
Abstract
Objectives:
Individuals with bipolar disorder are more frequently overweight or obese than the general population, but the reasons for this association are unknown. The aim of this study is to further understand the etiology of overweight and obesity in bipolar disorder.
Methods:
We invited patients in a specialty outpatient bipolar clinic to complete the Eating Inventory. Patients provided self-reported restraint, disinhibition, and perceived hunger as well as general perceptions of dietary intake.
Results:
Sixty-two individuals (37 female) between the ages of 18 and 67 (M = 41.5, SD = 13.38) and with an average body mass index (BMI) of 27.18 (SD = 5.71) completed the survey. Disinhibition and perceived hunger were positively correlated with BMI and self-reported difficulty eating healthy foods. Restraint was positively correlated with healthy eating (ps < .05). Stepwise linear regressions revealed that hunger was the most significant predictor of BMI (F(1) = 8.134, p = .006). Those participants with bipolar I or II disorder reported greater hunger scores (p < .01) and difficulty eating healthily (p < .05) than those without a full diagnosis.
Conclusions:
These results suggest that disinhibition and perception of hunger may be linked to the disproportionately high rate of obesity in bipolar disorder.
Introduction
Bipolar disorder is a severe, chronic, and recurrent mental illness, often characterized by episodes of mania, hypomania, and depression, along with poor quality of life and functioning and multiple psychiatric and medical comorbid conditions (Coryell et al., 1993; Salvatore et al., 2007; Young and Grunze, 2013). In particular, risk factors for cardiovascular disease (e.g. obesity, hypertension) and unhealthy lifestyle behaviors (e.g. poor nutrition, sedentary behavior) are disproportionately present among individuals with bipolar disorder as compared to the general population (Young and Grunze, 2013). Extant research estimates that over half of patients with bipolar disorder are overweight and that 20–40% are obese (McElroy and Keck, 2012). Increased weight and obesity are associated with worse course of illness, depressive symptoms, and treatment outcomes, in addition to shortened life spans (Fagiolini and Goracci, 2009). Pharmacotherapy is the first line of treatment for bipolar disorder, yet many medications are associated with weight gain and increased risk of cardiometabolic conditions, most notably lithium, valproate, olanzapine, and quetiapine (Torrent et al., 2008). Moreover, treatment-emergent weight gain tends to lessen treatment adherence and may not be fully reversed by changing medications to those less likely to cause weight gain, such as aripiprazole, ziprasidone, and lurasidone (McElroy et al., 2007; Stauffer et al., 2009). Additionally, existing psychosocial treatments aimed at weight loss have proven limited in their efficacy and feasibility (Daumit et al., 2013; Van Citters et al., 2010). As a result, there is a need to understand the relationship between obesity and bipolar disorder such that better, more focused treatments can be developed to prevent and treat weight gain in this clinical population.
A potential target of psychosocial interventions is eating behavior, as individuals with bipolar disorder tend to have poor nutrition (Fagiolini et al., 2008; Sylvia et al., 2013), yet there is a dearth of knowledge about the role of eating pathology in this pattern or in making lifestyle changes. In non-psychiatric samples, psychosocial eating behavior has significantly predicted the presence of metabolic syndrome and related disorders, even after adjusting for body mass index (BMI) and age (Hainer et al., 2006). Thus, the present study examines cognitive restraint, disinhibition, and perceived hunger as well as patients’ overall perceptions of their dietary intake using the Eating Inventory (Three Factor Eating Questionnaire; EI) and their association with BMI (Stunkard and Messick, 1985). To the best of our knowledge, the EI has only been used in one study examining bipolar disorder, however this study collapsed data for participants with bipolar disorder, schizophrenia, and schizoaffective disorder (Stauffer et al., 2009). Moreover, previous studies examining eating pathology have been limited in their application to bipolar disorder as they have often excluded participants with mental illness or those taking medications known to affect weight, metabolism, or appetite, or have not examined clinical levels of mood symptoms (Williamson et al., 2007). Thus, given the significant burden of obesity and related conditions in bipolar disorder and the lack of successful psychosocial or pharmacological preventative or therapeutic interventions, research on the role of psychosocial eating behavior in this population is a notable gap in the literature.
