufferers are preoccupied with their body shape and weight, enforce rigid diets and exercise routines to increase their muscularity, and experience substantial impairment in their occupational, social and interpersonal functioning (Murray et al., 2012; Olivardia et al., 2000; Pope et al., 2005). The claim that muscle dysmorphia may belong to the eating disorder spectrum is based on substantial overlap in eating disorder symptoms and body dissatisfaction, a shared preoccupation with body shape, size and weight, and frequent diagnostic cross-over between the conditions (Mosley, 2009; Murray et al., 2010, 2012). Epidemiological data for muscle dysmorphia are presently unavailable.
An understudied aspect of muscle dysmorphia is that, similar to anorexia nervosa, sufferers may experience the condition as ego-syntonic. Research suggests that muscle dysmorphia is often associated with self-denial about the problem and positive beliefs about harmful dieting, exercise routines and steroid use (Pope et al., 2005). Thus, there is reason to believe that the link between positive beliefs about anorexia and eating disorder symptomatology may also exist for muscle dysmorphia. Further, differences in the ‘ideal’ body type pursued by men and women suggest that the link between positive beliefs and anorexia nervosa and muscle dysmorphia may be sex-dependent, namely, women may be more likely to report positive beliefs about anorexia nervosa whereas men may be more likely to report positive beliefs about muscle dysmorphia.
With these considerations in mind, the goal of the current study was to examine sex differences in the associations between young peoples’ positive beliefs about anorexia nervosa and muscle dysmorphia and their own levels of eating disorder psychopathology. Consistent with previous research (Mond et al., 2006), it was hypothesized that more positive beliefs about anorexia nervosa would be associated with higher levels of eating disorder symptoms. Further, it was hypothesized that this association would be stronger for women than for men. Similarly, we hypothesized that more positive beliefs about muscle dysmorphia would be associated with higher levels of eating disorders symptoms. However, given that the ideal body type for young men is characterised by drive for muscularity, rather than drive for thinness (Pope et al., 2000; Ridgeway and Tylka, 2005; Strandbu and Kvalem, 2012), it was expected that the association between positive beliefs about muscle dysmorphia and levels of eating disorder symptoms would be stronger for men than for women.
Method
Participants
Participants were 521 undergraduates enrolled in an introductory psychology course at the University of Sydney who received course credit in return for their participation.
Data exclusion
Two valid-responding checks were included in the study. The first was an item embedded in the survey that directed participants to select ‘Markedly’ as their response for that item. The second check at the end of the study asked participants to name the character that they had been answering questions about. The proportion of correct responses to these questions was 91.7% and 88.7%, respectively. Twenty-eight participants who failed both valid-responding checks, or who otherwise provided an opposite-sex name for their character, had their data excluded. One additional participant was excluded because they indicated their sex as transgender (n = 1).
Participant characteristics
The post-exclusion sample of 492 participants included 179 men and 313 women (age range, 16–40 years; M = 19.36, SD = 2.76). Participants’ were predominantly Australian (57.8%), followed by North-East Asian (12.0%), South-East Asian (7.1%), and Southern and Central Asian (5.9%), with 17.2% indicating other backgrounds. Mean body mass index (BMI) for men was 23.95 (SD = 3.90), and for women, 22.04 (SD = 5.31). The BMI of the whole sample was in the range of 15.52–68.03 with a mean of 22.73 (SD = 4.92).
Materials and measures
Character descriptions
As shown in Appendix A, four character descriptions described either a male (‘Michael’) or female (‘Kelly’) character who was experiencing symptoms of either anorexia nervosa or muscle dysmorphia. The descriptions, which were closely based on research materials developed by Mond and colleagues (2004a, 2006) to assess individuals’ beliefs about people with bulimia nervosa (Mond et al., 2004a) and anorexia nervosa (Mond et al., 2006), described clinically significant symptoms of anorexia nervosa and muscle dysmorphia but did not explicitly state diagnoses. The decision to include a male and female version of the character for each mental condition was made so that the potential effect of the characters’ sex on participants’ beliefs could be examined and controlled for. All authors were involved in the creation of the character descriptions and consensus was reached on the final descriptions used.
