
Abstract
For clinical purposes, psychosis is defined as a discrete entity that can be identified by applying certain criteria. This does not mean, however, that this condition exists as such in nature. Disease at the level of the general population generally exists as a continuum of severity rather than an all-or-none phenomenon [1]. Evidence that variation in the psychosis phenotype can be better represented by the concept of a continuum comes from studies measuring psychotic symptoms in the general population [2–5]. These studies have found that the positive symptoms of psychosis are prevalent in the general population and show a similar pattern of correlation with each other as their equivalents do in clinical psychotic disorder.
The majority of individuals experiencing these ‘symptoms’ are not in need of care. However, longitudinal studies indicate that they may nevertheless have an increased risk of developing a clinical disorder [6–9]. It is crucial to understand the mechanisms that may mediate transition from having one or two psychotic symptoms to becoming a patient with a psychotic disorder. The study of these mechanisms would be particularly important in view of the interest in preventing individuals from making transitions from non-clinical to clinical psychotic states. In addition, it would further our understanding of the continuities and discontinuities between the expression of psychosis at the level of the general population and clinical psychotic disorder [10], [11].
A number of mechanisms relevant to transitions over the psychosis continuum can be envisaged, including biological, psychological, and social factors. The current paper will focus on possible psychological mechanisms. Current hypotheses on psychological mechanisms of psychosis have emphasized that response to abnormal experiences is cognitively mediated by beliefs or appraisals [12–14]. Thus, the mere experience of voices itself may not lead to full-blown psychotic symptoms, but attributing the voice to an external malevolent source and giving it personal significance does. It is this interpretation that causes the associated distress and disability [15], [16] and thereby increases the risk of developing need for treatment.
Another important determinant of the transition to clinical states may be the level of functional coping that the person mobilizes in the face of stressful (psychotic) experiences [17–20]. Active coping strategies, like problem solving, seeking help and distraction are reported to generate control and improve general functioning in people with a diagnosis of schizophrenia [21], [22]. In contrast, symptomatic coping, characterized by going along with and indulging in the content of psychotic symptoms, diminishes the feeling of control. Passive coping strategies such as isolating oneself or getting involved in non-specific activities, are reported to be unrelated to control experience [23], [24]. Previous studies suggested that individuals with psychiatric disorders tend to use more passive coping strategies than healthy controls [25], [26] with people with schizophrenia displaying the least efficient coping strategies such as withdrawal and avoidance [25], [27], [28].
In this article, we bring together data from three previously published papers, in order to investigate the following hypotheses: (i) a delusional interpretation and/ or a depressed response to hallucinatory experiences predicts the later onset of clinical psychotic disorder [29], [30] (Study 1); and (ii) presence of psychotic disorder would be associated with symptomatic coping strategies and less experience of control, whereas active coping strategies would reduce development of need for care status and increase the experience of control [31] (Study 2).
Method
Participants
The Netherlands Mental Health Survey and Incidence Study (NEMESIS) is a longitudinal cohort study of the prevalence, incidence, and course and consequences of psychiatric disorders in the Dutch general population. Subjects were contacted at three points in time, namely 1996 (baseline), 1997 (T1) and 1999 (T2), in order to identify incident cases and to monitor the course of existing symptoms and disorders over time [32], [33]. The sampling procedure and response rate is described in detail in previous work [5], [34]. A total of 7076 subjects aged 18–64 years were enlisted at baseline. At T1, 5618 subjects participated for the second time; at T2, 4848 subjects participated.
Instruments
The Composite International Diagnostic Interview (CIDI) version 1.1 was used [35]. The CIDI psychosis section (G-section) consists of 17 core psychosis items on delusions (13 items) and hallucinations (4 items): items G1-G13, G15, G16, G20 and G21. These items correspond to classic psychotic experiences like persecution, thought interference, auditory hallucinations and passivity phenomena. All these items can be rated in five ways: (i) no experience; (ii) experience present but not clinically relevant (not bothered by it and not seeking help for it); (iii) experience is the result of drug use or somatic disease; (iv) experience is not a real symptom because there appears to be some plausible explanation for it; and (v) true psychotic symptom. Categories ii-v will be denoted hereafter, respectively: NCR symptom (Not Clinically Relevant), secondary symptom, possible symptom and clinical symptom.