In this study, we hypothesized that BMI would be positively associated with disinhibition and perceived hunger and negatively associated with restraint, as it appears in non-psychiatric samples (Aldhoon Hainerová et al., 2013; Hainer et al., 2006). We expected that high restraint would be associated with healthy eating habits, as restraint was shown to be negatively associated with weight gain (Hays et al., 2002), and that low restraint and high disinhibition would be associated with unhealthy eating. We predicted that participants with a bipolar I or II diagnosis would report less restraint, more disinhibition, and greater perceived hunger than those with bipolar not otherwise specified or who were undiagnosed. Furthermore, lower restraint, higher disinhibition, and greater degree of feeling hungry are generally associated with poor health-related quality of life, and lower mood and psychosocial dysfunction; we would expect such characteristics to be more severe in those with a bipolar diagnosis compared to a sub-threshold diagnostic presentation (Karlsson et al., 1998). Finally, we expected that women in the sample would have, on average, greater BMI and report more disinhibition, as was found in other samples (Provencher et al., 2003; Sicras et al., 2008).
Methods
Participants
The present data were collected as a survey administered to individuals waiting in an outpatient clinic specializing in the treatment of bipolar disorder. The Institutional Review Board approved all procedures and participants completing the survey provided written consent. Participants (N = 62, 60% female) were 18 years of age or older and asked to provide demographic information (e.g. age, gender, diagnosis, height, weight, race, ethnicity, level of education), complete the EI, and answer two additional questions on their eating habits.
Measures
The EI assesses psychosocial eating behaviors and attitudes (Stunkard and Messick, 1985). Responses are recorded on a yes/no binary scale or a 1 to 4 Likert scale. This measure has demonstrated good internal consistency, reliability, and validity (Cappelleri et al., 2009; Stunkard and Messick, 1985) and is not affected by transient