Positive beliefs
Three items that assessed participants’ positive beliefs about the characters’ eating disorder symptoms were adapted from research by Mond and colleagues (2004a, 2006). The items assessed admiration for the character’s control over their eating: ‘How much do you admire Michael’s/Kelly’s ability to control his/her eating?’, control over their exercise: ‘How much do you admire Michael’s/Kelly’s ability to control his/her exercise?’, and desire to be more like the character: ‘Have you ever thought it might not be too bad to be someone like Michael/Kelly?’ Participants rated their level of agreement using a 5-point scale that ranged from ‘Not at all’ to ‘A great deal’ for the first two items, and from ‘Never thought it’ to ‘Always thought it’ for the last item. The content of the three items reflects the proposed centrality of self-control over eating and exercise in anorexia nervosa (Fairburn et al., 2003), the centrality of exercise in male presentations of anorexia nervosa (Murray et al., 2013), and evidence that self-control over eating and exercise are also central to muscle dysmorphia (Murray et al., 2012).
Eating disorder symptoms
The 22-item attitudinal component of the Eating Disorder Examination – Questionnaire (EDE-Q) (Fairburn & Beglin, 1994) was used to measure the occurrence and frequency of key eating disorder features during the past 28 days. A global score was calculated by averaging the mean scores of each of the four subscales of the EDE-Q – Dietary Restraint, Eating Concerns, Weight Concerns and Shape Concerns – that address key attitudinal aspects of eating disorder symptomatology. The global score can range from 0 to 6 with higher scores indicating higher levels of symptomatology. The EDE-Q has demonstrated sound psychometric properties in non-clinical women, although reliability and internal consistency has tended to be lower for non-clinical men (Mond et al., 2004b; Reas et al., 2012). Cronbach alphas for the EDE-Q global score in the current study sample were 0.92 and 0.95 for male and female participants, respectively.
Other measures
Data were also collected about participants’ personal mental health history with anorexia nervosa and muscle dysmorphia, their level of contact with others who have experienced anorexia nervosa or muscle dysmorphia, and their level of knowledge about anorexia nervosa and muscle dysmorphia. Participants were also asked to estimate sex differences in the prevalence of both conditions. BMI was calculated from participants’ self-reported height and weight. BMI calculated from self-report data is highly correlated (r = 0.97) with clinician-derived BMI (Mond et al., 2004c).
Procedure
Participants were randomly allocated to one of four groups using the random number function in Microsoft Excel. Each group of participants was directed to an online survey that contained the character description that corresponded to their group. Participants were asked to carefully read the description and were then asked to complete the questions addressing positive beliefs about the characters as well as items of the EDE-Q. The study was approved by the University of Sydney’s Human Research and Ethics Committee. This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Statistical analyses
All statistical analyses were conducted using SPSS version 21. Continuous data pertaining to participants’ positive beliefs about the characters and participants’ estimates of sex differences in the prevalence of the characters’ conditions were analysed using one-way ANOVAs. Categorical data pertaining to participants’ level of knowledge about the characters’ conditions, interpersonal familiarity with the characters’ conditions, and personal history with the characters’ conditions, were analysed using chi-square tests of independence.
Factor analysis
The three items measuring positive beliefs were submitted to an exploratory factor analysis using Principal Axis Factoring with Oblimin rotation. Results indicated that the data were unidimensional; the ratio of the largest eigenvalue to the next largest was 3.61, above the undimensionality threshold heuristic of 3.0 (Morizot et al., 2007). Thus, a single factor was extracted that represented positive eating- and exercise-related beliefs about a person with eating- and exercise-related problems. This factor was subsequently employed as the outcome variable in two multiple regressions.