Study 1
Baseline hallucinatory experience (HE) was broadly defined as any CIDI rating of NCR, secondary, possible or clinical symptom on any of the 4 CIDI hallucination items, and delusional ideation (DE) at baseline and T1 was broadly defined as any CIDI rating of NCR, secondary, possible or clinical symptom on any of the 13 CIDI delusion items. Baseline presence of depressed mood (DM) was assessed by item E2 of the CIDI depression section (‘Have you ever felt depressed most of the time for a period of 2 years or longer?’). At T1, the period between baseline and T1 was assessed and this rating thus reflects onset of DM 1 year before baseline. At T2, clinical re-interviews were conducted by telephone by a psychiatrist using the two positive psychosis items from the Brief Psychiatric Rating Scale (BPRS) [36] for all individuals who had a rating of NCR, possible or clinical symptom on any CIDI psychosis item. Telephone re-interviews were completed on 74.4% the subjects eligible for re-interview. Two T2 psychosis outcomes were defined, based on the BPRS interview at T2 and clinical judgement of need for care: (i) any psychotic experience at any level on either of the two BPRS items ‘unusual thought content’ and ‘hallucinations’ (score <1, hereafter: BPRS psychotic-like experiences); and (ii) a BPRS score on either of the two psychosis items that was greater than pathology level in terms of severity and functional impairment (i.e. BPRS score <3) and presence of clinical judgement of need for care (hereafter: needs-based diagnosis of psychosis).
All the analyses for this study were conducted in the group of individuals who (i) had undergone both the baseline and the T1 interviews and had received no lifetime diagnosis of any DSM-III-R affective or nonaffective psychotic disorder at either interview; (ii) had had a CIDI interview at T2; and (iii) at T2 had not missed re-interview by clinicians about the presence of psychotic symptoms if they had been eligible for this clinical re-interview. The risk set was the combination of (i) (ii) and (iii) and included 4672 individuals.
Study 2
Coping, subjective distress with and perceived control over the psychotic experience were assessed using the Maastricht Assessment of Coping Strategies (MACS), a semistructured interview administered by a clinician [21], [23]. The MACS focuses on 7 positive symptoms, suspiciousness, thought reading/broadcasting, passivity phenomena, thought insertion/interference, delusions of reference, hearing voices, and other hallucinations. If any of the seven MACS symptoms had been present, the subject was asked: (i) to indicate on a seven-point Likert scale the degree of distress associated with the symptom; (ii) to name all the strategies used to alleviate distress with symptoms; and (iii) to indicate on a seven-point Likert scale the degree of control experienced over the symptom. Patients' descriptions of coping could be scored under any of 14 different strategies (see http://www.macsinfo.homestead.com/index.html). In a previous study, factor analysis of the 14 coping strategies revealed an interpretable pattern of correlation yielding five factors explaining 71% of the variance. The coping strategies distraction, problem solving and help-seeking clustered together in an active problem solving coping factor; the coping strategies prescribed medication, non-prescribed substances, and physical change clustered together in a passive illness behaviour coping factor; the coping strategies shifted attention, socialization, task performance and indulgence clustered together in an active problem avoiding coping factor; the coping strategies isolation, non-specific activities and suppression clustered together in a passive problem avoiding coping factor, and the fifth factor was one on which only symptomatic behaviour (going along with the content of psychotic symptoms) loaded. These factors were not mutually exclusive; subjects could employ coping strategies in more than one domain.