hunger state (Witt et al., 2014). As described above, the EI encompasses three subscales: Restraint (the cognitive ability to restrain food intake; maximum possible score = 21), Disinhibition (tendency to lose control over eating; maximum possible score = 16), and Hunger (the perception of hunger; maximum possible score = 14). In addition to the EI, we developed two questions: (1) How healthy/nutritious are your eating habits? (‘Healthy Question’) and (2) How difficult is it for you to eat foods that are healthier/more nutritious? (‘Difficulty Question’). Participants responded on a 1 (unhealthy/not difficult) to 5 (very healthy/very difficult) scale.
Analyses
Pearson’s correlation coefficients were computed to assess the association of eating behavior and attitudes in our sample. T-tests were used to assess potential gender and diagnostic differences on eating behavior and BMI. We conducted stepwise linear regression analyses to evaluate how the EI subscales, Healthy Question, or Difficulty Question may predict BMI.
Results
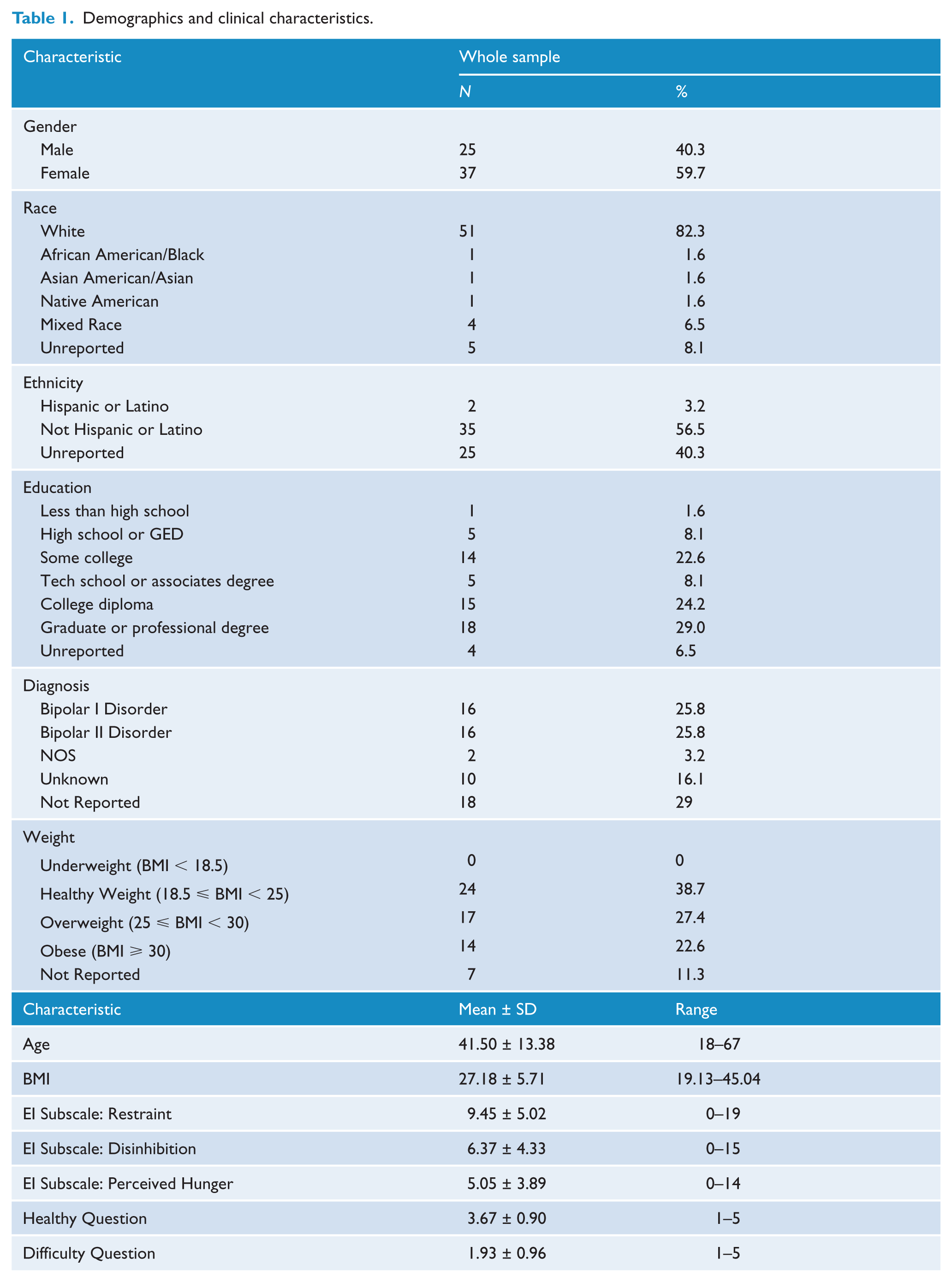
Demographic and clinical characteristics of the sample and a summary of questionnaire responses are presented in Table 1. Half of participants were overweight or obese (n = 31). As expected, healthy eating was positively associated with Restraint, but negatively correlated with the Difficulty Question, or difficulty eating well (ps < .001). BMI and difficulty eating well were positively correlated with Disinhibition (p = .024; p = .001) and Hunger (p = .009; p = .002). Finally, Disinhibition and Hunger were positively correlated (p < .001) (see Table 2). Men and women did not differ in their responses to any of the subscales of the questionnaire, however the mean BMI of men (M = 29.3, SD = 6.5) exceeded that of women (M = 25.7, SD = 4.7) (p = .01). Stepwise linear regressions revealed that Hunger was the most significant predictor of BMI, accounting for 13.5% of the variance (F(1) = 8.134, p = .006) (See Figure 1 for scatterplot). No other variables reached statistical significance.
Demographics and clinical characteristics.
Correlations between BMI and questionnaire factors in the whole sample.