Multiple regression analysis
Categorical data were recoded into dichotomous variables appropriate for linear regression: Personal history with the condition (yes/no), level of contact with others with the condition (none/some), and level of knowledge (some/a lot, for anorexia nervosa, and none/some, for muscle dysmorphia, reflecting participants’ higher level of knowledge about anorexia nervosa than muscle dysmorphia).
The first regression examined variables associated with positive beliefs about anorexia nervosa. At step 1, the independent variables were eating disorder symptoms, BMI, age, the sex of the participant, the sex of the character, level of knowledge about anorexia nervosa, interpersonal familiarity with anorexia nervosa and personal history of anorexia nervosa. At step 2, an interaction term representing the hypothesised interaction between participant sex and eating disorder symptoms was entered.
The second regression examined variables associated with beliefs about muscle dysmorphia followed the same procedure as the first regression. However, the variable representing personal history with muscle dysmorphia was not entered because very few participants reported any personal history with the condition.
Each of the statistical assumptions that underlie multiple regression were tested and satisfied. Cases with missing data were handled using listwise deletion and, overall, there were very little missing data.
Results
Table 1 shows the proportion of participants who selected each response option for questions that assessed positive beliefs about the characters, familiarity with anorexia nervosa and muscle dysmorphia (personal history, interpersonal familiarity and level of knowledge), and beliefs about the prevalence of the conditions. Characters with muscle dysmorphia were significantly more admired for their ability to control both their eating, F(1, 488) = 56.07, P <0.001, and exercise, F(1, 488) = 23.93, P <0.001, relative to characters with anorexia nervosa, and participants endorsed significantly more frequent thoughts that it ‘might not be too bad’ to be like the character with muscle dysmorphia, F(1, 488) = 18.81, P <0.001. Further, participants