The analysis of the effect of coping style on need for care focused on subjects who had at least one experience of a psychotic symptom (NCR experience, possible or clinical symptom) and no previous diagnosis of any psychotic disorder at T2 (n = 191). To validate the T2 CIDI ratings, clinical re-interviews were conducted over the telephone by an experienced clinician using questions from the Structured Clinical Interview for DSM-III-R (SCID) [37]. If the CIDI rating of the clinician did not coincide with the rating of the lay interviewer, the rating of the lay interviewer was replaced with the rating of the clinician. Telephone re-interviews were completed on 142 (74.4%) of the 191 subjects. In addition, 57 subjects were excluded from the analyses, because they had no NCR experience or clinical symptom rating left after re-interview, resulting in a sample of 85 subjects. All 85 individuals were interviewed with the MACS. Since coping only has meaning in the presence of a symptom generating at least minimal distress, only the individuals with symptom observations that were associated with at least minimal presence of symptom distress were included in the analysis. A total of 47 individuals had at least one symptom observation associated with minimum distress. Of these, 19 had received a needs-based diagnosis of psychosis according to the criteria described above and 28 did not have such a diagnosis.
Analysis
Study 1
In order to test the hypothesis that baseline hallucinatory experience would interact with delusional ideation or depressed mood at T1 in the development of the two psychosis outcomes (BPRS psychotic-like experiences, needs-based diagnosis), an interaction was fitted between presence of HE at baseline (absence vs presence) and presence of DE or DM at T1 (absence vs presence). The coefficient of this interaction reflects the difference in risk for the psychosis outcome between individuals with baseline HE who developed DE or DM at T1 compared to individuals with baseline HE who did not develop DE or DM at T1. In line with recent advances in the conceptualization of interaction, we calculated the statistical additive interaction rather than the multiplicative interaction, as the former is more likely to yield information on the degree of synergism between causes, that is the extent to which both causes depend on each other or coparticipate in disease causation [38]. In order to calculate the statistical interaction under an additive model, the BINREG procedure in the STATA statistical programme was used [39]. This procedure fits generalized linear models for dependent variables with a binomial distribution. The coefficients of the association between the dependent and the independent variables were expressed as the risk difference.
Study 2
The analysis of the coping data was conducted as described in previous publications [21], [23]. A data file was constructed in which each of the 47 subjects included in the study contributed 14 × 7 = 98 observations: one for each of the different combinations of 14 original coping strategies and 7 symptoms of the MACS. These observations will hereafter be referred to as ‘coping observations’. Thus, for each of these 98 combinations patients could have a score of either 0 (indicating they did not use the coping strategy for the symptom) or 1 (indicating they did use the coping strategy for the symptom). The binary coping variable, indicating the presence or absence of coping, was the dependent variable in the analyses. Additional variables included coping type (the 5 coping factors as described above), need for care status (1 = need for care, 0 = no need for care), level of control (scored on 7-point Likert scale), and level of distress (scored on 7-point Likert scale). The file thus contained 47 subjects × 98 = 4606 observations. Of these, 938 were associated with at least minimum distress. These 938 observations were included in the analysis.
Logistic regression analyses were used to investigate the presence of coping (i) in relation to coping type and need for care diagnosis; and (ii) in relation to coping type and the experience of control. Effect sizes were expressed as odds ratios (OR) with a 95% confidence interval (95% CI). Model contributions of independent variables and interactions were assessed by Wald test. Because one subject could have more than one symptom and for each symptom more than one coping strategy, observations were clustered within individuals. Therefore, the CLUSTER and ROBUST options were used in the STATA logistic regression analyses. The CLUSTER option combined with the ROBUST option allows for the use of observations that are not independent within clusters (in this case: within individuals), by using the Huber/White/sandwich estimator of variance instead of the traditional variance estimator.