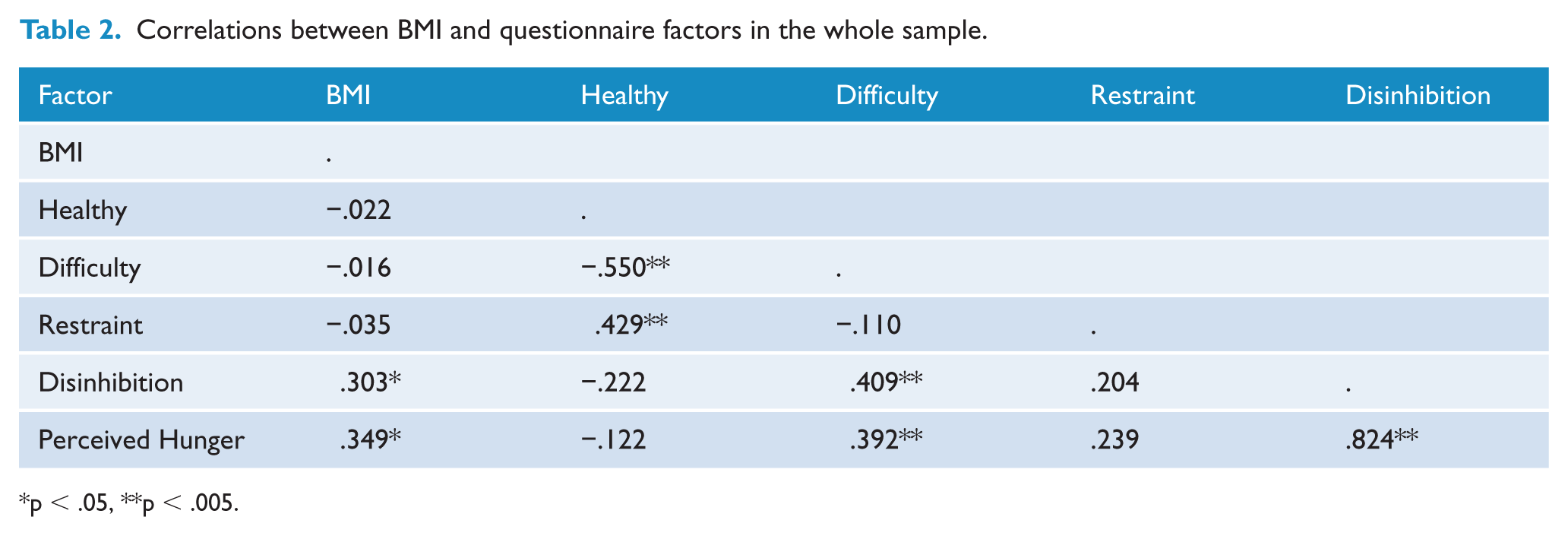
p < .05, **p < .005.
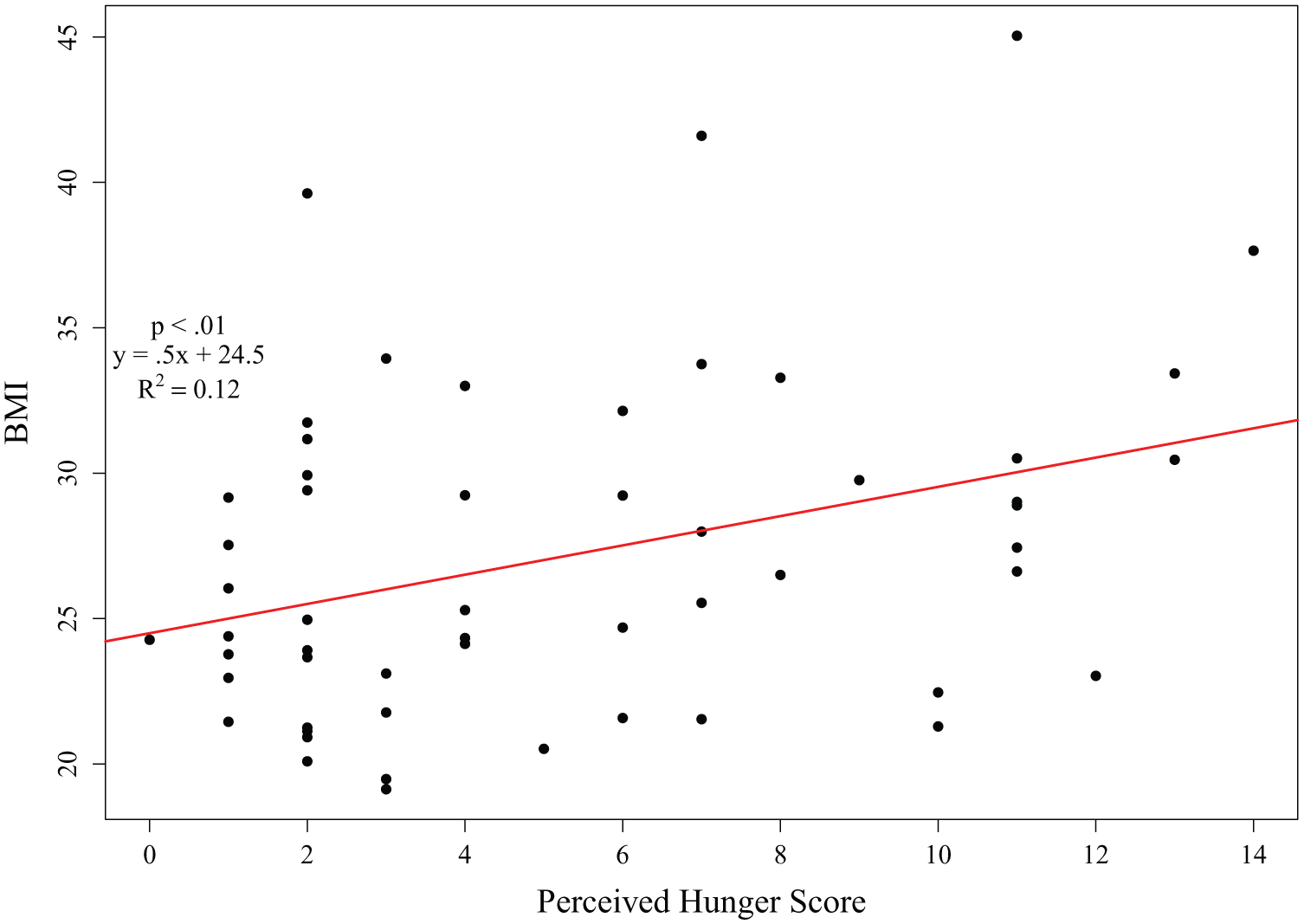
Scatterplot of self-reported hunger and body mass index (BMI).
When the sample was divided into a bipolar group (bipolar I or II diagnosis) and a sub-threshold group, diagnosis proved to be a significant predictor of subscale scores. The bipolar group (M = 6.5, SD = 4.0) reported greater Hunger scores than the sub-threshold group (M = 3.1, SD = 2.1) (t(60) = 4.15, p < .01). The bipolar group also reported greater difficulty eating healthily (M = 2.2, SD = 1.0) than the sub-threshold group (M = 1.7, SD = 0.7) (t(60) = 2.27, p < .05). Within the bipolar group, those with bipolar I disorder (M = 3.3, SD = .95) endorsed significantly less healthy eating habits than those with bipolar II disorder (M = 4.1, SD = .7) (t(30) = 2.71, p < .05). Participants with bipolar I disorder (M = 2.6, SD = 1.2) also reported more difficulty eating healthily than those with a bipolar II diagnosis (M = 1.8, SD = .7) (t(30) = 2.30, p < .05).
Discussion
Healthy eating was positively associated with restraint, and as expected, negatively associated with difficulty eating well. Greater disinhibition was correlated with greater perceived hunger, and both were correlated with greater BMI and difficulty eating well. Of all the subscales, perceived hunger was the most significant predictor of BMI. Although men and women did not differ on any of the subscales, men reported greater BMI on average than women, which was unexpected. Individuals with a bipolar I or II diagnosis reported greater hunger and difficulty eating well than the other participants. Furthermore, those with bipolar I disorder reported less healthy eating habits and more difficulty eating healthily than those with bipolar II disorder.