reported significantly more knowledge about anorexia nervosa, χ2(2, N = 488) = 205.78, P <0.001, significantly more interpersonal familiarity with anorexia nervosa, χ2(4, N = 486) = 10.57, P = 0.032, and significantly more personal history with anorexia nervosa,χ2(3, N = 485) = 22.10, P <0.001, relative to muscle dysmorphia. When asked about sex differences in the prevalence of the conditions, participants estimated that 28.5% of individuals with anorexia nervosa would be men compared to 67% of individuals with muscle dysmorphia, and this difference was significant, F(1, 486) = 635.99, P <0.001.
Percentage (%) of participants endorsing responses for each question. Percentages for participants who read the description of a character with anorexia nervosa (AN, n = 236) appear to the left of the percentages for participants who read the description of a character with muscle dysmorphia (MD, n = 256).
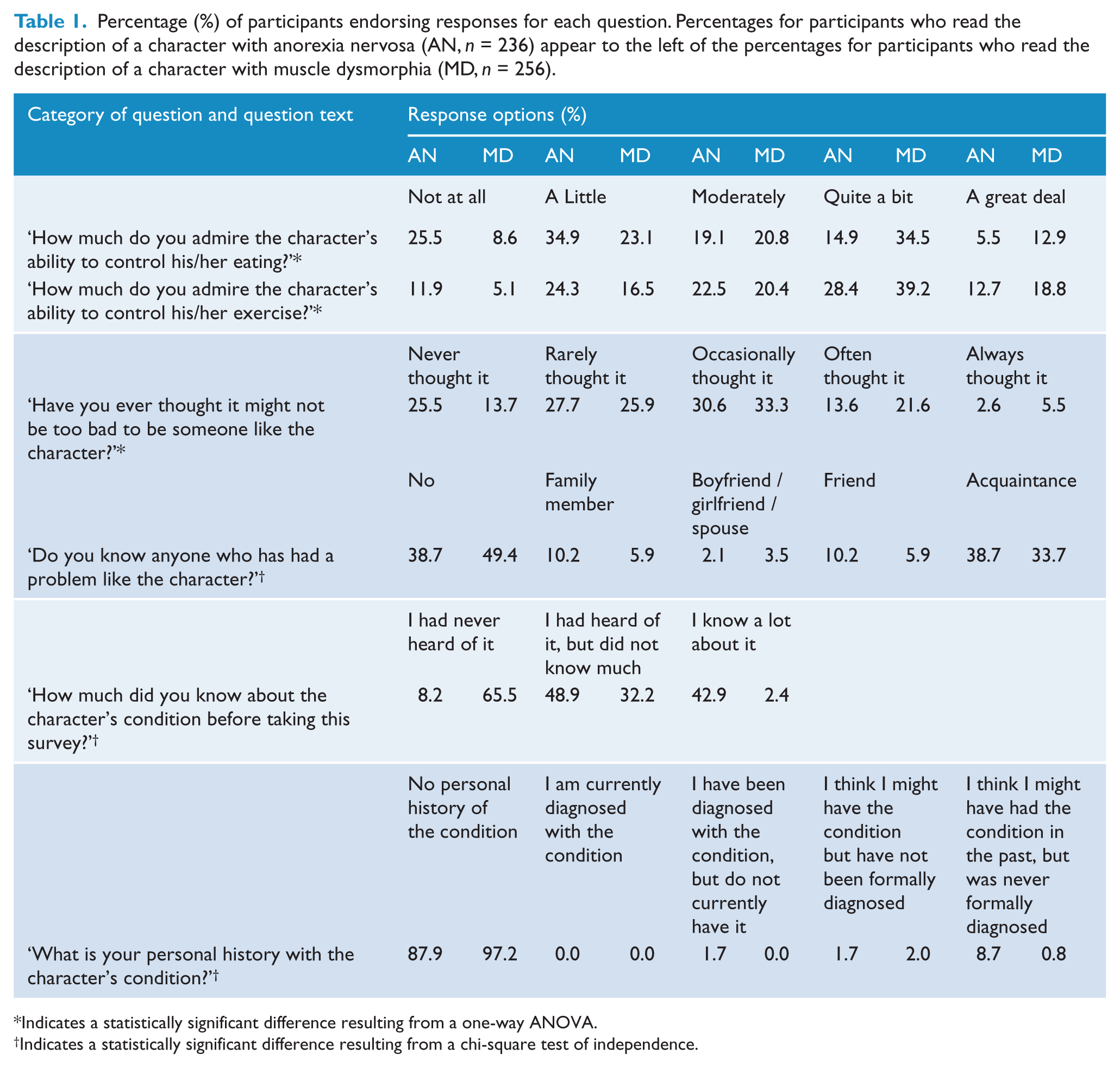
Indicates a statistically significant difference resulting from a one-way ANOVA.
Indicates a statistically significant difference resulting from a chi-square test of independence.
Regression – positive beliefs about anorexia nervosa
The regression for positive beliefs about anorexia nervosa was significant at Step 1, R2 = 0.16, F(8, 222) = 5.20, P <0.001. The addition of the interaction term at Step 2 did not contribute a significant proportion of explained variance to the model, ΔR2 = 0.01, F(1, 221) = 3.18, P = 0.076. Thus, the model at Step 1 was retained. Statistical output from this regression model is shown in Table 2. All the assumptions of multiple regression were satisfied; independent residuals (Durbin-Watson statistic = 1.97), no multicollinearity (Variance Inflation Factors were in the range of 1.04–1.39), no outliers (standardized residuals were in the range of −1.73−2.55, outlier threshold = ± 3), no excessively influential data points (Cook’s Distance values <0.42), linear relationships between the continuous independent variables and the outcome variable, and homoscedasticity.
Simultaneous multiple regression for positive beliefs about a character with clinically significant symptoms of anorexia nervosa.