Results
Study 1
The risk set consisted of 4672 individuals. The number of individuals with T2 BPRS psychotic-like experiences was 85 1.8% and 24 individuals [0.5%] had a need for care in relation to psychotic symptoms. At baseline interview, 287 individuals 6.1% reported HE. Given the presence of HE at baseline, the increase in risk on the additive scale of having the psychosis outcome at T2 was much higher in the group with DE at T1 (n = 30) than in those without DE at T1 (n = 257) (see Table 1). The difference in risks between the groups with and without DE at T1 was statistically significant for each of the two psychosis outcomes (see Table 1). After adjustment for the effect of DE at baseline, the interactions between DE at T1 and HE at baseline remained significant for both psychosis outcomes, indicating that the risk-increasing effect of DE at T1 reflected the emergence of DE between baseline and T1. Similarly, given the presence of HE at baseline, the increase in risk on the additive scale of having the psychosis outcome at T2 was higher in the group with DM at T1 (n = 24) than in those without DM at T1 (n = 263) (see Table 1), although not significantly so for the outcome of BPRS psychotic-like experiences, and this effect remained after adjustment for baseline presence of DM.
Interactions between baseline hallucinatory experiences (HE) and delusion formation (DE) or depressed mood (DM) at T1 in the models of the two T2 psychosis outcomes of BPRS psychotic-like experience and Needs-based diagnosis of psychosis, expressed as the risk difference
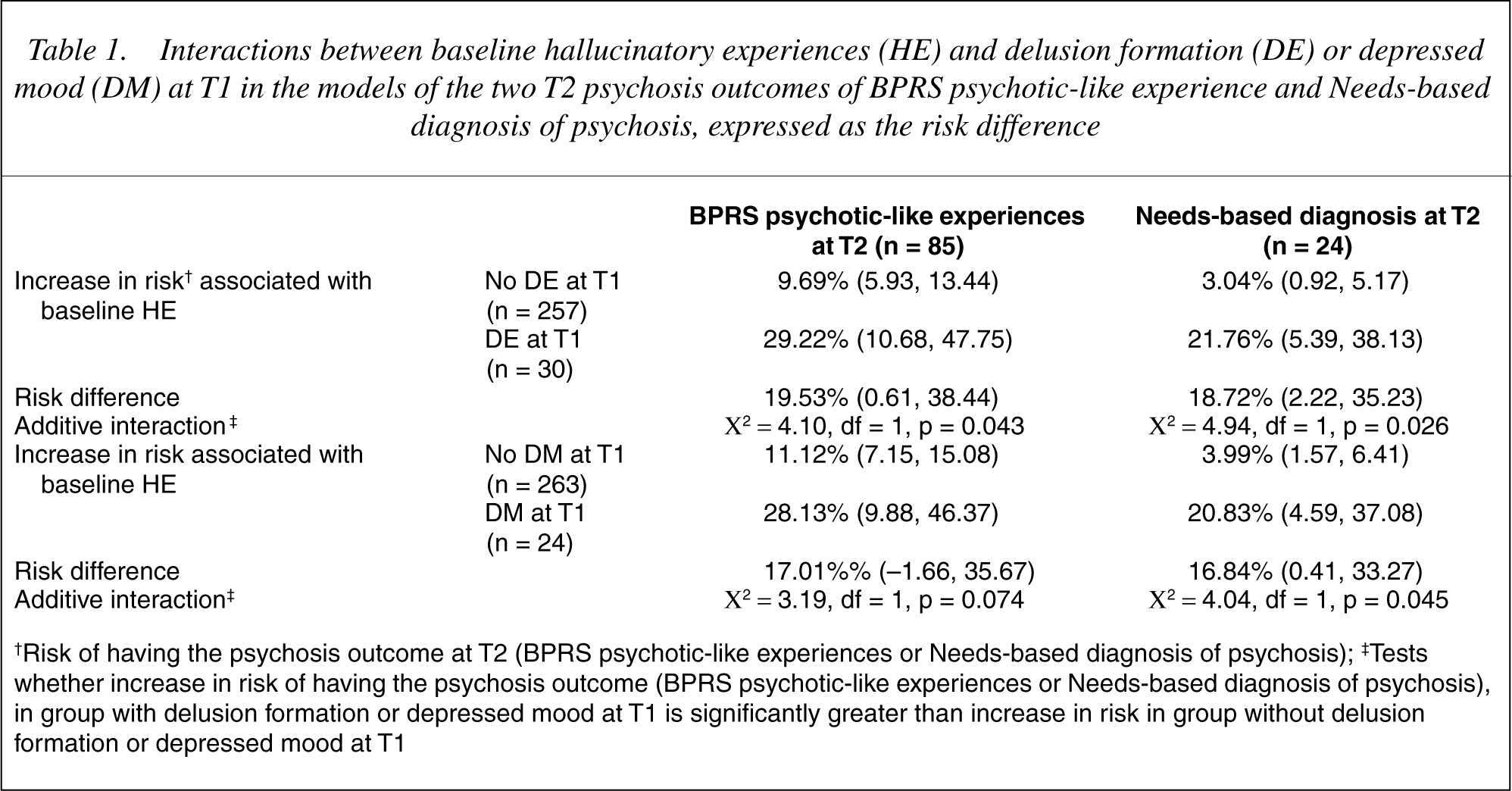
†Risk of having the psychosis outcome at T2 (BPRS psychotic-like experiences or Needs-based diagnosis of psychosis); ‡Tests whether increase in risk of having the psychosis outcome (BPRS psychotic-like experiences or Needs-based diagnosis of psychosis), in group with delusion formation or depressed mood at T1 is significantly greater than increase in risk in group without delusion formation or depressed mood at T1