These data are consistent with previous studies conducted in non-clinical populations, in that perceived hunger and disinhibition are positively correlated, but neither is correlated with restraint (Williamson et al., 1995). Participants who reported greater restraint in their eating tended to also report eating healthier; this is consistent with our finding that greater disinhibition and perceived hunger are associated with higher BMI and difficulty eating healthily. We expected this latter finding as decreased disinhibition and perceived hunger have been associated with weight loss in other samples (Aldhoon Hainerová et al., 2013; Stunkard and Messick, 1985). Additionally, impulsivity and diminished inhibition are common trait characteristics of bipolar disorder (Strakowski et al., 2010) that could reasonably translate to loss of control when eating, regardless of mood state. This finding with disinhibition could also partially explain the prevalence of comorbid binge eating in bipolar disorder (Castrogiovanni et al., 2009). Although restraint has been shown to relate to weight loss (Aldhoon Hainerová et al., 2013), it is slightly more complicated, as it can also be associated with bingeing with and without mood dysregulation and eating disorders (Allen et al., 2012; Blomquist and Grilo, 2011; Lowe and Maycock, 1988). These mixed findings could explain our null finding between restraint and BMI. Furthermore, it has been suggested that in healthy and depressed individuals actual eating behavior (rather than perceived intake) is more influenced by disinhibition compared to restraint (Smith et al., 1998).
Perceived hunger emerged as the greatest predictor of BMI. This is notable in a population comprised of individuals with bipolar disorder or related symptoms. Many psychiatric medications, particularly atypical antipsychotics, can bear side effects of weight gain. It is unclear, however, whether this increased weight is a direct result of the medications or if the medications precipitate weight gain by increasing appetite (Case et al., 2010). A limitation of this study is that we do not have data on participants’ medications, but approximately 45% of individuals with bipolar disorder are typically taking medications associated with weight gain (Rascati et al., 2011; Vancampfort et al., 2013) and we suspect that our sample was representative. Regardless, this study clearly highlights perception of hunger as a critical target of further investigation in a way that previous work has not. The unique role that perceived hunger seems to have on weight gain in bipolar disorder may underlie the disproportionate rates of obesity in this population.
Problem eating behavior commonly presents with psychosocial distress and other psychiatric symptoms, which was highlighted in our study and extended to individuals with severe pathology (Musci et al., 2013). For example, individuals with a full bipolar diagnosis reported more perceived hunger and more difficulty eating healthily than those with sub-threshold diagnoses. Moreover, those with a bipolar I disorder reported eating even less healthily and having even more difficulty eating healthily than those with bipolar II disorder. Thus, clinicians may want to be particularly vigilant of the eating behavior in their bipolar patients who have greater illness severity as well as consider this population at greater risk for gaining weight. These data on psychosocial eating behaviors also suggest the need for targeted therapies that identify and alter maladaptive cognitive and emotional processing to change eating habits and related quality of life (Sylvia et al., 2013). Collaborative approaches integrating pharmacotherapy and lifestyle interventions for weight loss, tailored to the unique presentation and symptoms of bipolar disorder, may be the most helpful for patients in this population (Stauffer et al., 2009).
Results should be considered within the context of the study limitations. First, we do not have data on participants’ medications, which may impact eating behavior and attitudes. For example, medications could impact participants’ perceived hunger and subsequently the prediction of BMI. Thus, it is important to look at eating behavior in all bipolar patients, or those taking and not taking medications, for this work to have good external validity. Future studies will need to explore the specific impact of psychotropic medications on the eating pathology of individuals with bipolar disorder. Additionally, clinical data on current symptoms was not collected. Nutrition and weight importantly appear to be issues for patients with bipolar disorder irrespective of mood state; however studying fluctuations based on changes in mood would be an important next step. This sample may not be representative of the entire bipolar population given the small sample size and that they are receiving or seeking treatment at a bipolar specialty clinic, however, the prevalence of increased weight and obesity in this sample does align with estimates for the larger bipolar population (McElroy and Keck, 2012). Data are self-report which could impact reliability. For example, previous studies have found that women and men with bipolar disorder often do not differ in BMI (Vemuri et al., 2011). Finally, this study is cross-sectional and therefore, we cannot infer causality. Given the scarcity of information on this topic, identifying relationships between specific psychosocial eating behaviors and increased weight for individuals with bipolar disorder proves to be a valuable starting point and merits future study.