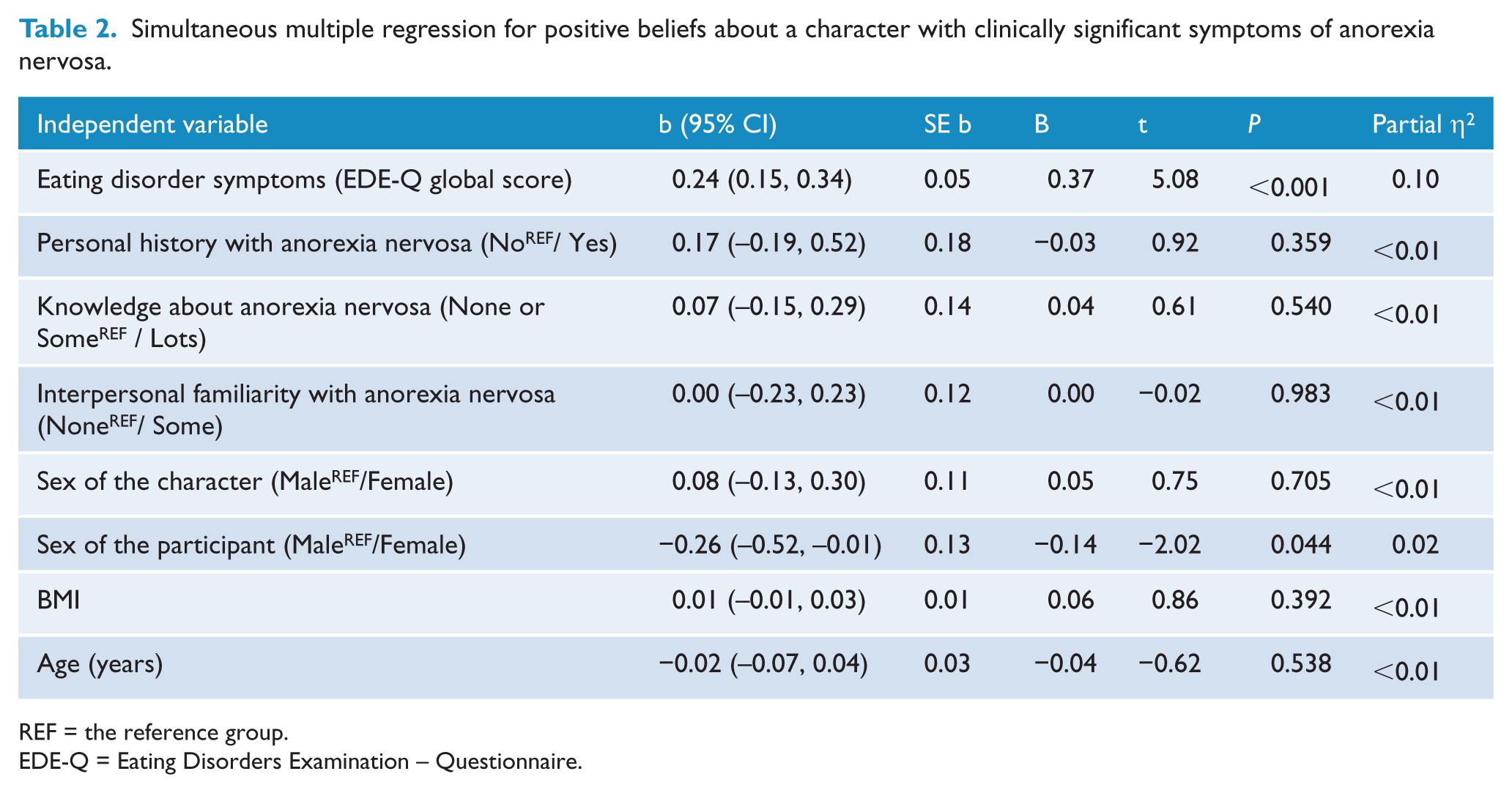
REF = the reference group.