In order to investigate whether the risk-increasing effects of DE at T1 and DM at T1 overlapped, separate analyses were performed in which the interaction between DE and HE was adjusted for DM and the interaction between DM and HE was adjusted for DE. Adjustment for DM at T1 did not change the interaction between DE at T1 and HE at baseline (for all analyses, changes in risk difference coefficients were between 0.01% and 0.5%). In contrast, adjustment for the presence of DE at T1 reduced but not nullified the risk-increasing effect of DM at T1 in those who reported hallucinatory experiences at baseline. After adjustment for DE, the risk difference between DM at T1 and no DM at T1 was 13.54% (95% CI: −4.34, 31.42; χ2 = 2.20, df = 1, p = 0.138) for the outcome of BPRS psychotic-like experiences, and 14.18% (95% CI: −1.34, 29.71; χ2 = 3.21, df = 1, p = 0.073) for the needs-based diagnosis of psychosis.
Study 2
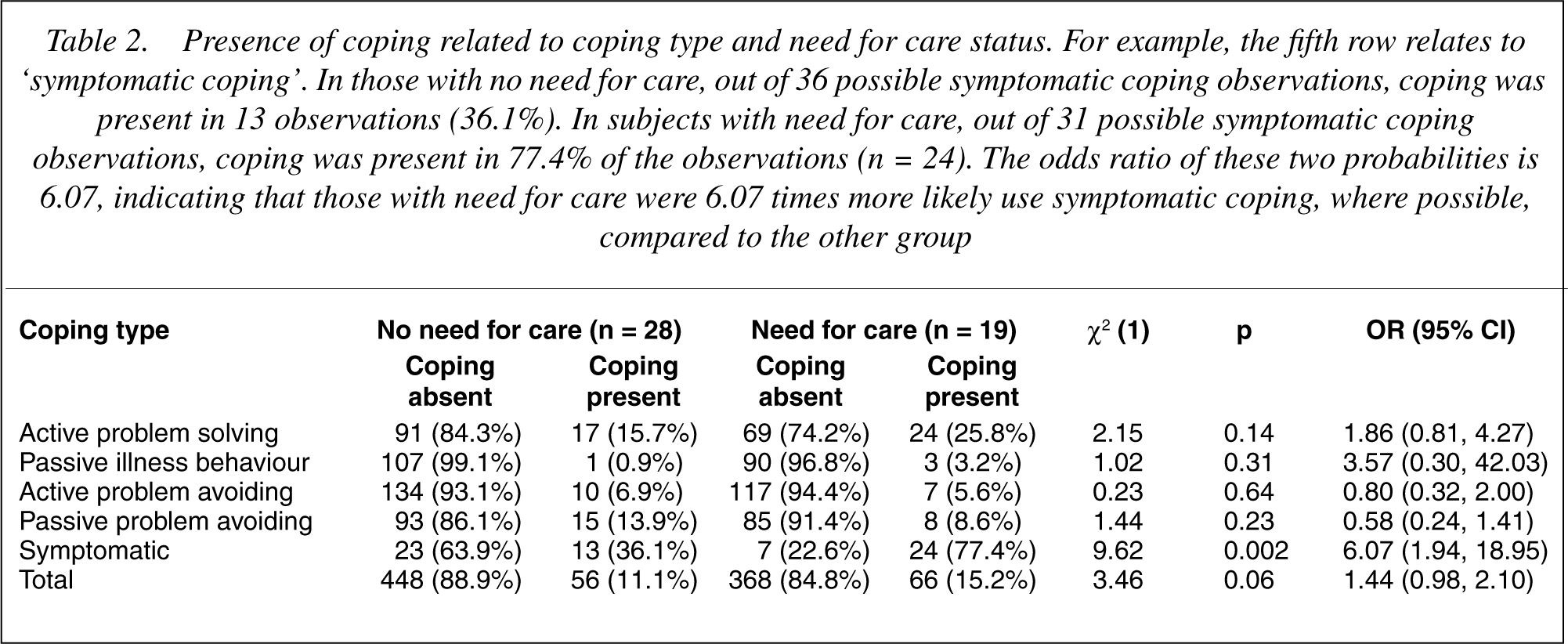
In the combined group of need for care and no need for care subjects, significant associations were apparent between the presence of coping and coping type, indicating differences in the frequency with which coping types were used (test statistic for the 5 coping factors: χ2 = 74.54, df = 4, p < 0.001). In both the need for care and the no need for care group, symptomatic coping was the most common strategy, followed by active problem solving and passive problem avoiding (Table 2). There was, however, a significant interaction between need for care status and coping type (χ2 = 11.15, df = 4, p = 0.025), also after correction for the two BPRS psychosis items as a measure of severity of psychotic symptoms (χ2 = 10.88, df = 4, p = 0.028). This interaction indicated that the two groups used one or more coping types with different frequencies. Examination of the relative distributions of coping type in both groups revealed that those with a need for care were much more likely to display symptomatic coping (OR = 6.07, 95% CI: 1.94–18.95), whereas the presence of the other four coping types was not different across the two groups (Table 2).
Presence of coping related to coping type and need for care status. For example, the fifth row relates to ‘symptomatic coping’. In those with no need for care, out of 36 possible symptomatic coping observations, coping was present in 13 observations (36.1%). In subjects with need for care, out of 31 possible symptomatic coping observations, coping was present in 77.4% of the observations (n = 24). The odds ratio of these two probabilities is 6.07, indicating that those with need for care were 6.07 times more likely use symptomatic coping, where possible, compared to the other group