In sum, individuals with bipolar disorder exhibit similar eating pathology to the general population, but one notable exception is the association of perceived hunger and BMI. These data indicate the importance of further research on psychosocial eating behavior in bipolar disorder and the importance of not assuming that it wholly maps onto patterns in the general population. Interestingly, participants’ perceptions of how healthy their eating habits were and how difficult it was for them to eat healthily were not associated with BMI, potentially indicating a lack of insight into the nature and consequences of their own eating behaviors. Thus, this study underscores the importance of assisting patients with their perception of hunger, or teaching them the difference between a psychological craving for food versus physiological need, in addition to addressing issues of psychoeducation, disinhibition, and restraint. Research in this area is therefore warranted to improve lifestyle interventions for weight loss in this population in order to address specific behaviors and cognitions in a more targeted way.
Footnotes
Funding
This study was supported in part by the National Institute of Mental Health, grant no. 5K23MH091182-02.
Declaration of interest
Ms. Bernstein reports no conflicts of interest.
Dr. Nierenberg has been a consultant for Abbott Laboratories, Astra Zeneca, Basilea, BrainCells Inc., Brandeis University, Bristol-Myers Squibb, Cephalon, Corcept, Eli Lilly & Co., Forest, Genaissance, Genentech, GlaxoSmithKline, Hoffman-LaRoche, Innapharma, Janssen Pharmaceutica, Jazz Pharmaceuticals, Lundbeck, Merck, Neuroscience Education Institute, Novartis, PamLabs, PGx Health, Pfizer, Ridge Diagnostics, Roche, Sepracor, Schering-Plough, Shire, Somerset, Sunovion, Takeda, Targacept, and Teva. He has stock or potential stock in Appliance Computing, Inc. (MindSite); Brain Cells, Inc., InfoMed (potential share of income) and Medavante. He has received research support from AFSP, AHRQ, Brain and Behavior Foundation, Bristol-Myers Squibb, Cederroth, Cyberonics, Elan, Forest Pharmaceuticals, GlaxoSmithKline, Janssen Pharmaceutica, Lichtwer Pharma, Eli Lilly, Mylin (formerly Dey Pharmaceuticals), NARSAD, NIMH, Pamlabs, PCORI, Pfizer, Shire, Stanley Foundation, and Wyeth-Ayerst. Honoraria include MGH Psychiatry Academy in the past three years. Dr. Nierenberg receives other income from legal case reviews for CRICO, MBL Publishing for past services as Editor-in-chief of CNS Spectrums, Slack Inc. for services as Associate Editor of Psychiatric Annals, and Editorial Board, Mind, Mood and Memory, Belvior Publications, and Physicians Postgraduate Press. He has copyright joint ownership with MGH for Structured Clinical Interview for MADRS and Clinical Positive Affect Scale and additional honoraria from ADURS, American Society for Clinical Psychopharmacology and Zucker Hillside Hospital and Forest and Janssen, Biomedical Development, Boston Center for the Arts, University of Pisa, University of Wisconsin at Madison, University Texas Southwest at Dallas, Health New England and Harold Grinspoon Charitable Foundation and Eli Lilly and AstraZeneca, Brandeis University, International Society for Bipolar Disorder, 2nd East Asian Bipolar Forum, Mid-Atlantic Permanente Research Institute, and potentially Up-to-Date. Dr. Nierenberg reports these relationships in the past three years that could be perceived to constitute a conflict of interest.
Dr. Deckersbach has received research support from NIMH, NARSAD, TSA, OCF, Tufts University, NIH, NIA, Janssen Pharmaceuticals, the Forest Research Institute, Shire Development Inc., Medtronic, Cyberonics, and Northstar. He has received honoraria, consultation fees and/or royalties from the following: Medacorp, MGH Psychiatry Academy, BrainCells Inc., Systems Research and Applications Corporation, Boston University, Tufts University, the Catalan Agency for Health Technology Assessment and Research, the National Association of Social Workers Massachusetts, Massachusetts Medical Society, and Oxford University Press.
Dr. Sylvia reports grants from NIMH and the American Foundation of Suicide Prevention. Dr. Sylvia reports being a shareholder in Concordant Rater Systems, being a consultant for United Biosource Corporation and Clintara, and receiving royalties from New Harbinger.