EDE-Q = Eating Disorders Examination – Questionnaire.
Two significant associations emerged, namely eating disorder symptoms and the sex of the participant. More marked eating disorder symptoms were associated with more positive beliefs about anorexia nervosa and women had less positive beliefs about anorexia nervosa than men.
Regression – positive beliefs about muscle dysmorphia
The regression for positive beliefs about muscle dysmorphia was significant at Step 1, R2 = 0.16, F(7, 246) = 6.59, P <0.001. The addition of the interaction term at Step 2 did not contribute a significant proportion of explained variance to the model, ΔR2 = 0.01, F(1, 245) = 2.54, P = 0.113. Thus, the model at Step 1 was retained. Statistical output from this regression model is shown in Table 3. All the assumptions of multiple regression were satisfied; independent residuals (Durbin-Watson statistic = 1.91), no multicollinearity (Variance Inflation Factors were in the range of 1.04–1.33), no outliers (standardized residuals were in the range of −2.76–2.17), no excessively influential data points (Cook’s Distance values <0.06), linear relationships between the continuous independent variables and the outcome variable, and homoscedasticity.
Simultaneous multiple regression for positive beliefs about a character with clinically significant symptoms of muscle dysmorphia.
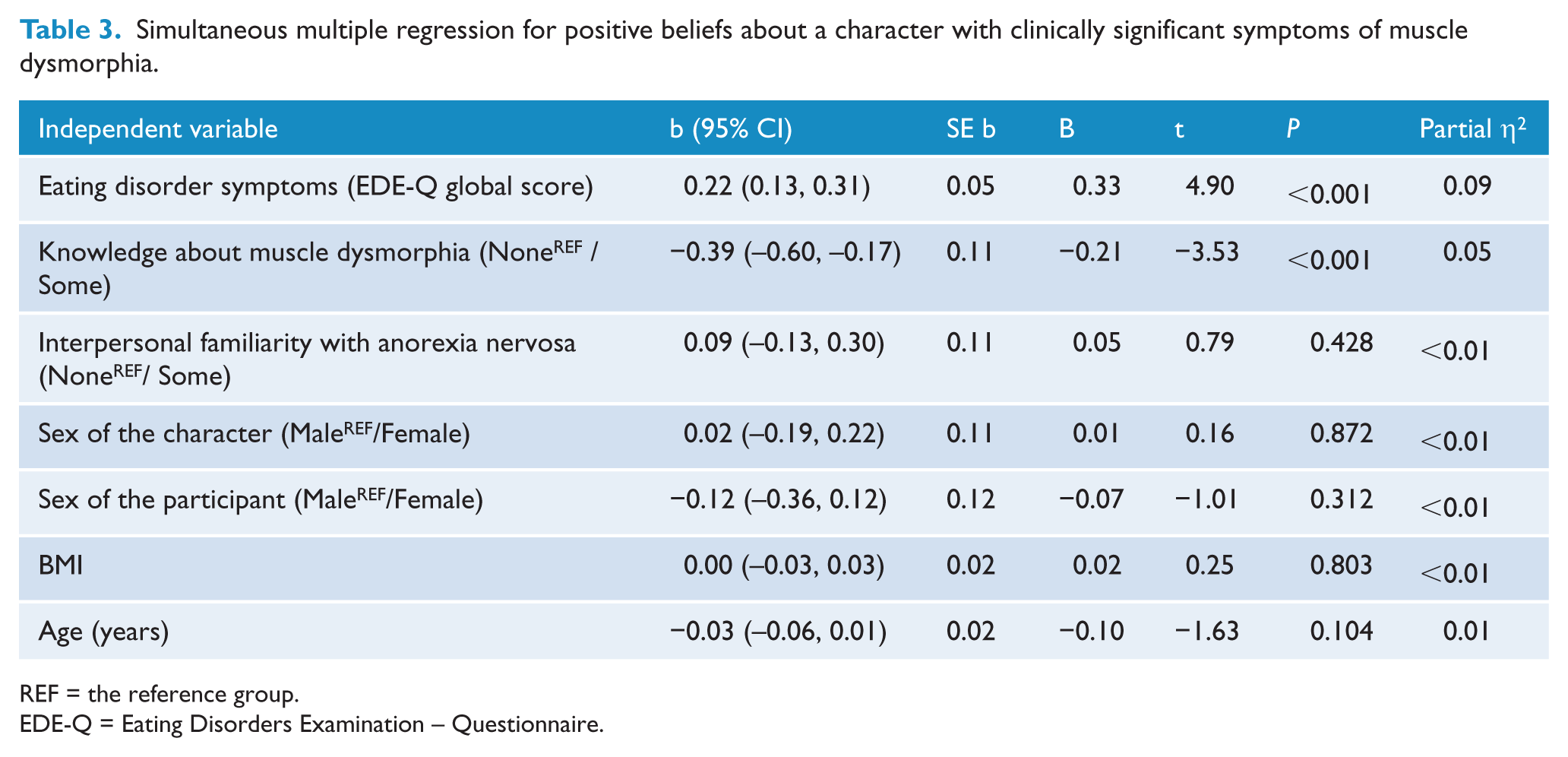
REF = the reference group.
EDE-Q = Eating Disorders Examination – Questionnaire.
Two significant associations emerged, namely eating disorder symptoms and participants’ level of knowledge about muscle dysmorphia. More marked eating disorder symptoms were associated with more positive beliefs about muscle dysmorphia and participants with some knowledge about muscle dysmorphia had less positive beliefs about the condition than participants who reported no knowledge about muscle dysmorphia.
Discussion