The presence of coping was not associated with perceived control (OR = 1.05, 95% CI: 0.97–1.13) and this remained so after adjustment for distress (OR = 1.05, 95% CI: 0.98–1.12). However, the association between the presence of coping and experience of control differed as a function of coping type (coping type x control interaction term: χ2 = 19.24, df = 4, p < 0.001). Stratified analyses per coping type revealed that symptomatic coping was negatively associated with control (OR = 0.79; 95% CI: 0.63–0.98), whereas active problem solving was positively associated with experience of control (OR = 1.28; 95% CI: 1.10–1.49).
Discussion
The findings of Study 1 show that, in the general population, the risk of developing clinical psychotic disorder in individuals with baseline self-reported hallucinatory experiences was higher in those who developed delusional ideation than in those who did not. Similarly, the development of depressed mood in those with baseline self-reported hallucinatory experiences increased the risk for onset of clinical disorder, but this effect was partly mediated by the development of delusional ideation. Adjustment for lifetime presence of delusional ideation or depressed mood did not change the pattern of results, suggesting that the risk-increasing effect reflects the effect of the emergence of delusional ideation or depressed mood between baseline and T1. In sum, delusional ideation and depressed mood may arise as a secondary response to hallucinatory experiences in the development of clinical psychotic disorder. A limitation of the current data is that the association between hallucinations on the one hand and delusions and depressed mood on the other is a general one, as we did not have any information linking content of specific delusions to content of specific voices, nor did we have any information that the link between hallucinations and delusions or depressed mood was mediated by cognitive appraisals.