The present study examined whether more positive beliefs about anorexia nervosa and muscle dysmorphia would be associated with more marked eating disorder symptoms among male and female university students. These associations were substantiated insofar as the results from two multiple regressions showed that more marked eating disorder symptoms were uniquely associated with more positive beliefs about characters with anorexia nervosa and muscle dysmorphia. The effect size indicators for these associations were moderate to large (partial eta-squared = 0.09–0.10), suggesting that a substantial proportion of the variance in positive beliefs about the conditions may be attributable to participants’ own eating disorder symptoms. Further, these associations did not interact with the sex of the participant, suggesting that the relationships between positive beliefs and eating disorder symptoms are of equal strength for men and women. Taken together, the results point to the potential significance of positive beliefs about anorexia nervosa and muscle dysmorphia in those who endorse eating disorder attitudes and behaviours.
The present findings are consistent with previous findings showing substantial positive valuation of anorexia nervosa symptoms among female university students (Mond et al., 2006). In fact, positive valuation of anorexia nervosa symptoms in the present study was higher than in previous research. When participants were asked about their admiration for the ability of the character with anorexia nervosa to control their eating and exercise, 39.5% and 63.6% reported ‘moderately’, ‘quite a bit’ or ‘a great deal’, respectively. Further, 46.8% of participants had ‘occasionally’, ‘often’ or ‘always’ thought that it ‘might not be too bad’ to be like the character. The higher percentages observed in the present study may be because male participants were recruited in the present study but were absent in the sample recruited by Mond and colleagues (2006). In extending previous findings to include male participants, men, somewhat surprisingly, reported more positive beliefs about the character with anorexia nervosa than women, which may reflect men’s tendency to view anorexia nervosa as a less serious condition than women do (Griffiths et al., 2013).