Study 2 shows that individuals with need for care in relation to their psychotic experiences used symptomatic coping more frequently than the individuals without need for care. This was not simply the result of the patient group having more severe psychotic experiences, since the interaction between need for care status and coping type was not reduced and remained significant after adjustment for both BPRS psychosis ratings. The use of coping strategies therefore differed between those with and without need for care independent of their differences in severity of symptoms. In addition, symptomatic coping was associated with less, and active problem solving with more perceived control over the psychotic experience.
Together, our findings suggest that transitions over the psychosis continuum are, at least in part, driven by the emotional, cognitive and behavioural responses to psychotic or psychosis-like experiences.
Mechanisms of delusion formation
The hypothesis that delusions may arise as a secondary response to hallucinations in the development of clinical disorder is not new. According to Maher, delusions reflect perceptual abnormalities, that through normal reasoning leads to a mistaken conclusion [40], [41]. However, the fact that hallucinatory experiences not necessarily evoke delusional interpretation suggests involvement of other factors as well. One of these factors may be information processing. Empirical studies have yielded evidence for cognitive abnormalities in deluded patients [42], particularly, a probabilistic reasoning bias or a ‘jumping to conclusions’ data gathering style [43], [44], a selective information processing bias focused at threat-related information [45], [46], an abnormal attributional style, i.e. strong externalizing and personalizing bias [46], [47], and poor ability to understand and conceptualize the mental processes of other people (theory of mind) [48–50].
Delusions and depression
Delusional ideation may in turn give rise to depressed feelings. It has been suggested that the depressive pathology in the patients with auditory hallucinations could be accounted for by the beliefs held by the individual about the power and intent of their voices, and not by voice topography or voice content [51]. According to these authors, the sense of entrapment in the context of a threatening and powerful entity leads to feelings of powerlessness and depression. These beliefs and the negative emotional states they provoke may then contribute to the maintenance of psychotic symptoms and to the development of illness behaviour [14], [52]. Our finding that the risk-increasing effect of depressed mood was partly mediated by the presence of delusional ideation may be explained along these lines.
Although the interpretation of our findings in terms of secondary beliefs about the voices is attractive, an alternative explanation could be that depression is merely an accompanying phenomenon of severity of the underlying disorder, without being causally involved in the development of need for treatment. On the basis of the current data, this possibility cannot be rejected. A causal explanation would be favoured if the depressed mood could be linked to the content or occurrence of the voices. Possible mechanisms need to be further examined in smaller samples, in which more detailed assessments can be used.
The findings on the role of coping behaviour lend further support to this interpretation of our data. A coping strategy characterized by going along with and indulging in symptoms, yielding less experience of control, discriminates between those with and those without need for care in the context of psychotic symptoms. If distress, anxiety and depression in relation to psychotic illness are associated with perceived controllability, and feelings of subordination to omnipotent voices [15], [51], a symptomatic coping strategy of going along with the content of psychotic experiences may give rise to low perceived controllability and thus contribute to the development of need for care.
Treatment issues
The proposed role for secondary beliefs and appraisals in the onset and maintenance of psychotic disorder has implications for treatment. Cognitive therapy focuses at the modification of cognitive processes [53], [54]. Cognitive behavioural re-appraisal techniques could be instrumental in reducing the depression and fear generated by the voices and enhancing the perceived control over the experience. This may in some individuals prevent the formation of delusions and/or reduce the need for care [16]. Several studies have now evaluated the cognitive approach and have found that modification of beliefs can be successful in reducing the amount of time spent hallucinating as well as in the disruption caused by them [55], [56]. Further elucidation of the cognitive processes involved in the onset and maintenance of clinical psychosis may contribute to the development of targeted psychological interventions.