In extending existing evidence to incorporate muscle dysmorphia, the findings point towards the substantial positive valuation of muscle dysmorphia symptoms among both male and female university students. For instance, when asked about their admiration for the ability of the character with muscle dysmorphia to control their eating and exercise, 68.2% and 78.4% reported ‘moderately’, ‘quite a bit’ or ‘a great deal’, respectively. Further, 60.4% of participants had ‘occasionally’, ‘often’ or ‘always’ thought that it ‘might not be too bad’ to like the character. Positive valuation was significantly higher for muscle dysmorphia than for anorexia nervosa. It may be that muscle dysmorphia generates less stigma than anorexia nervosa (Griffiths et al., 2013), making it more desirable and/or acceptable to hold positive beliefs toward the former. Nevertheless, the findings are novel in showing that muscle dysmorphia, unlike most mental illnesses, is subject to positive valuation by considerable numbers of university students.
Moreover, the positive valuation reported for symptoms of both anorexia nervosa and muscle dysmorphia was uniquely associated with greater endorsement of eating disorder symptomatology for both men and women. This association was of equal strength for both sexes and the strength of the association observed between positive beliefs about muscle dysmorphia and eating disorder symptomatology was comparable to that for anorexia nervosa. Thus, it appears that university-attending men and women who are highly invested in muscularity- or thinness-oriented eating, exercise, weight and shape (and the control thereof) report more admiration and desire to be like a character who has attained some degree of control over their eating, exercise, weight and shape, even if this control is clearly deleterious to the characters’ wellbeing. This positive valuation of the symptoms of anorexia nervosa and muscle dysmorphia may be of considerable clinical significance to those treating these conditions and to researchers who study prevention and early-intervention programs aimed at disordered eating and eating disorders.
Taken together, these findings suggest that greater consideration may need to be given to the potential role of positive beliefs about both thinness- and muscularity-oriented eating disordered behaviour as a factor in the development and/or maintenance of eating disorder symptoms. The findings also suggest that prevention and early intervention programs may need to give greater attention to positive beliefs about eating disorder symptoms. Greater attention to men and their beliefs in particular may be warranted, given that many current programs are heavily female-centric. Considerations already applied to female-oriented programs may be adapted to male-orientedprograms. For example, it has been suggested that female-oriented prevention programmes delivered by slender women recovered from eating disorders may unwittingly increase eating disorder symptoms among participants (Mann et al., 1997). For male-oriented prevention programs, it may be prudent to reconsider employing men recovered from muscle dysmorphia if they are large and muscular and embody the ‘muscular ideal’, lest there be a similar deleterious effect on participant outcomes.
Limitations of the present study should be noted. Relatively few items were used to assess positive beliefs about the respective conditions and the descriptions of these conditions employed did not undergo a process of external validation, for example, by mental health professionals. However, the anorexia nervosa vignette was closely based on those used in previous research and the muscle dysmorphia vignette was adapted from this based on the clinical experience of the authors. Further, since knowledge of muscle dysmorphia among mental health professionals may be limited (Murray and Touyz, 2013), validation of this kind may not be straightforward. The cross-sectional study design limits any inferences concerning the direction of the observed associations. It is plausible that individuals develop eating disorder symptoms independently of their beliefs about eating disorders and then retrospectively rationalise their behaviour as admirable or positive (Mond et al, 2004a). Finally, reliance on a student sample may limit the generalisability of the findings. However, the fact that the focus of the study was on associations between positive beliefs about the conditions in question and eating disorder symptoms, rather than positive beliefs or eating disorder symptoms per se, may limit concerns relating to sample bias. In any case, for all these reasons, the current research should be viewed as a preliminary investigation.
Notwithstanding these limitations, the present study suggests that more positive attitudes about anorexia nervosa and muscle dysmorphia are associated with higher levels of eating disorder symptoms among male and female university students. The results highlight the importance of including men in future research on the ego-syntonic qualities of eating disordered behaviour and of anorexia nervosa and muscle dysmorphia. Tackling the perceived desirability of these conditions poses a unique challenge for preventive interventions that have, historically, been largely confined to thinness-oriented eating and body image concerns as these present in women.
Footnotes
Appendix A
Declaration of interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.